
Abstract
Background
Decision conflict usually occurs from poor patient involvement in decision making which may cause regrets about the options that were chosen. Health professionals should impart antenatal education to enhance a mother’s belief about her birthing.
Objective
To assess the effect of supportive educational intervention on decision conflict among primipara mothers with a fear of childbirth (FOC).
Methods
An randomized controlled trial (RCT) was conducted on 205 primipara mothers with an FOC attending Gynae OPD. At 24–28 weeks of pregnancy, mothers were screened for FOC WDEQ-A and then randomly allocated to the experimental (103) and control group (102) and assessed for decision conflict by using a decisional conflict scale. The experimental group was given Supportive educational intervention. At 37–38 weeks of pregnancy, both groups were again assessed for decision conflict. Three participants from the experimental and two from the control group were lost to follow up and the final post-test was completed by 200 participants. Data analysis was done by calculating frequency, mean, standard deviation, Fisher Exact test, chi-square, t-test and F-test using SPSS version 18.
Results
There was a significantly lower post-intervention decision conflict score in the experimental group as compared to the control group (p < .001). No difference was observed in the pre-test score in both groups.
Conclusion
Supportive educational intervention was effective in primipara mothers for reducing decision conflict. Improving antenatal emotional well-being will lead to a positive childbirth experience with better perinatal outcomes.
Introduction
Fear of childbirth (FOC) has a role in women’s experiences of pregnancy and birth. Elevated fear during pregnancy has been related to the progression of birth (longer birth duration), an increased likelihood of intervention including augmentation of labour and emergency caesarean section and an increased likelihood of elective caesarean delivery. However, studies exploring the relationships between FOC and adverse birth outcomes are inconsistent and further examination is required. 1
Parturition fear encompasses a negative impact on a woman’s psychological well-being during gestation and her experience of birth. Childbirth fear is related to the poor emotional and mental state of the women. Psycho-education given by trained health professionals has proven to be effective in reducing high childbirth fear levels and helps to make confidence regarding childbirth. 2
Despite these fears and educational interventions to the primipara mothers, little is understood about women’s involvement in higher cognitive processes during labour. Higher cognitive processes involve making choices along with physicians about the screening, treatment and other aspects of care. A shared cognitive process tends to scale back decision conflicts, increasing delivery satisfaction and other positive feelings about the newborn and reducing fears. Decision conflict can arise on the premise of the mode of delivery, whether normal vaginal or caesarean delivery. Counselling and educational programs can increase knowledge and reduce decision conflict. 3
A systematic review was conducted to evaluate the effectiveness of patient decision aids made for pregnant women based on psychosocial and clinical results. It was concluded that obstetric care could be improved through patient decision aids. These aids were developed for prenatal testing, labour analgesia, vaginal birth after c-section, etc. 4
An exploratory cross-sectional study was conducted on 205 pregnant women to assess the relationship among various socio-demographic as well as obstetric factors, FOC and childbirth efficacy. Various questionnaires and inventory techniques were used to determine the factors determining childbirth self-efficacy. The study concluded that an increase in self-efficacy levels can promote normal childbirth. 5
During stressful and anxious conditions, adrenaline is produced which inhibits the activity of the uterus and causes prolonged labour. Therefore, a pregnant woman should be well informed regarding labour and pregnancy as influence is created on the progress of labour and the attitude of both the partners towards one another and the newborn baby. By providing education to women, they may be prepared for their role of decision-making so that they can make personal decisions that are right for them. This information has got to be evidence-based which may be the basis of the development of personal birth care plans and encourages women to choose their care provider and place of birth. 6
Objective: To assess the effect of supportive educational intervention on decision conflict among primipara mothers with an FOC.
Research hypothesis: There is a statistically significant decrease in decision conflict among primipara mothers with an FOC after the implementation of supportive-educational interventions at p < .05 level of significance.
Research methodology: A randomized controlled trial was conducted in Government Medical College and Hospital, Chandigarh. The primipara mothers in the age group of 20–35 years with an FOC attending Gynae OPD in Government Medical College and Hospital, Chandigarh were enrolled. Participants were 24–28 weeks pregnant, with a singleton pregnancy, having Wijma Delivery Expectancy Questionnaire score 61–85, in the age group 20–35 years, able to read and understand English/Punjabi/Hindi and willing to participate in the study. The sample was estimated by power analysis based on the daily OPD count of primipara mothers with an FOC using the following formula
N = population size 400 (estimated based on pilot study), Z = Z-score 1.96, Z 2 = 3.84 (critical value at 95% confidence), p = .5, e = margin of error e = 0.05, e 2 = 0.0025. On calculation sample size obtained was 196 and the researcher had selected 205 participants.
An interview schedule was used to collect data. It has the following sections:
Supportive educational intervention: It refers to the provision of informational and emotional support regarding pregnancy and the birthing process in two sessions. In the first session, Strategies for Empowering Natural Birthing Process with Physical and Mental Preparation regarding pregnancy and childbirth was given by teaching and distributing an educational booklet along with recorded audio for guided meditation. In the second session strategies to maintain strength during labour and preparation for the day of delivery by educating and providing an educational booklet to enable primipara mothers with an FOC to have physical and mental stamina, to have less FOC.
Data collection: Permission obtained from Director Principal GMCH, Chandigarh, Professor In-charge Academics GMCH, Chandigarh. Ethical clearance was obtained from the Institution ethics committee of GMCH, Chandigarh as per IEC Regd. No. ECR/Inst/PB/2014/RR-2017. Written informed consent was obtained from participants. Participants’ right to privacy was protected by confidentiality. Permission to use the tools was taken from the authors. Data was collected from March to November 2021. Initially, primipara mothers with an FOC were screened by using the W-DEQ-A between 24 and 28 weeks of pregnancy. Mothers whose scores were between 61 and 85 were selected (as shown in Figure 1).
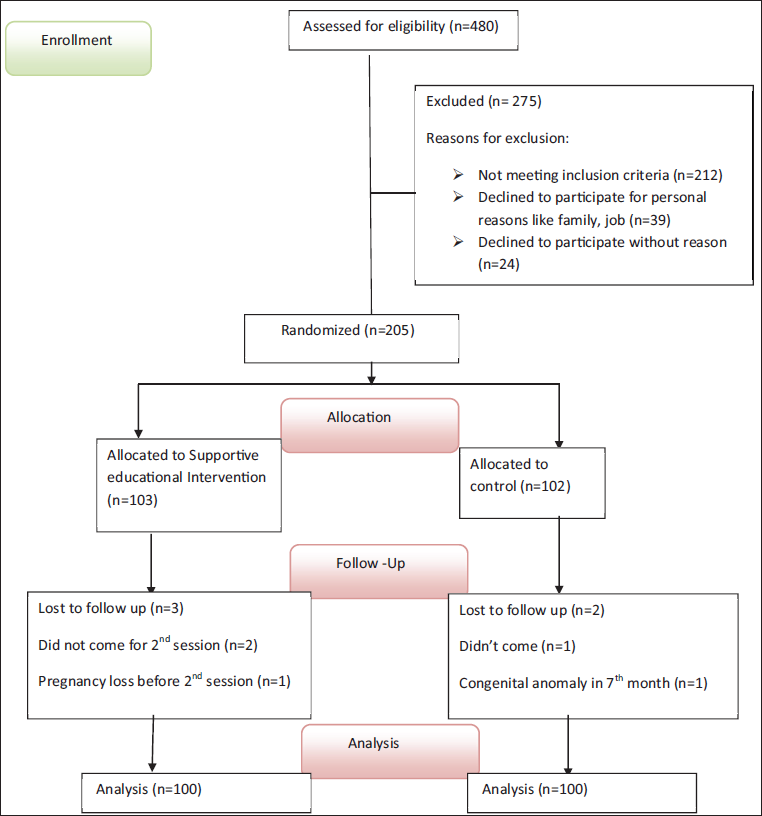
A total of 205 subjects had selected and randomised by lottery method into experimental and control groups, that is, 103 in the experimental group and 102 in the control group. Experimental group mothers received planned Session I of intervention at 24–28 weeks of pregnancy. Rapport and therapeutic connection between the researcher and mothers was made by acceptance of the woman’s perspective. The researcher interacted with the primipara mothers with an FOC to know about the cause of their fear related to childbirth and motivated them to talk about their fear so that possible solutions could be provided along with the care of mothers during pregnancy. They were also asked to write about her negative self-talk, beliefs and fear. The second session was given at 32–36 weeks. At 37–38 weeks of pregnancy, post-test was done. Three participants from the experimental group were lost to follow and the final post-test was taken by 100 participants in the experimental group and 100 participants in the control group (Figure 1). Data analysis was done by calculating frequency, mean, standard deviation, Fisher Exact test, chi-square, t-test and F-test using SPSS version 18.
Results
In the experimental group, more than half of the participants (71%) were in age groups 24–<30 years, 19% were in age groups of 18–<24 years and the remaining 10% were in age group of 30–35 years. In the control group, more than half of the participants (67%) were in age groups 24–<30 years and 21% were in age groups 18–<24 years. The educational status of 45% of participants in the experimental group and 40% in the control group were educated up to senior secondary. Husband’s education of 44% in the experimental group, and 48% of participants in the control group was up to senior secondary. Occupation, of 49% of participants in the experimental group and 51% of participants in the control group were housewives. Husbands of 62% of participants in the experimental group and 59% in the control group were employed in the private sector. The family monthly income of 49% of participants in the experimental group and 48% in the control group was in the range of Rs. 20,000–40,000. Support persons among 44% of participants in the experimental group and a similar percentage in the control group were husbands. Both experimental and control group were comparable in respect to age, educational status, occupation, monthly income and availability of support person in the family (p > .05 as per chi-square test).
History of adverse pregnancy outcomes in family/relatives was reported by 25% of participants in the experimental group and 24% in the control group. Three-fourths of participants (75%) had no adverse pregnancy outcomes and 25% had a history of adverse pregnancy outcomes in friends/relatives. In the control group, the majority of participants (76%) had no adverse effects and the remaining had a history of adverse pregnancy outcomes in friends/relatives.
According to the decision of conception, in the experimental group, 69% had mutually decided, 23% had the pressure of in-laws, 6% had self-made decisions and 2% had the pressure of husband for conception. In the control group, 72% had mutually decided, 24% had the pressure of in-laws, 4% had a self-made decision and no mother was having the pressure of husband for conception.
As per planning of pregnancy, in the experimental group, 87% had planned pregnancy and 13% did not plan the pregnancy. In the control group, 88% had planned pregnancy and 12% did not plan the pregnancy. Both experimental and control groups were homogenous as matching was done by calculating the chi-square value.
Assessment of Decision Conflict
Table 1 shows that during the pre-test, in the experimental group, 58% of participants had moderate decision conflict, and 42% had severe decision conflict among primipara mothers with an FOC. During the post-test, the majority of participants (91%) had moderate decision conflict, 8% had mild decision conflict and only 01 had severe decision conflict. In the control group, during the pre-test more than half of the participants (53%) had severe decision conflict, and 47% had moderate decision conflict. During the post-test, 61% of participants had moderate decision conflict, 5% had mild decision conflict and 5% had severe decision conflict.
Comparison of Decision Conflict Categories in Experimental and Control Group During the Pre-test and Post-test (N = 200).
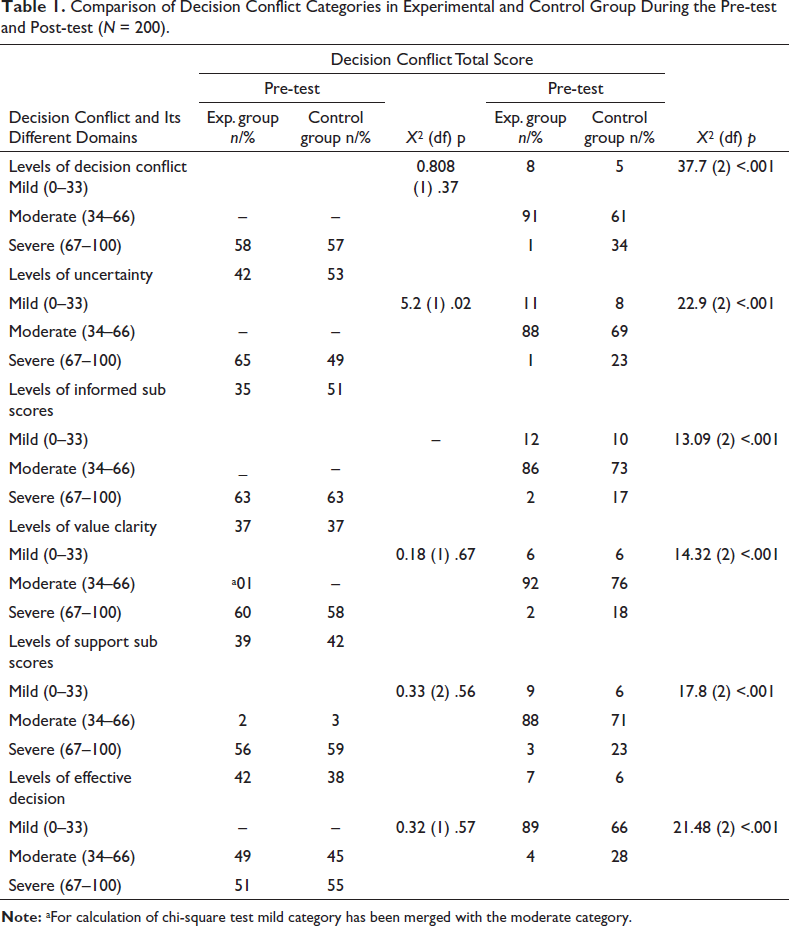
During the pre-test, in the experimental group, 65% of participants had moderate uncertainty and 35% had severe uncertainty. During the post-test, 88% of participants had moderate uncertainty, 11% had mild uncertainty and only 01% had severe uncertainty. In the control group, during the pre-test, half of the participants (51%) had severe uncertainty and 49% had moderate uncertainty. During the post-test, 69% had moderate uncertainty, 23% had severe uncertainty and 8% had mild uncertainty.
Further during the pre-test, in the experimental group, 63% of participants had moderately informed sub score and 37% had extremely uninformed sub score. During the post-test, the majority of participants (86%) had moderately informed sub score, 12% had extremely informed sub score and only 02 had extremely uninformed sub score. In the control group, during the pre-test, 63% of participants had moderately informed sub score and 37% had extremely uninformed sub score. During the post-test, the majority of participants (73%) had moderately informed sub score, 17% had extremely uninformed sub score and 10% had extremely informed sub score.
During the pre-test, in the experimental group. Overall, 60% of participants had moderately clear value clarity sub score, 39% had extremely unclear value clarity sub score and only 01 had extremely clear value clarity sub score. During the post-test, the majority of participants (92%) had moderately clear value clarity sub score, 6% had extremely clear value clarity sub score and only 2% had extremely unclear value clarity sub score. In the control group, during the pre-test, 58% had moderate uncertainty and 42% had extremely unclear value clarity sub score. During the post-test, the majority of participants (76%) had moderately clear value clarity sub score, 18% had extremely unclear value clarity sub score and 6% had extremely clear value clarity sub score.
Further during the pre-test, in the experimental group, 56% of participants had moderately supported sub score, 42% had extremely unsupported sub score and only two had extremely supported sub score. During the post-test, the majority of participants (88%) had moderately supported sub score, 9% had extremely supported sub score and only three had extremely unsupported sub score. In the control group, 59% of participants had moderately supported sub score, 38% had extremely unsupported sub score and only three had extremely supported sub score. During the post-test, the majority of participants (71%) had moderately supported sub score, 23% had extremely unsupported sub score and there were 6% had extremely supported sub score.
At last, during the pre-test, in the experimental group, 51% of participants had poor effective decision scores and 49 had fair effective decision scores. During the post-test, the majority of participants (89%) had fair decision scores, 7% had good decision scores and only 4 had poor decision scores. In the control group, during the pre-test, 55% of participants had poor effective decision scores and 45% had fair effective decision scores. During the post-test, 66% of participants had fair decision scores, 28% had poor decision scores and 6% had good decision scores.
Comparing categories of decision conflict and its different domains it was observed that during the pre-test there was no significant difference between the experimental and group about different categories of decision conflict and its different domains (except the level of uncertainty) such as informed, value clarity, social support and effective decision (p > .05 as per chi-square test) In both the groups participants were in moderate or severe category. After implementing the supportive educational programme during the post-test it was observed that in the experimental group, a significantly higher per cent of participants were in mild and moderate categories in the experimental group in decision conflict and its different domains as compared to the control group where most of the participants were in moderate and severe category (p < .05 as per chi-square test) (Table 1).
Comparison of Mean Pre-test and Post-test DCS
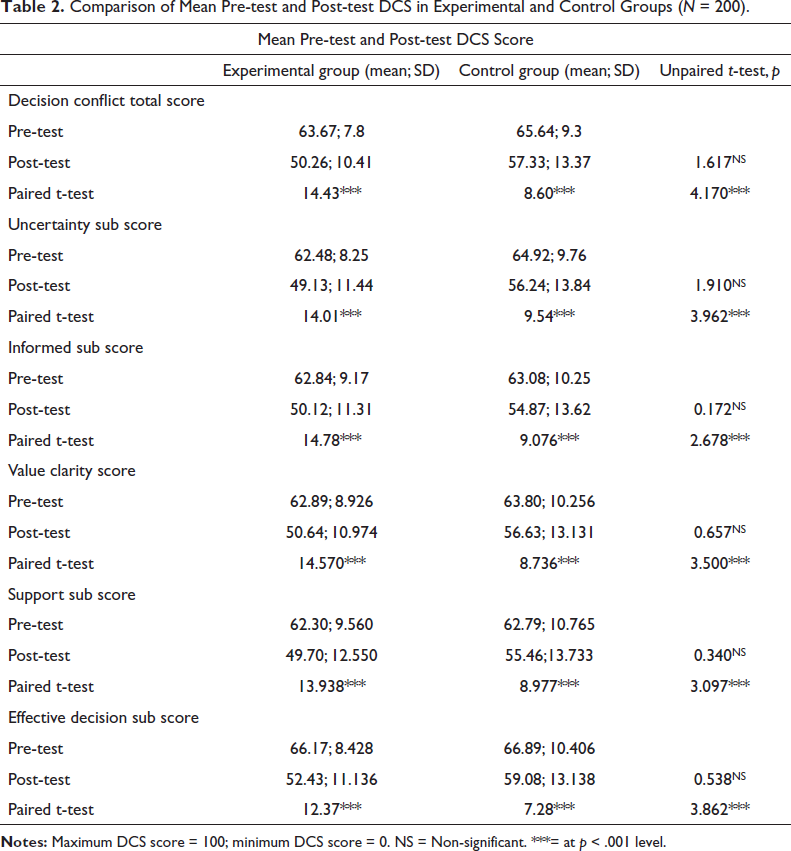
Table 2 shows that there was no significant difference between the mean pre-test decision conflict total scores of the experimental and control group but after the supportive educational intervention on decision conflict, there was a significantly lower mean decision conflict total score in the experimental as compared to the control group (p < .001). Similarly, there was no significant difference in the mean pre-test score of the experimental and control group in different domains of DSC subscales score, that is, informed, value clarity, social support, uncertainty and effective decision. After implementing supportive educational intervention there was a significantly lower score of DSC subscales, that is, informed, value clarity, social support, uncertainty and effective decision in the experimental group as compared to the control group. This indicated that supportive educational intervention was effective in reducing DCSs among primipara mothers. Hence research hypothesis was accepted as there is a highly significant effect of supportive educational intervention on decision conflict effective decision among primipara mothers at the level of p < .001. Though there was a significant decrease in the pre-test to post-test mean score in both the groups in the experimental group this difference was significantly higher than control group. In the control group, this difference may be due to routine care.
Comparison of Mean Pre-test and Post-test DCS in Experimental and Control Groups (N = 200).
Discussion
Imparting antenatal education will help to improve the physical and psychological well-being of pregnant mothers. The supportive-education intervention may facilitate a communicative and caring partnership with women to cut back or heal childbirth fear from mid to late pregnancy. Assisting women to reframe their perceptions about their ability to birth may be a critical strategy in preserving the normality of birth. The provision of educational and emotional support has the potential to healthy mothers and babies with good and emotionally stable birthing experiences which otherwise may turn into disappointing or traumatic births. Hence the present study was undertaken.
The findings of this study demonstrated the effect of supportive educational intervention on decision conflict. Primipara mothers with an FOC who received the supportive educational intervention reported lower levels of decision conflict and subscales score, that is, informed, value clarity, social support, uncertainty and effective decision than control at 37 weeks. As findings of the current study showed a significantly higher mean post-test decision conflict total score in the experimental group as compared to the control group (p < .001) indicating the impact of supportive educational intervention on decision conflict. Similar findings were reported by Byrne et al. 7 during which there was a statistically significant difference in DCS between the intervention group who received individual counselling (0.614; 0.626) and also the control group (1.216; 0.949) at p < .001. The study results indicated that the total scores of decision conflict as well as subscales score (i.e., informed, value clarity, social support, uncertainty and effective decision) were significantly lower in the intervention group and therefore the findings are in line with the current study Another finding was reported by Sun et al. 8 where midwife led psychoeducation was effective to scale back DCS in the experimental group than control but the difference was not statistically significant.
Conclusion
Supportive educational intervention was effective in primipara mothers for reducing decision conflict. Hence it is recommended for nurses working with pregnant mothers to incorporate such educational intervention in their day-to-day practice. A similar study can be replicated on a large sample by selecting multiple hospitals to validate and generalize findings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Yes, Institutional Ethics Committee (GMCH, Chandigarh). IEC Regd. No. ECR/Inst/PB/2014/RR-2017.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from participants.