
Abstract
The COVID-19 vaccine has been made available for emergency use in Bangladesh. However, willingness to receive the vaccine may be affected by varying factors across the country. Therefore, this study aimed to investigate the factors that influence willingness to receive the vaccine among Bangladeshi adults. A population-based cross-sectional online survey was conducted among a sample of 1,725 Bangladesh adults (age 18 years and older). The statistical analysis included univariate, bivariate and multivariate regression model. Findings show that 85% (n = 1463) of respondents were willing to receive the vaccine. Respondents with 1–2 children (aOR: 1.77, 95% CI: 1.00–3.13, P = . 048), perceived risk of being infected (aOR: 1.48, 95% CI: 1.03–2.14, P = . 03), perceived impact on daily life (aOR: 2.53, 95%CI: 1.45–4.44, P = . 001), history of co-morbidities (aOR: 2.04, 95% CI: 1.37–3.04, P < . 01), price of the vaccine (aOR: 3.58, 95% CI: 2.34–5.47), physician’s recommendation to receive vaccine (aOR: 2.06, 95% CI: 1.38–3.06, P < . 01), vaccines supplied by government (aOR: 2.31, 95% CI: 1.64–3.25, P < . 01) were found to be motivating factors for willingness to receive the vaccine. Findings indicate that willingness to receive the vaccine is likely to be affected by socio-demographic, and health system factors. This should be carefully considered in the rollout of the vaccination plans in Bangladesh.
Introduction
Several factors may influence the willingness to be vaccinated amongst a population. Prior studies have shown that socio-demographic characteristics, misperceptions, and/or rumours about vaccine efficacy, safety concerns, price, and socio-cultural factors may influence individuals’ willingness (Al-mohaithef & Padhi, 2020; Larson et al., 2014, 2018; Nguyen et al., 2011; Wu et al., 2018). For example, Chan et al. (2015) revealed that personal anxiety, previous vaccination history and inadequate knowledge about the A/H7N9 influenza vaccine resulted in a 50% reduction in its acceptance by respondents in a Hong Kong survey (Chan et al., 2015). Another study conducted in the United States showed that hypothetical influenza vaccine uptake was likewise dependent on societal influences, health insurance, and demographics, including younger individuals and those within a lower income group less willing to take the vaccine (Abbas et al., 2018). In recent decades, several countries have been experiencing a decline in vaccine coverage due to safety concerns, the effectiveness of vaccines, misinformation, religious beliefs, and level of income (Figueiredo et al., 2016, 2020; Malesza, 2020; WHO, 2020). More recently, and specifically with COVID-19, misinformation, conspiracy theories, and mistrust have been identified as potential factors that may influence individuals’ decision to not vaccinate (Burki, 2019; Guidry et al., 2020; Islam et al., 2021; Roozenbeek et al., 2020).
Bangladesh has a high COVID-19 transmission rate (2.53–6.72), slightly higher than the basic reproduction number (Ro) estimated in China (2.3–5.2) (Talukder et al., 2020). The country is experiencing a higher than average general record of vaccination (over 90% coverage) in children, however, vaccine acceptance among adults varies (WHO, 2020). Acceptance of vaccines for other communicable and non-communicable diseases for children and adults have been assessed in Bangladesh (Bhuiyan et al., 2018; Larson et al., 2016; Rahman & Obaida-nasrin, 2010), however, there is no or limited published literature on willingness to be vaccinated for COVID-19 till date. Understanding factors that may influence vaccine acceptance is crucial to enhance vaccine uptake. In response, we conducted a population-based cross-sectional study amongst Bangladeshi adults on as online platform to investigate factors that may impact their willingness to receive the COVID-19 vaccine.
Materials and Methods
Study Settings and Data Collection
The methods and data collection tools for this study have been adopted from previously published studies (Al-mohaithef & Padhi, 2020; Sherman et al., 2020). In summary, between 20 September and 5 October 2020, a team of social scientists and epidemiologists conducted a cross-sectional study on as online platform using Facebook, email, and WhatsApp. Bangladeshi adults aged 18 years and older were invited to complete a questionnaire. The questionnaire for this study was formulated based on recently published studies (Abbas et al., 2018; Al-mohaithef & Padhi, 2020; Harapan et al., 2020; Seale et al., 2021; Sherman et al., 2020; Wang et al., 2020). We chose the online media platform due to restrictions on movement and other COVID-19 preventative measures. We also chose this online platform to avoid face-to-face interactions with respondents during the pandemic. Further, we wanted to reach as many people as quickly as possible given the speed at which a vaccine was being developed for COVID-19 and the importance of the information for successful vaccine rollout (Harapan et al., 2020; Sherman et al., 2020). We used a combination of convenience and snowball sampling to recruit respondents; invitees were requested to share and/or forward the Google form with their friends who used any of the above mentioned online communication platforms (Harapan et al., 2020). Respondents who were less than 18 years of age, non-Bangladeshi citizens, and Bangladeshi citizens who were currently living abroad were excluded. Adopting from a previous study, we developed a bilingual (Bengali and English), self-administered and structured questionnaire (Al-mohaithef & Padhi, 2020). The key areas covered included socio-demographic information, history of co-morbidities and willingness to receive the COVID-19 vaccine. We pre-tested the questionnaire among 50 respondents who were not included in the study and revised the questionnaire based on their feedback on the structure of the questions, and translating the questions and responses into lay languages.
Analysis
We analysed the data by using the STATA software (STATA version 13). Initially, we performed a univariate analysis of demographic characteristics and exposure history to the COVID-19 virus of respondents. In the second stage, we completed a bivariate analysis to observe the association between exploratory variables and willingness to receive the vaccine. Finally, we performed a multivariate logistic regression using a generalised linear model. In the multivariate model, the variables with a p-value < .25 in the bivariate model were included. Backward elimination process was performed to finalise the multivariate model.
Ethical Considerations
The study protocol was reviewed and accepted by the Institutional Review Board of Jagannath University, Dhaka, Bangladesh [JnU/admin-1(96)/2008/part-01/8362]. Informed written consent was collected from respondents before completing the survey. Further, we did not include any minors in this study.
Results
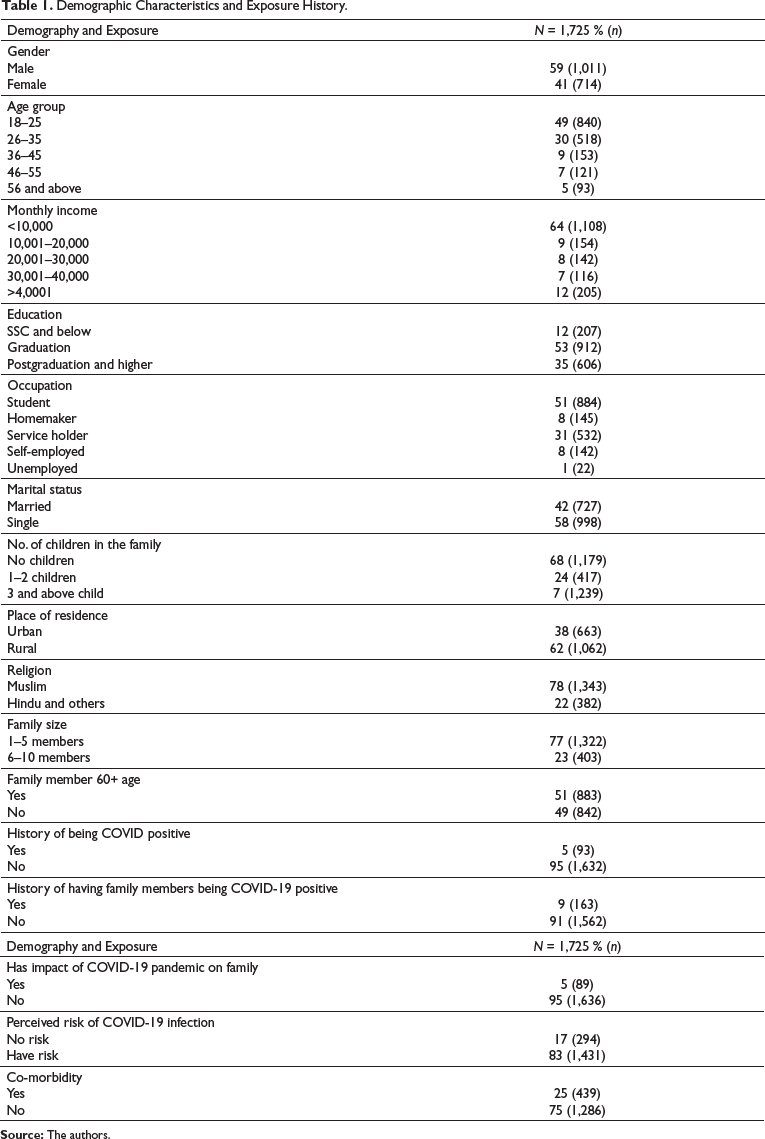
Demographic Characteristics and Exposure History.
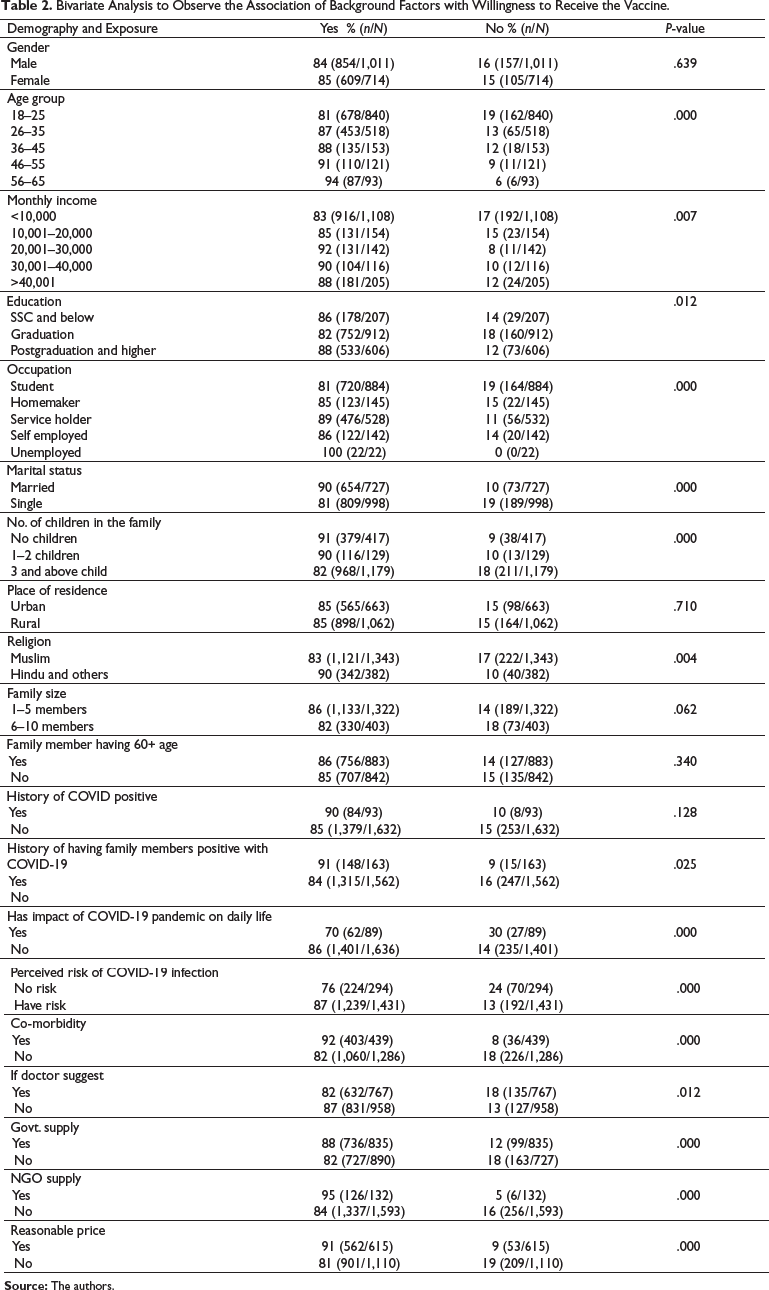
Bivariate Analysis to Observe the Association of Background Factors with Willingness to Receive the Vaccine.
Willingness to Receive the Hypothetical Vaccine Among Different Demographic Characteristics and Exposure History.
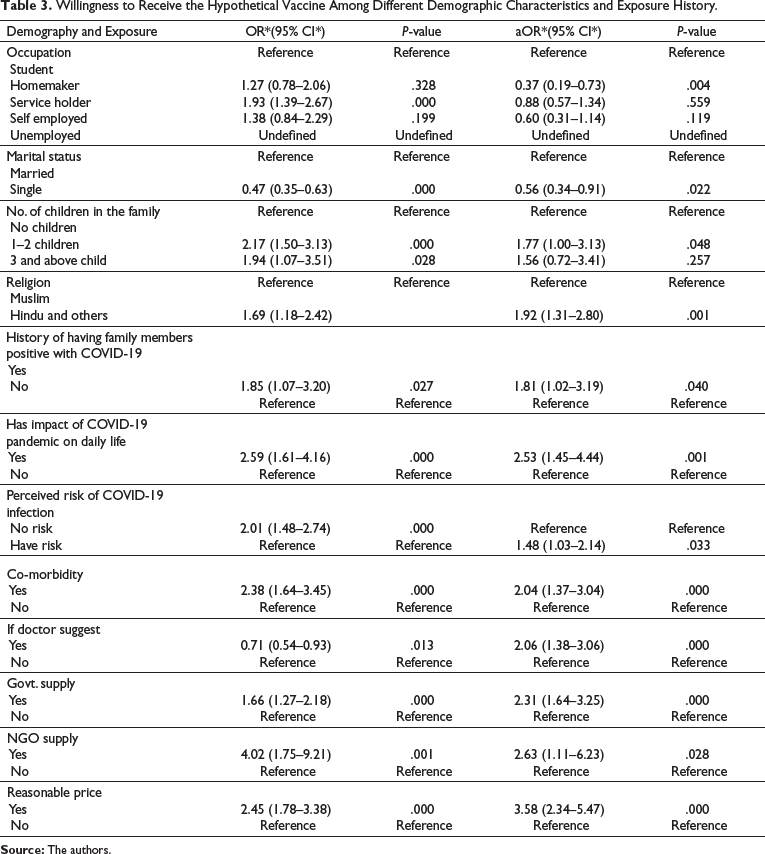
Homemakers were 63% (aOR: 0.37, 95% 0.19–0.73, P = . 004) less willing to accept the vaccine compared to students, and unmarried respondents were 44% less willing (95% CI: 0.34–0.91; P = .022) to receive the vaccine compared to their counterparts. In addition, respondents with religious background Hindus or others were 1.92 times (aOR: 1.92, 95% CI: 1.31–2.80, P < . 001) more willing to receive the vaccine compared to Muslim religious group (see Table 3).
Discussion
The study found a high willingness to receive the vaccine (85%) among the study respondents. Individual-level factors such as risk perception about COVID-19 and its impact on daily life, co-morbidity, family-level factors such as having children and history of family members positive with COVID-19, and health system factors that included supply of vaccines from the government or NGOs and physicians’ recommendations for COVID-19 vaccine all were the factors contributing for willingness to be vaccinated. Muslims, homemakers, and never married respondents were less likely to accept the COVID-19 vaccine. The price of vaccine was another concern where a reasonable and or affordable price might increase the vaccine acceptancy three and a half times.
Risk perception is a critical factor in vaccine decision. In this study, the risk of morbidity and probably risk mortality motivated the respondents willing to receive the vaccine. Respondents who believed they were at risk of COVID-19 infection had 1.48 times higher odds of willing to be vaccinated, which is consistent with the findings from several other studies focused on the willingness to be vaccinated against COVID-19 (Harapan et al., 2020; Sherman et al., 2020; Wang et al., 2020). This finding indicates that the respondents perceived COVID-19 vaccine as a necessary step to prevent new infection as well as disease transmission. Moreover, we found the respondents with co-morbidity were more willing to receive the vaccine, which may be due to elevated COVID-19 mortality rate. This finding coincides with a study conducted in the UK where populations at greater clinical risk of serious illness from COVID-19, showed higher intention of vaccination (Sherman et al., 2020). Moreover, our study revealed significant association between impact of COVID-19 on daily life and willingness to receive the vaccine. Similar findings were reflected in studies published in China, and Indonesia (Harapan et al., 2020; Wu et al., 2018). Recent studies on COVID-19 vaccine acceptability found higher exposure to knowledge and affordability might be the triggering points for vaccine uptake among this population (Harapan et al., 2020; Malik et al., 2020; Sherman et al., 2020). In low-and middle-income countries, the NGOs are contributing substantially to immunisation services. NGOs have improved access to immunisation services in hard-to-reach areas, slums, and rural remote areas. People’s low confidence and trust in government institutions due to bureaucratic inertness, for example, delaying the procedure of vaccine administration; nepotism, for example, selecting vaccine recipients bypassing the highest vulnerable group; and corruption, for example, in vaccine pricing and vaccine distribution might act as the key factors for people preferring the NGO sectors’ management of vaccine administration (Abdullah, 2021). In our study, the respondents showed interest to receive vaccine from the NGOs and this could be because of their everyday interaction with NGOs workers, their trust in NGO services or their easy access to NGO services and reduced cost/higher perceived quality of products (Levin & Kaddar, 2011). As of December 02, 2020, there were 2,513 NGOs working in Bangladesh that can be a great resource to run COVID-19 vaccination campaign in the country (NGOAB, 2020).
Government vaccine policy influences vaccine decisions. The respondents showed their interest to adhere to government COVID-19 vaccine policy. The Bangladesh government has already declared free vaccine administration of first purchased 30 million doses among citizens (The Daily Star, 2021b). Moreover, our findings showed that physician’s recommendations may increase the willingness for vaccination which indicates physicians might play a critical role in motivating people and improving vaccine acceptancy. The question is how to train the physicians so that they can play a transparent role in motivating people for the COVID-19 vaccine. The physicians can be trained on available COVID-19 vaccines, their reagents, its efficacy and effectiveness so that they can answer people’s concerns.
The price of the vaccine was also found strongly associated with the willingness to receive the vaccine (acceptance may increase 3.5 times if the price of the vaccine is affordable). The price of the only available vaccine in Bangladesh is fixed at 425 BDT (USD 5) per shot (bdnews24.com, 2020) which raises concern among the Bangladeshi people and may impact the vaccine decision, particularly for the low-income group (The Daily Star, 2021a). However, the Bangladesh government is providing two doses of the COVID-19 vaccine free of cost to people who are susceptible to COVID-19. This is positive for the citizens to be more willing to receive the vaccine as per the findings of this study (bdnews24.com, 2021).
This study revealed that respondents with religious background Hindus and others were more interested to receive vaccines compared to their counterparts. The reduced willingness to receive vaccines among the Muslims could be due to the halal status of the vaccine as well as permissibility of receiving vaccine that originated from a haram source in Islam (Paddock, 2021; Voice of America, 2020). There were several COVID-19 vaccine misinformation circulating online that the vaccine reagents were made from aborted foetus and this misinformation raised the concern of whether the vaccine is Halal (Islam et al., 2021). Homemakers were also found reluctant to receive the vaccine and this could be due to their low involvement in income-generating activities, poor decision making power or limited access to COVID-19 vaccine-related information.
This study identified individual, familial and health system factors influential for vaccine decision. The findings of this study may help government, national and international policymakers and other stakeholders working on COVID-19 vaccine at different tiers to formulate effective intervention to minimise barriers behind implementation of mass COVID-19 vaccination in Bangladesh and countries with similar socio-demographic contexts in the future.
The study has several limitations. First, a face-to-face survey was not feasible during the current pandemic period, and so an online platform was chosen. A key concern is the representativeness of the online convenience and snowball sample gathered. To address this, we enrolled a large sample size that included diverse groups from different parts of the country. Second, the findings of our study should be read with caution. This study might estimate higher percentage of willingness to receive vaccine. The study was conducted before the actual vaccine rollout in the country and thus, our findings were less likely to be affected by the ongoing vaccine rumours and misinformation. Third, the current study collected data at a given point of time which might change depending on the severity of the disease and increasing awareness about the effectiveness of the vaccine. Last, the current study did not explore the reasons behind individuals not willing to receive vaccines in depth and detail.
Conclusion
The current study revealed that a great majority of the respondents were willing to be vaccinated. Major concerns that influenced respondents’ willingness included their personal experiences related to COVID-19 (e.g., COVID-19 positive family members, history of diabetes and asthma), price of the vaccine and the recommendation of physicians regarding vaccine uptake. The findings of this study can be helpful to Bangladeshi public health authorities to consider the factors that influence vaccine uptake or decline during a pandemic and thus formulate effective strategies to ensure a successful immunisation program. This is critically important at this time with the COVID-19 virus and to formulate effective strategies for future immunisation programs in the case of any public health emergency. Findings of our study also support the need for government and its health partners to develop community-specific behaviour change communication and implications to manage rumours regarding the COVID-19 vaccine (Lazarus et al., 2020), and strategies to modify the perception of people about vaccination and their own risk of the disease (Nguyen et al., 2011). Local physicians and non-government organisations, in particular, may help build trust among Bangladeshi adults with the COVID-19 vaccine.
Footnotes
Acknowledgements
We are thankful to the respondents for their time in participating in the study. We are also grateful to Syeeda Tarannum for her review and feedback on the questionnaire.
Authors’ Contributions
AHMK conceived the study, undertook the data collection. AHMK and TS contributed equally to develop this journal paper. TS also assisted with the statistical analysis and interpretation of the results. MSI had a significant contribution in data analysis and development of the journal paper. SKR and MMK assisted with the design of the study and study tools. MSI had a significant contribution in data analysis and development of the journal paper. SHK, MSH, SMMH, CAD and HS reviewed the manuscript and provided valuable feedback. All authors approved the final version of the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.