
Abstract
Background:
India carries one of the world’s highest tuberculosis burdens, with nearly one-fourth of adults estimated to harbour tuberculosis infection (TBI). Consequently, patients with systemic inflammatory rheumatic diseases (SIRDs) receiving biological disease-modifying antirheumatic drugs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) are at significant risk of reactivation. The World Health Organization (WHO) has recently revised terminology; ‘latent TB infection’ (LTBI) is now termed TBI, while active disease continues as TB disease. Accordingly, WHO and India’s National TB Elimination Programme (NTEP) have updated TBI screening recommendations.
Objective:
This article provides India-specific clinical guidance for TBI screening before initiating b/tsdmards, considering high TB prevalence, universal Bacille Calmette-Guérin (BCG) vaccination, and limited national resources.
Methods:
This article summarises NTEP-endorsed screening tools-tuberculin skin test (TST), interferon-gamma release assays (IGRAs), chest radiography, and the newer Cy-Tb test-evaluating their performance, strengths, and limitations in immunomodulated patients.
Results:
TST remains inexpensive and accessible but is confounded by BCG-induced false positives and reduced sensitivity in immunosuppressed individuals. IGRAs offer greater specificity and single-visit convenience but are costly and infrastructure-dependent. Chest radiography remains essential to exclude active or prior TB. Emerging Indian data support Cy-Tb as a promising alternative. A tiered approach is recommended: (a) TST + chest X-ray in resource-limited settings; (b) IGRA alone in moderately resourced clinics; and (c) combined TST + IGRA + X-ray in tertiary centres or high-risk cases.
Conclusion:
Mandatory, resource-sensitive TBI screening before b/ts-DMARD therapy provides a practical, evidence-based strategy to prevent TB reactivation in Indian SIRD patients.
Abbreviations
Bacille Calmette-Guérin
Biologic or targeted synthetic disease-modifying antirheumatic drugs
Interferon-gamma release assays
Indian Spinal Injuries Centre-Joint Disease Clinic
Latent Tuberculosis Infection
India’s National Tuberculosis Elimination Programme
Systemic immunoinflammatory rheumatic diseases
Tuberculosis disease
Tuberculosis Infection
TB preventive therapy
Tuberculin skin test
The World Health Organisation
Introduction
Tuberculosis (TB) continues to be a major global health challenge, with India accounting for nearly one-fourth of the world’s TB burden.1,2 Beyond the millions of active TB cases, a much larger reservoir of infection lies in the form of tuberculosis infection (TBI), earlier called latent tuberculosis infection (LTBI). 3 According to the World Health Organization (WHO), a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifest active TB, should now be identified as TBI4-6; a change from the earlier term LTBI. 3 Accordingly, the NTEP, Government of India, has adopted this terminology and recommends its use in clinical practice. 7 The National TB Prevalence Survey (2019-2021) estimated that approximately 21%-22% of Indians aged >15 years harbour TBI, translating to more than 350 million individuals.2,8,9 This large reservoir of ‘TBI’ remains the source, not only for reactivation but also for ongoing transmission, more so in immunosuppressed individuals due to their disease itself or due to immunomodulator/immunosuppressive therapies.10,11 In rheumatology practice, the risk of TB reactivation is of particular concern. Patients with systemic inflammatory rheumatic diseases (SIRDs), such as rheumatoid arthritis, spondyloarthritis, and systemic lupus erythematosus, frequently require prolonged immunomodulatory/immunosuppressive therapy.12-15 It is to be noted that the introduction of biological disease-modifying antirheumatic drugs (bDMARDs) (such as inhibitors of tumour necrosis factor), and tsDMARDs (such as JAK inhibitors), has dramatically improved outcomes in SIRDs. However, these therapies are associated with an increased risk of reactivation of TBI, most notably with anti-TNF agents. 16 Therefore, screening for TBI is now recommended as a standard global practice to identify at-risk patients and prevent potential TB development before starting these medications.16-18 However, applying unmodified international recommendations for the TBI screening of Indian patients requires caution. This is because of the ‘Universal BCG vaccination’ programme in India, which is known to interfere with the interpretation of the most widely used test for TBI, namely, the tuberculin test (TST).19,20 Similarly, high prevalence of environmental mycobacteria in India (as well as reported from other countries) also makes the interpretation of the tuberculin test difficult.21-23 The often-used drugs bDMARDs also complicate test performance. 24 Furthermore, the choice between the TST and interferon-gamma release assays (IGRAs), and whether both should be performed, remains debated in India.25,26 Based upon these publications relevant to India, our article compares the diagnostic tools for TBI and proposes practical, resource-sensitive endorsements tailored for India.
Material and Method
Updated TBI guidelines from the WHO’s Global Tuberculosis Programme, and its ‘TB Knowledge Sharing Platform’, for the screening and treatment of TBI; Centres for Disease Control and Prevention (CDC, USA) for TBI guidelines (and its updates); and the Indian sources consisting of National Tuberculosis Elimination Programme (NTEP) and Ministry of Health and Family Welfare, Government of India, were referred for this purpose.7,9,27,28
Results
Available Screening Tests for TBI in India
Two main tests are currently recommended and used for the screening of TBI worldwide (including India): (a) the TST (an intradermal skin test) and (b) IGRAs. A chest radiograph is often used to exclude active TB and to detect prior infection.
Tuberculin skin tests (TST)
Screening for TBI using Purified Protein Derivative (PPD): Ministry of Health and Family Welfare (MoHFW) Government of India, recommends 1 TU PPD (RT23 with Tween-80 (Polysorbate 80; also called polyoxyethylene (20) sorbitan monooleate), standardised to approximate 5 TU PPD-S used in the USA.
7
Advantages of TST use: It is inexpensive, widely available and simple. It has a sensitivity of 60%-76%.
29
Disadvantages of TST use: It may give false-positive results because of prior BCG vaccination and environmental mycobacteria. Similarly, it can give false negative results in immunosuppression, requires highly skilled manpower to perform the test and read the result (induration in the skin), and therefore is highly operator-dependent. Additionally, the test requires two clinic/hospital visits. Cy-Tb test ‘Cy-Tb’ (Made in Serum Institute, Pune, India; included in NTEP).
7
This test offers high specificity in TBI diagnosis and addresses key drawbacks of TST and IGRAs. While applied and read like the TST,
30
Cy-Tb is based on ESAT-6 and CFP-10 antigens, the same targets as in IGRAs, making it highly specific.
29
Points in favour of Cy-Tb use: The test has high specificity, its performance is not affected by prior BCG vaccination, and it is cost-effective. It employs a universal 5 mm induration cut-off, irrespective of BCG or HIV status. Since the test is administered and interpreted in the same way as the traditional TST, no additional specialised training is required for healthcare workers. Points against Cy-Tb use: This test, like the Mantoux test, requires highly skilled manpower to perform the test and read the result (induration in the skin); therefore, it is highly operator-dependent. The test requires two clinic/hospital visits. Currently, this test is available only in hospitals associated with NTEP.
Interferon-gamma release assays (IGRAs)
Available in India: ‘QuantiFERON-TB Gold Plus’, ‘T-SPOT.TB’
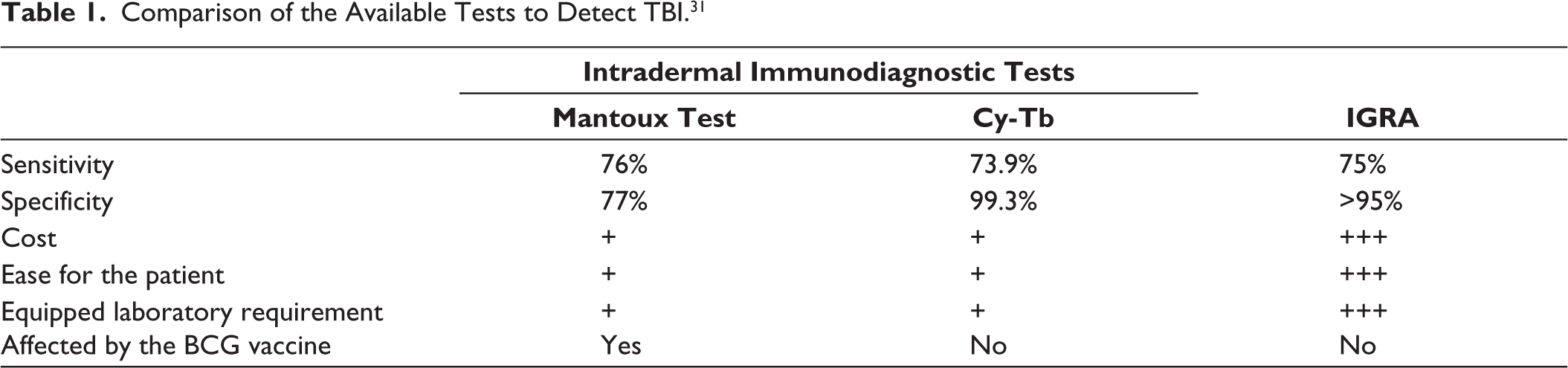
Table 1 provides a comparison of the three available tests.
Comparison of the Available Tests to Detect TBI. 31
Chest radiograph
Mandatory to rule out active TB and identify old healed lesions; findings require clinical correlation.
Additional details and comparison of the tests are given in Table 1:
Special considerations for use in patients with SIRDs
Immunosuppression: Glucocorticoids and DMARDs reduce TST sensitivity; IGRAs are less affected.
32
Anergy and PPD dose: Increasing PPD to 5-10 TU does not overcome anergy reliably and reduces specificity. Indian standard remains 1 TU PPD-RT23.
7
Dual testing: TST + IGRA improves sensitivity, recommended for high-risk patients. In a high burden country like India, combining TST and IGRA helps in increasing the predictive value for TB disease than either test alone, but only slightly. This minimal incremental predictive benefit of combining the two tests is not observed in low-burden countries.
33
Chest X-ray: Should be performed in all SIIRD patients before initiating b/tsdmards, regardless of test results.
International and National Guidance FOR THE SCREENING OF TBI:
WHO: Recommends TST, M. tuberculosis antigen-based skin tests (TBSTs), which use the same antigens as Cy-Tb, or IGRA for high-risk individuals; treat TBI after ruling out active disease (Table 2).
3
Populations Recommended for TBI Screening Across Major Guidelines.
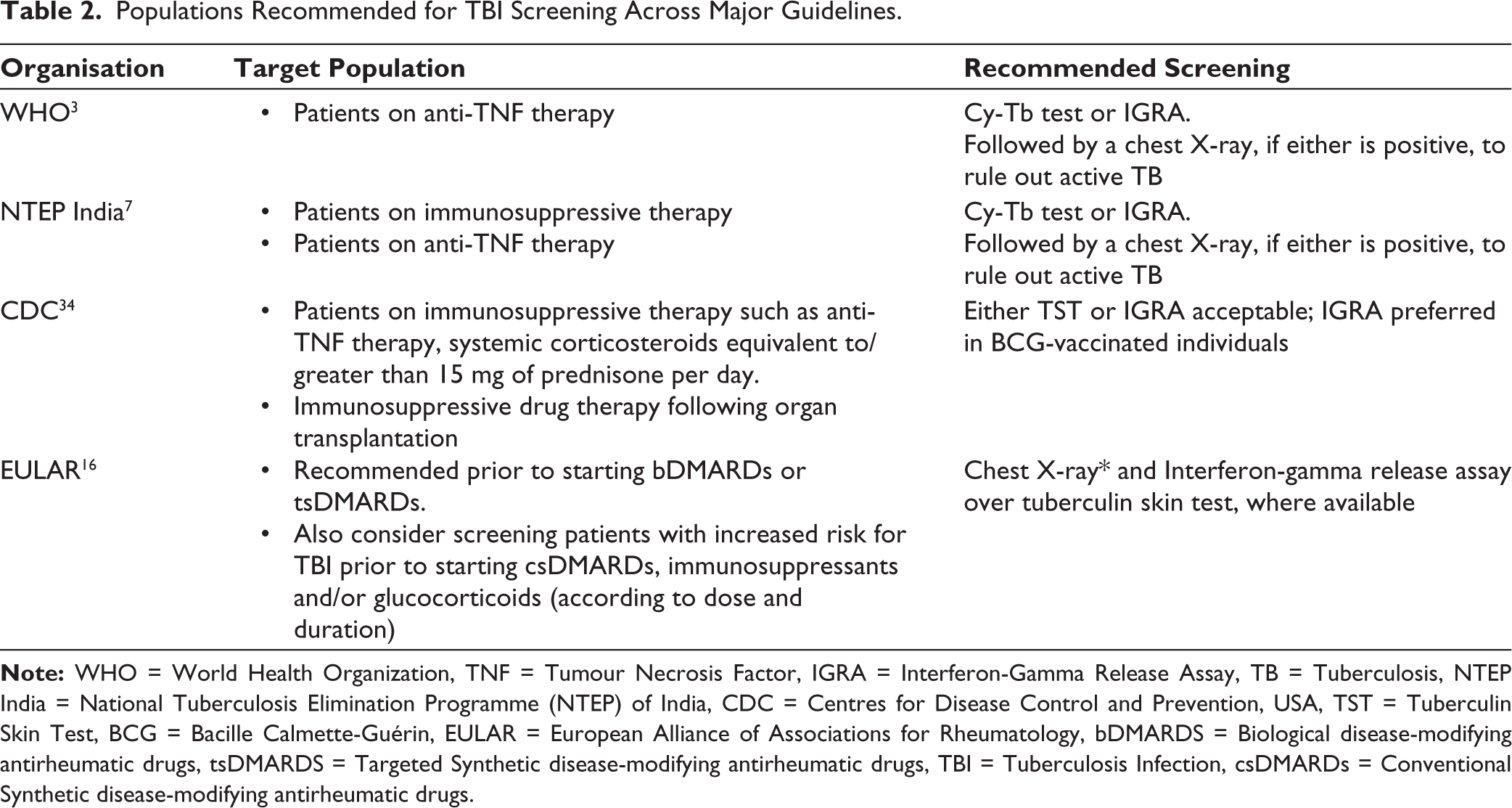
NTEP: Recommends Cy-Tb or IGRA for high-risk individuals; treat TBI after ruling out active disease. 7
CDC: Either TST or IGRA acceptable; IGRA preferred in BCG-vaccinated individuals. 34
European Alliance of Associations for Rheumatology (EULAR): Prefers IGRA over TST in BCG-vaccinated populations; combine with history and chest X-ray. 16
Preventive Therapy
Timing
Based upon the evidence cited, the recommendation is to initiate TBI treatment at least 4 weeks before starting b/tsDMARDs. 3 However, in routine practise, the clinical condition of the majority of patients does not allow holding appropriate treatment for 4 weeks. Therefore, most rheumatologists initiate appropriate DMARDS (if required, with glucocorticoids) simultaneously with the preventive treatment of TBI.
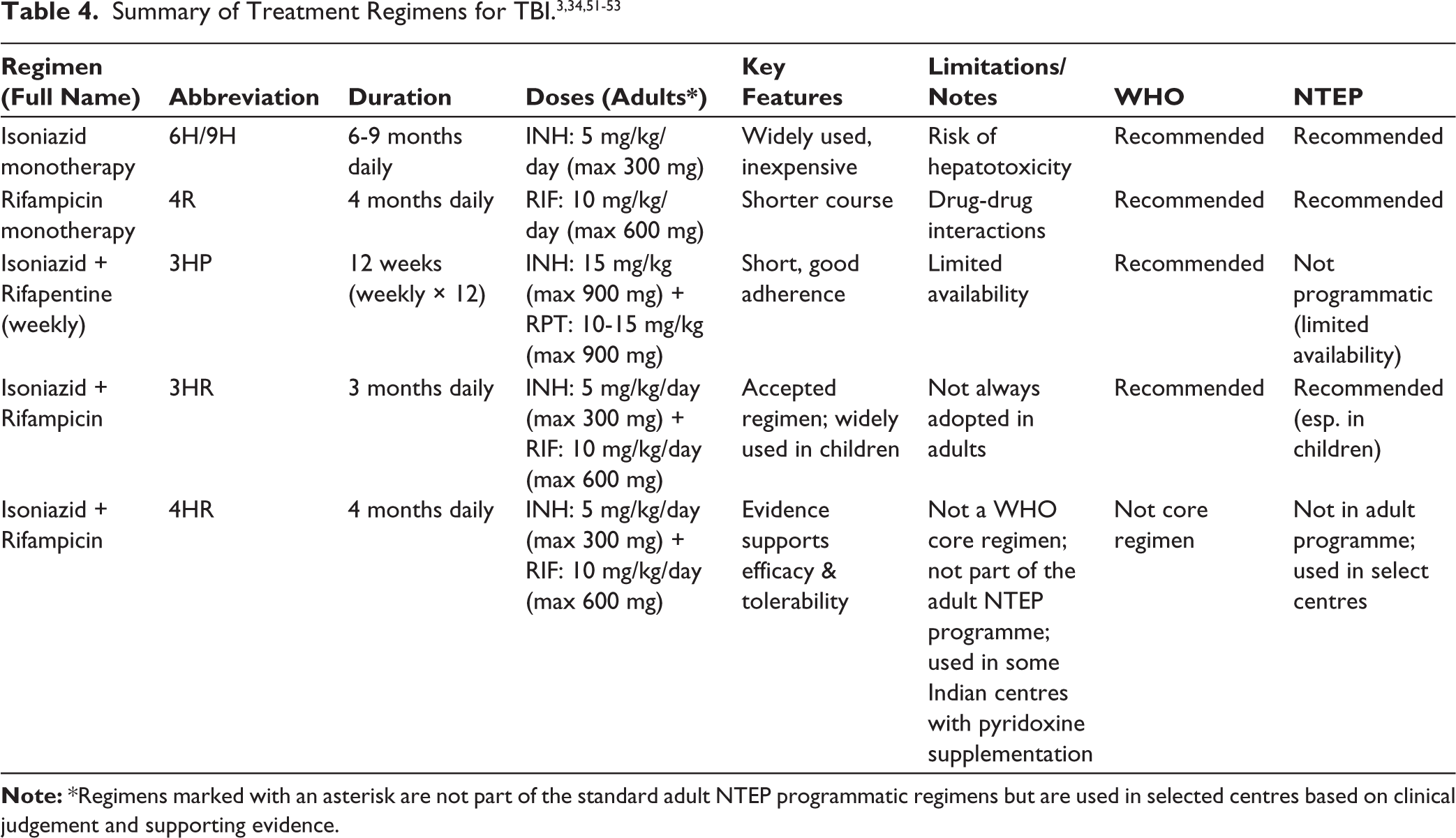
Recommended Regimens (WHO/NTEP)
Isoniazid (H/INH) daily × 6-9 months (short-form: 6H/9H): widely used, inexpensive, but with some degree of hepatotoxicity risk.
Rifampicin (R) daily × 4 months (short-form: 4R): shorter, but drug-drug interactions.
H + Rifapentine (P) weekly × 12 weeks (short-form: 3HP): shorter, good adherence, limited availability.
H + R daily × 3 months (short-form: 3HR): accepted regimen, especially in children under NTEP.
H+ R daily × 3/4 months (short-form: 4HR. 3HR): Evidence supports efficacy and tolerability [Though not formally listed by WHO as a core regimen, and not part of adult NTEP programmatic regimens, it is used in some Indian centres with pyridoxine supplementation (ISIC-JDC)].3,34
Proposed practical algorithm for the screening of TBI in patients with rheumatic & musculoskeletal diseases (RMDS) in India. 7
Resource-limited: TST + chest X-ray; treat if either positive.
Moderate resources: IGRA + chest X-ray; treat if IGRA positive or suspicion high.
High-risk/tertiary care setting: Dual testing (TST + IGRA) + chest X-ray; treat if any test positive or suspicion remains high (Exception: Dual testing is not recommended by NTEP).
Universal: Chest X-ray and history for all patients.
Monitoring
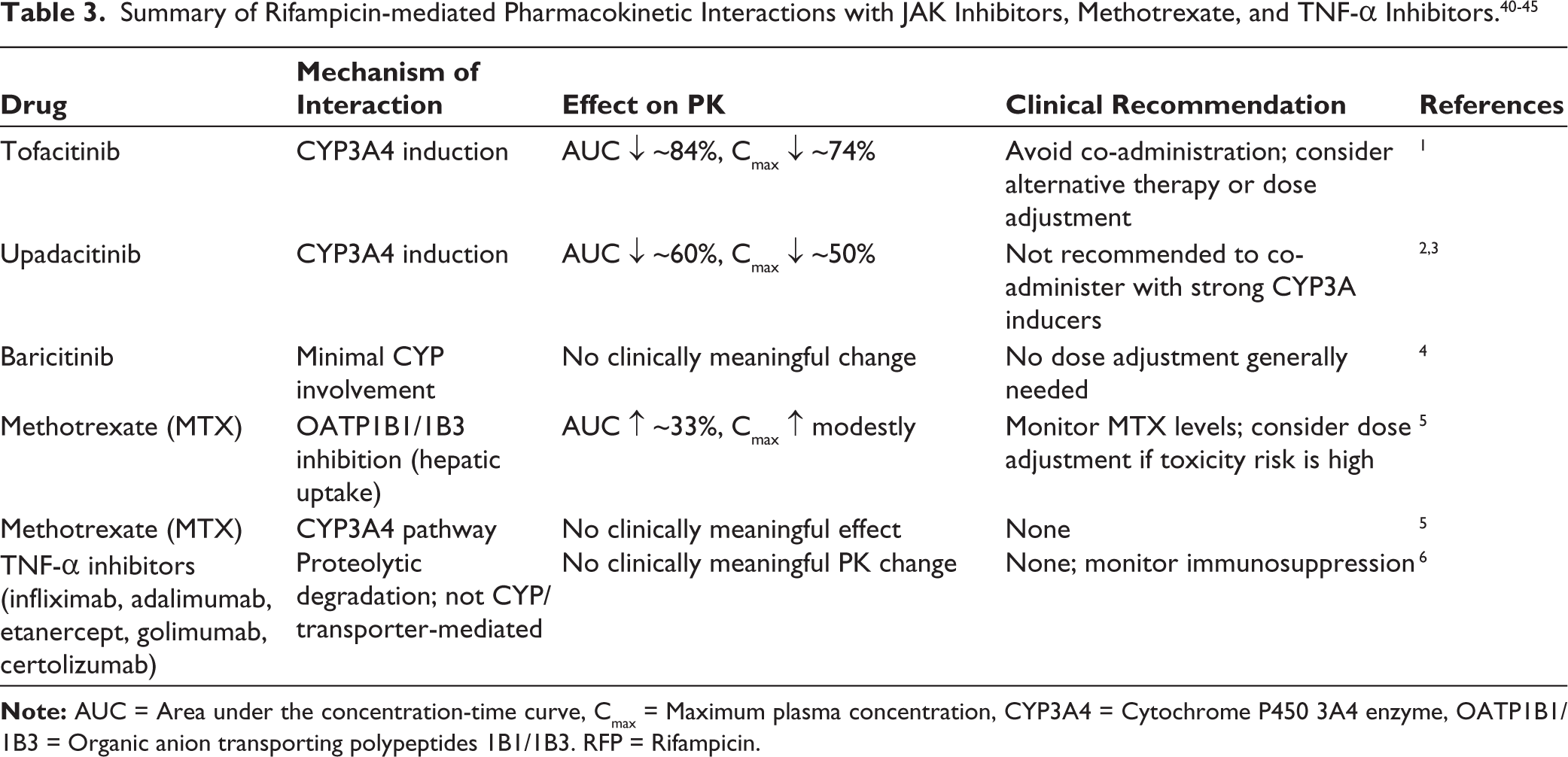
Rifampicin, a strong CYP3A4 inducer, reduces exposure of CYP3A4-metabolised JAK inhibitors like tofacitinib and upadacitinib, while baricitinib is minimally affected. Methotrexate, cleared via hepatic and renal transporters, is influenced by rifampicin through OATP1B1/1B3 inhibition. TNF-α inhibitors, as monoclonal antibodies, are not affected.
Baseline and periodic LFTs; watch for hepatotoxicity and rifampicin-related drug interactions (methotrexate, leflunomide, JAK inhibitors).
Discussion
There are only a few studies that have reported on the performance of TBI testing in SIRDs from India. In a 2009 report, Malaviya et al. highlight the high TB risk in patients with SIRD and the need for formal TBI screening in Indian patients starting anti-TNF therapy. 35 These authors again reported in 2018 their ‘Real Life Experience’ of a screening strategy for TBI (the called LTBI) before the start of treatment with bDMARDs in Indian Patients with SIRDs.17,18
Chandrashekara and colleagues reported on 943 patients who had undergone IGRA pre-screening prior to the initiation of biologics or tsDMARDs. 18 Among the selected subjects, 125 patients (13.3%) were TBI positive. They find that the accuracy of IGRA in predicting the absence of TB reactivation was 99.6%, with an error rate of 0.46. Their conclusion was that TBI screening prevents reactivation of TB in patients with SIRDs prior to the prescription of biologics or tsDMARDs. They also state that IGRA is ideal for identifying patients with an increased likelihood of developing TB upon receiving biologics or tsDMARDs with reasonable accuracy. Neema S et al. showed the discordance and diagnostic nuances of TST versus IGRA in psoriasis patients in India. 36 A study by Sarkar S. et al summarises Indian data on TB risk with biologics and discusses TBI screening strategies. 37 The study by Saha S. et al. is an India-context overview touching on screening before biologics, along with practical notes on TST/IGRA sequencing. 38 A study by Ghoshal A. et al. is an India-focused guidance stressing TBI screening/treatment in high-risk groups, including patients on immunosuppressives.38,39
Summarising these reports from India, the studies show variable concordance between TST and IGRA; combining tests increases yield in some cohorts. Screening and treatment of TBI prior to biologic initiation has been associated with reduced incidence of TB in Indian practice-based reports and expert reviews. Immunosuppressive/immunomodulatory drugs (high-dose steroids, biologics, JAK inhibitors) reduce the sensitivity of TST and can cause false-negative results, and it is important to consider this when testing patients already on therapy. CY-TB (next-generation intradermal skin test) has been introduced under the NTEP in India. It aims to combine the operational simplicity of TST with improved specificity comparable to IGRAs. But the practical application of this test in the clinics/hospitals has not been reported as yet.
TBI management in India must balance sensitivity, specificity and feasibility. TST is cheap but cumbersome, requires two visits and specially trained healthcare workers. IGRA is specific but costly. Chest X-ray is indispensable. A tiered algorithm based on resources offers pragmatic safety. Clinical judgement remains crucial, as negative tests do not exclude TBI in immunosuppressed patients.
Practical Considerations for Indian Rheumatology Clinics
Use a structured pre-treatment checklist: TB symptoms, history of TB, household exposure, prior BCG vaccination and chest radiograph.
Test selection should consider local availability, cost and clinical context: TST (widely available, low cost), IGRA (higher specificity, higher cost), CY-TB (NTEP-endorsed option combining features of both but limited availability).
If the patient is immunosuppressed or on steroids, IGRA may be preferred when available; consider repeat or dual testing (TST+IGRA/CY-TB) to improve detection.
Always perform chest radiography to exclude active pulmonary TB prior to starting preventive therapy.
Suggested Screening Algorithm
Before starting biologics/immunosuppressants—baseline assessment:
Symptom screen for TB (cough, fever, weight loss, night sweats) and exposure history. Chest radiograph (CXR). If CXR suggests active TB → evaluate with sputum/Cartridge-based nucleic acid assay test (CB-NAAT) and treat per NTEP.
TBI testing (choose according to availability & context)
Option A (Resource-limited/routine): TST (Mantoux) → read at 48-72 h. If ≥10 mm (or 5 mm for high-risk like recent contacts), consider TBI positive. Option B (Preferred if available, immunosuppressed or prior BCG): IGRA (e.g., QuantiFERON/T-SPOT). Positive → TBI positive. Option C (NTEP-available alternative): CY-TB intradermal test using 5 mm universal cut-off as per NTEP SOP. If the initial test is negative but high clinical suspicion (recent exposure, severe immunosuppression), consider dual testing or repeat testing after stopping short-term steroids when feasible.
If TBI positive (test ± CXR clear of active disease)
Offer TB preventive therapy (TPT) per national/regional guidance (regimens may include isoniazid or rifamycin-based regimens; consider drug interactions with planned immunosuppressants). Defer biologic/major immunosuppression until TPT is started, and the clinician judges it safe to proceed (timing per local policy and clinical urgency).
If test indeterminate/discordant
Reassess risk factors and chest X-ray. When there is discordance between IGRA and TST, repeat the test that is negative. If still in doubt in high-risk patients, consider treatment with TPT.
Monitoring
Monitor for TPT adverse effects (esp. hepatotoxicity) and for signs of active TB on follow-up. Maintain documentation (e.g., ‘Ni-kshay’ enrolment if CY-TB used under NTEP protocols).
Practical Tips and Caveats
CY-TB uses a universal 5 mm induration cut-off per NTEP SOP 30 and is reported to be unaffected by prior BCG.
False negatives can occur with ongoing immunosuppression; interpret negative tests cautiously in patients on high-dose steroids or biologics.
Drug interactions: rifamycin-based TPT regimens may interact with some DMARDs/biologics → consult pharmacy or TB specialist when planning regimens. Table 3 summarises possible drug interactions while using rifamycin-based TPT regimens.40,46-50
Document decisions and informed consent when starting TPT in complex patients.
TPT remains a cornerstone. While Isoniazid monotherapy is standard, rifampicin-based regimens (4R, 4HR, 3HR) and 3HP offer shorter courses but require caution for drug interactions. Wider access to 3HP and Indian-made IGRA assays like ‘Cy-Tb’ (made in India) may transform practice.
Case Scenarios for TBI Screening in Rheumatology Practice (High TB Burden Setting)
Case Scenario 1: ‘Previously Treated Pulmonary TB; Is TBI Testing or Treatment Needed?’
Clinical Presentation
A 48-year-old woman with seropositive rheumatoid arthritis is being considered for initiation of a biologic DMARD (anti-TNF agent). She had sputum-positive pulmonary TB 3 years ago, for which she received a complete 6-month regimen of anti-tubercular therapy (ATT). She has been asymptomatic since and has no current evidence of active TB on chest X-ray.
Key Clinical Questions
Can this patient receive biologic therapy?
Should she undergo testing for TBI (TST or IGRA)?
If positive, does she need prophylactic treatment?
If negative, is it safe to start biologic therapy?
Reasoning
Past TB history:
Treated pulmonary TB in the past is not a contraindication to biologic therapy if treatment was complete and cure is established.
7
However, patients with prior TB remain at higher risk of reactivation.
Testing for TBI:
Both TST and IGRA may remain positive for years after active TB and cannot reliably distinguish between resolved infection and latent infection. 41
Hence, the test result in this patient is not useful for decision-making.
Guideline perspective (India, NTEP + rheumatology practice):
This patient should receive TPT, as past history of TB is not a contraindication for TPT.
7
Careful clinical monitoring during immunosuppression is advised.
Practical Recommendation for this case:
TBI testing (TST/IGRA) will not help in decision-making, since prior treated TB invalidates its utility. Start biologic therapy with close vigilance for TB reactivation (baseline chest X-ray and symptom surveillance at every visit).
Case Scenario 2: Strongly Positive TST in an Asymptomatic Patient
Clinical Presentation
A 35-year-old woman with active psoriatic arthritis is being considered for secukinumab. She has never had TB, but her Mantoux test shows 18 mm induration. IGRA is not available. She has no symptoms, and the chest X-ray is normal.
Questions
Does she have TBI?
Should she be treated before biologics?
Reasoning
Recommendation
Treat TBI with any of the TPT regimens mentioned in Table 4.
Delay biologic initiation until at least 4 weeks of TBI therapy are completed. 39
Case Scenario 3: BCG Vaccination Scar but no TB History
Clinical Presentation
A 25-year-old man with ankylosing spondylitis is planned for adalimumab. He has a BCG vaccination scar, no past TB, no symptoms of TB at present and a normal chest X-ray.
Questions
Should he be tested for TBI?
If the test is positive, should he be treated?
Reasoning
Recommendation
Case Scenario 4: Indeterminate IGRA on Immunosuppressive Therapy
Clinical Presentation
A 42-year-old woman with lupus nephritis is on prednisolone 20 mg/day and mycophenolate mofetil 2 g/day. Her IGRA result is indeterminate; TST shows 6 mm induration. She needs Rituximab for control of her disease activity.
Questions
How to interpret indeterminate IGRA?
Should TBI prophylaxis be given?
Reasoning
Immunosuppression can blunt both TST and IGRA responses. 10 In high-risk countries, clinical judgement + Chest X-ray should guide. A borderline/indeterminate result cannot exclude TBI. 7
Recommendation
Immunosuppressive therapy may blunt responses to IGRA and TST. Treatment for TBI should be based on clinical judgement and a chest X-ray. 7
If no risk factors are present, and the chest X-ray is clean, start rituximab without TBI therapy but under strict TB surveillance.
Case Scenario 5: Chronic Kidney Disease Patient on Dialysis
Clinical Presentation
A 55-year-old man with RA needs anti-TNF therapy. He is on regular dialysis for end-stage renal disease (ESRD). There is no TB history, and the chest X-ray is normal.
Questions
Is TBI screening mandatory in dialysis patients?
Which regimen is safe?
Reasoning
Dialysis patients are at very high risk of TB.
Screening for TBI is strongly recommended before immunosuppression.
Isoniazid and Rifampicin metabolism is not significantly altered in CKD, but pyridoxine supplementation is essential. 45
Recommendation
All patients of CKD on dialysis should undergo screening with TST or IGRA for TBI. 9
If positive, treat with Isoniazid + pyridoxine for 6 months (or 3HR if tolerated). 45
These five scenarios together cover the major clinical dilemmas:
Prior TB (already treated). Strongly positive TST with no symptoms. BCG versus TBI confusion. Immunosuppressed patient with an indeterminate result. High-risk comorbidity (ESRD/dialysis).
Footnotes
Author’s Contribution
ANM: Conceived the need for this article, prepared and wrote the article outline, prepared the first draft of the main manuscript, and revised ad re-revised the manuscript.
NK: Assisted with finding appropriate references, inserting references at appropriate places in the draft-manuscript.
MP: Helped in ensuring that all the relevant references are included in the manuscript. Also helped in improving the language.
SK: Critically evaluated the rough draft, suggested inclusions, exclusions and deletions of statements and references
SG: Critically evaluated the rough draft, suggested inclusions, exclusions and deletions of statements and references
A. Mohan: Critically went through the manuscript checking the correctness of the facts, statements and references from the standpoint of an ‘Expert in Tuberculosis’ and made corrections from the standpoint of a TB-expert.
Chandrashekara S: Helped with searching and helping with Indian published work on the subject of the article.
Clinical Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not required.
Permission to Reproduce Material from Other Sources
No third-party content was reproduced in the manuscript.