
Abstract
Affordable access to medicines is a key determinant of a country’s resilience to health crises. The modern hyper-connected international trade and production networks have a vital role to play in ensuring this accessibility, especially in the context of a pandemic. This article focuses on medicines and medical equipment and analyses the synergistic role of the two international organisations—The World Trade Organisation (WTO) and The World Health Organisation (WHO), in assuring affordable access to these goods globally. WHO is responsible for global healthcare regulations; however, the medical supply chain originates in a few developed countries, manufactured in bulk (in case of medicine) at low cost in developing countries, and finally traded worldwide. Here, the role of WTO comes in where it facilitates global trade cooperation and intellectual property rights monitoring, both key elements in medical goods production and trading. Despite the need for cooperation in mitigating COVID-19, much of the global response to COVID-19 has been fragmented and inward-looking. This lack of coordination has serious repercussions especially for developing countries. We use qualitative content analysis methodology, connecting concepts of cooperation theory and global governance to identify the joint role of the two organisations in fostering global cooperation in medical goods accessibility.
Keywords
Introduction
The World Trade Organisation (WTO) and the World Health Organisation (WHO) can both be viewed as institutions of global governance because they are a part of the U.N. system. The present global pandemic has presented the unique situation in which both these institutions could play a crucial role in mitigating this crisis. By the end of October, 2021, about 246 million total cumulative cases of COVID-19 have been found while 4.9 million cumulative total deaths have been reported (WHO, 2021). Due to the highly infectious nature of the COVID-19 severe lockdown was imposed across countries as a precautionary measure which drastically reduced the economic activities around the globe. The WHO for the obvious reason that this crisis is a global crisis for public health, and the WTO because this crisis is also challenging for the global trading system, have a key role to play in ensuring the wide reach of affordable pharmaceutical products. Both these organisations’ role converges because the urgency of the smooth supply of medical items is one of the key necessities in times of a global health crisis, but in times of a crisis, this smooth supply is one of the first things that is likely to get hampered because many of these traded goods face a rise in protectionist measures as in times of previous crises. As such, the role these institutions play can be huge.
According to a pre-COVID publication of the WHO, two billion people around the world face challenges of access to essential medicines at an affordable price (Chan, 2017). Patented or proprietary medicines are expensive due to the high R&D cost that has been incurred by the originator on the innovation of new medicine (Dimasi et al., 2016). Patent holders enjoy exclusive rights over the drugs, hence restricting the manufacturing, selling and trade of their low-price generic versions. The people in least developed and developing countries suffer more from such restrictions. Apart from the vaccines now available, which are preventative, not prescriptive in nature, no exact medicine is available for prescription to cure COVID-19 but existing medicines judged suitable are being given to the infected person on a trial-and-error basis depending on the severity of the infection or seriousness of the patient’s condition. These perceived suitable medicines comprise both patented and generic medicines. The price of patented medicines or manufacturing and trade of generic version of patented medicine, both are affected by the presence of the TRIPS agreement, which makes the process of access to universal healthcare goals of the WHO more challenging. This article analyses the compliance of healthcare policies of these two international organisations, that is, WHO and WTO, while also taking into account the access to medicines in general in the post-COVID condition.
Literature Review
WHO, TRIPS and Access to Medicines
The problem of affordable medicine access worldwide has deteriorated since the signing of the TRIPS Agreement with the formation of WTO in 1995 (Arora & Chaturvedi, 2017). The number of new drugs might have increased, but these proprietary drugs are out of reach for common people, especially in developing countries, due to their high monopoly price. The patenting system increases the price of patented drugs particularly newly developed medicine or the medicines, which are being sold by a single firm (Duggan et al., 2016). Any price regulation or control over the patented drugs attracts delayed launch or no launch at all in the countries that impose regulations or controls (Cockburn et al., 2016). TRIPS agreement has indeed provided flexibilities to member countries to design their domestic patent law in such a manner that would promote easy access to medicines to its people. However, TRIPS flexibilities are not well defined and vague in interpretation.
This vagueness provides ample room to originator countries to interpret them in their own favour while developing and least developed countries have their own interpretation. This is the reason originator countries sign stricter IPR provisions along with narrow TRIPS flexibility under Free Trade Agreement (FTA) with the partner countries. Such FTA’s terms are devoted mainly to promote market exclusivity at the expense of competition and affordability, restricting the accessibility to cost-effective drugs. Additionally, through FTAs data exclusivity—a TRIPS-plus measure to protect IPR, effectively enforced preventing the entry of generics, affecting access to medicines in developing and least developed countries (Guennif & Lalitha, 2007).
Unfortunately, neither TRIPS nor WTO has any strong policy provision to safeguard the access to affordable medicines by restricting such FTA’s. In contrast, it has strong policy measures to limit generic drugs for manufacturing and selling if these activities deviate from the provisions of TRIPS or WTO’s rules for IPR protection. Originator drug manufacturers are even involved in the settlements through which these companies pay generic firms to settle patent litigation and delay entering the market (Carrier, 2017). Delay in the entry of generic drugs simply maintains the monopoly price of branded drugs in the absence of competition. In case a country attempts to control the monopoly price of proprietary drugs, it tends to discourage rapid product entry (Lanjouw, 2005). Contrary to this, the WHO itself assumes that the promotion and use of generic medicines will result in lower prices and thus increase access to drugs (WHO, 2015). Lack of access to medicines is one inequality that can be measured by the number of preventable deaths (Chan, 2017). In the case of ongoing pandemic where thousands of deaths have been reported every day, equitable access to medicines is a pressing concern. Gurgula and Lee (2021) emphasise that governments should utilise TRIPS flexibilities to ensure swift and equitable access to COVID-19 therapy. Similarly, McMahon (2020, p. 147) points out that for any sense of global normality to return, everyone globally must have affordable access to future effective COVID-19 vaccines and diagnostics as soon as possible and suggests reconsidering the level of control which patent holders have over essential health technologies. Krikorian and Torreele (2021) claim that availability and access to COVID-19 vaccines has remained highly inequitable, in part because companies insist on retaining their monopolies and refuse to share technologies; further the COVID-19 crisis has added to the growing understanding that the scarcity of many essential medicines, vaccines and raw material is not inevitable but rather the consequences of policies and decisions by the industry and governments.
Theoretical Background on Cooperation
Lack of cooperation, as Busby (2020) points out, is puzzling because global health has been previously more amenable to cooperation as compared to other areas, whether it is the U.S.–Soviet Union cooperation on smallpox eradication or the more recent U.S.–China collaboration on Ebola. Barrett (2007) has also pointed out efforts like smallpox eradication, which required a modest amount of money, also almost failed because of the tendency of countries to diminish the costs and burden of cooperation for themselves, despite it being in their interest to cooperate. These concerns were echoed by Krasner (1991) and Greico (1988) that these international distributional conflicts act as impediments to cooperation. Oye (1986), in his application of elementary game theory to international cooperation, has explained that if there is a strong incentive to cooperate, but actors refuse to do so, the situation resembles a deadlock. In case of a public health crisis the cost of inaction or the inability to find means to cooperate, can have serious consequences. This is a situation in which a (global) public good is involved, and where there are public goods, the issue of free riding arises.
This leads to the classic problem of under-provisioning of public goods as research on collective action has identified. This also has links with hegemony, as often when the world has had a hegemonic power at its peak or in rise, the hegemon itself takes the lead on its own (provided it is a ‘benign’ hegemon and not a ‘coercive’ one), according to the Hegemonic Stability Theory (Kindleberger, 1986). This has built on Olson’s (1965) analysis of how privileged groups dominated by one actor can overcome the collective action problem. For example—the United States played an important role in combating the HIV-AIDS pandemic through programs like President’s Emergency Plan for AIDS Relief (PEPFAR), and through its support for the multilateral Global Fund to Fight AIDS, Tuberculosis and Malaria. Around $90 billion in funds have been relegated to HIV-AIDS efforts over the past two decades.
The present political reality, however, is that of the hegemonic decline of the United States, with cooperation efforts further undermined due to the unilateralist trade policy that has been the defining feature of the Trump presidency. It is important to note, however, that later research has shown the possibility of cooperation even in the absence of a dominant/hegemonic actor (Keohane, 1986) and also through the development of the framework of non-cooperative game theory showing the possibility of cooperation even in seemingly the most discouraging circumstances. The Folk Theorem has generalised the outcomes of these researches by indicating a possibility of cooperation in any recurring situation where there are joint gains to be made from cooperation. The keyword here is recurring. Reciprocity becomes possible when situations recur, and hence actions can have implications on a states’ international reputation (Keohane, 1986). A defector is likely to lose trust of even third-party actors and not just the one they defected from.
Kreps (1990) explains that for establishing a reputation to support cooperation, defection or cooperation must be observable. If not observable, then there needs to exist institutions that facilitate transparency by being a repository of accessible information on the actions of the actors involved. This is why institutions play a role or have the potential to play a role. They have even been defined along the lines of ‘organizational forms that enhance monitoring and information transmission’. As already discussed previously, the role that institutions like the WTO and WHO have played has been significant, in certain circumstances and vastly ineffective in others. The framework they provide, however, can play a vital role in creating circumstances where cooperation becomes possible.
Gaps in Global Governance, Institutional Funding and the Path Ahead
The Oxford Handbook on the World Trade Organisation (Narlikar et al., 2012) identifies four sets of ‘structural/contextual’ factors that cut across research paradigms in international relations: interests, institutions, ideas and information, when it comes to explaining the existence and continuity of a deadlock. In a similar vein, Weiss (2016) identifies five global governance gaps—knowledge, norms, policies, institutions and compliance.
Knowledge, because disputes/lack of consensus over knowledge, that is, what the issues are, has a direct connection to clashes over policy formulation approaches like top-down versus bottom-up, development assistance versus self-sufficiency and debt-relief versus accountability.
Norms, because consensus on universally accepted norms is not easy to come by.
Policy is the codification of these norms.
Institutions that provide a structure within which these policies are housed. Few global institutions have overarching authority over individual member states. International organisations, even the most powerful bodies, such as the U.N Security Council do not have resources or authority commensurate with the size of the trans-border problems that are expected to address. And finally,
Compliance has always been a governance gap, owing to the lack of global institutions to effectively enforce accountability.
The reason behind using this framework of gaps is to allow a conceptualisation of the essential tasks for the pursuit of more order, stability, predictability and prosperity along with distributional justice among countries. On top of this, new gaps are also constantly arising and thus are rarely ever likely to get filled up completely, so the process is dynamic. Furthermore, to understand the impact of these sets of factors and use them to anticipate potential deadlocks, the mitigating impact of actors’ behavioural choices needs to be taken into account.
The application of the concept of polycentricity in governance also indicates an alternative way of envisioning global cooperation. The term polycentric governance connotes a complex form of governance with multiple centres of decision making, each of which operates with some degree of autonomy (Carlisle & Gruby, 2019). It has been widely researched specially since Ostrom’s (1990) influential contribution to commons theory, which formulated eight institutional design principles that she found to be associated with institutions robust enough to maintain common- pool resources.
Methodology
To study the policies of WHO and WTO and to identify the obstacles, we have collected relevant literatures by these two global organisations. For information and news on medicine access in context of the pandemic we have collected the information from various known websites by using key terms. The key terms that were used, in combination with one another to search relevant information are—access, medicines, coronavirus pandemic, COVID-19, WHO, WTO, TRIPS, Doha, patent, health policy, trade policy, price, international cooperation, etc., along with the terms supportive to these terms. Information, reports, publications and other documents were also collected from WHO. All the collected contents have been classified into four categories such as institutional documents, research articles, online news content, and other supportive online content. A comprehensive study of the final grouped content was done to construct the description of the analysis.
WHO–WTO Policy Compatibility: Background on the Institutional and Legal Framework
In 2005, WHO published International Health Regulations (IHR, 2005), which laid down the principles that have to be followed in a health emergency or in the case of the spread of a potential infectious disease in any member state. As per the principles of IHR, the implementation of the regulations shall be with full respect for the dignity, human rights and fundamental freedoms of persons (Article 3.1) and the implementation of these regulations shall be guided by the goal of their universal application for the protection of all people of the world from the international spread of disease (Article 3.3). Being accountable to that end, the WHO issues guidelines related to health concerns to member states, constitutes a team of health experts, and with the help of its associate organisations assists members states to procure affordable medicines and medical devices.
However, WHO can only influence the demand side mechanism of the medicines or medical devices, the supply side mechanisms are influenced by WTO through its TRIPS arrangement. The principle of TRIPS agreement allows member countries to adopt necessary measures to protect public health and nutrition (Article 8.1). However, members may take appropriate measures to prevent the abuse of intellectual property rights by rights holders or to resort to practices which unreasonably restrain trade or adversely affect the international transfer of technology subject to provisions of this agreement (Article 8.2). Article 28(a and b) of the agreement prevents third parties not having the owner’s consent from making, using, offering for sale, selling or importing for these purposes that product whether patented under product or process.
Such conditions provide the product under patent the strongest protection and such protection results in a monopoly price of medicines or medical devices and restricts the entry of a generic version of it or parallel imports of the same in the market. TRIPS provide limited flexibilities subject to its provisions hence, the access to medicines needs special attention while implementation of agreement. Public health requires that healthcare and healthcare products need to be treated differently from other products (Hoen, 2017). The provision of compulsory licencing provided under TRIPS even requires that ‘adequate remuneration’ (Article 31h) has to be paid to the patent holder, which has the potential to make the medicines expensive, manufactured under a compulsory licence. Similarly, the agreement stipulates (Article 31f) that if the law of a member country allows for other use (other than that allowed under Article 30 of this agreement) of the subject matter of a patent without the authorisation of the right holder, such use shall be authorised predominantly for the supply of the domestic market only. This provision indeed neutralises the potential benefit of the TRIPS agreement’s flexibilities because the least developed countries and most of the developing countries have no infrastructure and technical know-how to manufacture the medicines on their own (WHO, 2011). In such a situation, the only option left with these countries is to either be deprived of these medicines, or pay a high price for the same or wait untill the patent expires.
As Pegram (2020) has explained, despite predictions of epidemics as early as 2007, wealthy member countries have been averse to redistributive policies/demands by developing countries. The independence, power, resources given to the WHO have not been adequate. The large wealthy economies have also tended to prioritise health sector loans, with strings attached, through the World Bank (bringing a large number of investments and capital inflow to the financial market). ‘Strings attached’ means the lenders are the ones controlling the terms on which these loans are approved, and the primary interest is thus their financial gain and not necessarily genuine assistance to the health infrastructure of developing or least-developed countries.
After signing the TRIPS agreement in 1995, developing countries realised that Article 31(f) of the TRIPS agreement might be detrimental to their interest by not allowing export–import of the drugs produced under compulsory license. Considering the severity of the provision, developing and least developed countries raised their voice in WTO’s fourth ministerial conference in Doha, Qatar, in 2001 (Doha Declarations, 2001). The Doha round (WTO, 2020) came up with a declaration on the TRIPS Agreement and Public Health on 14th November 2001. Para. (4) of the declaration states that the TRIPS Agreement does not and should not prevent members from taking measures to protect public health and the agreement can and should be interpreted and implemented in a manner supportive of the WTO members right to protect public health and promote access to medicines for all. Most importantly, Para. (6) of the declaration states that WTO members with insufficient or no manufacturing capacities in the pharmaceutical sector could face difficulties in making effective use of compulsory licencing under the TRIPS agreement. Therefore, the TRIPS council was instructed to find an expeditious solution to this problem and report to the general council before the end of 2002 (WTO, 2002).
Finally, the decision on 30th August 2003 for Para. 6 of the Doha declaration waived the restriction on compulsory licence for domestic use only and allowed import and export of the generic version of the patented medicines manufactured under compulsory licence subject to certain conditions (Correa, 2004). However, the 2003 decision did not waive Article 31(b) of TRIPS, which requires that applicant for a compulsory licence, prior to such use should have made efforts to obtain authorisation from the right holder on reasonable terms and conditions and within a reasonable time. This condition is sufficient to delay the timely launch of the generic versions of patented medicines. However, the same article allows the member country to waive this requirement in case of national emergency or other circumstances of extreme urgency or in case of public non-commercial use.
Despite this, in the case of the ongoing COVID-19 pandemic, which satisfied the condition of Article 31(b) of the TRIPS agreement, none of the Member countries have issued compulsory licence utilising the flexibilities provided in the TRIPS agreement or Declaration of Doha ministerial conference or decision of 30th August 2003 on Para. 6 of Doha declaration. This non-issuance of compulsory licencing has resulted in higher prices for brand name generic medicines. For example, the patent holder of Remdesivir (an antiviral drug being prescribed to serious COVID-19 patients) has granted a non-exclusive licence to many generic drugs manufactures in India and other countries to manufacture and sell the generic version of Remdesivir. However, the price of brand name generic of Remdesivir seems higher than what it could have been, had it been produced under compulsory licencing or under emergency use provision of the TRIPS agreement. Under voluntary licence, the licensee has to pay a royalty for the patented subject matter they use. This royalty finally added up to the cost of medicines by the manufacturer and thus medicines become expensive to the end consumer, which is the ultimate concern for the patient in general.
The 30th August 2003 decision might have made it seem as though the final barriers to the access to affordable, high-quality medicines had been removed. Still, the disputes that have since been raised at the WTO’s dispute settlement body related to pharmaceutical exports exposed the complexities ingrained in the international agreements and relations and access is still not as easy in practice as it might seem in policy. Certain incidents depict this policy and implementation gap. For example, a shipment of the generic drug (Losartan Potassium) produced in India and destined to Brazil was seized in transit at Schipol Airport, in the Netherlands, in December 2008, based on complaints of suspected infringement by alleged owners of patents (WTO, 2008). The reason for the seizure was justified by the Netherlands on the ground of border regulation as the drugs were in transit through the European Union territory. However, the regulations in their current form are not adequately resolving the risk of interception in Europe, of medicines lawfully manufactured and exported from India and destined for lawful import in a non-European country (Baker, 2012). These gaps in policy and practice lead to an environment of uncertainty. To prevent the harmful effects caused by such an atmosphere, the need for transparency in the current scenario of COVID-19 pandemic becomes even more urgent. To facilitate the smooth flow of medicines and medical devices, there needs to be a commitment to notify the WTO of any trade-related emergency measures designed to tackle COVID-19. The WTO has long played a role in improving transparency regarding trade-related restrictions by creating a notifications system. It may not be an ideal system, but it does provide an established, pre-existing platform for countries to inform other countries of any restrictions they have imposed. This platform of trade policy monitoring needs to be put to use. It can minimise the impact of uncertainty and prevent governments from indulging in guess-work about each other’s trade policy.
Drug Candidates for COVID-19
Until 31st March 2020, WHO had not recommended any medicines because it did not find any safe and effective medicines for the treatment of COVID-19. However, several existing medicines were suggested as potential investigational therapies. In many countries, doctors were prescribing medicines to COVID-19 patients that have not been approved for this disease, which is also considered as off-label use. Off-label use of medicines is the use of licensed medicines for indications that have not been approved by a national medicines’ regulatory authority.
The prescription of medicines for off-label use by doctors may be subject to national laws and regulations (WHO, 2020a). However, the WHO is closely monitoring the drug candidates that are being prescribed to COVID patients in different countries A number of medicines have been suggested as potential investigational therapies, many of which are under clinical trials. Besides this, many countries in their prevailing capacity are conducting clinical trials on potential drugs candidates, which might be effective in treating COVID-19. The foremost drug shown efficacy in the treatment of COVID-19 is Remdesivir an antiviral drug prescribed for HIV and other indications. Remdesivir is proprietary medicine of Gilead Science, which has licenced generic manufacturer like Cipla, Dr Reddy’s to manufacture and sell. Since the drug patent has been voluntarily licenced on a commercial term, the resulting generic version of it is being sold at a high price. Other repurposed proprietary drugs for COVID-19 are Tocilizumab, Itplizumab and Azithromycin. Although all these patented drugs were developed for other therapeutic indications however, since it has shown some positive effect on the hospitalised COVID-19 patient, medical experts were suggesting these drugs to only severe cases. For example, Tocilizumab is suggested for severely infected COVID-19 patient, unfortunately, its short supply compels relatives of the critical COVID-19 patient to run from pillar to post to get required doses of the drugs even at multiple times higher price compared to its print rate (Bloomberg Quint, 2020). Drug prices rose as India found itself in the deadly second wave of the pandemic in 2021. According to a Business Standard, report in the first half of 2021 key COVID-19 related drugs saw a 180 per cent price rise over the course of a four-month period (Das, 2021). As of October 2021, API’s (Active Pharmaceutical Ingredients) and other raw materials (mostly imported from China) used in drug manufacturing are seeing a steep price rise (Kumari et al., 2021). This has severely impacted small and medium scale manufacturing units, which in turn could lead to shortages of essential medicines. Even non-COVID specific medicines and commonly used drugs, for example, Paracetamol has seen a general price rise owing to the rise in price of raw materials and APIs (Sharma, 2021).
Along with these expensive patented drugs, few off-patented drugs were also on the list of drugs being prescribed to COVID-19 patients in combination with other drugs based on severity of the infection. Such off-patented drugs are Favipiravir, Lopinavir/Ritonavir, Oseltamivir, Ivermectin, Methylprednisolone and Dexamethasone. Most of these off-patented or generic drugs are usually affordable and easily available in India but this might not be the same case in other developing or least developed countries. One of the reasons might be the lack of transfer of technology required (Article 8.2 of TRIPS) for the manufacturing of drugs as was revealed by the advocacy group of the strong patent regime which opines that strong patent regime promotes innovation and transfer of technology. The Indian pharmaceutical industry has acquired expertise in reverse-engineering, thus, for the Indian generic manufacturer the task of manufacturing generic versions of off-patented drugs is not difficult. However, countries that neither have expertise in reverse-engineering nor the access to technology, cannot manufacture off-patented drugs even when they have other required resources.
Access to Protective Equipment
The demand for protective equipment had risen rapidly in a short time period. Unfortunately, the protective equipment industry was neither ready nor had capacity to supply bulk equipment and devices on short notice so the WHO had to urge industry and governments to increase manufacturing by 40 per cent to meet rising global demand (WHO, 2020b). This was particularly relevant during the initial days of the pandemic and over time the supply adapted to the new demand as far as protective equipment like masks and PPE kits are concerned.
Interestingly, China controlled the spread of disease in just a couple of months following the outbreak, allowed its factories to work on full capacity and started supplying this equipment to the world. However, as consignments reached the destination country, it was found that the equipment were substandard, defective or faulty and hence many countries returned the products to China. Such incidence necessitates the WTO and the WHO to formulate a common minimum level of standard for medicines and medical devices including equipment.
Trade Policy and Medical Goods
Protectionism
Given that medical equipment and pharmaceuticals are limited in supply and in high demand at the moment and were more so during the initial months of the outbreak because of the lack of preparedness, countries sought competitive protectionist measures by locking down supplies for themselves rather than explore a more open and inclusive option. Bradley (2020) has reported that developing countries in Africa and Latin America were facing a shortage because the developed countries were overstocking up and outbidding the poorer nations. International assistance through USAID had also been halted and put under review. An extreme example of the zero-sum, exclusionary reaction is the attempt made by the Trump administration to get German scientists to relocate and deliver a vaccine exclusively to the United States. This international inequity in access to pharmaceuticals and medical supplies is not new and was also seen during the H1N1 outbreak of 2009.
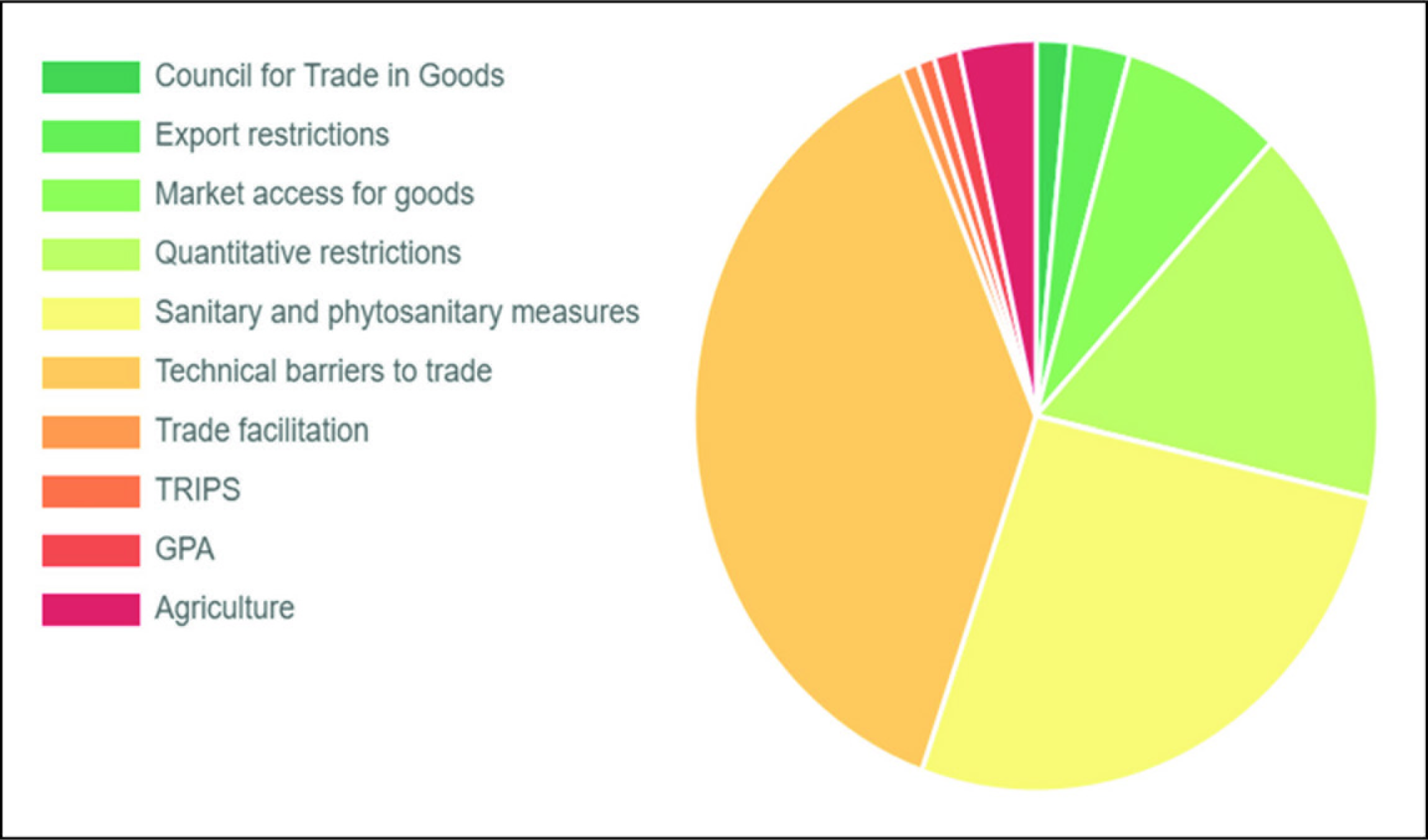
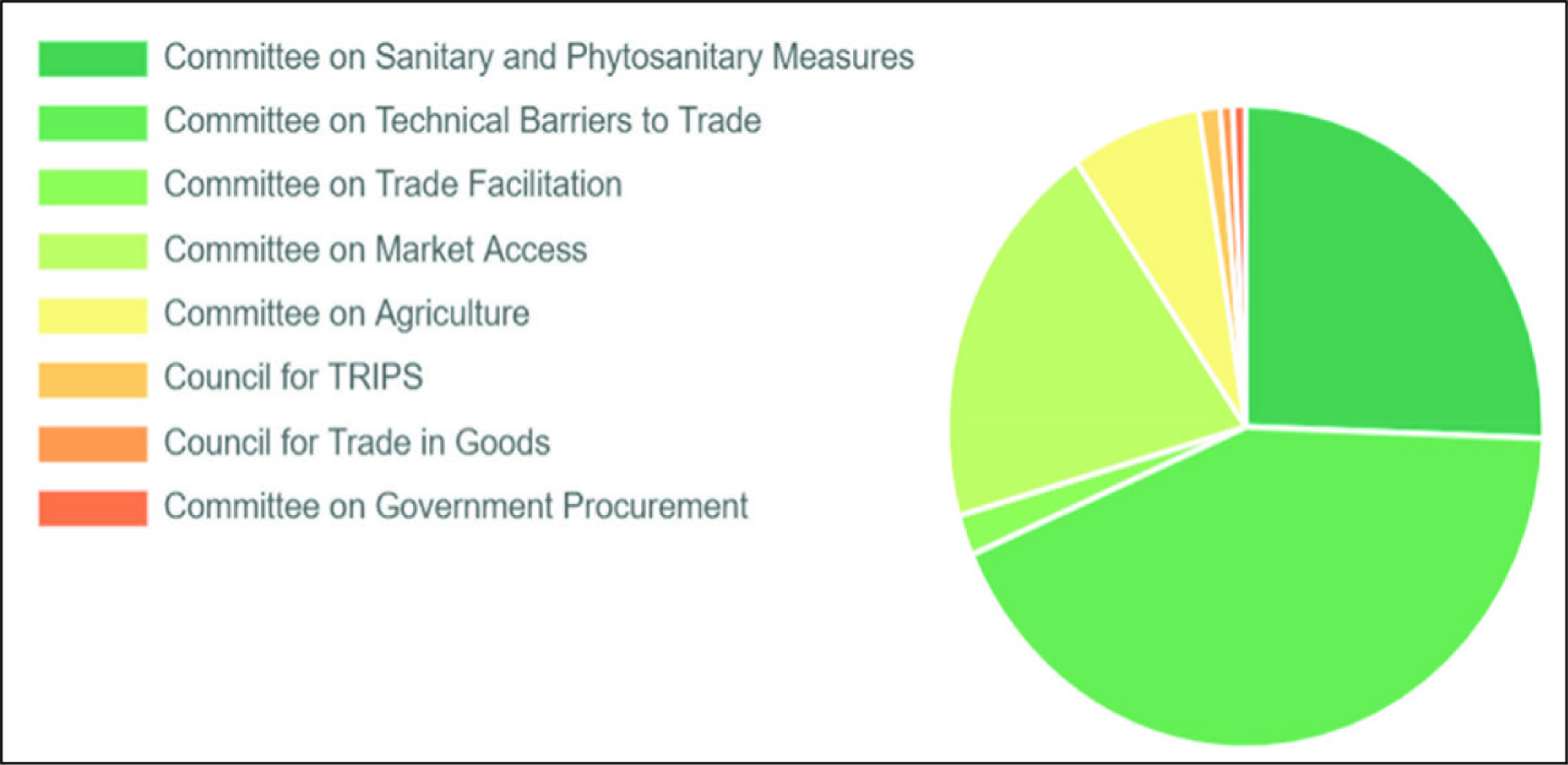
The response to the pandemic has been a fragmented one, that is, nation-specific solutions have mostly been adopted. Moreover, economic nationalism is on the rise, along with antitrade localism under the pretext of reducing dependency on other countries. Both United States and European Union imposed trade restrictions. The United States, the biggest source of funding for the WHO sought to halt this funding and accordingly cuts have been proposed. Production-wise, China has fast increased supply to other countries while coming under scrutiny for supplying defective equipment. While China clamped down on manufacturers it brought to attention the necessity of international standards and product quality assessments. The absense of coordination on technical NTMs like SPS, TBT and pre-shipment inspection, opens up room for fraudulent trade practices. Figures 1 and 2 clearly show how large a part SPS and TBT measures occupy in COVID-19 related trade policy measures notified to the WTO. Apart from these measures, quantitative restrictions and market access measures are among the next most common category of notifications on COVID-19 to the WTO. Conversely, lack of coordination, and lack of transparency go hand in hand, which can lead to a lack of trust among trading partners, fear-mongering, and a rise in hostility towards certain nationalities. The top notifying countries are a pretty varied group, with the United States and European Union at No. 3 and No. 5 positions respectively, in a list comprising mostly of Asian and Latin American developing countries, with Brazil taking the top spot by a long margin.
Stellinger et al. (2020) pointed out that along with necessary measures, unnecessary measures have also been used, such as import bans, licensing requirements, and ‘buy-national’ procurement conditions—that protect domestic industry rather than the patients on whom those goods would ultimately be used. Some countries have also been imposing high tariffs on medical devices, medicines, disinfectants and soap long before the pandemic started. Moreover, in addition to import tariffs, there have also been exporting bans on medical essentials and even food exports. Though it is worth to point out that as early as April 2020, 77 countries had also reduced trade barriers (mostly tariffs) on medical goods.
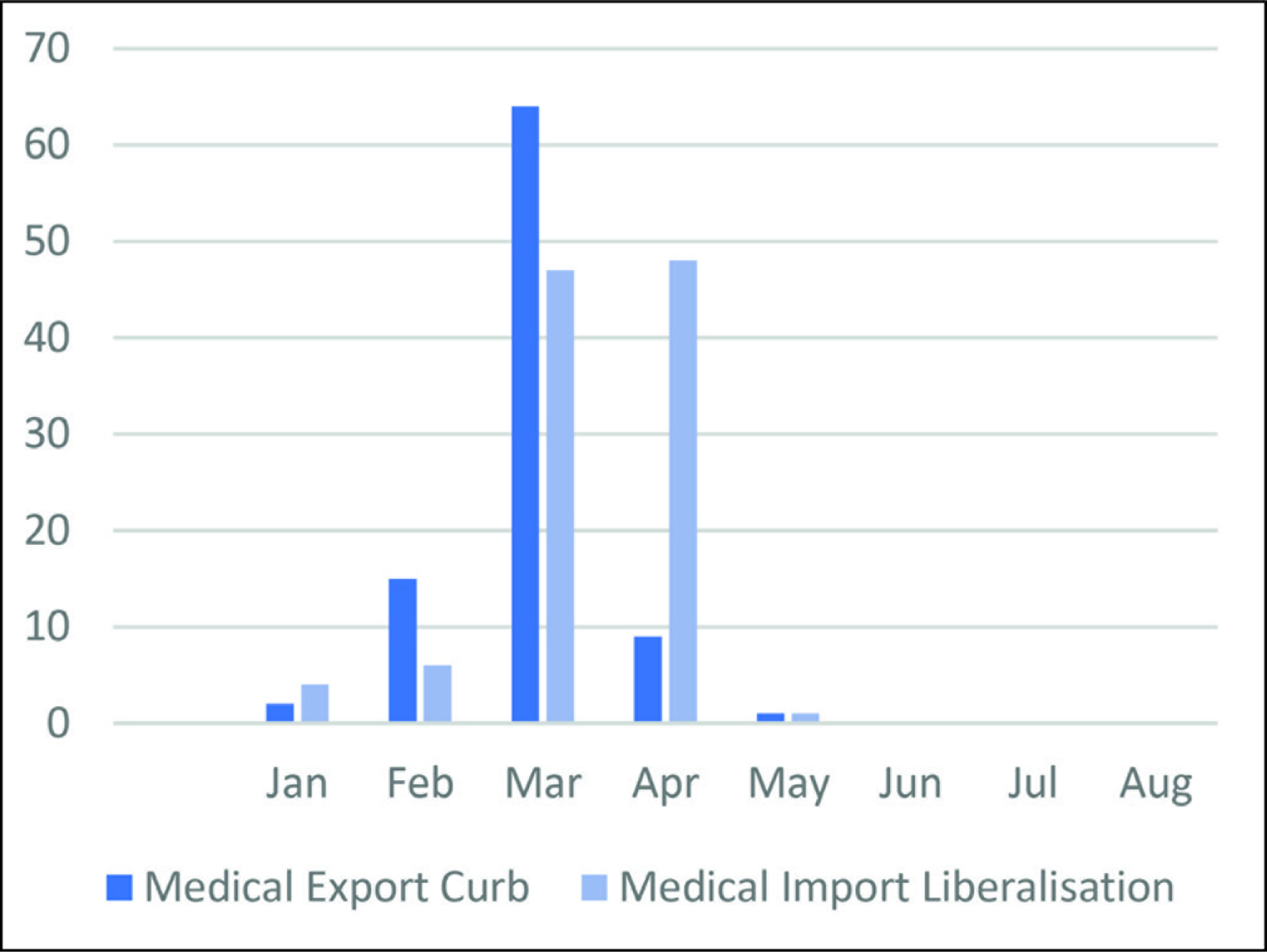
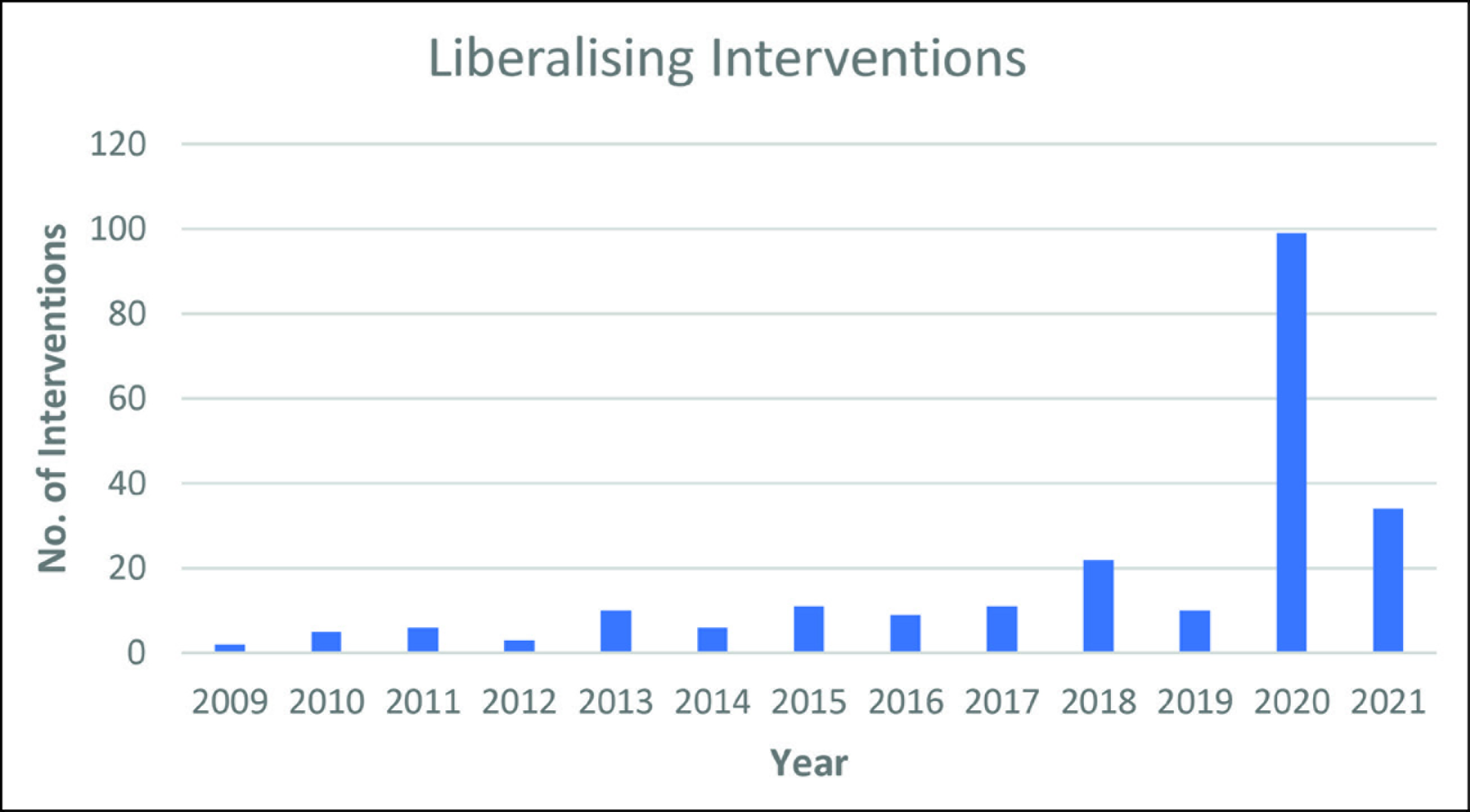
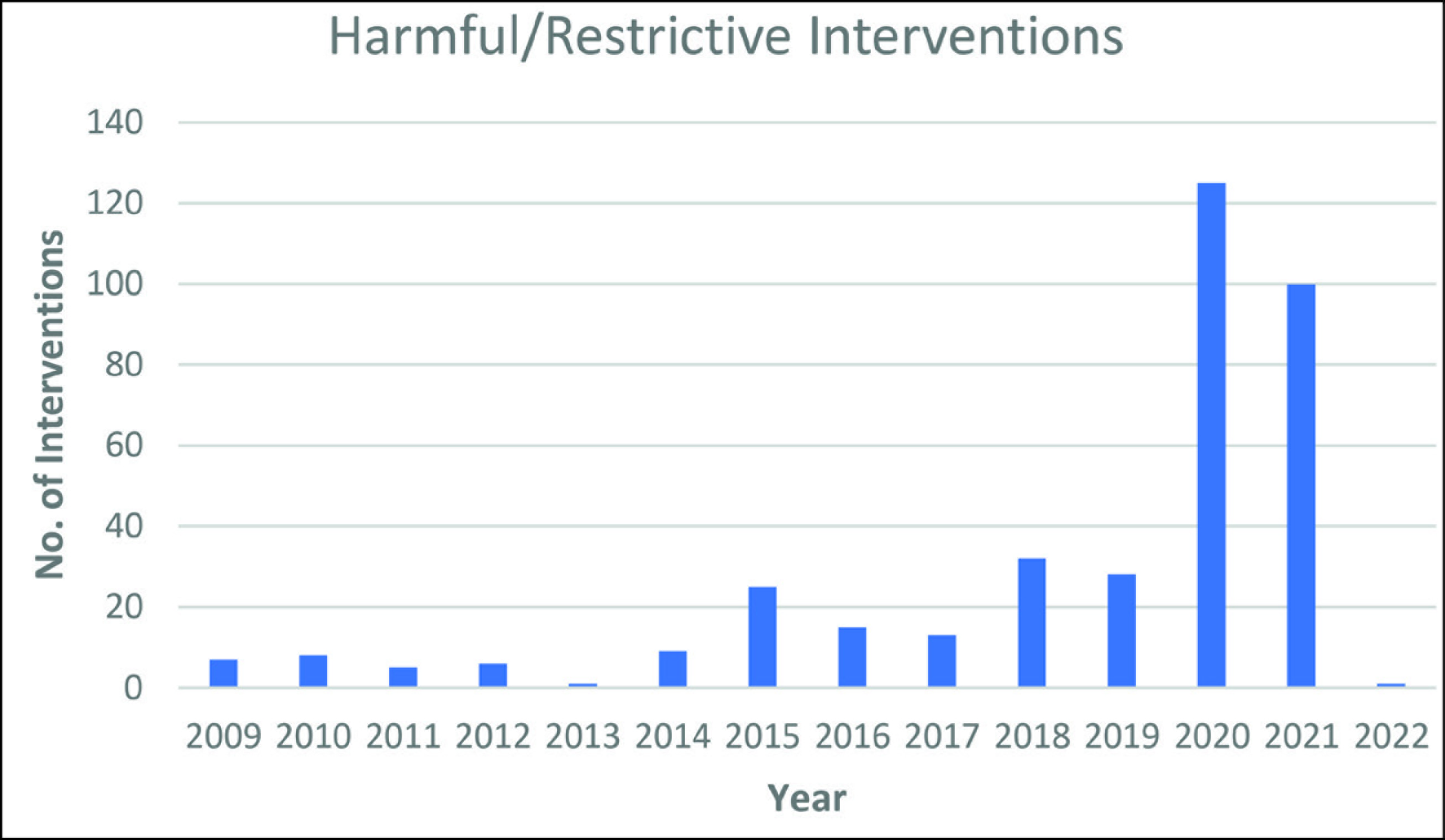
This can be seen in Table 1 and Figure 3, which show both export curbs and import liberalisation measures for essentials, in aggregate and monthly form, respectively. As it can be seen—the early months of the pandemic saw the immediate application of curbs followed immediately by import liberalisation measures in medical goods. It is to be noted here that while the import liberalisation measures can be seen as a step in the right direction not to let the scenario of scarcity arise, the primary purpose it served was to ensure that the domestic supply did not suffer because they were followed by export restrictions as well. Though the restrictions especially in medical goods were confined to the month of March, they appear to have already been on an upward trajectory since February as the outbreak had started moving beyond China to the rest of the world during that time. Figures 4 and 5 show a steep rise in both restrictive and liberalising policy measures in the pharmaceutical sector in 2020, and while 2021 has seen marginally lesser restrictive measures, they continue to be much higher in number than in the pre-COVID times and comparable to 2020. In contrast 2020 saw a large number of liberalising interventions, which have now drastically gone down, indicating the temporary nature of the liberalising measures. So restrictions continue to be imposed on countries while liberalisations have died down.
Initial Trade Policy Measures on Medical Goods between January–August 2020

Firm-level case studies discussed in Fiorini et al. (2020) have illustrated how the use of export restrictions to facilitate domestic supplies of essential goods might seem logical and justifiable but have unintended consequences in the form of reducing access to critical supplies, increase average prices, increase market volatility and distort investment decisions. It also ultimately reduces trust among the countries. Hoekman et al. (2020) have pointed out that governments have attempted to use trade policy instruments to maximise the domestic supply of essential goods, but this has been done without accounting for the actual effectiveness of the measures as second-order incentive effects or spillovers created in the affected markets have not been taken into consideration.
Interdependence versus Self-Reliance in Medical Goods Supply
Conversations have started taking place about the high amount of dependency that most countries have with their key trading partners and countries dominating the global supply chain—particularly China, and how more self-reliance is necessary.
This line of thought ignores the fact that a global supply chain diversifies the supply of goods and spreads out the risk among multiple countries, thereby reducing the chance of a complete shutdown if something happens in one particular production unit or even region. Localised or concentrated production activity is far more susceptible to such risks. Miroudot (2020), drawing from risk-management literature, has warned against equating self-sufficiency with robustness—‘Firms that have diversified suppliers and a production network across different countries can adjust their production when a disaster occurs in one place’. A fully localised production network is detrimental to robustness (the ability of a unit/system to function in times of a crisis). Javorcik (2020) explains that it was the stability of the trading rules that emerged over years of world trade liberalisation and cooperation (where the GATT/WTO had a significant role to play), which encouraged producers to set up production networks spanning the globe.
Summary
There exists an unevenness in power relations between the countries of the world and the COVID-19 crisis is likely to perpetuate and sharpen this global inequality further because, despite a pandemic being a collective struggle, it has emerged in ‘a context of governance fragmentation and acute inequality’ (Blanco & Rosales, 2020). Moreover, an uneven power structure has always been present in the system of global governance, where some states are far more capable actors than other states and non-state actors. This unevenness makes some states better equipped to handle such crises, while putting other less developed states in a far more vulnerable position with regards to both health and economic repercussions of the crisis.
Indeed, both WHO and WTO have differing set of goals, principles, objectives and responsibility, however interest of both the organisations coincide with the issues related to access to medicines where WHO represents the demand side of provision of medicines while the WTO represents the supply side of medicines. To this end both each organisation follows its own set of policies. Our analysis found that there are differences in the policy orientation of these two organisations, which hampers the WHO to achieve its stated goal of universal access to medicines and to contain the frequent occurrence of pandemics that the world has been dealing with, such as SARS, MERS, Ebola and at present COVID-19, which requires access to affordable medicines and medical devices in bulk amount and on urgent basis.
Conclusion
The issue of access to affordable medicines is not a new one. The problem existed which is why the WHO was established. However, the issue of access to medicines continues to exist today even after more than seven decades of the formation of WHO. The prominent reasons causing the issue are institutions external to the WHO’s system of healthcare arrangement and the most notable such institution is the WTO and its agreements that govern international trade, including the trade in medicines and medical devices.
Since both the international organisations have a different set of interest groups and goals, they follow different policies to achieve those goals. The policies of WHO and WTO must be in the same direction to achieve the goal of universal access to affordable medicines. This necessitates the WTO to align it policies with the policies of WHO for access to medicines. The issue of access to medicines can be minimised or eliminated if the WHO’s policy on access to medicines is complied to by WTO policy on trade and IPR for medicines and medical devices. Resolution of this issue has the potential to improve healthcare access and save lives of millions of people worldwide. This is not just about these two organisations but also about the general structure of the system of global governance that exists and the seeming lack of alignment and fragmentation of their goals. There also exists a mismatch between their purported objectives and the authority and resources these organisations actually have versus the ones they need to successfully achieve those objectives.
The limits of global governance without global government have to be accepted but the numerous gaps that exist do need to be plugged in better ways to address key problems confronting the world, case in point, the present pandemic. Weiss (2016) has stressed that for global governance to be effective does not mean creation of an exclusive policy jurisdiction but an optimal partnership among the actors involved. In essence, creating a scenario conducive to coordinated responses to global crises. Applying the interdisciplinary lessons from international economics and International Cooperation Theory (ICT) has valuable learnings in reforming the global health and global trade governance system so that these institutions can be effectual in mitigating global crises.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Mrityunjay Kumar is an Institute Fellow at Indian Institute of Technology, Patna, funded by the Ministry of Education, Government of India.
Ayesha Fatma is a Senior Research Fellow funded by the University Grants Commission (UGC), Government of India. ID- 3764/(NET-DEC2015).