
Abstract
Introduction:
The objective of our study was to examine the clinical characteristics and underlying risk factors of acute ischemic stroke in patients aged 18–45.
Materials and Methods:
We prospectively studied etiology of patients aged 18–45 with acute ischemic stroke presenting to our hospital from September to December of the following year. We aimed for 80% statistical power at a 5% significance level with a precision of 0.15, which led us to a calculated sample size of 39.
Results:
Fifty patients were observed. The main risk factors identified were alcohol use (36%), smoking (30%), and hypertension (22%). Prothrombotic states were found to be a significant risk factor in cases where the stroke’s origin was undetermined. The most common stroke subtype was large-artery atherosclerosis, which was followed by strokes with other underlying causes. There was a statistically significant association between hypertension and ischemic stroke subtypes (P = 0.01). Hypertension was associated with small-vessel disease (92.3%) and strokes with undetermined causes (56.5%), with P = 0.023 and P <0.001, respectively.
Conclusions:
Hypertension was associated with multiple stroke subtypes in young individuals. Therefore, it is essential to strictly control hypertension through antihypertensive therapy and lifestyle changes. As alcohol use and smoking are becoming more prevalent among young individuals, early implementation of awareness programs targeting primary stroke prevention is highly desirable.
Introduction
According to current estimates, around 10% to 15% of all stroke cases occur in young adults, which has a significant impact on public health despite being less common.[1] Stroke in young individuals requires a different management due to a more diverse range of risks. Smoking and alcoholism are important risk factors among the younger population. While general management approaches remain similar, primary prevention measures deserve particular attention. Our purpose was to observe the clinical profile and underlying risks of ischemic stroke in patients aged 18–45.
Materials and Methods
We conducted a prospective observational study at the Department of Neurology, Indraprastha Apollo Hospital in New Delhi, for 16 months, from September to December of the following year. The sample size was determined based on a previous study using the formula proposed by Charan and Biswas in 2013.[2-3] With 80% power, a 5% significance level, and a precision of 0.15, the estimated sample size was 39. We included patients aged 18–45 who were diagnosed with acute ischemic stroke (clinically and radiologically confirmed) and admitted to the outpatient department, ward, or emergency department. Patients of any gender who provided consent to participate were included in the study, whereas those with head injuries, subarachnoid hemorrhage, cerebral venous thrombosis, intracerebral hemorrhage, age below 15 years or above 45 years, or brain lesions were excluded from the study. A total of 50 patients were included in the study. Detailed history taking, physical examinations, and investigations were conducted using a semi-structured pro forma, which collected information on patient particulars, presenting complaints, family history, past medical/surgical history, and substance abuse history. General physical and systemic examinations were performed using the national institute of health stroke scale (NIHSS) scoring scale. Relevant investigations such as complete blood count, blood glucose, serum lipid profile, serum protein C, protein S, homocysteine, antithrombin III, and antiphospholipid antibody were conducted and recorded. Additional tests, including chest X-ray, computerized tomography scan of the brain, magnetic resonance imaging of the brain, magnetic resonance angiography of the brain, electrocardiography, and echocardiograms, were performed on a case-by-case basis.
The trial of org 10172 in acute stroke treatment (TOAST) classification consists of five major categories: large-artery atherosclerosis (LAA), cardioembolism (CE), small-vessel occlusion, stroke of other determined cause (OC), and stroke of undetermined cause (UND). Personal interviews and reviews were conducted to gather relevant information from patients or their relatives. Laboratory values were obtained from the hospital facility. The study protocol received ethical committee clearance, and subjects provided informed consent before enrollment. The results were analyzed using frequencies, percentages, and mean ± standard deviation. The Chi-square test was used for comparisons, with a P <0.05 considered significant. Statistical analysis was performed using SPSS version 16.0 (Chicago, IL, Inc., USA).
Results
Maximum patients were > 40 years (34%), followed by 36–40 years (24%), 31–35 years (22%), 25–30 years (18%), and < 25 years (2%). The mean age was 36.58 ± 6.10 years (24–45 years). The majority was males (82%), as shown in Figure 1.
Distribution of patients according to clinical presentation
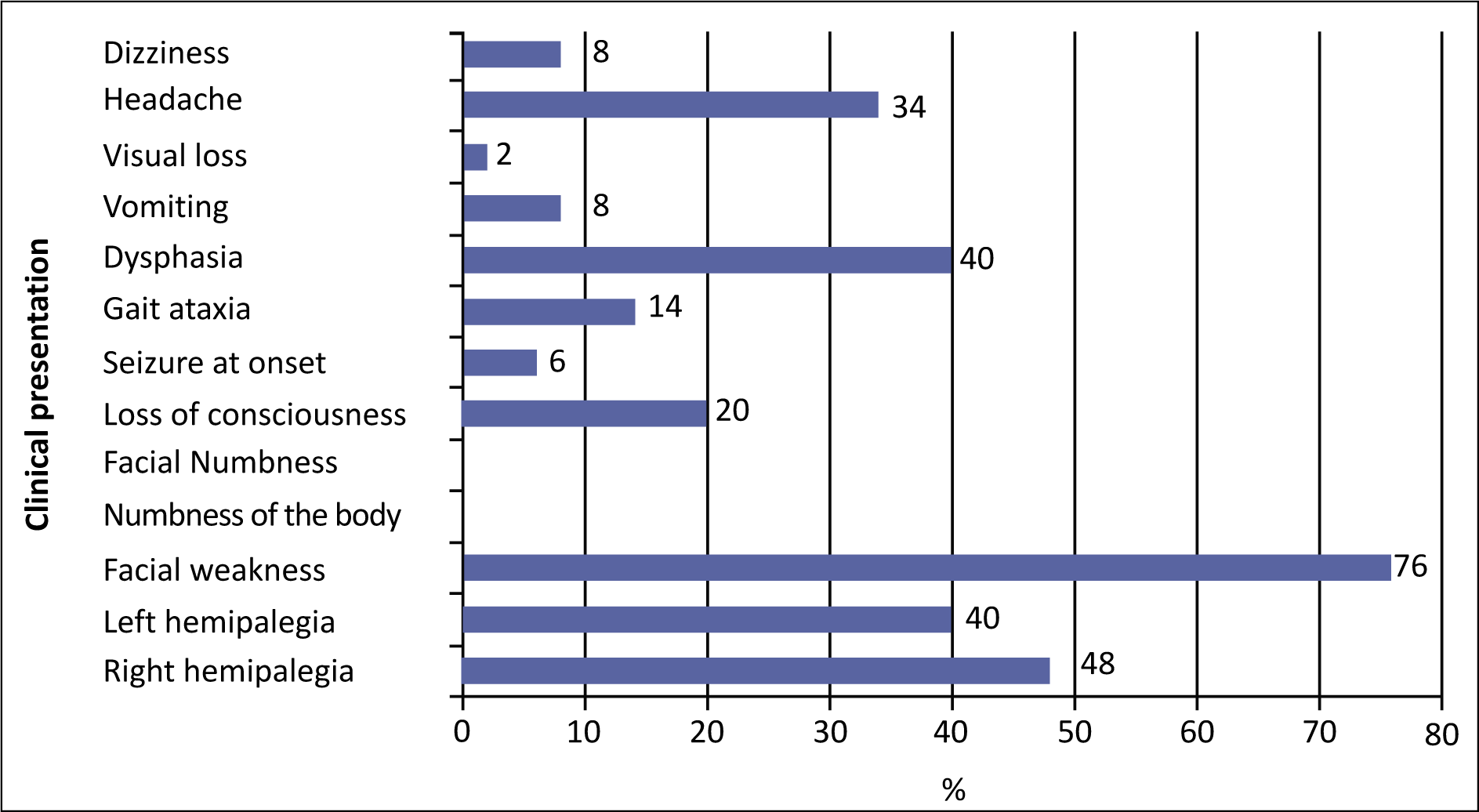
Out of 50 patients who had a stroke, alcohol intake was most common risk factor (36%), followed by smoking (30%), hypertension (22%), and type 2 diabetes mellitus (20%).
Among prothrombotic state as a risk factor for ischemic stroke, abnormal serum homocysteine was among 74% of patients, abnormal protein C and S in 26%, and abnormal antithrombin III was among 24% of patients.
As per national institute of health stroke scale (NIHSS), moderate stroke was among the majority of patients (70%), followed by minor stroke (24%) and severe stroke (6%).
LAA (embolus/thrombosis) ischemic stroke subtype was most common in ages 30–40 years (44.4%). However, CE (high-risk/medium-risk) ischemic stroke subtype was most common in ages > 40 years (29.4%). Small-vessel occlusion (lacunae) ischemic stroke subtype was most common in ages > 40 years (23.5%). There was no statistically significant (P > 0.05) association of age with ischemic stroke subtypes [Figure 2].
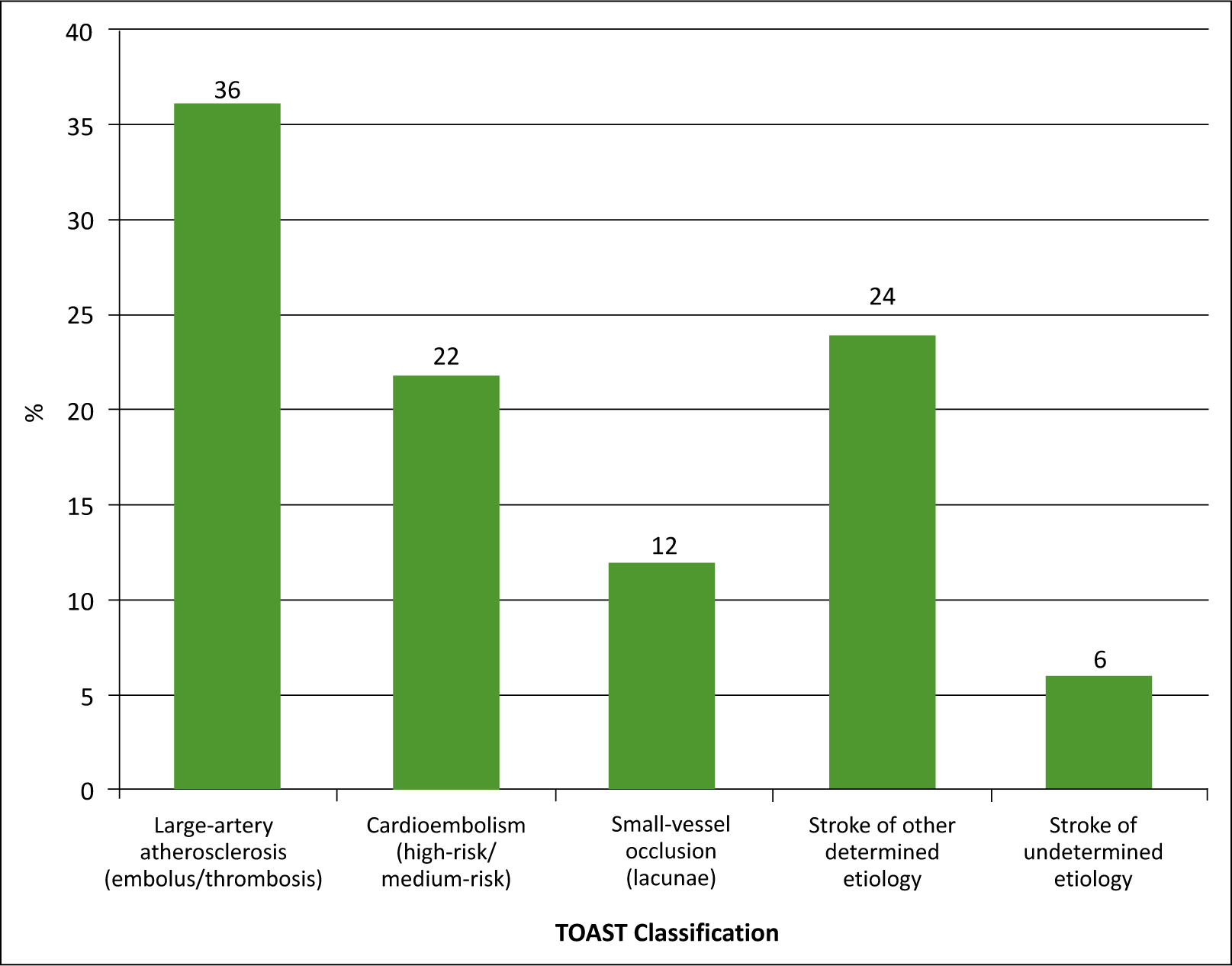
The distribution of patients according to TOAST classification
In studying the association of body mass index (BMI) with ischemic stroke subtypes, LAA (embolus/thrombosis) ischemic stroke subtype was found to be most common in preobese patients (43.8%). However, CE (high risk/medium risk) ischemic stroke subtype was most common among normal BMI patients (45.5%). Small-vessel occlusion (lacunae) ischemic stroke subtype was most common in preobese patients (18.8%).
Table 1 shows the association of risk factors with ischemic stroke subtypes. Stroke of other determined etiology ischemic stroke subtype was most common among whom hypertension risk factor was present (54.5%). The hypertension is associated with ischemic stroke (P = 0.01).
Association of risk factors with ischaemic stroke subtypes
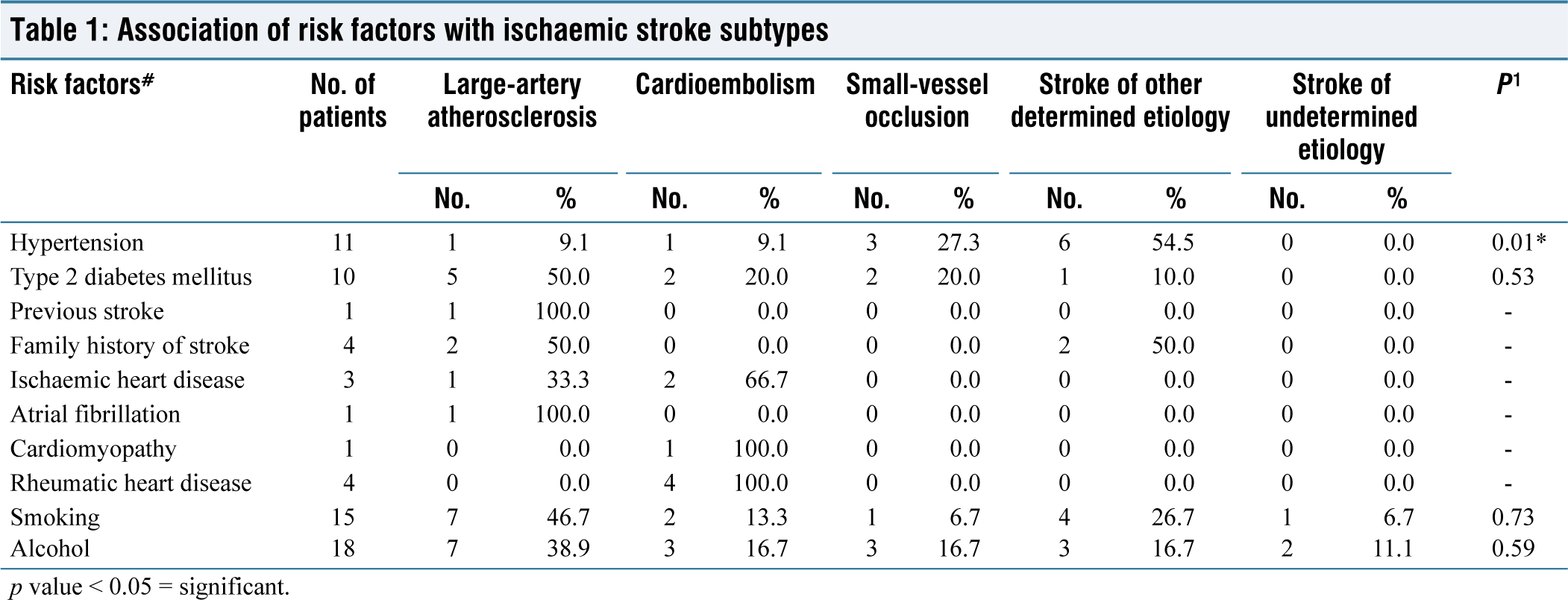
p value < 0.05 = significant.
Table 2 shows the association of lipid profile, erythrocyte sedimentation rate, antinuclear antibody, and C-reactive protein levels with ischemic stroke subtypes. LAA (embolus/thrombosis) ischemic stroke subtype was most common among those total cholesterol (60%), triglycerides (40%), high-density lipoprotein (46.4%) and low-density lipoprotein (53.8%) were abnormal (i.e. dyslipidemia present).
Association of serum levels with ischaemic stroke subtypes
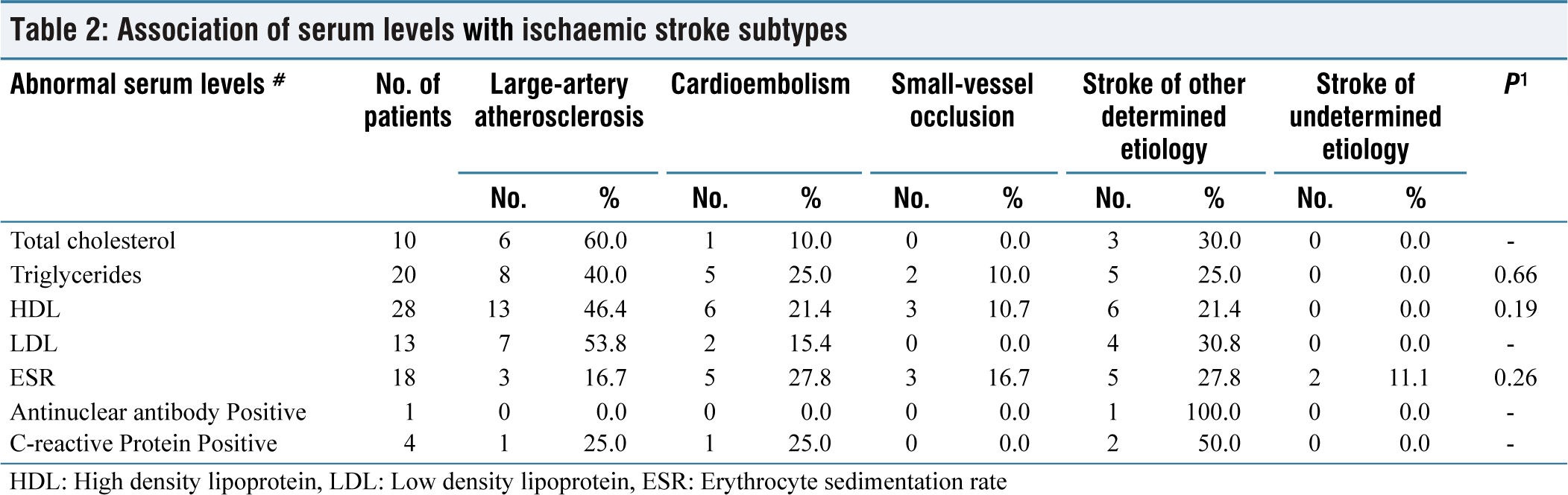
HDL: High density lipoprotein, LDL: Low density lipoprotein, ESR: Erythrocyte sedimentation rate
Table 3 shows the association of hypercoagulable state with ischemic stroke subtypes.
Association of Hypercoagulable state with ischaemic stroke subtypes
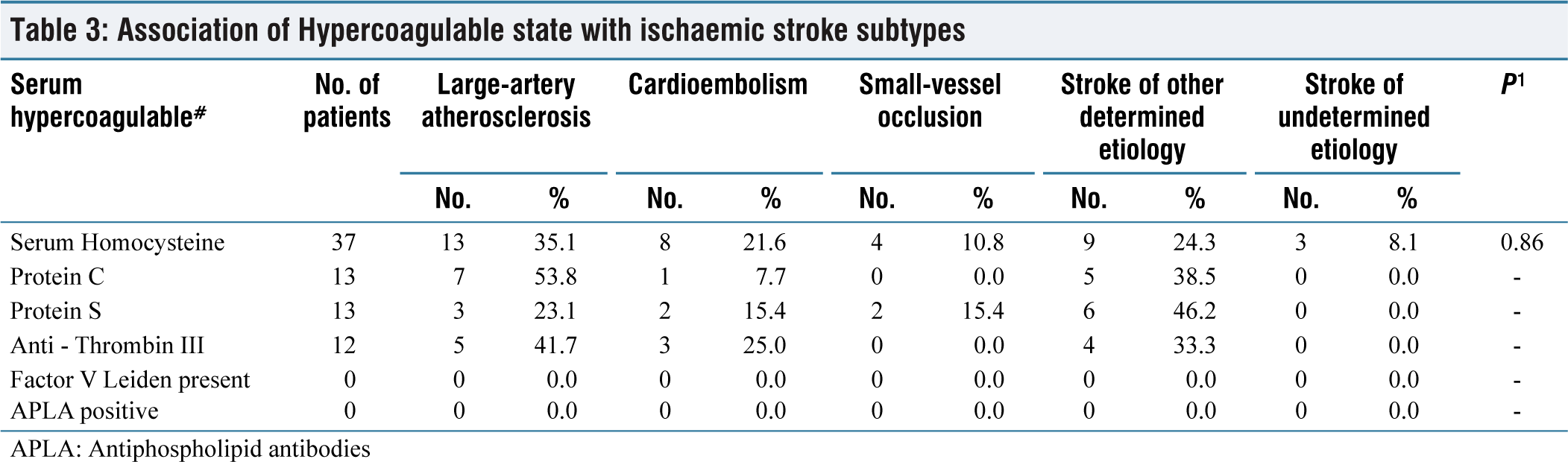
APLA: Antiphospholipid antibodies
Discussion
Stroke incidence increases exponentially after the age of 30 years, and the risk factor of stroke varies across different age groups. While the majority of strokes occur in individuals over 65 years old, there is a growing prevalence of stroke among younger people.[4,5]
In a study from North India by Mehndiratta et al. in 2004, the mean age was 31.97 years, with males having a mean age of 30.66 and females 33.28 years.[5-6] In our study, the average age of patients was 36.58 ± 6.10 years, with a higher proportion of patients over the age of 40 years.
The most common risk factors in our study were alcohol intake (36%), smoking, hypertension, and type 2 diabetes mellitus.[7] Hypertension was independently associated with small-vessel disease and diabetes in a study by Arboix et al. in 2007.[7-8]
Among strokes of OC, our study found that a significant number of cases had a prothrombotic state related to deficiencies in protein C, protein S, or antithrombin III. Abnormal serum homocysteine levels were observed in 74% of patients. Studies have found protein C and protein S deficiency in 2.5% and 6.8% of cases, respectively, among young ischemic stroke patients. Antithrombin III deficiency was present in 1.9% of patients.[9,10]
Regarding the severity of stroke, our study revealed that 55.91% of patients had a moderate stroke at the time of admission, whereas 24.19% had a severe stroke, and 12.37% had a very severe stroke. Only 18.82% of patients had a minor stroke.[5]
According to the TOAST classification, the most common subtype of ischemic stroke in our study was LAA (embolus/thrombosis), accounting for 36% of cases, followed by stroke of OC (24%), CE (22%), small-vessel occlusion (lacunae) (12%), and stroke of UND (6%). Similar results were found in studies conducted by Harris et al. in 2018, Porcello Marrone et al. in 2013, and Deleu et al. in 2011.[6-15]
Conclusions
Our study’s most common etiology of ischemic stroke was LAA, followed by a stroke of OC. This study showed that hypertension was significantly associated with stroke subtypes. Alcohol abuse and smoking were found to be common risk factors for ischemic stroke in young. Hence, primary prevention with antihypertensives and abstinence from alcohol and smoking is warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Ethical Committee Approval
All methods were carried out in accordance with relevant guidelines and regulations. All investigational protocols and methodologies were approved by ethics committee. A written informed consent was taken from each participant of this study for participation in the study and for sharing their clinical details in the manuscript. A written consent was taken from the patient for sharing clinical details in the manuscript and publication of the same online in an open access journal.
CRediT Author Statement
The submission is based on our original work and had not been published elsewhere. The manuscript has been read and approved by all the authors. Author Shivangi Garg, Priyal, Dinesh Mohan Chaudhari, Anjali Mishra, Pushpendra Nath Renjen and Kamal Ahmad collected data, analyzed it, made the draft of the article and were directly involved in patient care. Each of the above mentioned authors proofread and validated the accuracy of data and were involved in analysis, and interpretation. All author read and validated the final draft.
Data Availability
Data was collected and made available for study based on strict interpersonal effort.
Use of Artificial Intelligence
No artificial intelligence was used by authors for the draft compilation. The author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.