
Abstract
This study aims to document the cultural significance of vertical birthing positions and knowledge of easing complicated deliveries among the Porja hilly tribal group, Visakhapatnam district, Andhra Pradesh, India. With the purposive sampling method, 31 postpartum mothers were selected on the inclusion criteria of having been given childbirth in the last six months. The socio-demographic profile of the respondents was presented to understand the socio-cultural living conditions. The qualitative data collection involved 31 face-to-face in-depth interviews with postpartum women and two focus group discussions involving six to eight traditional birth attendants (TBAs) on the cultural efficacy of upright positions. Handwritten transcripts of the interviews and conversations were transcribed and coded into themes and categories. Qualitative themes reveal that the pregnant women with anaemia and morbidity conditions had been exposed to maternal distress and foetal distress (breathing problems and loss of consciousness) but had managed by adopting immediate alternative vertical birthing positions with the suggestion of TBAs. The findings suggest that vertical birth positions are age-old childbirth customs which have been adopted as as a priority option by labouring women, especially in socio-economically disadvantaged societies where medical facilities are unavailable.
Keywords
Introduction
Homebirths and vertical birthing positions are considered the oldest forms of childbirth practices adopted in many corners of the world, where childbirth occurs in non-medical facilities. 1 This combination remains, widely used in least developed and developing countries including India, especially where homebirths are a traditional practices, particularly among the tribal societies.2, 3 Here, it may be noted that tribes in India constitute 8.6% to the Indian national population. 4 Childbirth is an inherently cultural event. Maternal and neonatal care practices are deeply rooted in socio-cultural beliefs among tribes. 5 Homebirths with vertical birthing positions (squatting and half-squatting positions) under the supervision of traditional birth attendants (TBAs) are age-old traditional practices executed to ease complicated labours and in the absence of modern medical facilities.6, 7
A chain of Cochrane review studies and international health agendas suggest that giving birth in an upright position can benefit the mother and baby for several physiological reasons. 8 Upright birth positions have the capacity to reduce the risk of compressing the mother’s aorta, which means there is a better oxygen supply to the baby, which helps the uterus contract more strongly and efficiently. As a result it helps the baby get in a better position.9–11 At the international level, the World Health Organization (WHO) promotes encouraging women to take comfortable positions, allowing movement during labour, stimulation of upright positions in childbirth, and a restrictive practice of episiotomy which stand out among the ‘Good Care Practices for Labour/Delivery and Childbirth’. 12 Even the tribal women often give homebirths in upright positions like standing, squatting or kneeling by holding a sari dropped from the roof under the supervision of trained or cultural birth attendants.13, 14 However, the reproductive health indices of tribal communities are typically poor with a maternal mortality of 230 per 100,000 live births (double of National MMR) and 62% of the tribal women suffer from at least one gynaecologic morbidity.15, 16 It is important to understand regarding the role of homebirths or upright birth positions or maternal morbidities as towards tribal maternal and neonatal morbidity or mortality in India. 17
This context requires focused investigation by detail analysis of the documents around the tribal childbirth practices in India. This study, therefore, aims to explore with the objectives of describing the child birthing positions and, existing cultural ways of dealing with obstetric danger signs, and inherently developed sustainable coping strategies to avoid maternal mortality by tribal women-namely Porja, one of the Particularly Vulnerable Tribal Groups (PVTGs) living in hilly regions of Visakhapatnam district, Andhra Pradesh, India.
Materials and Methods
Study Design
This study was a community based-qualitative observational study among the Porja tribal community conducted between the period February 2022 to August 2022 in the 10 hilly tribal study villages situated in Munchingiputtu mandal, Visakhapatnam, Andhra Pradesh, India (Figure 1). The tribal villages were inhabited by the Porja tribal population—A Particularly Vulnerable Tribal Group (PVTGs) in India. The Government of India recognized PVTGs, based on the pre-agricultural level of the economy, extremely low literacy rate (35%), stagnant population growth, and having their own dialect are the characteristics for their vulnerability status.18, 19
India Map Showing the Study Area Located in the Eastern Ghats of Andhra Pradesh, India.
Study Sample
With the purposive sampling method, 31 postpartum mothers were selected with the inclusion criteria of recently delivered at-home childbirths.
Data Collection
We undertook participant observations, face-to-face in-depth interviews (IDIs) involving 31 postpartum women and two focus group discussions (FGDs) with six to eight TBAs to document the practices around vertical birth positions. Tool like semi-structured household survey and interview schedules were employed to document the socio-demographic profile, maternal morbidities and the childbirth vulnerabilities faced by the postpartum women. Each IDI lasted 30–55 minutes and FGD for 1 hour 40 minutes.
Data Analysis
Qualitative data Extraction
Handwritten transcripts of the interviews and conversations were transcribed and coded into themes and categories. The data was analysed with a thematic approach. 20 All the field observations, informal information, IDIs and FGDs were construed and categorized into units of meaningful codes. Open coding was undertaken by hand where data coding was undertaken by repeated reading of the written text in interview schedules. The codes were listed, sorted, categorized to systematize the various aspects and properties of each main code. This approach led to develop two themes and six sub-themes. Description of the characteristics of the study population was undertaken to assess respondents’ basic socio-demographic profile. Results were presented in the form of tables along with their summary descriptions.
Results
Table 1 represents the characteristics of the interviewed participants. Of the 54 deliveries during the study-specific period, 57.4% (31 mothers) had home deliveries with the help of untrained TBAs. Home deliveries were highly resorted by illiterates (54.8%) than literates (45.2%) due to the cultural belief that medical intervention is not required (29.0%) and at the insistence of family member for adhering only to traditional customs (25.8%). The age at the marriage of all the home-delivered mothers was within the late adolescence period (16–19 years of age). The home-delivered mothers were observed to be farmers by occupation in their own agricultural lands (producing rice, ragi, turmeric, pepper, coffee and also own livestock). Nearly half of the mothers (48.4% includes 12 primi and 3 multigravida) belonged to the adolescent age group. Substance use is commonly found during pregnancy among the tribes. 11 In the study-specific period, 38.7% of postpartum women had a habit of drinking liquors followed by 22.6% chewing different tobacco products and liquors; 9.7% had the habit of chewing tobacco products, and 6.5% had smoked during their pregnancy period.
Characteristics of Interview Participants.
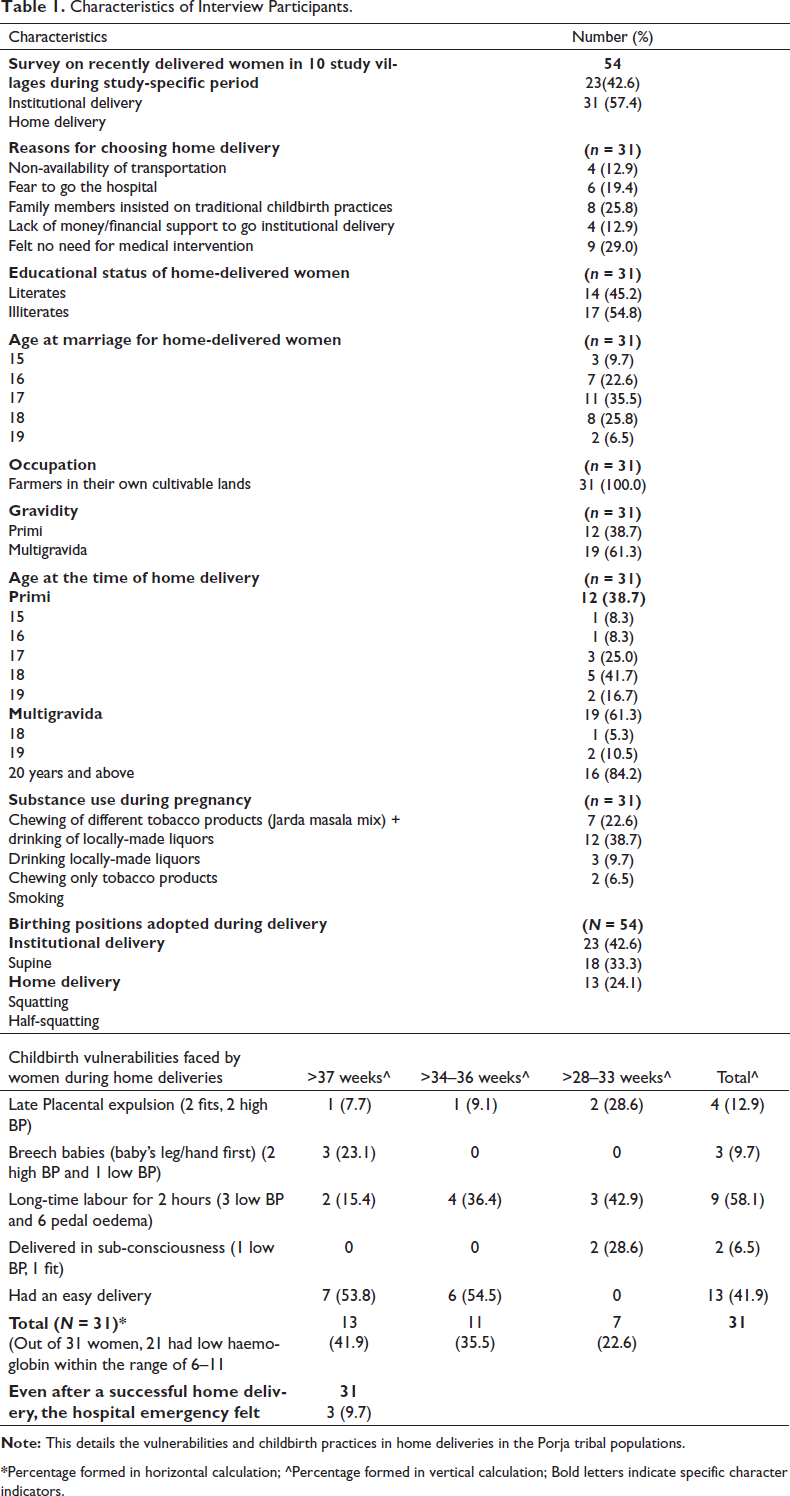
*Percentage formed in horizontal calculation; ^Percentage formed in vertical calculation; Bold letters indicate specific character indicators.
Table 2 represents gestational risks of the pregnant women and risks of low weight babies. Highly adopted home delivery birthing positions were squatting (33.3%) and half-squatting (24.1%). In the home deliveries, a greater number of mothers had longer-time labour (58.1%), in which, three had low BP and six had pedal oedema (high BP); following this, the late expulsion of placenta (12.9%) were faced by women with fits and high blood pressure; breech babies (9.7%) were recorded among women with high BP and poor gestational weight; women were reported of delivering in sub-conscious state (6.5%) with gestational history of suffering from low BP and fits.
Gestational Weeks Wise Exposure to Difficulty Labour (DL), Anemia, Illnesses and Low-birth Weight among Related Children.
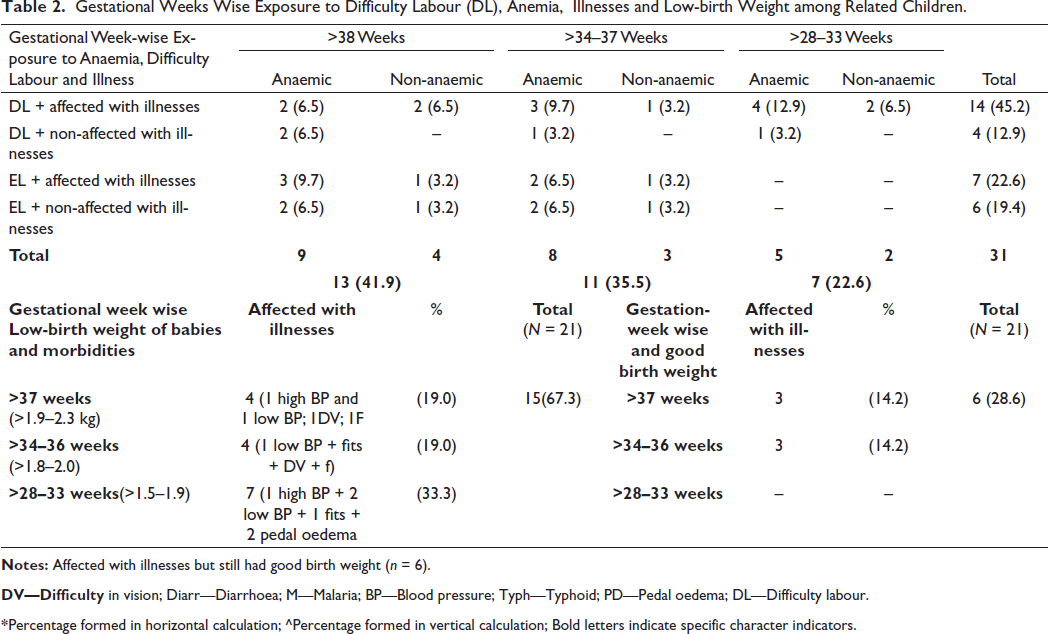
DV—Difficulty in vision; Diarr—Diarrhoea; M—Malaria; BP—Blood pressure; Typh—Typhoid; PD—Pedal oedema; DL—Difficulty labour.
*Percentage formed in horizontal calculation; ^Percentage formed in vertical calculation; Bold letters indicate specific character indicators.
Of 31 postpartum women, 21 women were anaemic; 18 experienced difficult labour. Analysing linkages and complexities in the gestational weeks wise, 12.9% and 9.7% mothers were exposed to difficulty labour along with illness and anemia during >28–33 and >34–36 weeks respectively.
Qualitative Views
Postpartum Mothers’ Perspectives on Adopted Vertical Birthing Positions
Women’s Experience of Using Different Birthing Positions During Their Labour
Nearly 18 postpartum women reported the adoption of varying vertical birthing positions. Shifting from squatting to half-squatting during their labour is the most common practice in the long-hour labour pains to avoid maternal and neonatal injury and mortality.
Circular walking by holding an old saree dropped down from the roof helps early labour, reduces pain and pressure. (IDI 8, 9, 10, 21, 26)
Four of the postpartum mothers had childbirth in sub-conscious state explained that they could complete the safe delivery with the help of their mothers-in-law and TBAs, could complete a though they faced difficulty in expelling the placenta. However, adopting a half-squatting birthing position with constant longer breathing helped to expel the placenta with post-delivery reporting of difficulties like swollen private parts due to pressure on the birth membranes.
Squatting is the Best-known and Highly Preferred Birthing Position
In this study, 26 respondents reported that the squatting position is the most commonly adopted method during their labour period, which is in most cases advised by their birth attendants. As per them, this position propagates easy dilation of the baby and controls breathing activities without leading to maternal distress.
Squatting position gives relief and promotes quick labour. (IDI 3, 11, 18)
The significance of the squatting position envisioned through the IDIs with postpartum mothers reveals that the old TBAs advise the squatting position as the most convincing method.
Adopted Half Squatting Position as Instructed by the TBAs
Over 18 postpartum mothers reported that the half-squatting position ensures strength when the mothers start feeling the loss of consciousness and cannot breathe enough to deliver the baby. Some of the qualitative expressions felt by the mother were
I had no energy, became blurred (Sub-conscious) due to the severity of labour pains. But with the instruction of TBA, I delivered in half-squatting position (IDI 14, 17, 29).
Another qualitative expression was captivated from 19-year-old mother with similar reporting from other other two:
I had prolonged labour pains, but less dilation. The traditional birth attendant made me walk circular in half squatting by holding a saree then the delivery happened (IDI 3, 18, 24).
TBAs’ Perspectives on Suggested Birthing Positions
False Pains are a Sign of Breech Babies, no Home Deliveries are Possible
All the TBAs were observed to have good knowledge of false labour pains occurring in the third trimester, which were explained as follows. As months increase, frequent exposure to pains such as pressure on the pregnant women’s genital region, and digging pain in either of the pelvic regions is considered a set of false labour pains due to the baby’s movement and dislocation from the birth canal. These signs alert the TBAs to be cautious enough not to take obstetric risks leading to mortality of either mother or child, or both. However, TBAs resort to making home deliveries when the region is under harsh climatic conditions (heavy rainfalls from May to October) and in the absence of elderly female family members. The pregnant women are examined with two ways of indigenous method for identifying the baby’s position for attempting delivery.
The first method is performed on the day of onset of labour pains, in which TBA pours castor oil (10–15 drops) in the notch of the pregnant woman’s chest region. The straight passing down of the oil onto the pregnancy bump is ready confirmation for safe home delivery, which the TBA in the home can easily handle. Second is that the slight dislocation of linea nigra from the navel region is said to be riskless for home deliveries than the higher dislocation. Few of the TBAs’ qualitative expressions were
Our indigenous tests help us ensure enough before attempting home deliveries. Otherwise, our community members blame us for any mishappen that cause difficulty to our community living with restriction on food grains and free move (though all are close kins in the village. (TBAs of 41 years old; 51 years old; 44 years old).
Half-squatting Position Eases Complicated Deliveries and Shortens the Painful Labour Timing
TBAs were interviewed about how the home deliveries proceeded even after encountering labour complications and dealing with obstetric danger signs. For this, TBAs responded that the half-squatting position is the safest for labouring women with enduring longer labour pains. This position helped the shortening of the duration of labour to 20–40 minutes from two to 3 hours in squatting. Also, TBAs were aware that two of the birth outcomes were critical because of the umbilical wirings around the baby’s body, leg or hand, leading to the execution of home-based newborn resuscitation to retrieve the breath as observed in a few of the cases (n = 7), only one hand grabbed umbilical wirings and leg in others.
Longer labour pains and complications are eased with half-squatting positions that reduces pressure on the mother and baby’s body parts. Otherwise, the baby has irregular-sized body parts (becomes a physically challenged person). (Three TBAs of 48 years old, 51 years old, 55 years old).
Despite the significant benefits of the half-squatting position, the TBAs also highlighted the disadvantages associated with the half-squatting position. Three of the TBAs called off half-squatting on around seven study participants.
Half-squatting is immediately called off, if there is a labour resulting in maternal distress, severe vomiting or excretion by the labouring woman. (Two TBA of 55 years old; 43 years old)
Vertical Birthing Positions are an Age-old Cultural-based Birthing Method
Knowledge, beliefs and practices around vertical birthing positions persuaded the TBAs to get the actual reason for adopting only vertical birthing positions. Two of the TBAs responded that their older generations were accustomed to vertical birthing positions, aware of their benefits, and had passed them down to their generations to execute successfully. Two TBAs explained that delivery in the supine position is not found in their societies, except in the hospitals. One TBA responded that these positions ensure the mother’s safety and easy delivery of the child without leading to abnormalities.
Our elderly TBAs’ were conducting home deliveries with vertical birthing positions. Even we had adopted vertical positions in our childbirths and now suggest the same for the labouring women for safe survival of the mother and child (TBAs of 41 years old; 48 years old; 53 years old).
Discussion
Pregnancy and childbirth are regarded as critically important life-cycle events in tribal women’s life and are socio-culturally constructed to ensure the health and well-being of mothers and foetus/child.21, 22 The present study reports the two indigenous methods adopted by TBAs before conducting homebirths as efforts towards safer childbirths. First, the massaging with oil to identify the baby’s head near to or away from the birth canal with the passage of oil on to navel region, and second, through the properly aligned or zigzag appearance of linea nigra. The TBAs informed that delivery would be out of her capacity and with immediate recommending the pregnant women to go for institutional births when the child’s head is dislocated and zigzag/dislocated linea nigra from the navel region.
TBAs played a significant role in the whole labour process.23, 24 TBAs executed vertical birthing positions as an age-old birth custom, which is culturally considered of ensuring women’s comfort, avoiding maternal distress, promoting early labour and preventing maternal and foetal death. 25 The vertical/upright birth positions are believed to help reduce complicated situations by shortening labour duration, helping in uterine perfusion, contractions effectiveness, and on foetal alignment to the pelvic angles and diameters. 26 , 27
Another finding reveals that TBAs allowed labouring women to freely choose between the squatting and half squatting position during severe and labour pains. This practice helps reduce labour length, and promoted a positive perception of the physiological event in relaxed and felt comfortable, resulting in increased women’s comfort and satisfaction even after childbirth.28, 29 Various studies have highlighted that vertical birthing positions were widely adopted during early phases of modern medicine. But vertical birthing positions are subject to more difficult medical management when peculiar conditions (amniotomy, oxytocin, induction, foetal monitoring, uterine contraction tracings) and interventions (epidural analgesia) are required and during the requirement to assess spontaneous movements of the foetus. 10
There were no reported maternal and neonatal mortality due to vertical birthing positions in the study period. However, two of the families sought immediate healthcare intervention for the eclampsia mothers. But the four of the neonates were extremely exposed to infections within the first week of life due to extreme socio-cultural practices of applying turmeric, and different ashes on the neonates’ bodies.
The study also revealed that adolescent conceptions, low gestational weight, eclampsia, anaemic conditions and high and low blood pressure compounded childbirth vulnerabilities irrespective of the gestational weeks. Low-birth weight of newborns (1.8–2.1 kg) were born to women affected with maternal morbidities. This could be due combination of low socio-economic status, poor nutritional intake, irregular uptake of antenatal care, avoidance of health worker advice, low education level of mothers, non-availability and non-accessibility to health facilities, low knowledge on pregnancy emergencies and subsequent close conceptions.30, 33 Preterm labour, and pedal oedema observed in our study could be a consequence of anaemia conditions.
The present qualitative observational study indicates that vertical birthing position has positive perinatal outcomes and absence of maternal and neonatal mortality with good positive pregnancy outcomes in the study population context. With the provision of good antenatal care, early detection of maternal and foetal complications, and dissemination of knowledge on early care and management at the household level, tribal maternal health and mortality status can be improved in hard to reach settings. TBAs’ knowledge of false pains and their suggestion on encouraging pregnant women to institutional deliveries is a highly encouraging finding in our study. We acknowledge the fact that our study is limited to this particular tribal group in the study region. However, the findings are important as it include the tribal women’s plans and efforts for successful childbirths and are full of knowledge on the facts around the execution of vertical birth positions.
Conclusion
Our study shows that culture-specified childbirth practices still play a crucial role in shaping the maternal health of hilly tribal communities. Promoting beneficial traditional childbirth positions can help improve the maternal health outcomes of tribal women living in inadequate health facilities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was conducted as apart of post-doctoral research and the research protocol was reviewed and approved by the Institute of Human Ethics Committee at Indian Council of Medical Research-Regional Medical Research Center, Bhubaneswar, India.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Verbal and written consent were obtained from the respondents before conducting the interviews.