
Abstract
Objective:
The study aims to assess baseline immune factors that can predict the risk of severe infections in autoimmune rheumatic disease (ARD) patients, to aid in optimising immunosuppressive therapy.
Methods:
The prospective, observational study was carried out at a tertiary centre in India between December 2019 and March 2022, targeting adult patients with ARDs who required escalated immunosuppressive treatment. A comprehensive medical history, clinical examination, and baseline laboratory tests were conducted, including complete blood counts, inflammatory markers, immunoglobulin levels, immune cell counts, complement levels, and viral screening. Patients were followed for one year to track infections and hospitalisations. Descriptive statistics, ANOVA, chi-square tests, t-tests, and Fisher’s exact tests were employed for data analysis, with ordinary least squares (OLS) regression performed to identify significant factors predicting infection risk.
Results:
The study analysed 102 ARD patients over 13.1 months. Older age (OR: 1.050; CI: 1.003-1.100), low CD4 count (OR: 6.855; CI: 0.854-55.037), low CD4/CD8 ratio with (OR: 2.625; CI: 0.282-24.435), low IgG (OR: 4.500; CI: 0.251-80.565)/IgM (OR: 5.036; CI: 0.925-27.414), thrombocytopenia (OR: 3.865; CI: 1.148-13.012), high NLR (OR: 3.870; CI: 0.998-15.013), and positive anti-HBs (OR: 3.750; CI: 1.190-12.679) were linked to severe infections or death. Steroid use was significantly associated with severe outcomes, while other prior medications, including immunosuppressive therapy and biologics, showed no notable differences.
Conclusion:
CD4 counts, IgM levels, and the CD4/CD8 ratio, as well as platelet counts, are strong predictors of severe infections and mortality. Increased levels of inflammatory markers, such as ESR and NLR, also elevated the risk. Older age and steroid treatment further increase susceptibility. Patients with these characteristics should be closely monitored and given appropriate prevention strategies to reduce infection risks and related mortality.
Keywords
Introduction
Individuals with autoimmune rheumatic diseases (ARDs) have a higher risk of infections compared to the general population. 1 Infections significantly contribute to morbidity and mortality in systemic ARDs due to immune alterations caused by both the disease itself and immunosuppressive treatments. 2 Such patients experience 1.8 fold higher risk for first severe infection, a 2.1-fold higher risk for the total number of severe infections, and a 1.6-fold higher risk of infection-related mortality. 3 The increased risk of infections could be attributed to intrinsic immune dysregulation and the use of immunosuppressive therapies such as glucocorticoids and biologics, which impair host defence mechanisms. 4 Additional factors like age, comorbidities, and low baseline immunoglobulin or lymphocyte levels further increase vulnerability to severe or opportunistic infection. 5
Severe infections, defined as those requiring hospitalisation, are a primary cause of morbidity and mortality in ARDs. 6 A recent population-based study indicated that SLE patients have 82% higher risk of infections and 61% increased risk of infection-related mortality compared to non-SLE controls. 3 Similarly, in 1953, an observational study of 583 rheumatoid arthritis (RA) patients revealed that 25% of the 137 deaths were due to infections. More recently, a matched case-control study comparing RA patients to the general population showed that RA patients have a 70% higher risk of infection. 1
Patients with ARDs are at risk for both minor and life-threatening infections. To prevent infections, it is crucial to implement screening, limit exposure to potential infection sources, and minimise the use of immunosuppressive agents, while effectively managing disease activity. This proactive approach is vital for patient safety. An independent cohort study 7 was recently conducted by the current authors to evaluate baseline immune parameters by comparing two groups: one with mild infections and the other with moderate to severe infections. The aim was to identify immune factors that may predict infection risk and to determine variables associated with morbidity and mortality over a one-year follow-up period. 1 Building on these previous findings that identified general predictors of infection, this study specifically focused on recognising patients who are more susceptible to severe and life-threatening infections.
The study aims to evaluate baseline immune parameters that predict the risk of severe infections in patients with ARDs. Specifically, it prospectively compares infection rates to identify key factors contributing to infection-related morbidity and mortality, which may help tailor immunosuppressive therapy.
Materials and Methods
Study Population
The prospective, observational study was carried out at a tertiary rheumatology centre in India from December 2019 to March 2022, focusing on adults with ARDs requiring escalated immunosuppressive therapy. Escalation was defined as an increase in mycophenolate dosage, the addition or switching over to cyclophosphamide or rituximab, or an increase in steroid doses. Eligible participants had well-controlled comorbidities like hypertension or diabetes, as long as these did not significantly affect their daily life. Exclusions were made for patients at higher risk of infection, those unable to communicate, individuals with other immunodeficiencies, or those with hepatitis B/C, HIV, or pregnancy. Informed consent was obtained from all participants, and ethical approval was granted.
Sample Size Calculation
The study targeted a sample size of 100 for a preliminary exploratory investigation, with the intention of forming approximately two groups. Sample size was calculated based on the ‘rule of 12’ for pilot studies. 8
Data Collection
Baseline immune parameters were assessed at the time of recruitment, prior to the escalation of immunosuppressive therapy, using a comprehensive panel of tests. This included a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) levels. Serum immunoglobulin levels (IgA, IgM, IgE, and IgG) were measured, and complement components C3 and C4 were quantified using turbidometry. Cellular immune markers such as CD4, CD3, CD8, CD19, and CD56 were analysed using flow cytometry to evaluate immune cell populations. Immunisation status was determined by measuring anti-HBs (hepatitis B surface antibodies) and Rubella IgG levels. Additionally, virological assessments were performed for cytomegalovirus (CMV), herpes simplex virus (HSV), Epstein-Barr virus (EBV), and varicella-zoster virus (VZV) by analysing IgM and IgG antibodies for each virus.
Patients were followed for one year to track episodes of infection, treatments, and hospitalisations, whether at the study centre or elsewhere. Participants were categorised based on their diagnoses (SLE, systemic sclerosis, or other conditions), and parameters were evaluated accordingly. During the follow-up period, participants were categorised into five groups based on the Common Terminology Criteria for Adverse Events (CTCAE): (a) those with mild, asymptomatic, or no infections requiring no treatment; (b) those with moderate infections requiring minimal local or non-invasive interventions; (c) those with severe infections that were medically significant but not immediately life-threatening; (d) those requiring hospitalisation or experiencing life-threatening infections; and (e) those who died from an infectious cause. 9 To examine factors influencing the risk of severe infections, patients were grouped into two categories. Group 1 included individuals with mild to moderate infections; Group 2 included patients from the remaining categories, classified as having severe infections.
The immunoglobulin levels (IgA, IgG, IgM, IgE), T-cell markers (CD3, CD4, CD8), CD19, CD56, complement levels (C3, C4), haemoglobin, white blood cell count (WBC), platelet count, and neutrophil-to-lymphocyte ratio (NLR) were categorised based on reference levels as normal, low, or high. NLR, ESR, and CRP were classified as normal, high, or significantly high. For Rubella, HSV (1 and 2), CMV, and EBV, IgG and IgM levels were classified as positive or negative, and participants were grouped into four categories: not infected, infected but not active, reactivated, and acute infection.
For VZV, participants were categorised based on whether their infection was active or inactive, and anti-HBs titres were classified as either reactive or non-reactive. Rheumatoid factor (RF), anti-CCP, ANA, and ANA profile antibodies were recorded as positive or negative. The use of steroids and immunosuppressive therapy was documented and analysed between the two groups.
Statistical Analysis
Data collection and organisation were carried out using MS Excel (Version 2409 Build 16.0.18025.20030). Descriptive statistics were employed to analyse participants based on their disease diagnoses, with a focus on predicting severe infections that necessitated hospitalisation, as well as fatal infections. Categorical variables were expressed as percentages, while continuous variables were reported as mean ± SD.
For continuous data, ANOVA was utilised, whereas categorical data were evaluated using chi-square tests, t-tests, and Fisher’s exact tests, all conducted in SPSS version 21. Ordinary least squares (OLS) regression was applied for predictive analysis, and the results were documented accordingly. Odds ratios and relative risks were calculated for participants with mild, moderate, or no infections compared to those with severe infections or mortality. A regression table was generated using Python code in Jupyter Notebook (version 6.5.4), and OLS regression analysis was conducted for all variables as well as for each significant variable individually.
Results
The study initially enrolled 106 patients, of whom 4 were excluded due to complications not related to infections during the 3-month follow-up. Consequently, 102 patients were included in the final analysis. The cohort had a mean age of 38. 21 ± 12.73 years and a mean follow-up duration of 13.1 ± 8.35 months. None of the participants had received any vaccinations other than routine childhood immunisations.
Before enrollment, 32 patients were on methotrexate (MTX), 30 on mycophenolate mofetil (MMF), 71 on hydroxychloroquine (HCQ), 71 on moderate-dose steroids, and 16 on biologic treatments. After recruitment, 69 patients received rituximab (RTX) at doses of 1-2 g/day, 7 received escalating doses of MMF (2-3 g/day), and 70 were treated with high-dose steroids (>1 mg/kg body weight). Diagnoses included 58 patients with SLE, 4 with RA, 18 with systemic sclerosis, 7 with myositis, 6 with ANCA-associated vasculitis, 3 with Sjögren’s syndrome, and 10 with other unclassified connective tissue diseases (Supplementary Table S1). RTX was administered for underlying autoimmune rheumatologic indications, including SLE, RA, scleroderma, myositis, ANCA-associated vasculitis, Sjögren’s syndrome, CTD, overlap syndromes, and other related conditions (Supplementary Table S2).
Key findings showed that severe infections or mortality were associated with older age (OR: 1.050), indicating a 5% increase in risk per year of age. Among immunoglobulin levels, low IgM (OR: 4.500) and low IgG (OR: 5.036) showed a potentially elevated risk, but with borderline significance. A low CD4 count (OR: 6.855) and a low CD4/CD8 ratio (OR: 2.625) were also associated with a higher risk of severe infections or mortality. Additionally, positive anti-HBs titres were linked to severe outcomes (OR: 3.750). Low platelet counts (OR: 3.865) and a high NLR (OR: 3.870) were linked to increased risk. In terms of medications, none showed significant associations except for steroid use (P = .036). These findings emphasise that age, certain immune markers, and inflammatory responses are key indicators of infection severity or mortality risk (Table 1). The baseline values for all the variables are provided in Supplementary Table S3.
Significant Variables (P < .05) Identified by Comparison Between Patients With Mild, Moderate, or No Infections and Those With Severe Infections or Death.
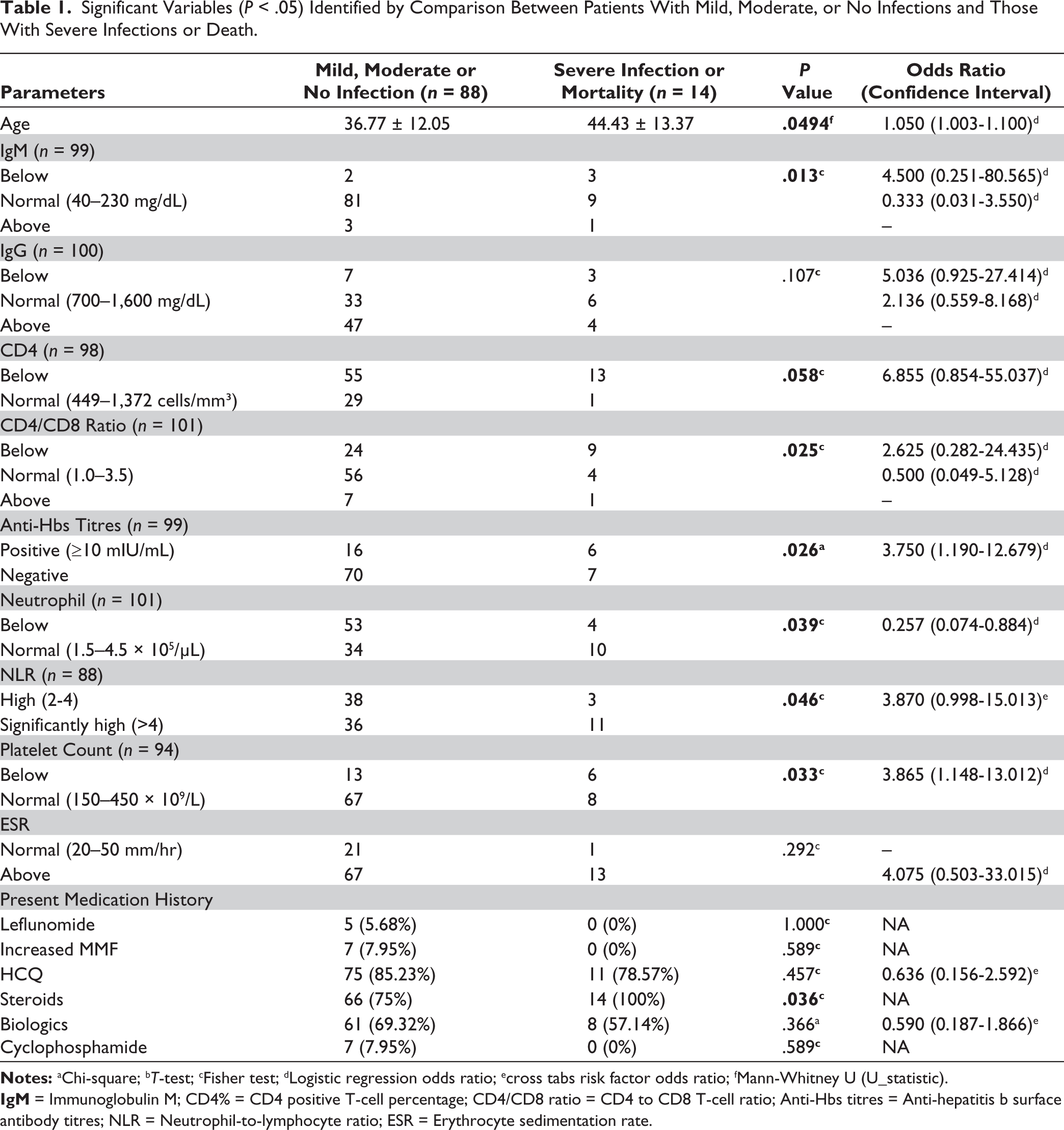
No significant differences were observed in immune markers such as CD8 count, total lymphocyte count, CRP, complement levels (C3 and C4), rheumatoid factor (RF), and anti-nuclear antibody (ANA) titre. Similarly, treatment-related factors, including immunosuppressive therapy, biologics, NSAIDs, and other immunological parameters such as NK cells and Rubella-specific IgG, also showed no notable differences. Additionally, no significant differences were found for HSV, EBV, haemoglobin, WBC, neutrophils, lymphocytes, IgA, IgE, IgG, IgM, CD3, CD19, or NK cells (Supplementary Table S3).
Mild, asymptomatic, or no infections occurred in 71 patients; moderate infections were observed in 15 patients, and severe infections that were medically significant but not immediately life-threatening occurred in 2 patients. Infections requiring hospitalisation or considered life-threatening were seen in 6 patients, and 8 patients died due to infectious causes. Infections were clinically categorised, including bacterial, viral, and fungal types. Microbiological confirmation was partial; some aetiologies were unascertained. Multiple infections occurred in certain patients, reflecting real-world biologic therapy practice (Supplementary Table S4).
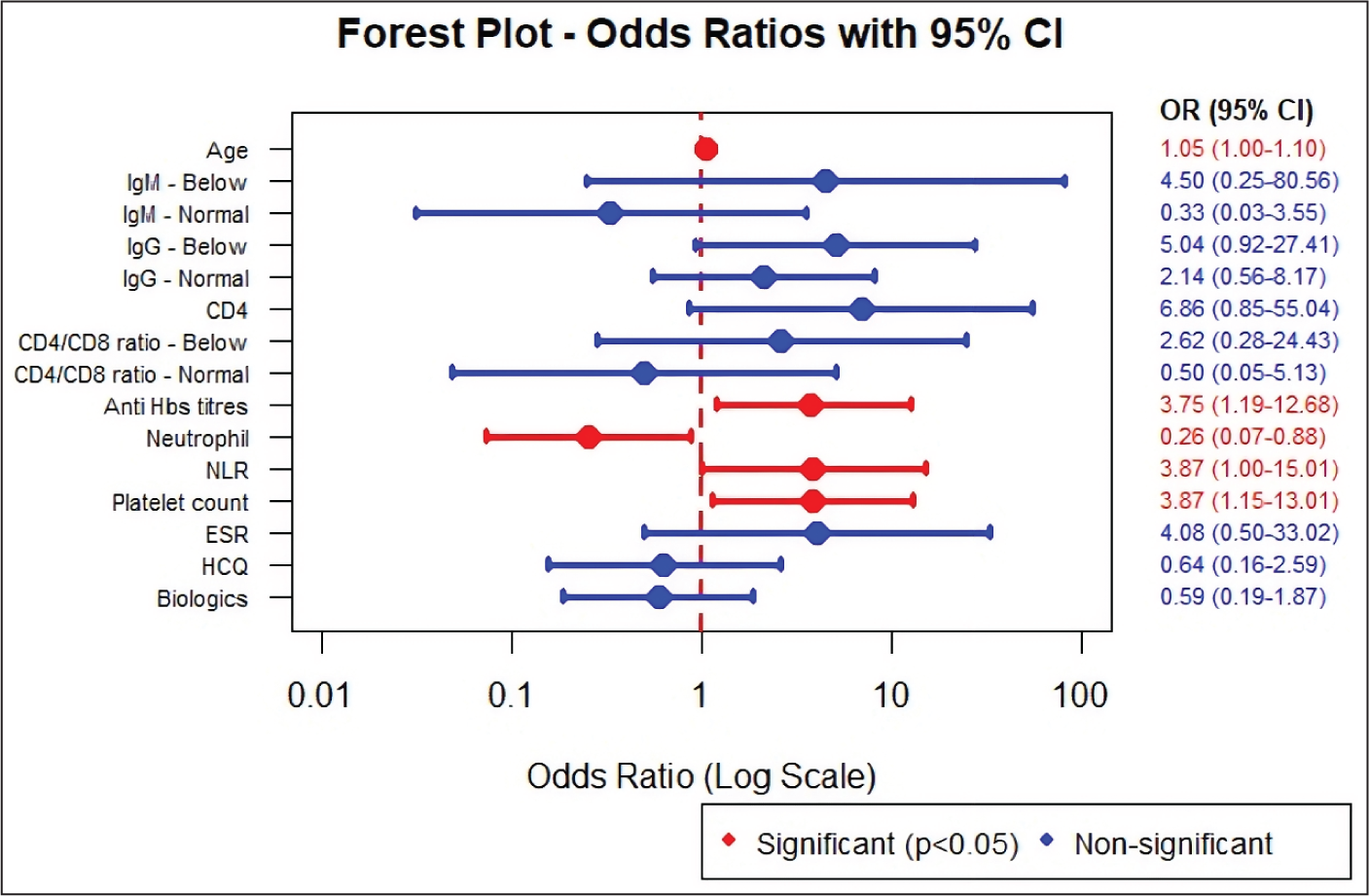
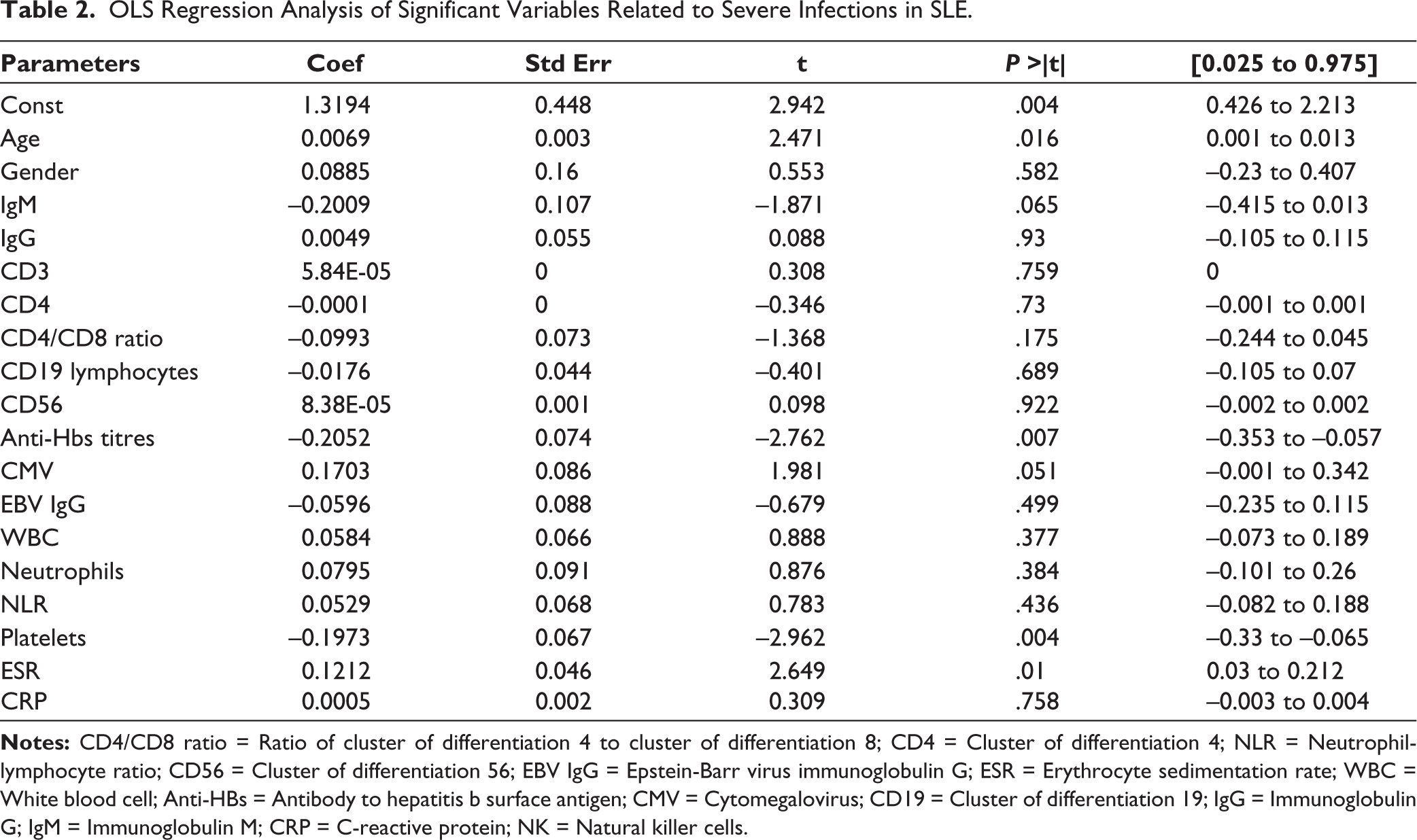
The Bonferroni correction was initially considered for this study, but was not applied due to its overly conservative nature. Instead, the Bonferroni-Hochberg and FDR corrections were implemented, yielding a value of 0.006. Furthermore, the relationships between predictive factors were examined using odds ratios and regression analysis. The majority of the results remained consistent across these methods, with all findings being statistically significant. The significance of the Bonferroni-Hochberg and FDR values indicates that the results are robust, holding true under both conservative and more flexible error control approaches, thereby enhancing the reliability of the findings. OLS regression analysis identified key predictors of severe infections, including age, IgM levels, CD4/CD8 ratio, anti-HBs titres, CMV antibodies, platelet count, and ESR (Table 2). A Forest plot of odds ratios with 95% confidence intervals is provided in Figure 1.
Forest Plot Depicting Odds Ratios with 95% Confidence Intervals.
OLS Regression Analysis of Significant Variables Related to Severe Infections in SLE.
Discussion
The study findings suggest that moderate and severe infections in patients with ARDs share overlapping but distinct risk profiles. Common predictors for both moderate and severe infections included older age, low IgG levels, thrombocytopenia, elevated NLR, and steroid use. 7 Severe infection or mortality was additionally linked to low IgM, reduced CD4 count, low CD4/CD8 ratio, positive anti-HBs titres, and elevated ESR. These findings suggest a broader spectrum of immunological dysfunction and possible immune exhaustion in patients with life-threatening infections.
The current study also reaffirmed that advancing age is a significant independent risk factor for infections, a trend consistently observed across various ARDs. Previous studies by Doran et al., Salmon et al., and Favalli et al. have similarly shown that older adults with ARDs, including RA, are at an elevated risk of severe infections and related complications. 10 The present study identified low IgM as a predictive factor for severe infection risk. Daniel E. Furst also reported similar findings. Sustained, very low levels of immunoglobulins, particularly IgM, are significant predictors of infection risk in ARDs. Specifically, patients with IgM levels below 20 mg/dL for extended periods experience an increased risk of recurrent and potentially life-threatening infections. 11 In contrast, Almaghlouth et al. found that low IgG and low IgM levels do not show the same degree of association with infection risk. 12
The current study identified elevated NLR and ESR, and low platelet count as significant predictors of severe infections in patients with ARDs. These findings align with existing literature highlighting the diagnostic and prognostic value of haematological markers in systemic inflammation and infection. Gasparyan et al. emphasised the clinical utility of haematologic indices, particularly NLR, as indicators of disease activity, neutrophilic inflammation, infectious complications, and severe organ damage in SLE. NLR has demonstrated strong predictive value in rheumatic diseases where neutrophilic inflammation predominates. 13
Similarly, ESR serves as a valuable marker in identifying patients at risk of severe infections. Supporting this, Hou et al. found a correlation between elevated ESR levels and infection risk in SLE, while Zahra et al. demonstrated that ESR is a reliable indicator for osteomyelitis in diabetic patients.14,15 In addition, thrombocytopenia has emerged as a critical marker of poor prognosis. Chen et al. reported that low platelet counts in SLE patients were significantly associated with higher mortality and end-organ damage, with an odds ratio of 4.57 (95% CI: 2.28-9.17; P < .001). 16
According to the current study findings, a low CD4% and a reduced CD4/CD8 ratio are associated with an increased susceptibility to severe infections in patients with ARDs. These observations are supported by previous studies. Ng et al. identified lymphopenia as a significant risk factor for major infections in Chinese patients during the early stages of SLE. 16 Similarly, a univariate analysis by Merayo-Chalico et al. revealed lymphopenia as one of the independent risk factors for severe infections in SLE. 17
Although not statistically significant in the current study, lower CD19 lymphocyte counts were associated with a potential 40% increase in the risk of severe infections. However, the predictive value of B-cell counts remains controversial. Lazarou et al. found that pre-therapy B-cell counts are not reliable indicators of infection risk. 18 In contrast, Heusele et al. observed that SLE patients with a history of serious infections were older, had comorbid diabetes, lower CD19 counts, and frequently received their first rituximab infusion while on high-dose prednisone. 19
The present study suggests that positive anti-HBs titres may be associated with a lower risk of serious infections in patients with SLE and related connective tissue diseases, while elevated CMV antibodies may indicate an increased risk. 20 Tsai et al. observed significantly higher counts of CMV-infected leukocytes in deceased individuals (P = .013), suggesting a critical association between CMV reactivation and poor outcomes in immunocompromised populations. 21 Although not all patients in the present study had evidence of active CMV infection, the presence of elevated CMV antibody titres may reflect an underlying state of immunological dysfunction.
The finding that steroid use was significantly associated with severe infections reinforces the need to minimise corticosteroid exposure whenever possible. The results also support the importance of tailoring immunosuppressive regimens based on individual immune status rather than applying a uniform escalation strategy. Similarly, Ruiz-Irastorza et al. indicated that the risk of major infections in patients with SLE is primarily influenced by treatment. Prednisone, even at moderate doses, raises the risk of infections, whereas antimalarials provide a protective effect. 22
As a pilot study, this research provides a comprehensive analysis of immune parameters and clinical data to identify factors associated with severe infections in patients with ARDs. The incorporation of these predictors into clinical decision-making has the potential to improve patient management and reduce infection-related morbidity and mortality. Notably, baseline immune profiling, particularly measurements of immunoglobulin levels and T-cell subsets, may help clinicians identify patients at higher risk. This, in turn, enables the consideration of alternative treatment strategies or the implementation of closer monitoring prior to initiating potent immunosuppressive therapies such as rituximab or high-dose corticosteroids. The one-year follow-up period further adds value by allowing comprehensive monitoring of infection episodes, treatment responses, and hospitalisation rates, thereby strengthening the applicability of the findings to both inpatient and outpatient settings.
Machine learning models, including Random Forest, Gradient Boosting, Support Vector Machine (SVM), and deep learning, have demonstrated high accuracy in predicting infections in immunocompromised patients using clinical and immunological data. Existing risk calculators, such as risk, Injury, Failure, Loss, End-stage renal disease (RIFLE), Clinical Risk Index for Babies II (CRIB-II), and modified sepsis scores, incorporate related biomarkers that align with those identified in the current study, enhancing predictive performance.23–26
However, several limitations must be acknowledged. The single-centre design may limit the generalizability of results to broader and more diverse populations. The modest sample size (n = 102) may have limited the statistical power to detect subtle associations. As this was an observational study, causality cannot be inferred, and unmeasured confounders may have influenced the outcomes. Variability in immunosuppressive regimens prior to enrollment further complicates the interpretation of infection risk in relation to baseline immune parameters. Additionally, the absence of detailed dosage data for immunosuppressants restricts the ability to evaluate dose-response effects. No significant differences were observed in steroid dosing between groups, and the small sample size limited meaningful dose-related analyses. Furthermore, the absence of systematic polymerase chain reaction (PCR) testing for viral infections restricted comprehensive identification and characterisation of these infections, potentially affecting the accuracy of infection risk stratification. Although participants were followed for an average of 12 months, this timeframe may not fully capture long-term infection risk. Additionally, the clinical significance of certain markers, such as IgM levels, in predicting severe infections warrants further investigation in larger, prospective cohorts.
Conclusion
The study highlights the importance of vigilant monitoring and preventive strategies for ARD patients with identified risk factors, including older age, low IgM and IgG levels, reduced CD4 count, low CD4/CD8 ratio, elevated NLR, thrombocytopenia, and high ESR. Positive anti-HBs titres, while typically considered protective, showed an unexpected association with increased infection risk in this immunocompromised population, suggesting altered immune dynamics that warrant further investigation. Developing AI-driven algorithms and predictive models based on these biomarkers could enhance individualised risk stratification and support tailored treatment planning.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Research Assist (http://www.research-assist.com) for their support in editing the manuscript and conducting the statistical analysis.
Authors’ Contribution
S. Chandrashekara and Prakruthi J contributed to the study design and conceptualisation. Renuka Panchagnula supervised the laboratory component of the study. All authors contributed to data collection, patient recruitment and manuscript preparation. S. Chandrashekara provided overall guidance for the study. All authors had access to the data and approved the final version of the manuscript.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This observational study was conducted in accordance with the principles of the Declaration of Helsinki and the ICMR National Ethical Guidelines for Biomedical and Health Research involving Human Participants (2017). The study received approval from the Scientific Review Board and Institutional Ethics Committee (IEC-CRICR/SN-122/015/2020).
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the APLAR Research Grant 2020.
Informed Consent
Written informed consent was obtained from all participants prior to their inclusion in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.