
Abstract
Rheumatic and musculoskeletal diseases (RMDs) are an escalating cause of disability in India, a burden managed by a critically limited specialist workforce. This imbalance, particularly in non-urban settings, contributes to diagnostic delays and suboptimal outcomes. Artificial intelligence (AI) is increasingly explored as a decision-support tool with the potential to augment clinical capacity across the continuum of rheumatology care. This narrative review synthesises contemporary evidence to examine the current landscape of rheumatology services in India and to outline key AI paradigms relevant to clinical practice. We discuss emerging applications in diagnostic support, disease monitoring and workflow optimisation, while critically examining limitations related to model interpretability through the lens of retrieval-augmented generation architectures. Significant implementation challenges remain, including fragmented health data, medico-legal uncertainty under the Digital Personal Data Protection Act, 2023 and the ‘prediction-reasoning gap’, wherein AI systems may produce correct outputs via clinically unsound reasoning pathways. We propose a calibrated vision for AI not as an autonomous authority, but as a supervised ‘algorithmic colleague’ that complements clinical expertise, supported by investments in representative data infrastructure and clinical AI literacy tailored to the Indian context.
Keywords
List of Abbreviations
ABDM: Ayushman Bharat Digital Mission
ACR: American College of Rheumatology
AI: Artificial Intelligence
DL: Deep Learning
DPDP Act: Digital Personal Data Protection Act
EHR: Electronic Health Record
LLM: Large Language Model
ML: Machine Learning
RAG: Retrieval-augmented Generation
RMSE: Root Mean Square Error
RMDs: Rheumatic and Musculoskeletal Diseases
SDoH: Social Determinants of Health
The Current Landscape: Rheumatological Care in India
Disease Burden: Rheumatic and Musculoskeletal Diseases in India
Rheumatic and musculoskeletal diseases (RMDs) are a silent epidemic in India, inflicting a heavy toll of chronic pain and disability. Though often overshadowed in public health discourse by communicable diseases and metabolic syndromes, their cumulative impact is staggering. Foundational studies estimated the prevalence of rheumatoid arthritis (RA) in the adult Indian population to be approximately 0.75%. 1 More recent and alarming data from the Global Burden of Disease (GBD) database, analysing trends from 1990 to 2021, reveal that India experienced the most rapid growth in RA incidence globally during this period. 2 This finding is compounded by data showing India not only registered the highest age-standardised mortality rate from RA by 2021 but, with over 1.3 million cases, also carries the world’s second-highest absolute number of elderly RA cases.2,3
As a significant and growing contributor to disability, RMDs rank among the top causes of years lived with disability (YLDs) in India, imposing a substantial burden on the population.4,5 RMDs trigger catastrophic health expenditure and significant loss of productivity, establishing them as a pressing national health priority.2,6,7
Access to Rheumatology Care: Delayed Diagnosis and Specialist Shortage
The immense and growing burden of RMDs is met with a stark and alarming reality: A severe shortage of qualified rheumatologists. A recent report from the Global Rheumatology Summit indicates there are fewer than one rheumatologist for every one million people in India. 8 This national average, while dire, masks an even more critical issue of distributional inequity. The vast majority of rheumatologists are concentrated in Tier-1 and Tier-2 metropolitan centres, creating a care vacuum for the nearly 70% of the Indian population residing in rural and semi-urban areas.8,9
This manpower chasm creates a vicious cycle of delayed diagnosis. Patients in remote areas often see non-specialists, missing the therapeutic window to prevent irreversible joint damage. 10 This ‘diagnostic odyssey’ can result in a median diagnostic delay of 18 months, primarily due to referral lags from primary care. 11 Consequently, patients often reach rheumatologists with established deformities and functional impairment, requiring more complex interventions and facing poorer outcomes. 12
Systemic Hurdles: Data Fragmentation and the Leapfrog Opportunity
Beyond the manpower crisis, several systemic hurdles impede effective rheumatological care, including low public awareness and the high cost of advanced therapies.6,13 Underpinning these challenges is the infrastructural problem of data fragmentation. Most encounters are documented on paper and existing Electronic Health Records (EHRs) are typically proprietary, non-interoperable silos.14,15 This chaotic data ecosystem cripples large-scale research, national registries and the deployment of data-driven technologies like AI. 15
However, this weakness presents a paradoxical opportunity. Having largely sidestepped the cumbersome, institution-centric EHRs of Western systems, India can ‘leapfrog’ directly to an agile, mobile-first, cloud-based ecosystem. 16 Leveraging its high mobile penetration and initiatives like the Ayushman Bharat Digital Mission (ABDM), India can build its digital health infrastructure on modern, AI-native platforms, reframing a historical weakness into a strategic advantage. 17
The Rise of the Algorithmic Colleague: AI Paradigms for Clinical Medicine
Search Strategy
This narrative review is based on a comprehensive literature search conducted to synthesise evidence on the application of AI in the Indian rheumatology context. The search was performed across several electronic databases, including PubMed/MEDLINE, Scopus, IEEE Xplore and supplementary searches via Google Scholar, to capture a wide range of medical, computer science and health policy literature. The search was supplemented by a review of pre-print servers such as arXiv and medRxiv for the latest research and targeted searches of government and institutional websites for relevant policy documents and reports.
The search strategy was initially conducted up to mid-2025 and subsequently updated with key publications identified through targeted alerts and reference tracking, employing a combination of keywords and Medical Subject Headings (MeSH) where applicable. Search terms were grouped into three core domains: (a) Clinical context: ‘rheumatology’, ‘rheumatoid arthritis’, ‘musculoskeletal diseases’, ‘healthcare delivery’, ‘workforce shortage’, AND ‘India’; (b) Technological concepts: ‘artificial intelligence’, ‘machine learning’, ‘deep learning’, ‘large language models’, ‘generative AI’, ‘retrieval-augmented generation’, ‘RAG’; and (c) Implementation and ethical issues: ‘algorithmic bias’, ‘data fragmentation’, ‘interoperability’, ‘Electronic Health Records’, ‘DPDP Act’, ‘medico-legal’, ‘ethics’, ‘prediction-reasoning gap’, ‘data colonialism’, ‘AIFORALL’. These domains were combined using Boolean operators (AND/OR) to refine the search results.
Inclusion criteria were peer-reviewed articles, pre-prints, government reports and policy documents published in English. The reference lists of key articles were also manually reviewed to identify additional relevant sources. No strict date limitations were applied to the initial search to include foundational epidemiological and policy documents, though a preference was given to literature published in the last decade to ensure currency.
The central thesis of this review is the vision of AI as an ‘algorithmic colleague’. While the concept of human-AI collaboration forming a ‘hybrid decision-making entity’ is an area of growing academic discourse, its application to the specific confluence of challenges in a low-resource, high-burden setting like Indian rheumatology remains underexplored. 18 This framework moves the discussion away from AI as a replacement for clinicians and towards a pragmatic, augmentation-focused model suited to the realities of Indian healthcare.
From Machine Learning to LLMs: Promise and Peril in Clinical AI
AI enables systems to perform human-like tasks, with machine learning (ML) and deep learning (DL) using algorithms to find patterns and make predictions.19,20 A recent paradigm shift is generative AI, particularly large language models (LLMs), which can generate new content and have shown high diagnostic accuracy.21,22 However, their use is perilous due to risks of ‘hallucinations’. 23 A 2025 analysis of legal AI tools found hallucination rates between 17% and 33%, a cautionary statistic for high-stakes medical fields. 24 Furthermore, the ‘prediction-reasoning gap’—where correct predictions arise from flawed logic—poses a risk of cognitive errors if clinicians rely on these tools blindly. 25
Retrieval-Augmented Generation (RAG): Foundations for Clinical AI
To mitigate these risks, RAG has emerged as a critical architecture for clinical AI. 23 Unlike standard LLMs that rely exclusively on pre-training, RAG systems retrieve contextually relevant information from trusted external knowledge bases—such as ACR or EULAR clinical practice guidelines—prior to generating responses, thereby grounding outputs in verifiable evidence and improving transparency.23,26
Recent evaluations have begun to quantify this safety advantage. In 2025, a public health-oriented study using the MEGA-RAG framework demonstrated a substantial reduction in hallucination rates compared with baseline LLMs, along with improved task-level performance metrics, supporting the role of retrieval-based grounding in safety-critical domains. 27
Similarly, in clinical radiology workflows, RAG-enhanced models were associated with markedly lower hallucination rates during contrast media consultation tasks when compared with non-retrieval-based language models, reinforcing the cross-disciplinary relevance of retrieval grounding for clinical safety. 28
While RAG is not a panacea and remains fundamentally dependent on the quality, currency and governance of its underlying knowledge sources, its ability to constrain generative outputs to traceable evidence represents a meaningful step toward safer clinical deployment. By effectively requiring the model to ‘show its work’, RAG currently represents the most plausible pathway for integrating LLMs into supervised, clinician-led clinical practice, with emerging architectures such as iterative and modular RAG offering further potential for improvement. 29
AI in the Rheumatology Clinic: Clinical Applications and Decision Support
The true value of AI in rheumatology lies in its potential to function as an ‘algorithmic colleague’, augmenting the clinician’s capabilities across the entire patient care journey rather than replacing human clinical judgement. 23
Augmenting Diagnosis: Automated Imaging and Early Arthritis Classification
In routine Indian practice, precise quantification of imaging findings is often constrained by time pressure and workforce limitations. In this context, AI has emerged as a pragmatic decision-support tool capable of automating standardised assessments while preserving clinician oversight.
Rheumatoid Arthritis (RA)
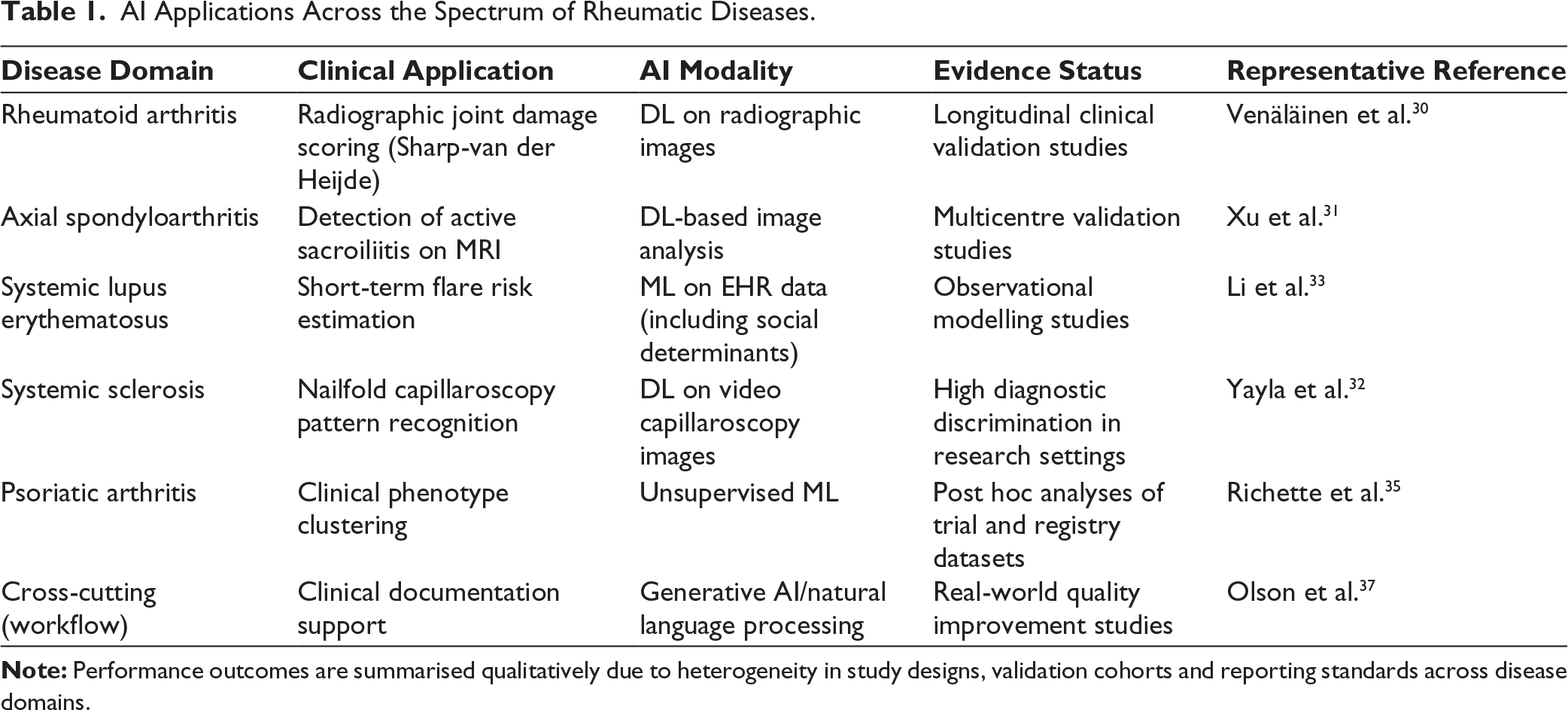
DL-based systems have demonstrated the ability to automatically quantify radiographic joint damage using established scoring frameworks such as the Sharp-van der Heijde score. Recent longitudinal validation studies have shown that AI-derived scores correlate closely with expert radiologist assessments and are sensitive to disease progression over time, supporting their potential role in monitoring structural damage in routine clinical care. 30
Axial Spondyloarthritis (axSpA)
For the detection of active sacroiliitis, convolutional neural network-based models applied to MRI have now been validated across multicentre cohorts. These systems demonstrate moderate-to-good sensitivity and specificity and, while not intended to replace subspecialist interpretation, can outperform non-specialist readers and function as effective triage or referral-support tools in settings with limited expertise. 31
Systemic Sclerosis (SSc)
AI-assisted analysis of nailfold video capillaroscopy has shown particularly strong performance, with DL models achieving excellent discrimination between early, active and late systemic sclerosis patterns. 32 The integration of such algorithms with low-cost imaging platforms holds promise for expanding screening and early disease recognition in underserved and rural populations.
Personalising Care: Predicting Treatment Response and Disease Flares
One of the most promising applications of AI in rheumatology is its potential to support a shift from reactive disease management toward more anticipatory, individualised care.
Systemic Lupus Erythematosus (SLE)
ML models leveraging longitudinal electronic health record data have demonstrated the ability to estimate short-term flare risk in patients with SLE. 33 Importantly, recent approaches have incorporated social determinants of health alongside clinical variables, acknowledging the influence of socioeconomic context on disease activity and outcomes—an aspect particularly relevant in heterogeneous populations such as India. In parallel, emerging studies suggest that physiological signals captured through wearable devices may show detectable deviations weeks before clinically overt flares, highlighting a potential role for remote monitoring in selected patients. 34
Psoriatic Arthritis (PsA)
Unsupervised ML techniques have been increasingly applied to address the clinical heterogeneity of PsA. Analyses of clinical trial and registry datasets have identified reproducible patient phenotypes characterised by differing patterns of skin, joint and systemic involvement. 35 These phenotypic clusters have been associated with variable therapeutic responses, suggesting a future role for data-driven stratification in guiding treatment selection rather than a uniform ‘one-size-fits-all’ approach.
Reclaiming Time: Documentation Support and Administrative Burden
One of the most immediate areas where AI may support rheumatology practice is in addressing the administrative workload that contributes to clinician fatigue and burnout, particularly in resource-constrained healthcare settings. 36
Ambient Clinical Documentation Support
So-called ambient clinical intelligence systems use natural language processing to capture clinician-patient conversations and generate draft clinical documentation for subsequent clinician review. 20 Recent real-world evaluations suggest that the introduction of such tools can reduce clerical burden and improve workflow efficiency. In a 2025 multicentre quality improvement study, the deployment of ambient AI scribes was associated with a measurable reduction in self-reported physician burnout over short-term follow-up, although causality and long-term sustainability require further study. 37 In high-volume Indian outpatient settings, where rheumatologists may see 50–60 patients per day, even modest reductions in documentation load could meaningfully improve workflow sustainability and clinician well-being.
System-level Analytics and Health System Planning
At a system level, AI-enabled analytics can aggregate clinical data to identify disease patterns, treatment gaps and regional variations in care delivery, supporting quality improvement and policy planning when aligned with national digital health frameworks. 15 In the Indian context, integration with initiatives such as the ABDM may enable actionable insights while preserving clinician-led governance. The major clinical applications of artificial intelligence across different rheumatic disease domains are summarised in Table 1.17,38
AI Applications Across the Spectrum of Rheumatic Diseases.
Implementation Challenges: AI Adoption in the Indian Context
While the promise of AI in rheumatology is compelling, its real-world implementation within the Indian healthcare system is constrained by multiple structural, ethical and regulatory challenges. A critical appraisal of these barriers is essential to ensure that AI deployment is responsible, equitable and clinically safe.
The Data Dilemma: Quality, Privacy and Linguistic Diversity
The principle of ‘garbage in, garbage out’ is foundational to ML. In India, the development of reliable clinical AI is hindered by three interrelated data challenges. First, health records remain fragmented, with a predominance of paper-based documentation and non-interoperable electronic health record systems, limiting the availability of high-quality, longitudinal datasets.14,15 Second, the Digital Personal Data Protection (DPDP) Act, 2023 introduces essential safeguards through consent requirements, purpose limitation and data minimisation, but also adds regulatory complexity for large-scale clinical data aggregation and secondary use.39,40 Third, India’s linguistic diversity—including widespread code-switching between English and regional languages—poses significant challenges for natural language processing models trained predominantly on Western corpora.14,15
Together, these factors necessitate the development of India-specific data infrastructures and governance frameworks that balance innovation with patient privacy and legal compliance.
The Trust Deficit: From ‘Black Boxes’ to the Prediction-reasoning Gap
Beyond data constraints, clinician trust represents a major barrier to clinical AI adoption. While many AI systems report high diagnostic accuracy, emerging evidence highlights a concerning ‘prediction-reasoning gap’, wherein correct outputs may be generated through flawed or clinically unsound reasoning pathways. 25 This limitation reinforces the need to conceptualise AI tools as decision-support systems requiring human validation, rather than autonomous decision-makers.
Of particular concern is the long-term educational impact of such systems. Over-reliance on opaque AI outputs risks ‘cognitive entrenchment’, especially among trainees, whereby clinical reasoning skills may be gradually eroded if AI recommendations are accepted uncritically. 41 Addressing this risk requires not only technical solutions such as explainable and retrieval-grounded models, but also formal integration of clinical AI literacy into postgraduate training.
Equity, Bias and the Risk of Digital Exclusion
A central ethical question for India is whether AI will reduce or exacerbate existing healthcare inequities. High-cost, proprietary AI solutions risk reinforcing a new digital divide if their benefits remain confined to urban, resource-rich settings. Additionally, algorithms trained primarily on Western populations may perform suboptimally in Indian patients due to differences in genetics, disease phenotype, environmental exposure and healthcare access. 42
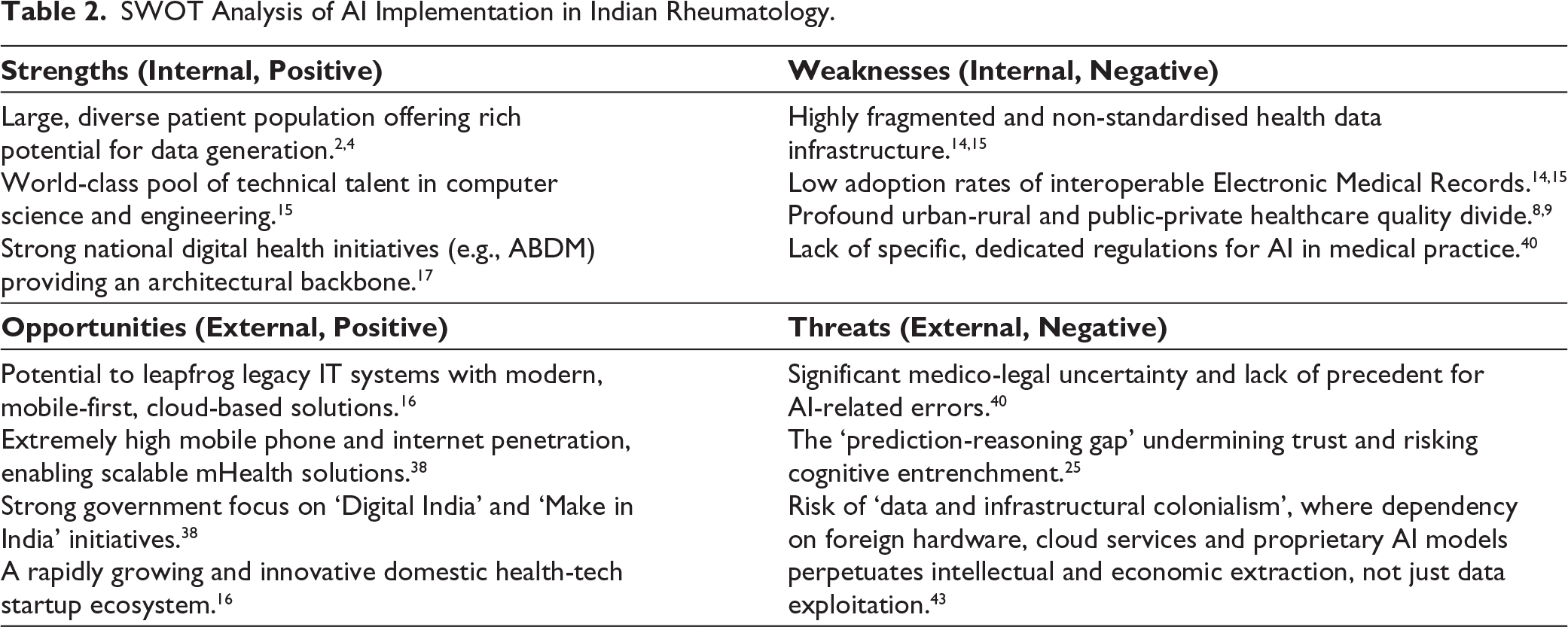
Mitigating algorithmic bias and ensuring equitable benefit will require the creation of diverse, representative Indian datasets. In this context, the establishment of a National Rheumatic and Musculoskeletal Disease (RMD) Registry is not merely a technical aspiration but an ethical imperative.17,43 Such an initiative would support transparent model development, local validation and sovereign data stewardship aligned with national digital health priorities. Key systemic and implementation challenges relevant to AI integration in rheumatology practice in India are outlined in Table 2.
SWOT Analysis of AI Implementation in Indian Rheumatology.
Conclusion: A Proactive Roadmap for an AI-augmented Future
The integration of AI into rheumatology practice in India should be viewed not as a technological inevitability, but as a socio-technical challenge requiring careful governance, clinical oversight and contextual sensitivity. Emerging evidence suggests that AI-enabled tools can meaningfully support diagnosis, risk stratification, documentation and system-level planning when deployed as supervised decision-support systems rather than autonomous authorities. Realising this potential will require a proactive roadmap centred on three priorities: the development of representative, sovereign clinical datasets; the incorporation of clinical AI literacy into medical education and specialist training; and the prioritisation of frugal, scalable innovations suited to resource-constrained settings. If pursued responsibly, the ‘algorithmic colleague’ can help bridge workforce gaps while reinforcing—rather than undermining—equity, clinical reasoning and patient-centred care in Indian rheumatology.
Footnotes
Acknowledgements
During the preparation of this manuscript, AI-assisted tools were used solely for language editing and clarity. All scientific content, interpretations and final decisions were made by the authors, who take full responsibility for the accuracy and integrity of the work.
Authors’ Contribution
Both authors contributed equally to the conception, drafting, critical revision and final approval of this manuscript.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration of AI Usage
AI–assisted tools (including LLMs) were used solely to support language editing, clarity and organisation of the manuscript. All scientific content, interpretations, clinical perspectives and final decisions regarding the manuscript were conceived, written and approved by the authors, who take full responsibility for the integrity and accuracy of the work.
Ethical Approval and Informed Consent Statements
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.