
Abstract
Introduction
Aromatase inhibitors (AIs) are widely used in the adjuvant treatment of hormone receptor-positive breast cancer but are frequently associated with musculoskeletal adverse effects, collectively termed AI-associated musculoskeletal syndrome (AIMSS). Tenosynovitis is a recognised but underreported manifestation and may significantly impact quality of life and treatment adherence.
Case Report
A 39-year-old woman with invasive ductal carcinoma of the left breast (ER/PR positive, HER2/neu negative, Ki-67 index 6%–8%) underwent neoadjuvant chemotherapy, followed by left modified radical mastectomy, adjuvant chemotherapy and radiotherapy. She was initiated on letrozole as part of adjuvant hormonal therapy.
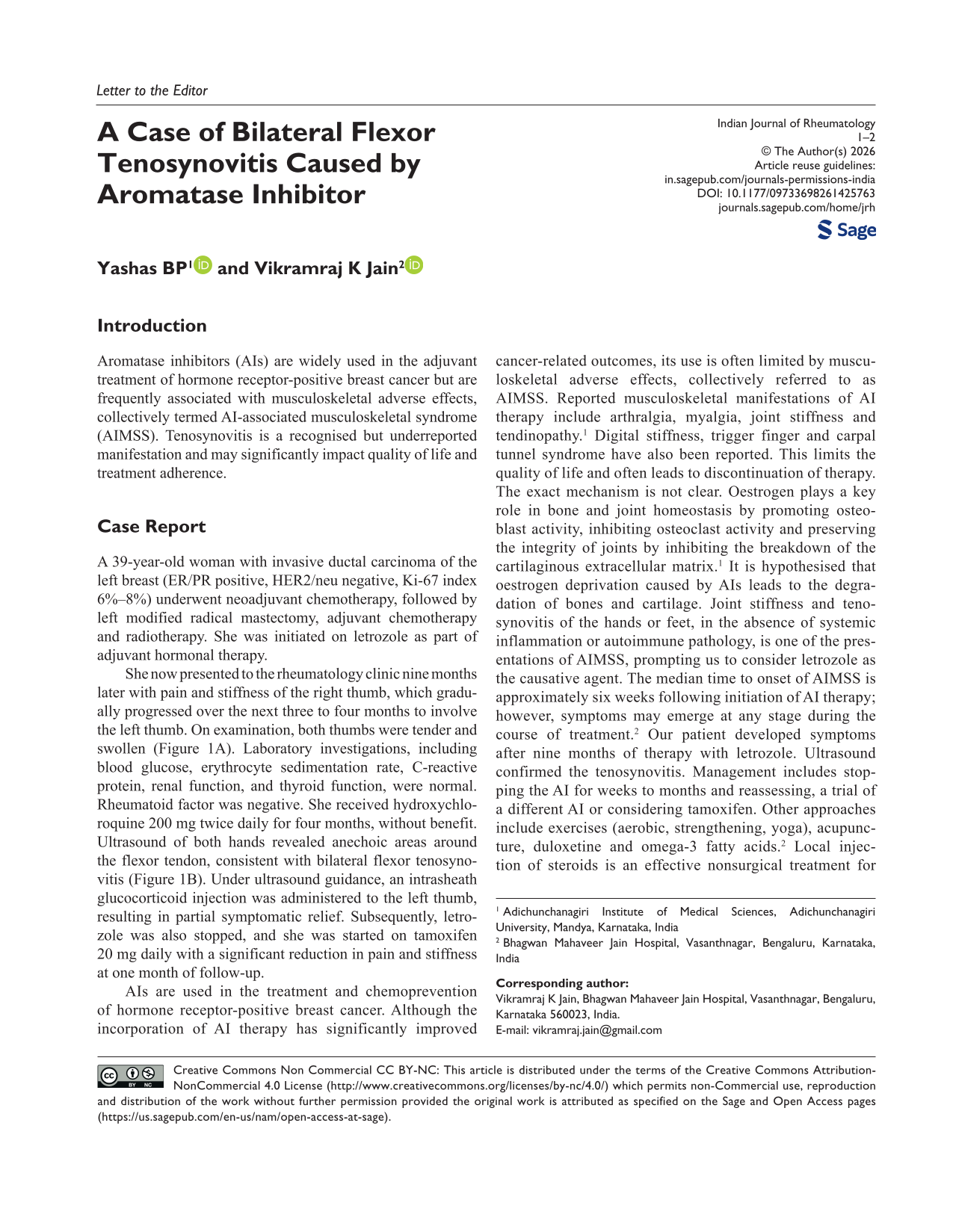
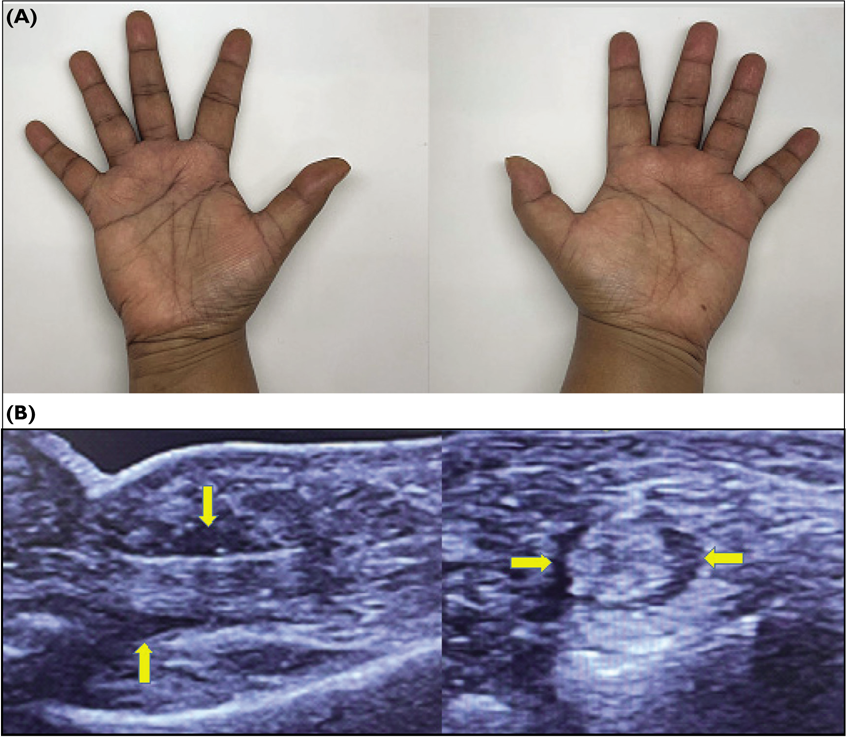
She now presented to the rheumatology clinic nine months later with pain and stiffness of the right thumb, which gradually progressed over the next three to four months to involve the left thumb. On examination, both thumbs were tender and swollen (Figure 1A). Laboratory investigations, including blood glucose, erythrocyte sedimentation rate, C-reactive protein, renal function, and thyroid function, were normal. Rheumatoid factor was negative. She received hydroxychloroquine 200 mg twice daily for four months, without benefit. Ultrasound of both hands revealed anechoic areas around the flexor tendon, consistent with bilateral flexor tenosynovitis (Figure 1B). Under ultrasound guidance, an intrasheath glucocorticoid injection was administered to the left thumb, resulting in partial symptomatic relief. Subsequently, letrozole was also stopped, and she was started on tamoxifen 20 mg daily with a significant reduction in pain and stiffness at one month of follow-up.
A (Top Panel): Photograph of Both Hands Showing Swelling in Both Thumbs; B (Bottom Panel): Longitudinal (Left) and Transverse View (Right) of the Flexor Tendon of Thumb Showing Anechoic Area Surrounding the Tendon (Yellow Arrows) on High-resolution Ultrasound (Frequency 16 MHz) Using Hockey Stick Probe (GE LOGIQ e).
AIs are used in the treatment and chemoprevention of hormone receptor-positive breast cancer. Although the incorporation of AI therapy has significantly improved cancer-related outcomes, its use is often limited by musculoskeletal adverse effects, collectively referred to as AIMSS. Reported musculoskeletal manifestations of AI therapy include arthralgia, myalgia, joint stiffness and tendinopathy. 1 Digital stiffness, trigger finger and carpal tunnel syndrome have also been reported. This limits the quality of life and often leads to discontinuation of therapy. The exact mechanism is not clear. Oestrogen plays a key role in bone and joint homeostasis by promoting osteoblast activity, inhibiting osteoclast activity and preserving the integrity of joints by inhibiting the breakdown of the cartilaginous extracellular matrix. 1 It is hypothesised that oestrogen deprivation caused by AIs leads to the degradation of bones and cartilage. Joint stiffness and tenosynovitis of the hands or feet, in the absence of systemic inflammation or autoimmune pathology, is one of the presentations of AIMSS, prompting us to consider letrozole as the causative agent. The median time to onset of AIMSS is approximately six weeks following initiation of AI therapy; however, symptoms may emerge at any stage during the course of treatment. 2 Our patient developed symptoms after nine months of therapy with letrozole. Ultrasound confirmed the tenosynovitis. Management includes stopping the AI for weeks to months and reassessing, a trial of a different AI or considering tamoxifen. Other approaches include exercises (aerobic, strengthening, yoga), acupuncture, duloxetine and omega-3 fatty acids. 2 Local injection of steroids is an effective nonsurgical treatment for stenosing tenosynovitis, such as trigger finger and De Quervain’s disease. Rheumatologists must be aware of possible drug-related adverse effects as a potential aetiology of flexor tenosynovitis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. The patient’s identity has been adequately anonymised, and confidentiality has been maintained.