
Abstract
Background:
A novel COVID-19 has spread worldwide and created a big threat for the public and their daily life. Due to its rapid transmission and the mortality rate, governments across the world had created many restrictions such as social isolation which leads to economic crisis that also leads to the source of fear, stress, anxiety, and mood conditions and negatively affects people’s mental health (Praveen et al., 2021). Although the initiatives were prepared, the coronavirus may also cause mental defects. These defects also affected the medical students, since they were the backbone and the future of public health, hence the study would describe the quality of well-being by different domains.
Materials and Methods:
The study was designed by the questionnaire based on the World Health Organization Quality of life-BREL, Subjective Well-Being Inventory (SWBI), and Beck Anxiety Inventory (BAI) research tool. A total of 288 students were participated in the study.
Results:
A total of 288 medical students were participated in the study, according Cronbach Alpha method, all three domains had obtained a value of above 0.7, and the descriptive analysis showed the highest score of about 67.12 with physical activity. According to the BAI, 84% of medical students with low anxiety, the study also investigates the quality of well-being and compared with gender, with religion, with family type, place of living, religions, and among family’s monthly income. The results of the study were statistically defined, and it has a significant relationship with environment and SWBI.
Conclusion:
The quality of well-being was assessed on medical students and the study revealed that there is no impact with gender, religion, year of study, and family’s monthly income. Although the study also revealed that the mean score of social well-being is high with physical activity and considerably low with psychological and environmental activity.
Keywords
Introduction
A novel coronavirus infection disease 2019 (COVID-19) was first identified at Wuhan, China, during December 2019. Besides, it was started to spread vigorously worldwide and it has created a public health emergency. Meanwhile, the World Health Organization (WHO) announced that COVID-19 is a pandemic disease on March 11th, 2020.[1,2] In India, the first case COVID-19 case was confirmed on January 30th, 2020, and as of April 27th, 2020, nearly 30,000 cases were diagnosed and the mortality reached above 900 numbers.[3] Due to the high transmission and mortality rates of COVID-19, the scientific community has been actively engaged in monitoring its global spread and focusing on the development of treatment methods, vaccines, and prevention strategies.[4] Apart from that the epidemic seems to sustained and leads to extended social isolation and adverse economic effects. Moreover, COVID-19 has been considered a source of fear, stress, anxiety, and mood conditions and negatively affects people’s mental health.[5]
The fear of the COVID-19 pandemic can harmfully affect disease management. Fear is an emotional response developed by an individual against any kind of threat, and it leads to physiological changes in the human.[6,7] Infectious diseases are a predominant and leading source of fear because they are transmissible, imminent, and invisible. Hence, the COVID-19 pandemic is considered an important source of fear across the world.[8]
Since there are many negative changes were observed during the time of COVID-19 spread, such as the shutdowns of most of universities and institutions all over the world. Moreover, resident students are shifted to off-campus in some cases to decrease the transmission rate in intensive hostel settings. Addition to that direct physical classes were modified to online classes to avoid direct contact of teachers with students in person. Besides, many students were adversely influenced by work conditions and financial losses and finally, it is end with suicides in the worst scenario. The suicide happened at India during the lockdown time, a female student thought that her educational performance was greatly affected due to the online class since she does not have the facility to attended the online or television learning content.[9,10]
During the time of COVID-19 lockdown, fear is spread among the public and it can psychologically affect the public mind[11] and their lifestyle behaviors.[12] Psychological factors are very essential for understanding and handling broader societal problems related outbreaks.[13] Even though COVID-19 does not have a properly defined treatment, vaccine and the inability to control the disease spread directly affects the psychological health of people.[14] Some scientists have already carried out the studies on fear of people against COVID-19 that is spreading among worldwide. The Fear of COVID-19 Scale (FCV-19S) was developed with the aim of quelling fear of COVID-19 and for other goals.
During the COVID-19 time, India faced the biggest restriction on human movement in history. The daily routine is important for human life for their physical and mental health, and most important for students in their psychological and emotional development. Medical students are the backbone and future of the health system and the general public always looks up to them as the role model of society. During the COVID-19 lockdown of the country, mental health problems with respect to the quality of life (QOL) often remain neglected in medical students. The WHOQOL-BREF is being developed as a short version of the WHOQOL-100 for use in situations where time is restricted; where respondent burden must be minimized, and where facet-level detail is unnecessary. This tool was used to evaluate the QOL among medical students in Erode district, Tamil Nadu, India.
Materials and Methods
Study design
The study was a descriptive and qualitative method that utilizes research tools, random sampling method techniques were used. A total of 288 medical students were participated in this analysis. The self-administered, questionnaire was proposed using three domains WHOQOL-BREF, Subjective Well-Being Inventory (SWBI), and Beck Anxiety Inventory (BAI).
The reliability analysis was done by analyzing the reliability of the questionnaire to all domains by Cronbach alpha method. The sociodemographic analysis of participants was analyzed through various variables such as gender, birth order, number of siblings, religion, type of family, place of living, year of study, and monthly family income.
Demographic tool
According to the Cronbach alpha, the relativity measured above 0.7 was considered to be acceptable Likert questionnaire analysis. The QOL well-being is analyzed by WHOQOL-BREF has four domains, namely physical health, psychological health, social relationships, and environment, total SWBI developed by Sell and Nagpal[15] that contains 11 factorial domains such as positive effect, expectation-achievement congruence, confidence in coping, transcendence, family group support, social support, primary group concern, inadequate mental mastery, perceived ill-health, deficiency in social contacts and general well-being negative affect, and total Beck anxiety inventory (BAI). The score ranges from 1 to 3, the positive effect secures the highest score, and the negative effect secures the least score. The sum of all questionnaires results in overall well-being.
Data analysis
The survey results of the questionnaire were extracted and recorded using MS Excel and then imported and analyzed using Statistical Package for Social Sciences for Windows, Version 22 (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. IBM Corp). Univariate descriptive analysis such as frequency and the percentage was for sociodemographic and categorical (nominal and ordinal) demographic variables and dependent variables were analyzed. Descriptive statistical measures were calculated for numeric scale variables. Chi-squared test of association was used to study the significant associations between categorical sociodemographic variables versus categorical-dependent variables. One-way analysis of variance (ANOVA) was used to compare the mean values of numeric variables with demographic variables containing more than two levels. Pearson correlations were used to examine the relationship between any numeric variables (personality traits, global scores, and subscales of the Pittsburgh Sleep Quality Index [PSQI]). P < 0.05 is considered statistically significant.
Results
The reliability analysis for all the domains according to their questionnaires was done by the Cronbach alpha method and the values above 0.7 are acceptable, by observing the value, all three domains had values above 0.7 and the results are shown in Table 1.
Reliability analysis of all domains
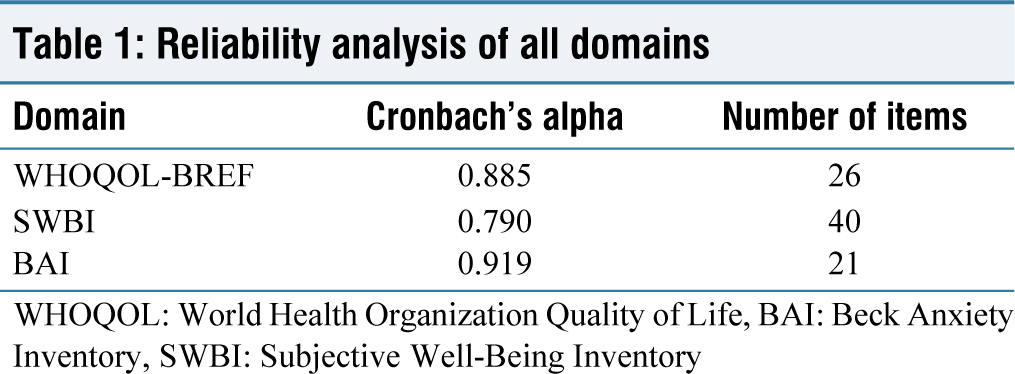
WHOQOL: World Health Organization Quality of Life, BAI: Beck Anxiety Inventory, SWBI: Subjective Well-Being Inventory
A total of 288 students were participated in the study, majority of the participants were female (68.4%) and male students were about (31.6%), by birth order, the youngest were 41%, the eldest were 36.1%, by number of siblings, n = 1 had reported the highest count for about 62.8%, by religion Hindus were about 81.9%, followed 10.4% of Christians and 7.6% of Muslims, by type of family, nuclear family has the highest number of participants, by place of living, rural student participants were high and it was about 35% and by family’s monthly income, 61,000–75,000 were about 21.5% [Table 2].
Types of participants differentiated by demographic variables
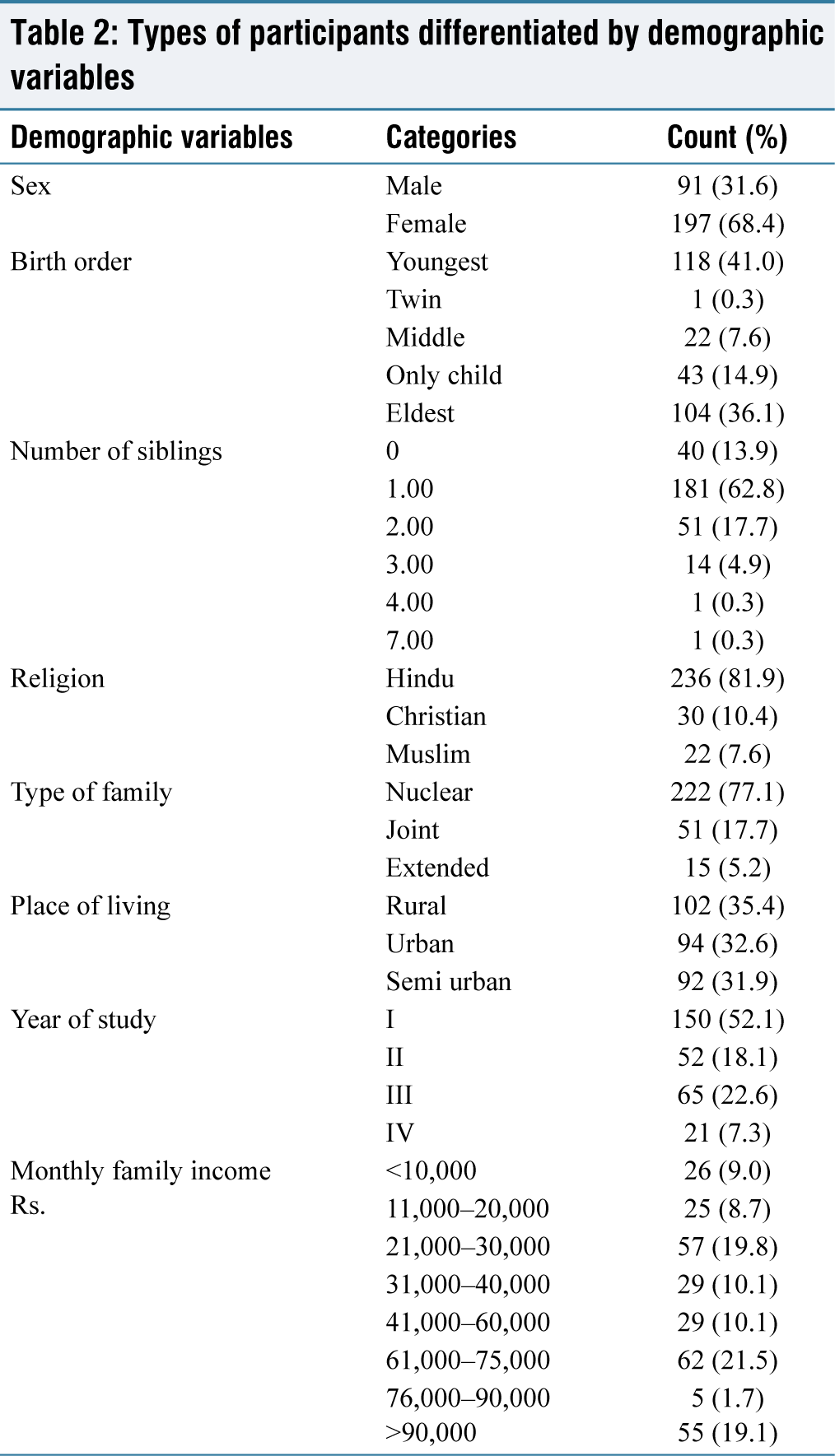
Table 3 shows the descriptive statistics of all domains among medical students on the QOL includes physical, psychological, social, and environmental activities. The highest score was obtained with a physical activity of about 67.61 and the least of about with psychological of 60.74. The study found that there were no significant differences in quality of life between males and females on any of the WHOQOL-BREF domains (physical, psychological, social, and environment) or on the SWBI total score. However, males had a significantly lower BAI total score than females, indicating that they had less anxiety [Table 4].
Descriptive statistics of all domains
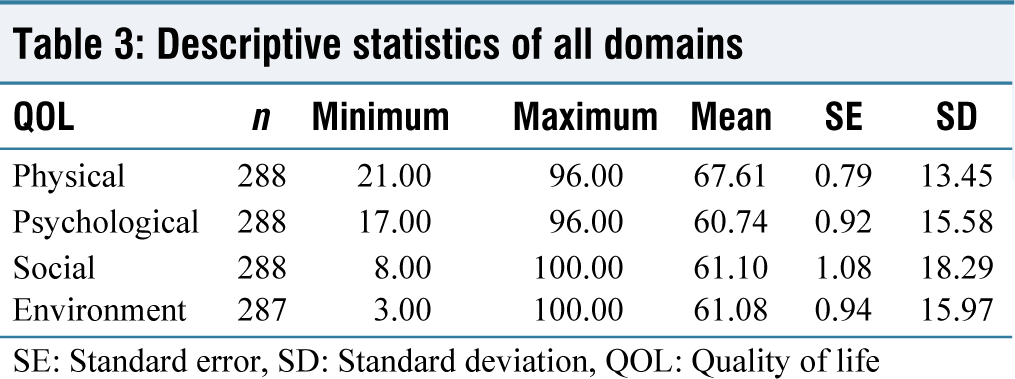
SE: Standard error, SD: Standard deviation, QOL: Quality of life
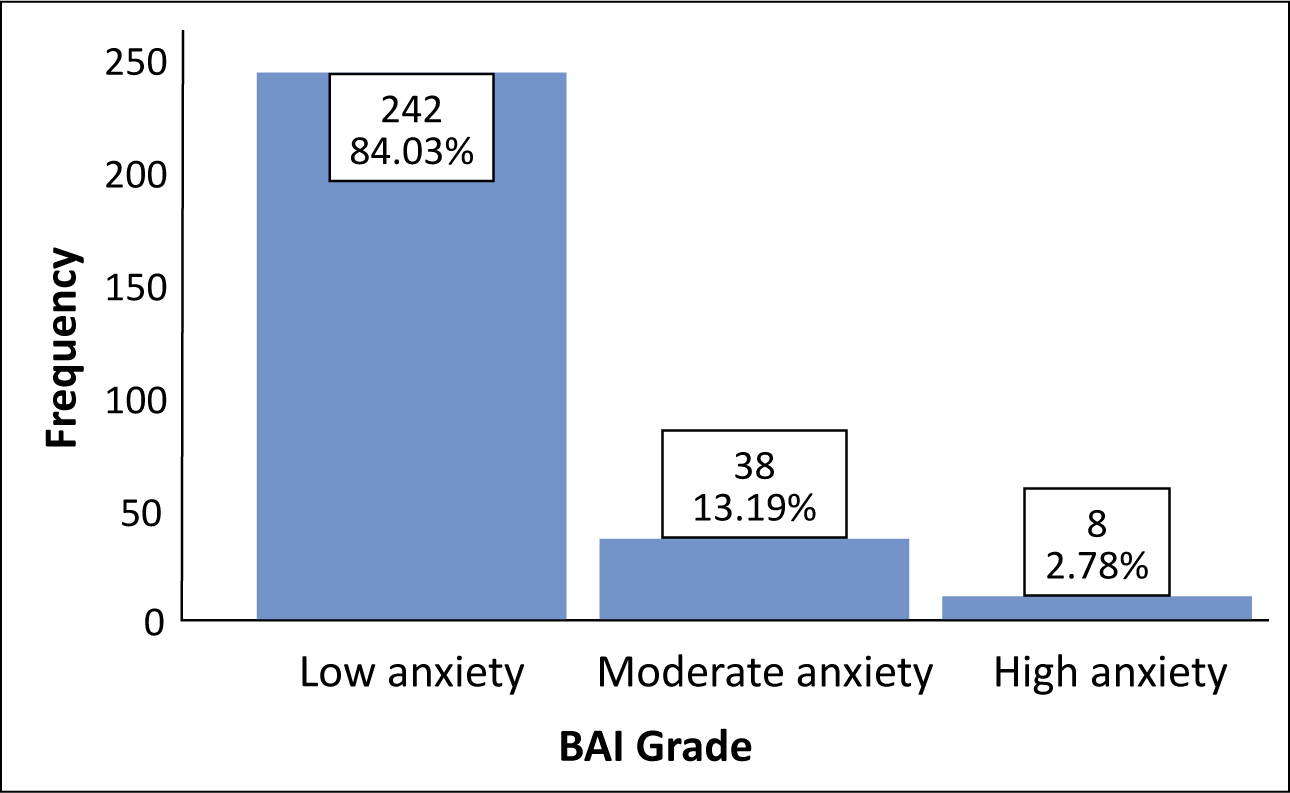
According to the BAI, the sum of 21 items revealed the score for the grade of anxiety which showed 84% of medical students were showed low anxiety, 13.2% of them were in moderate anxiety, and 2.8% of students were under high anxiety [Figure 1].
The Chi-square tests revealed that there was a significant association observed between PSQI grade, depression, anxiety, and BAI grade versus types of the family (P < 0.05). It was also observed that there is no significant association between other parameters such as gender, place of living, religion, family’s monthly income, and year of study.
Subject well-being inventory and anxiety variable
The comparison of quality of well-being with the Subject Well-Being Inventory and anxiety variable under four domains revealed that there is no significant difference between males and females, with religion, with family type, place of living, religion, and among family’s monthly income. It was also observed that there is a significant relationship was observed between environment and SWBI (P < 0.05).
One-way ANOVA test results show that the mean score of physical QOL only significantly differs among birth order which obtains 0.02 (P < 0.05). There was no significant difference in the mean score of the rest of the domains with the birth order of students (P > 0.05).
By comparing the monthly income groups, one-way ANOVA test results show that the mean scores of depression and anxiety differ significantly among the different income levels (P < 0.05). However, the rest of the domain mean scores did not differ significantly among the different income levels.
Comparing the mean score of quality of life, subject well-being, and anxiety with gender
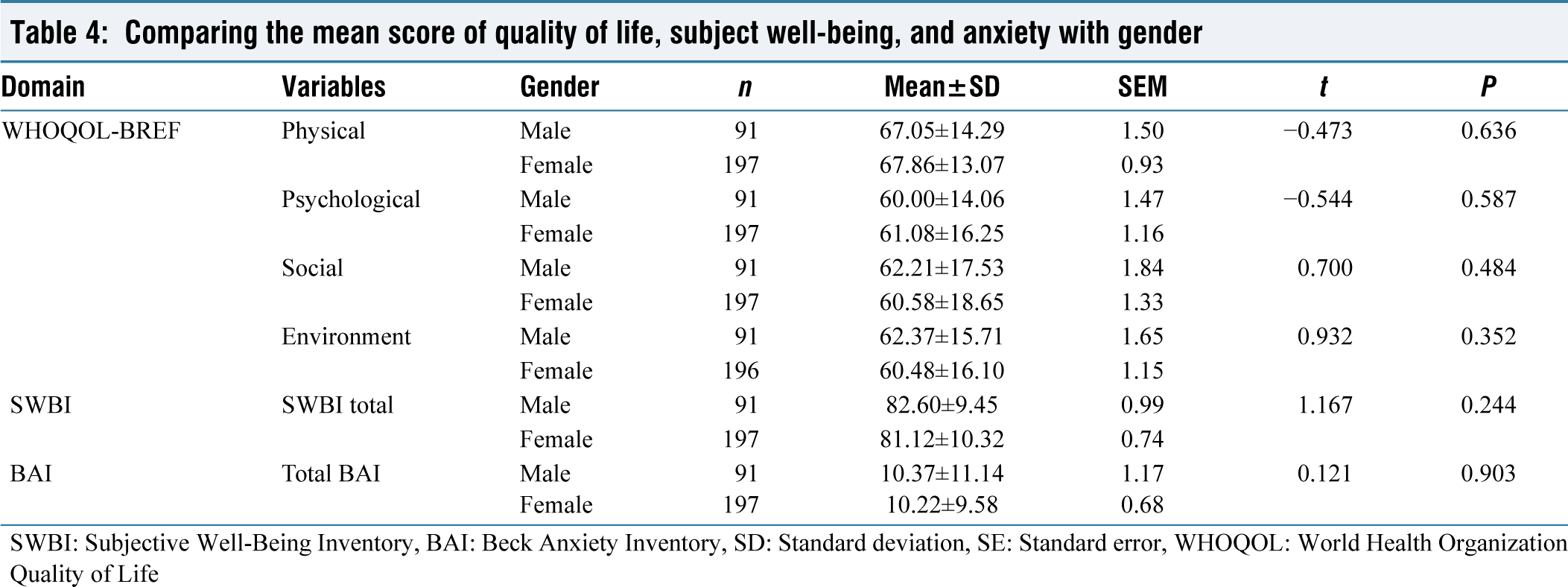
SWBI: Subjective Well-Being Inventory, BAI: Beck Anxiety Inventory, SD: Standard deviation, SE: Standard error, WHOQOL: World Health Organization Quality of Life
Beck Anxiety Inventory percentage of medical students during the COVID-19 lockdown. BAI: Beck Anxiety Inventory
Discussion
Human beings are considered habit creatures and favor to live in a highly sophisticated and well-organized environment.[16] An unnatural and unhealthy merited stress is the source for rapid changes of human healthy life in one’s day-to-day lifestyle. Human are able to create a routine and organized lifestyle through their habits.[17] These habits are used to possess their legendary activity in one’s day-to-day living constant. In these contrast, Judah et al.[18] quoted that the behavior of habit forming is a healthy and fundamental inspiration. The COVID-19 pandemic lockdown occurred at an unexpected time and it has interrupted many of our ingrained and important habitual acts, which has led to a psychological impact of human beings.
In our present study, we have chosen four criteria such as physical, psychological, social, and environmental changes to check the QOL of medical students. The four different selected criteria were analyzed by three different statistical tools such as WHOQOL-BREF, SWBI, and BAI. Our investigations output revealed that Cronbach alpha values of WHOQOL-BREF, SWBI, and BAI attained 0.885, 0.790, and 0.919, respectively. Cronbach’s alpha is an appropriate assessment tool used to evaluate the reliability or internal consistency of a composite score. Many of the other sources indicated that above 0.70 is an acceptable range of reliability.[19] Our study results matched with, Peterson[20] stated that, the acceptable value of Cronbach’s alpha can vary between 0.5 and 0.95 depending on the type of research. For basic research, Cronbach’s alpha should be higher than 0.7–0.8. Similar to our study,[3] reported that, Cronbach’s α coefficient value was 0.883 for the questionnaire WHOQOL-BREF toward the impact of coronavirus lockdown on the mental health of medical students. Another study on SWBI assessment of the mental health of European public during the COVID-19 pandemic outbreak clearly indicated that Cronbach’s alpha is observed in the range of 0.806 in psychological stress and 0.892 in mental health.[21] Landaeta-Díaz et al. studied the relationship between lockdown and the level of anxiety through the BAI and reported that the level of anxiety was found to be a 0.719 Cronbach’s alpha value.[22]
The mean score our current study attained highest for physical (67.61 ± 13.45), followed by social (61.10 ± 18.29), environment (61.08 ± 15.97), and lowest for the psychological domain (60.74 ± 15.58). Similar to our work, a study on the impact of COVID-19 on the quality of medical students at Himachal Pradesh, India, showed the environmental domain managed the highest mean score of 72.10 ± 13.0, followed by physical (67.23 ± 13.74), social (57.13 ± 20.1), and psychological (52.10 ± 17.45).[3] Likewise, Henning et al. reported the highest score for the physical domain (71.74 ± 15.12), followed by social (68.95 ± 20.28), environmental (68.66 ± 14.53), and lowest for the psychological domain (65.20 ± 16.41).[23]
In our study, the mean score of physical (67.86 ± 14.29 vs. 67.05 ± 14.29) and psychological domain (61.08 ± 16.25 vs. 60.00 ± 14.06) was found higher in females, whereas social (62.21 ± 17.53 vs. 60.58 ± 18.65) and environmental (62.37 ± 15.71 vs. 60.48 ± 16.10) were found higher in male students. Our study findings were supported by different researchers and were reported the same as females were found higher in physical and psychological domains in different countries.[24] Nayak et al. reported that a mean score of physical (73.8 ± 11.8 vs. 70.0 ± 12.0), psychological (67.3 ± 12.8 vs. 61.3 ± 15.5), and social domain (71.3 ± 17.5 vs. 69.5 ± 19.9) was seen higher in students belonging to rural areas while environmental domain (67.4 ± 12.0 vs. 67.9 ± 14.3) score was higher in students with the urban nativity.[24]
Conclusion
The COVID-19 pandemic negatively impact higher education due to the ongoing pandemic lockdown. In general, medical students are always under stressful conditions due to their overwork load and variety of training sessions, since the COVID-19 pandemic lockdown has caused additional stress and anxiety among medical students by disrupting their routine life. Our present findings demonstrated that during this lockdown time, medical students were weaker in all four domains of QOL. Considering the importance of medical students, since they are the backbone of our health system and they are essential to provide the QOL to the general public. Considering this aspect, it is crucial to maintain the mental health of the medical student during this pandemic lockdown time.
Footnotes
Acknowledgements
We sincerely thank each and every one of the participants for taking the time to complete our study. The authors thank the Government Erode Medical College and Hospital, Perundurai, Tamil Nadu, for providing the necessary facilities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval Number
Ethical approval for the study was given by the Government Erode Medical College and Hospital, Perundurai, Erode Institutional Ethical Committee Vide Reference number: IEC/001/GEMC and H/2020 dated: July 31, 2020. Written digital consent was obtained from study participants before completing the survey form. Participants gave their consent by ticking the designated box. Personal identifiers such as names were not collected during the study.
CRediT Author Statement
Conceptualization: Panneerselvam Periasamy Data curation: R. Niruba and A V Mathivadhana Formal analysis: Vijayalakshmi I and R. Niruba Methodology: K C Subha and Panneerselvam Periasamy Project administration: Panneerselvam Periasamy Resources: Vijayalakshmi I and A V Mathivadhana Supervision: Vijayalakshmi I and K C Subha Validation: Panneerselvam Periasamy Visualization: R. Niruba and Panneerselvam Periasamy Writing - original draft: R. Niruba and A V Mathivadhana Writing - review and editing: K C Subha and Panneerselvam Periasamy.
Data Availability
All datasets generated or analyzed during this study are included in the manuscript.
Use of Artificial Intelligence
No, authors have not used Artificial Intelligence in this research.