
Abstract
Objective/Aim:
Sustained remission (SR) has become increasingly achievable in rheumatoid arthritis (RA), but the optimal strategy for abrupt tapering or discontinuing conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) remains uncertain. This study aimed to compare relapse outcomes following csDMARD abrupt tapering versus discontinuation in RA patients maintaining SR and to identify potential predictors of relapse.
Methods:
We conducted a retrospective cohort study of 101 RA patients fulfilling the 2010 American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) classification criteria and maintaining SR defined as a Disease Activity Score in 28 joints using C-reactive protein (DAS28-CRP <2.6 for ≥12 months) on csDMARD monotherapy between January 2019 and January 2024. Patients were categorised into abrupt tapering (n = 40; a single-step 50% dose reduction) and discontinuation (n = 61) groups. Patients were followed for a median of 48 months (interquartile range [IQR]: 24–70 months) to assess relapse. Relapse was defined as DAS28-CRP >2.4 confirmed within four weeks. Kaplan-Meier and Cox regression analyses assessed relapse-free survival and predictors of relapse. Propensity score matching was applied to minimise confounding.
Results:
During a median 48-month follow-up, relapse occurred in 44 patients (43.6%): 16 (40.0%) in the abrupt tapering group and 28 (45.9%) in the discontinuation group (P = .55). Relapse-free survival did not differ significantly (hazard ratio [HR], 1.18, 95% CI 0.64–2.18, P = .60). No demographic, serologic or disease-related factor independently predicted relapse.
Conclusions:
Abrupt tapering and discontinuation of csDMARD monotherapy yielded comparable relapse outcomes in RA patients maintaining SR. These findings suggest that relapse risk is governed more by immunologic stability than by the de-escalation method. Patient preference and shared decision-making can guide csDMARD withdrawal in clinical practice.
Introductıon
Rheumatoid arthritis (RA) is a systemic autoimmune inflammatory disease that primarily affects the joints, leading to progressive disability, premature mortality and substantial socioeconomic burden.1,2 Advances in diagnostic criteria, therapeutic agents and treatment strategies have made disease remission an attainable goal for many patients. Early treatment initiation, regular monitoring and rigorous treat-to-target approaches have enabled a growing proportion of RA patients to achieve and maintain sustained remission (SR). Consequently, an increasing number of asymptomatic individuals continue long-term therapy with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), either as monotherapy or in combination with other agents.
In accordance with recommendations from the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR), csDMARD de-escalation (tapering or discontinuation) may be considered in patients who maintain SR. However, the optimal de-escalation strategy remains uncertain, as reflected in the conditional nature of current guideline recommendations.3–6 While numerous studies have explored tapering of biologic DMARDs, 7 a significant evidence gap persists regarding csDMARD de-escalation, particularly in direct comparisons between tapering and complete discontinuation under real-world conditions. A recent systematic review underscored the lack of head-to-head studies comparing these approaches, highlighting that clinical decisions are frequently driven by physician preference rather than high-quality evidence.8,9
DASs, particularly the Disease Activity Score in 28 joints using C-reactive protein (DAS28-CRP), are well-established measures to assess remission and to guide de-escalation decisions. 10 Yet, it remains unclear whether tapering provides superior protection against relapse compared with discontinuation in patients in SR. Furthermore, the identification of reliable predictors of relapse after de-escalation remains elusive. Prior studies have proposed potential associations between seropositivity, disease duration and baseline disease activity and the risk of relapse11,12; however, results have been inconsistent. This uncertainty complicates clinical decision-making and underscores the need for a personalised approach to csDMARD de-escalation.
The present retrospective cohort study aimed to compare relapse outcomes between csDMARD tapering and discontinuation strategies in RA patients in SR and to identify clinical, demographic and serologic predictors of relapse.
Materıals and Methods
Study Design and Population
This retrospective cohort study included 101 patients with RA in SR who underwent csDMARD de-escalation between January 2019 and January 2024 at the outpatient rheumatology clinics of two different hospitals. Patients were assigned to either an abrupt tapering group (n = 40) or a discontinuation group (n = 61) based on physician judgement in a real-world clinical setting. To mitigate potential selection bias arising from the non-randomised design, robust statistical adjustments, including propensity score matching and multivariable regression analyses, were performed.
All participants met the 2010 ACR/EULAR classification criteria for RA 13 and fulfilled the definition of SR, characterised by a DAS28-CRP <2.6 maintained for ≥12 months while on csDMARD monotherapy. This definition was chosen for its established use in both clinical practice and research, facilitating the inclusion of a cohort representative of patients typically considered for treatment de-escalation. De-escalation was defined as either (a) abrupt tapering, defined as a single-step dose reduction to 50% of the maintenance dosefor methotrexate (MTX; from 20 mg/week to 10 mg/week), leflunomide (LEF; from 20 mg/day to 10 mg/day) and sulfasalazine (SSZ; from 2 g/day to 1 g/day), maintained for at least six months; or (b) discontinuation, defined ascomplete cessation of csDMARD therapy without prior tapering. For consistency, remission status was also verified using the more stringent ACR/EULAR Boolean remission criteria in prespecified sensitivity analyses to test the robustness of the primary outcomes. 14
Exclusion Criteria
Patients were excluded if they: Received concurrent csDMARD combination therapy, were on biologic or targeted synthetic (b/ts) DMARDs at de-escalation, used chronic corticosteroids (CS) (>5 mg/day prednisolone equivalent), had another inflammatory rheumatic disease, underwent de-escalation for reasons other than SR such as toxicity, surgery, pregnancy), or had irregular follow-up preventing reliable outcome assessment.
Additionally, patients with prior csDMARD switches or previous b/ts DMARD exposure were included if such therapies had been discontinued well before baseline and patients were in SR on csDMARD monotherapy at the time of de-escalation. Patients were followed for relapse over a median period of 48 months (IQR: 24–70 months).
Data Collection
Demographic variables (age, sex, body mass index, family history of RA, smoking status [never, former, current]), laboratory parameters (erythrocyte sedimentation rate, CRP at diagnosis and during de-escalation, rheumatoid factor [RF] and anti-citrullinated protein antibody [ACPA] serostatus) and disease-related variables (symptom duration, time to diagnosis, time to remission, DAS28-CRP) were extracted from medical records. Treatment-related variables included csDMARD type, adherence (defined as uninterrupted use for at least three months before de-escalation), 15 previous bDMARD and CS use. Extra-articular manifestations such as interstitial lung disease, rheumatoid nodules, episcleritis and pleural effusions were also recorded.
Outcomes
The primary outcome was disease relapse, defined as a DAS28-CRP score >2.4, in line with Outcome Measures in Rheumatology (OMERACT) RA Flare Group recommendations, 16 and confirmed within four weeks to minimise misclassification due to transient fluctuations. Time to relapse was measured from the date of de-escalation initiation.
Statistical Analysis
All analyses were conducted using International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 28.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as medians with interquartile ranges (IQRs) and compared using the Mann-Whitney U test, while categorical variables were expressed as frequencies and compared using the chi-square or Fisher’s exact test, as appropriate. Relapse-free survival was analysed using Kaplan-Meier curves and compared with the log-rank test. Cox proportional hazards regression models were used to identify predictors of relapse. Variables with P < .10 in univariate analyses were entered into multivariable models. Missing data were addressed using a complete-case approach and patients lost to follow-up were right-censored at their last visit.
Propensity scores were estimated using logistic regression, with treatment group (tapering vs. discontinuation) as the dependent variable and age, sex, symptom duration, RF and ACPA status, baseline DAS28-CRP and csDMARD type as covariates. Nearest-neighbour 1:1 was performed with a calliper width of 0.2 times the standard deviation of the logit of the propensity score. Covariate balance was assessed using standardised mean differences, with values <10% indicating adequate balance. Additional sensitivity analyses employing inverse probability weighting and subgroup analyses were conducted to evaluate the robustness of findings. A post hoc power analysis demonstrated that the study had 80% power to detect a hazard ratio (HR) of 1.5 at a two-sided alpha of 0.05.
The study protocol was approved by the Ethics Committee of İstanbul Physical Medicine and Rehabilitation Education and Research Hospital (protocol number: 2025-11; approved March 6, 2025). Due to the retrospective design involving only the analysis of anonymised medical records, the ethics committee waived the requirement for individual written informed consent.
Results
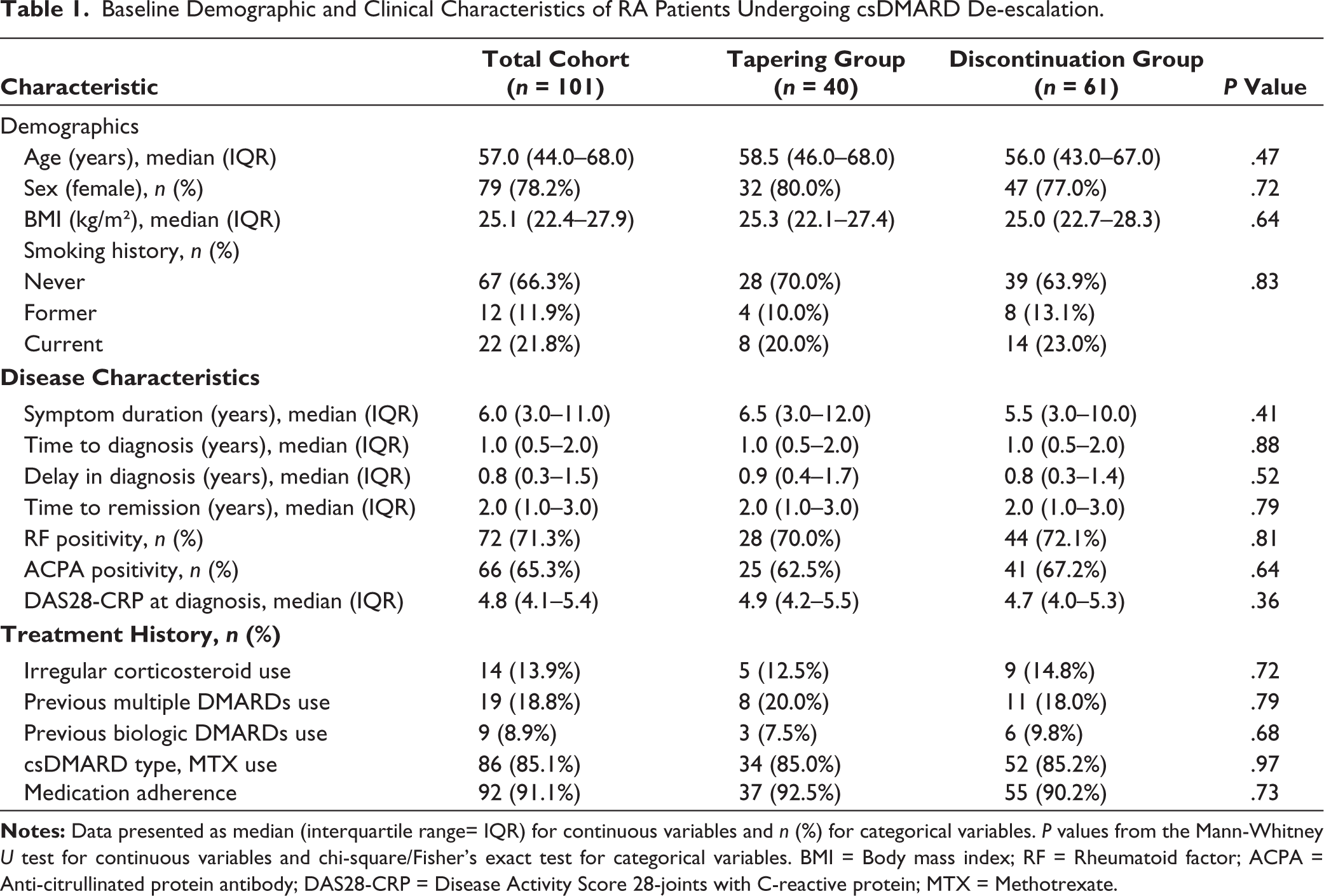
A total of 101 RA patients in SR who underwent csDMARD de-escalation were included in the final analysis. Patients were divided into abrupt tapering (n = 40, 39.6%) and discontinuation (n = 61, 60.4%) groups. Baseline demographic and clinical characteristics were comparable between groups, with no significant differences in age, disease duration or baseline DAS28-CRP (all P > .05; Table 1). The median age was 59 years (IQR 49–67) and 91.1% were female. Median symptom duration was six years (IQR 4–11). Seropositivity rates were 71.3% for RF and 65.3% for ACPA and MTX was the most frequently used csDMARD (85.1%).
Baseline Demographic and Clinical Characteristics of RA Patients Undergoing csDMARD De-escalation.
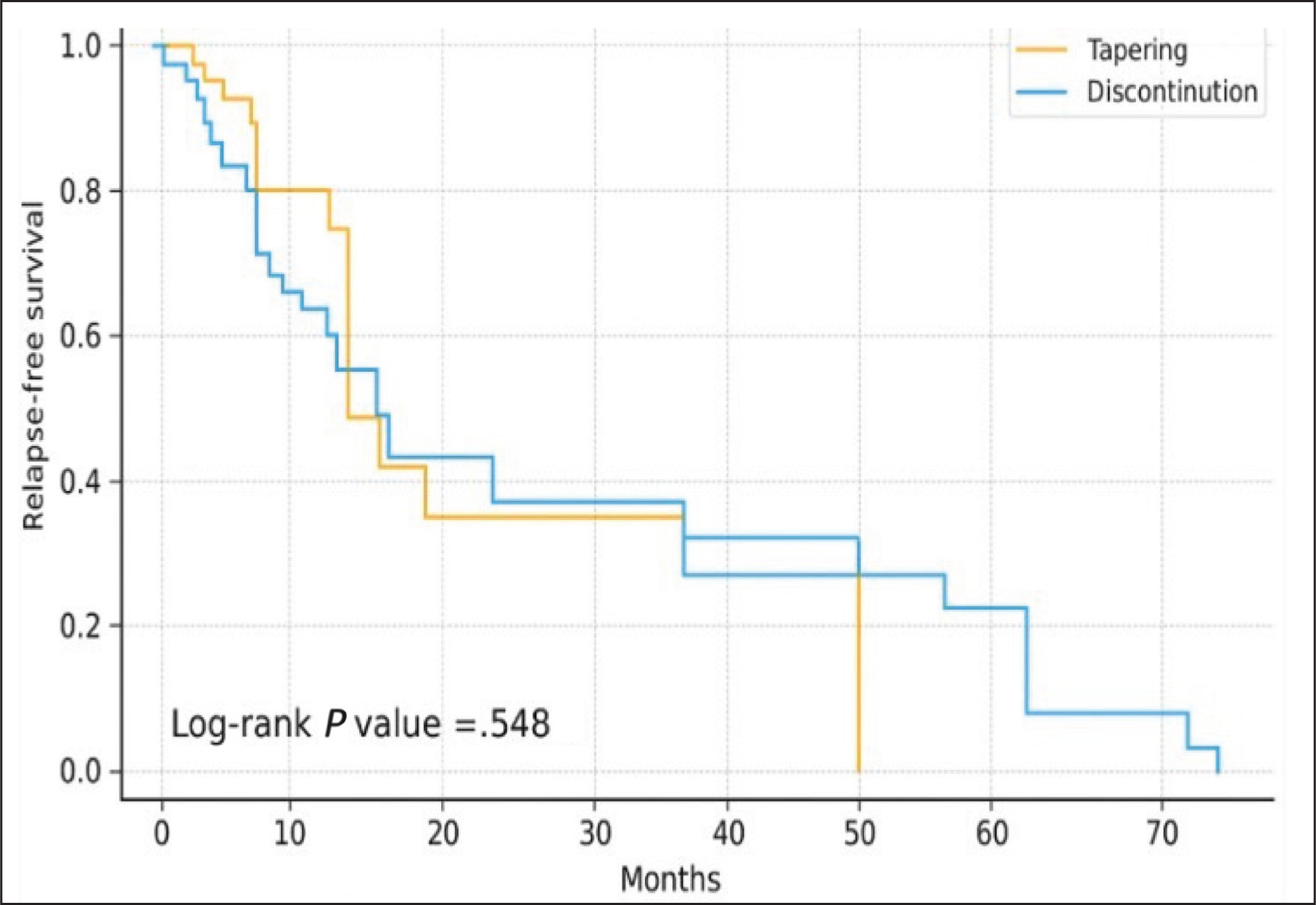
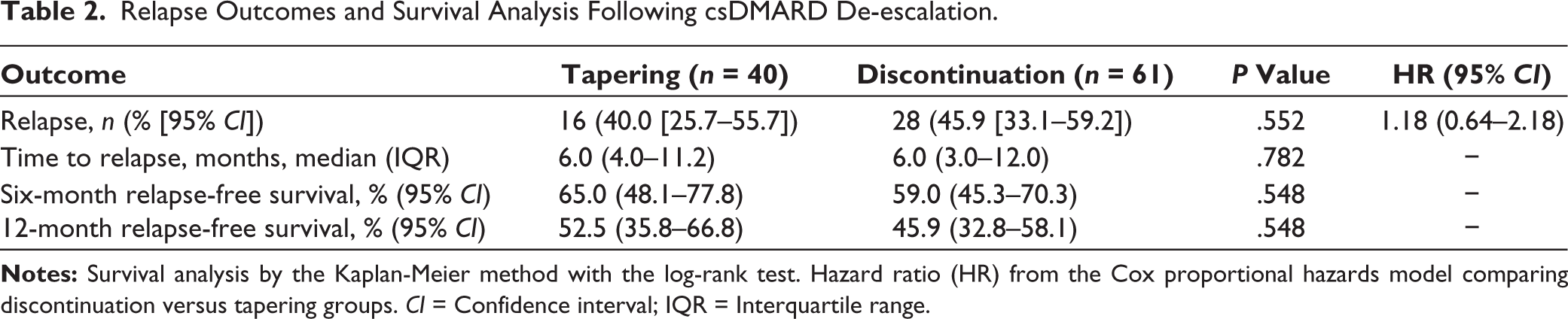
During a median follow-up of 48 months (IQR: 24–70 months), 44 patients (43.6%) experienced disease relapse, 16 (40.0%) in the abrupt tapering group and 28 (45.9%) in the discontinuation group (P = .552). Relapse outcomes and survival analyses following csDMARD de-escalation are presented in Table 2. Median time to relapse was 6 months in both groups (IQR, 4–11.2 vs. 3–12.0 months, P = .782). Kaplan-Meier analysis showed no significant difference in relapse-free survival between strategies (log-rank P = .548; Figure 1). The 6- and 12-month relapse-free survival rates were 65.0% and 52.5% for tapering and 59.0% and 45.9% for discontinuation, respectively.
Kaplan-Meier Curves Showing Relapse-free Survival in RA Patients Undergoing csDMARD De-escalation via Abrupt Tapering Versus Discontinuation Strategies (log-rank P = .548).
Relapse Outcomes and Survival Analysis Following csDMARD De-escalation.
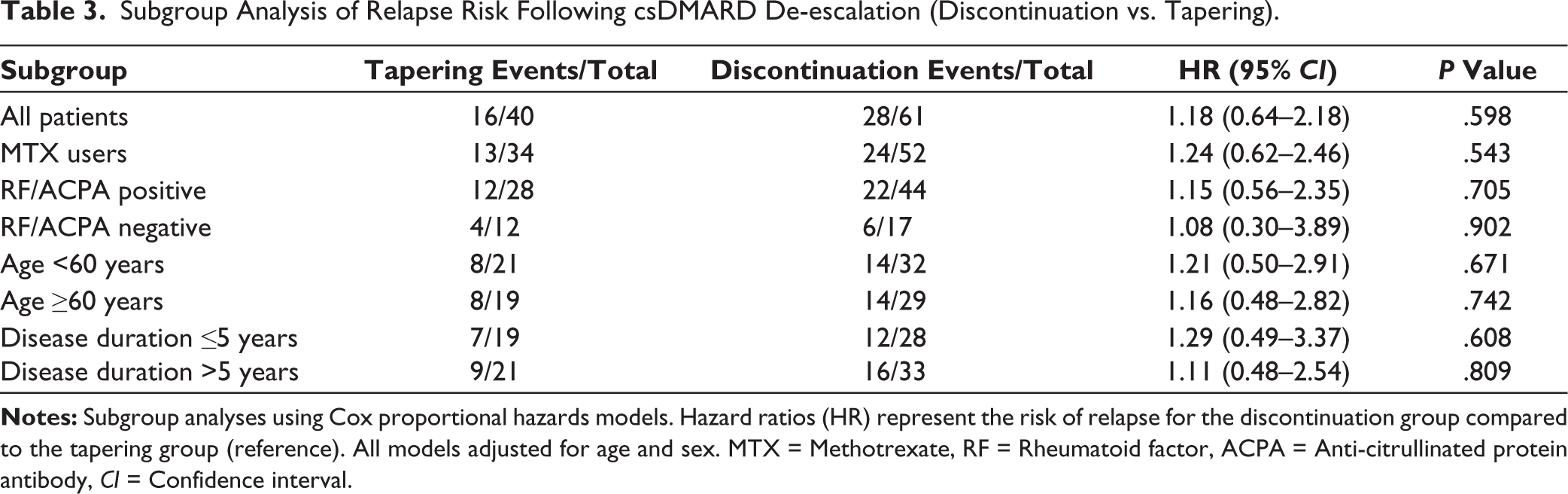
In Cox regression analysis de-escalation strategy was not associated with relapse risk (HR, 1.18, 95% CI 0.64–2.18, P = .598) and none of the covariates including age, sex, seropositivity or baseline DAS28-CRP, emerged as independent predictors (Table 3). Neither time to diagnosis (OR 1.03, 95% CI 0.93–1.15, P = .547) nor time to remission (OR 1.01, 95% CI 0.91–1.12, P = .838) predicted relapse risk. In a post-hoc analysis prompted to address the differential efficacy of specific csDMARDs, we directly compared outcomes between patients de-escalated while on MTX versus SSZ monotherapy. Among the 39 patients in the MTX subgroup, 32 (82.1%) maintained SR after abrupt tapering, compared to 30 of 37 patients (81.1%) in the SSZ subgroup. This difference was not statistically significant (P = .91). In extended analyses assessing disease timeline variables, neither time to diagnosis (OR 1.03, 95% CI 0.93–1.15, P = .547) nor time to remission (OR 1.01, 95% CI 0.91–1.12, P = .838) predicted relapse risk. Subgroup analyses stratified by seropositivity, csDMARD type and disease duration yielded consistent results (all P > .05).
Subgroup Analysis of Relapse Risk Following csDMARD De-escalation (Discontinuation vs. Tapering).
Propensity score matching produced 32 well-balanced pairs (standardised mean differences <0.1). A sensitivity analysis excluding the six patients with prior biologic DMARD exposure yielded consistent results. In the bDMARD-naïve cohort (n = 95), relapse rates remained comparable between the tapering (17.9%, 5/28) and discontinuation (17.2%, 11/64) groups (P = .931). In this matched cohort, relapse risk remained comparable between groups (HR 1.12, 95% CI 0.58–2.16, P = .732). Sensitivity analyses using inverse probability weighting confirmed these findings (HR 1.15, 95% CI 0.62–2.13, P = .661). In logistic regression analysis addressing ACPA role, ACPA positivity alone was not significantly associated with relapse risk (OR 0.68, 95% CI 0.26–1.76, P = .429).
Dıscussıon
This retrospective cohort study shows that abrupt tapering produced relapse outcomes comparable to those seen with discontinuation in RA patients who achieved SR on csDMARD monotherapy. The primary finding, which was consistent in sensitivity and subgroup analyses, not only contrasts with the prevailing therapeutic paradigm that often favours tapering over discontinuation4,6 but also challenges the basic tenet that tapering is intrinsically superior. This finding offers solid empirical support for medication de-escalation strategies in this growing population of patients maintaining SR.17,18
A potential explanation for this finding is thatduring long-term remission, the stability of the underlying immunological condition may be a more important predictor of relapse than the pharmacokinetic profile of the drug being withdrawn. From a biological perspective, this may indicate that csDMARDs do not essentially reset the abnormal immune response in RA, but rather sustain remission by inhibiting inflammatory activity. 19 Therefore, the probability of relapse may be more controlled by the pre-existing, patient-specific immunological ‘set-point’ than by the de-escalation technique once the suppressive effect is eliminated, whether gradually or suddenly.19,20
The practically identical relapse-free survival curves between the tapering and discontinuation groups, as well as the lack of a significant difference in relapse rates (40.0% vs. 45.9%), suggest that the stability of remission itself may be more important than the protocol of csDMARD withdrawal. This finding is consistent with the increasing amount of research indicating that treatment continuation may not provide further benefits after a certain point of immunological quiescence.17,18,21 Our findings’ external validity is supported by the fact that our total relapse rate of 43.6% is within the 30%–60% range documented in earlier prospective and retrospective studies.17,18 The equivalence between strategies, however, contrasts with some earlier studies that found gradual tapering reduced the likelihood of flares.22,23 Such discrepancies could be the result of variations in the depth of remission and patient selection. The current study focused exclusively on patients maintaining SR on csDMARD monotherapy, which may represent a biologically more stable subgroup. Previous studies often included patients on combination or biologic therapies, who may have residual subclinical inflammation and thus a higher propensity for relapse after stopping treatment.4,19 Direct comparison is further complicated by variations in follow-up duration, remission definitions and tapering techniques among studies.
A key secondary finding was the absence of identifiable clinical or serological predictors of relapse. Our multivariable analysis found no relationships with seropositivity, longer duration of disease or higher baseline disease activity, which have been highlighted as potential predictors in previous reports.4,24,25 The lack of conventional clinical and serological markers to predict relapse is particularly noteworthy in this study. This implies that the clinical phenotype of ‘SR’ can be a point of convergence where traditional prognostic predictors lose their ability to discriminate. The lack of association between disease timeline variables (time to diagnosis and time to remission) and relapse risk further supports the concept that once deep SR is achieved, the predictive utility of these conventional clinical markers may diminish. A concept supported by emerging translational data on immune modulation during pharmacologic remission supports the idea that achieved immunologic quiescence under csDMARD therapy creates a state of ‘secondary immune tolerance’ that temporarily overrides the innate aggressiveness associated with seropositive disease.19,25 This finding raises the possibility that recurrence risk may be controlled by more subtle immunological or molecular processes, as traditional clinical indicators may lose their prognostic utility once deep and SR is attained. The robustness of our conclusion is further supported by the consistency of our findings across all predefined subgroups, including those stratified by age, disease duration and serostatus. Interestingly, since seropositive patients are typically thought to have more aggressive illness and worse prognostic outcomes, the lack of a significant link in this group is remarkable. 20 One possible explanation is that prolonged immune modulation through csDMARDs may induce partial immune tolerance, thereby diminishing the clinical distinction between seropositive and seronegative phenotypes in the context of remission. Moreover, even when analysed independently as suggested by current literature, ACPA status alone did not emerge as a significant predictor of relapse in our cohort, further underscoring the limited prognostic utility of conventional serologic markers in the specific context of de-escalation from SR. Emerging evidence from translational studies supports this hypothesis, demonstrating that regulatory T-cell restoration, decreased synovial macrophage activity and normalisation of cytokine networks occur during pharmacologic remission.19,25 However, clinical indices such as the DAS28-CRP might not accurately reflect these immunologic equilibria.
Furthermore, a post-hoc analysis investigating the potential confounding effect of differential csDMARD efficacy yielded an unexpected insight. The comparable rates of SR after tapering between patients on MTX and those on SSZ suggest that within the specific context of maintaining deep, SR, the initial efficacy hierarchy of csDMARDs may become less relevant. This observation aligns with and reinforces our primary conclusion: Achieving a prolonged state of immunologic quiescence may create a common biological threshold where the risk of relapse upon de-escalation is determined more by the stability of this acquired state than by the specific pharmacologic properties or initial potency of the background csDMARD.19,20 It further supports the concept that ‘SR’ itself could be a phenotypic and immunologic convergence point that temporarily overrides traditional prognostic markers, including the choice of csDMARD monotherapy.
Our findings carry direct implications for clinical decision-making. In the absence of a clear superiority for either strategy, the decision between abrupt tapering and discontinuation can be guided based on patient preference, shared decision-making and pragmatic considerations. Discontinuation, for example, may be a reasonable and effective goal for a patient who is worried about long-term drug toxicity or who has difficulties in medication adherence, especially since it falls within the scope of guideline recommendations to consider de-escalation in SR.4,5 On the other hand, even though a tapering strategy has not been shown to be more effective, it might be the better choice for a psychologically anxious patient who values a sense of control. This effectively ‘democratises’ the de-escalation process, empowering clinicians and patients to choose the path that best aligns with individual values and circumstances, without compromising the clinical outcome.
While our study was sufficiently powered to detect a large clinically significant difference (HR ≥ 1.5) based on a priori sample size calculation, a modest but potentially important difference between strategies could still exist. 26 For example, a subtle benefit of tapering in a specific, yet unidentified, patient subgroup might have been undetected. Furthermore, our operational definition of tapering as a 50% dose reduction, even though it is standardised, does not capture the full spectrum of tapering protocols used in real-world practice, such as more gradual dose reductions or interval lengthening. This may affect the generalisability of our findings. Third, while we excluded patients using b/ts DMARDs at baseline, some included patients had past bDMARD exposure. Although a sensitivity analysis excluding these patients confirmed our primary results, we cannot define a precise washout period from the available data. Most importantly, the retrospective, non-randomised design, despite robust statistical adjustments including propensity score matching, remains susceptible to unmeasured confounding factors, 27 such as subtle differences in physician mindset or unrecorded patient characteristics that influenced the initial choice of de-escalation strategy.
To move the field beyond the ‘no difference’ paradigm, future research must focus on stratifying patients by their underlying biological relapse risk. We propose a shift in the research question from ‘Which de-escalation strategy is better?’ to ‘Which strategy is better for which patient?’ Prospective studies should systematically incorporate advanced biomarkers such as ultrasonographic synovitis, multi-omics profiles such as transcriptomics and proteomics) or detailed immunophenotyping of peripheral blood and/or synovial tissue collected at the time of de-escalation. The goal should be to develop a precision medicine toolkit that can identify the ‘safe stoppers’ who can discontinue therapy with minimal risk from the ‘obligate relapsers’ who require continued treatment, irrespective of the de-escalation method. Hence, future research integrating synovial or serological biomarkers could elucidate the biological underpinnings of relapse after csDMARD de-escalation.20,28
Conclusıon
In RA patients maintaining SR on csDMARD monotherapy, the method of treatment de-escalation, whether through tapering or discontinuation, appears to be less consequential than the underlying stability of the immunological state itself. These findings liberate clinical decision-making from a one-size-fits-all approach, positioning patient preference and individual context as the primary guides for de-escalation. The critical task for the future is no longer to identify the superior strategy, but to develop the precision medicine tools capable of distinguishing patients who can safely stop therapy from those who require continued treatment, thereby moving from a paradigm of universal de-escalation to one of personalised withdrawal.
Footnotes
Acknowledgements
We acknowledge Fatih Yıldırım, MD, for the contribution of a biostatistical consultant for reviewing the statistical analyses and methodology used in this study.
Authors’ Contribution
NK conceived and designed the study, performed data collection and statistical analysis and drafted the manuscript.
HH contributed to study design refinement, data interpretation and critical manuscript revision for important intellectual content.
Both authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Availability of Data and Materials
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Consent for Publication
Not applicable; this study does not contain any identifiable individual data or images.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval and Consent to Participate
This retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Committee (protocol No. 2025-11). Due to the retrospective design involving the analysis of anonymised medical records, the requirement for individual written informed consent was waived by the ethics committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.