
Abstract
Background:
Nintedanib, a multi-tyrosine kinase inhibitor, is an approved anti-fibrotic agent for idiopathic pulmonary fibrosis (IPF) and Systemic Sclerosis-Associated Interstitial Lung Disease (SSc-ILD). This study aimed to comprehensively assess the efficacy and safety of nintedanib across the broader spectrum of Systemic Autoimmune Disease-Associated Interstitial Lung Disease (SARD-ILD) patients receiving standard immunosuppressive therapy, focusing primarily on the annual rate of decline in Forced Vital Capacity (FVC).
Methods:
We conducted a systematic review and meta-analysis of Randomised Controlled Trials (RCTs) and retrospective observational studies investigating the effects of nintedanib on FVC decline and safety outcomes in SARD-ILD patients. A systematic literature search spanning the last 20 years, up to November 2023, was executed across PubMed, Scopus, Embase, and Cochrane Central. Studies were restricted to those published in English.
Results:
The systematic review included a total of eight RCTs and seven observational studies, comprising 1099 SARD-ILD patients. Of these, two studies provided suitable data for quantitative synthesis (meta-analysis). Pooled results demonstrated a significantly reduced annual rate of FVC decline in the nintedanib arm compared to the placebo arm (MD = 52.49 mL/yr, 95% CI = 18.38–86.59).
Conclusion:
This systematic review and meta-analysis suggest that nintedanib is associated with a significant reduction in the annual decline of FVC in patients with SARD-ILD who are on standard immunosuppression, highlighting its potential therapeutic benefit and favourable safety profile in this complex patient population.
Keywords
Abbreviations
American College of Rheumatology
Anti-neutrophil cytoplasmic antibody
Anti-synthetase syndromes
American Thoracic Society/European Respiratory Society/Japanese Respiratory Society
Connective tissue disorder
Diffusion lung capacity for carbon monoxide
European League Against Rheumatism
Fibroblast Growth Factor Receptor
Forced Vital Capacity
Idiopathic inflammatory myositis
Interstitial lung disease
Interstitial pneumonia with autoimmune features
Idiopathic pulmonary fibrosis
Mixed connective tissue disorder
Non-specific interstitial pneumonia
Platelet-derived growth factor receptor
Rheumatoid arthritis
Randomised controlled trial
Systemic autoimmune rheumatic diseases
Safety and Efficacy of Nintedanib in Systemic Sclerosis
Sjögren syndrome
Systemic lupus erythematosus
Systemic sclerosis
Systemic sclerosis-associated interstitial lung disease
Usual interstitial pneumonia
Vascular endothelial growth factor receptor
Introduction
Interstitial Lung Disease and the Challenge of SARD-ILD
Interstitial lung disease (ILD) is a broad category of pulmonary conditions defined by inflammation and subsequent scarring (fibrosis) in the lung parenchyma, exhibiting diverse clinical courses and therapeutic requirements. 1 Systemic Autoimmune Disease-Associated Interstitial Lung Disease (SARD-ILD) accounts for a significant proportion, approximately 20%, of all ILD diagnoses. 2 This heterogeneous group includes pulmonary complications arising from systemic sclerosis (SSc), rheumatoid arthritis (RA), idiopathic inflammatory myositis (IIMs), anti-synthetase syndromes (ASS), mixed connective tissue disorder (MCTD), systemic lupus erythematosus (SLE), Sjögren’s syndrome (SjS), and ANCA-associated vasculitis.3,4 Managing SARD-ILD presents a considerable therapeutic challenge, often requiring a specialised, multi-disciplinary approach, with treatment protocols frequently guided by evidence derived from SSc cohorts. 5
Nintedanib: Mechanism of Action and Clinical Evidence
Nintedanib, a small molecule that functions as a multi-tyrosine kinase inhibitor (TKI), exerts its effect by targeting key cellular signalling pathways. It inhibits receptors such as the platelet-derived growth factor receptor (PDGFR), vascular endothelial growth factor receptor (VEGFR), and fibroblast growth factor receptor (FGFR). 6 By blocking these receptors, nintedanib effectively slows the fibrotic process by impeding neo-angiogenesis and the proliferation of myofibroblasts. 7
The clinical utility of nintedanib has been demonstrated across several pivotal trials. The SENSCIS trial established its effectiveness in reducing the decline in Forced Vital Capacity (FVC) in patients with Systemic Sclerosis-Associated Interstitial Lung Disease (SSc-ILD), 5 while the INBUILD trial showed similar benefit in subtypes of progressive fibrosing ILD, including various connective tissue disease-related ILDs. 8 Importantly, analyses across ILD subgroups have indicated that the efficacy of nintedanib in slowing lung function decline appears consistent, irrespective of the underlying specific ILD diagnosis. 9
Additional evidence supports its role in primary fibrotic lung disease. The IMPULSIS-2 and TOMORROW trials confirmed that nintedanib helps delay the occurrence of acute exacerbations in idiopathic pulmonary fibrosis (IPF).6,10 The combined data from these two trials highlighted a low incidence of the first acute exacerbation in the nintedanib group (HR = 0.53; 95% CI = 0.34, 0.83; P = .0047). 11 Furthermore, the long-term safety and efficacy profile over three years was substantiated by the IMPULSIS-ON extension trial. 12 Despite this compelling evidence across various fibrotic ILDs, its clinical application outside of SSc-ILD remains restricted.
Objectives of the Review
Given the current evidence gap concerning its widespread use, this review aims to comprehensively evaluate the efficacy and safety profile of nintedanib within the broader SARD-ILD patient population. The primary objective is to quantify the rate of decline in FVC and Diffusion Capacity of Carbon Monoxide (DLCO) in SARD-ILD patients receiving nintedanib therapy. The secondary objective is to characterise the adverse event (AE) profile associated with nintedanib use among SARD-ILD patients.
Materials and Methods
Reporting Standards and Protocol
This systematic review and meta-analysis adhere to the standards outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 13 The protocol for this review was officially registered on PROSPERO, the international prospective register of systematic reviews. As this study exclusively utilised previously published data and did not involve direct patient recruitment, formal patient consent and institutional ethical clearance were not required.
Search Strategy and Study Identification
A rigorous systematic literature search was performed across four major electronic databases: PubMed, Cochrane Central Register of Controlled Trials, Embase (via Embase interface), and Scopus. The search aimed to retrieve relevant Randomised Controlled Trials (RCTs), prospective, and retrospective observational studies investigating the efficacy and safety profile of nintedanib in patients diagnosed with SARD-ILD.
The search was constrained to articles published in the English language within the last 20 years, up to November 2023. This language restriction was imposed to prevent potential data misinterpretation arising from the unavailability of suitable translations. Google Scholar was utilised for supplementary electronic searching. The primary search results were further augmented by abstract searches on the official websites of the American College of Rheumatology (ACR), 14 the European League Against Rheumatism (EULAR), 15 and the American Thoracic Society (ATS). 16
The detailed search strategy is outlined in e-Figure 1. It incorporated a combination of controlled vocabulary, including Medical Subject Headings (MeSH) and Embase Subject Headings (Emtree), related to the target disease and intervention (e.g., interstitial lung disease, connective tissue disease, systemic autoimmune rheumatic disease, nintedanib, and specific disease terms like systemic sclerosis, myositis, rheumatoid arthritis, etc.). These terms were combined using the Boolean operators ‘AND’ and ‘OR’. Completeness was ensured by performing a manual cross-reference check of the bibliographies of all identified full-text articles.
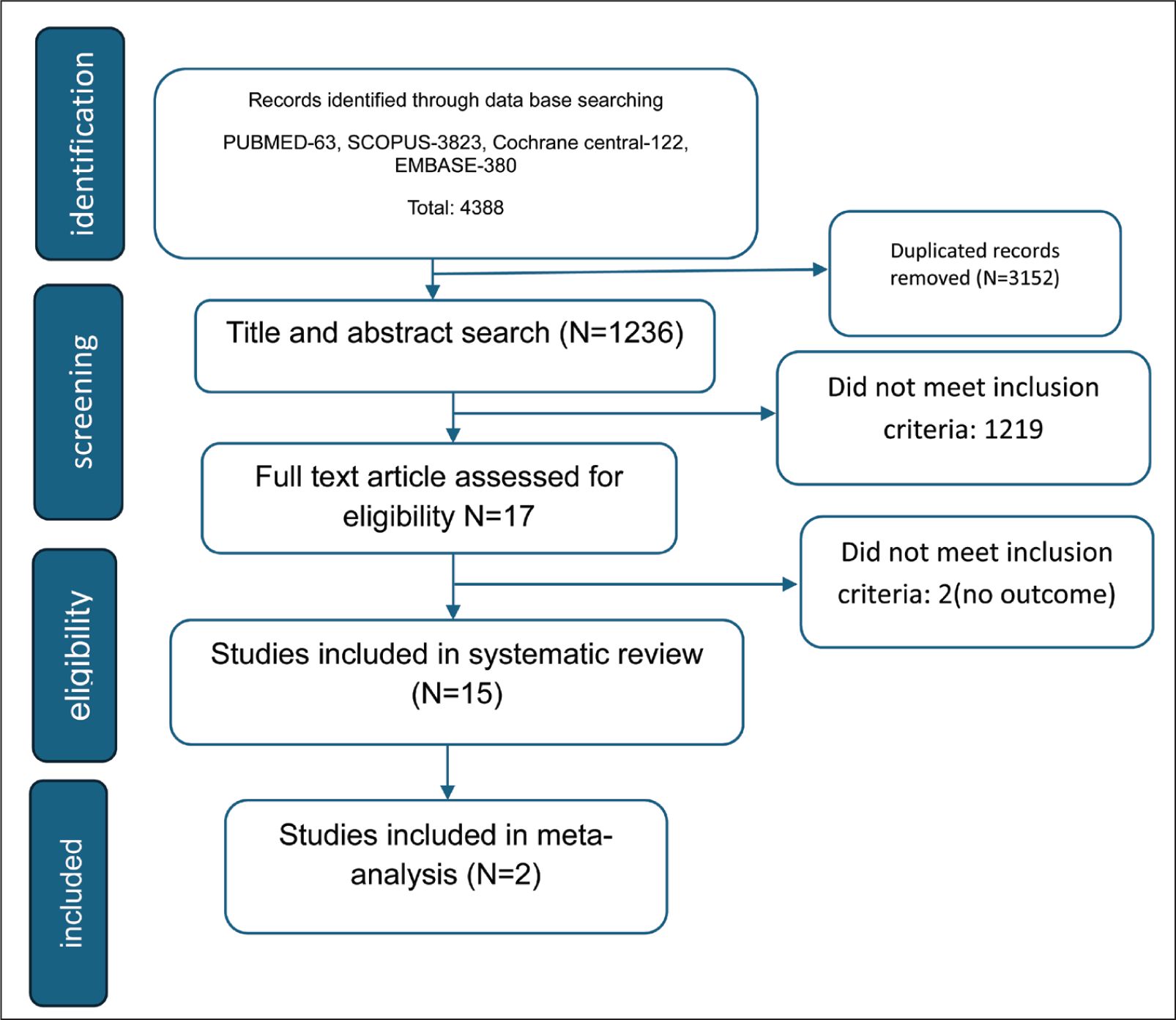
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) Flow Diagram.
Study Selection Process
To minimise the risk of overlooking relevant publications, the initial title and abstract screening was conducted using Rayaan software. Two independent researchers (P.P.S. and A.K.G.) screened all retrieved titles and abstracts. Any abstract not marked as definitively ineligible by both evaluators proceeded to the full-text review stage.
The full texts were independently evaluated for relevance by P.P.S. and A.K.G. against a pre-specified checklist based on the inclusion and exclusion criteria. Discrepancies at any stage were resolved through collaborative discussion, with additional researchers (M.K. and V.S.P.) acting as arbitrators.
Inclusion and Exclusion Criteria
Inclusion criteria required studies to meet all of the following:
Study design: RCTs, prospective, or retrospective observational studies. Population: Patients aged ≥ 18 years with a confirmed SARD-ILD diagnosis, radiographic evidence of involvement ≥ 10%, baseline FVC ≥ 40% of predicted, and baseline DLCO between 30% and 79% of predicted. Intervention: Nintedanib administered at any dose as initial therapy, in combination with standard immunosuppression and glucocorticoids. Outcomes: Reporting on the rate of decline in FVC and/or DLCO, mortality, or serious AEs in SARD-ILD patients. Follow-up period: Outcomes reported anytime beyond 24 weeks after randomisation. Publication date: Published within the last 20 years, up to November 2023.
Exclusion Criteria encompassed all studies that did not satisfy the inclusion criteria, studies featuring ILD aetiologies other than SARD-ILD (e.g., IPF, occupational ILD), studies evaluating anti-fibrotic agents other than nintedanib, case series involving fewer than 10 patients, case reports, and conference abstracts lacking complete full-text data.
Data Extraction and Risk of Bias Assessment
Two reviewers (P.P.S. and A.K.G.) independently extracted data from each eligible study. Extracted information included study design, setting, population characteristics, intervention strategy, and outcome measures. Data for outcomes reported beyond 24 weeks, and for longer-term follow-up for pre-specified subgroups, were systematically extracted.
The methodological quality and potential for bias in the included studies were assessed using the Cochrane Risk of Bias Tool (RoB 2) 17 by two independent reviewers (P.P.S. and A.K.G.). A study was categorised as high-quality if it met at least five of the seven methodological criteria defined by RoB 2. Disagreements regarding data extraction or quality assessment were resolved through consultation with arbitrating reviewers (A.S. and M.K.).
Outcome Measures
Primary Outcome
The change in FVC, assessed using several metrics:
Annual rate of decline in FVC. Proportion of patients with an absolute or relative decline in percent predicted FVC >5%. Proportion of patients with an absolute or relative decline in percent predicted FVC >10% or more. Change in the relative or absolute value of percent predicted FVC. Change in the absolute value of FVC.
Secondary Outcomes
Change in the Diffusing Capacity of the Lung for Carbon Monoxide (DLCO).
AEs, defined as any unfavourable or unexpected signs, symptoms, or diseases associated with the drug’s use, irrespective of causality.
Data Synthesis and Statistical Analysis
Data synthesis and statistical analysis were performed using Review Manager version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). 18
Heterogeneity among the studies was evaluated using the I 2 statistic. Heterogeneity was classified as low (I 2 < 25%), moderate (I 2 > 50%), or high (I 2 > 75%). A random-effect model was employed for pooling results in the presence of high heterogeneity; otherwise, a fixed-effect model was utilised.
Forest plots were constructed for the visual representation of the effect estimates. For categorical data, the Odds Ratio (OR) and Risk Ratio (RR) with 95% CI were calculated. For continuous data, the mean difference (MD) with 95% CI was estimated. A P value of <.05 was considered statistically significant.
Risk of Bias Assessment Summary
The RoB 2 tool was used to evaluate the methodological quality, providing objective criteria for bias judgement to enhance reliability. Based on the assessment, one included study was determined to have a low risk of bias, while the other was rated as having ‘some concern’. A graphical representation of the risk of bias across domains is provided in Figure 2.
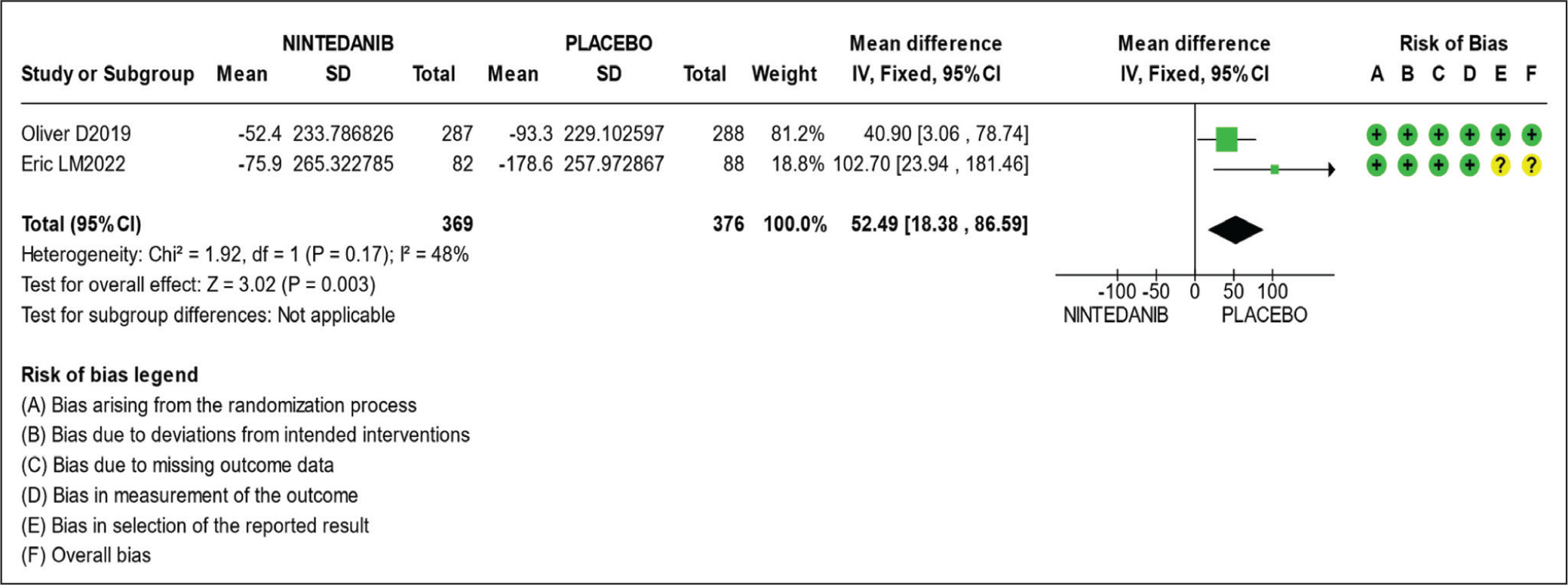
Meta-analysis of the Annual Rate of Decline in FVC (mL/year) Over 52 Weeks with Nintedanib.
Results
Literature Search and Study Inclusion
The initial comprehensive search, following PICOS principles, retrieved a total of 4,388 records. After the removal of duplicates, 1,236 records were identified as potentially relevant and underwent title and abstract screening. Seventeen articles were retrieved for full-text evaluation, resulting in the final inclusion of 15 studies for the systematic review. Ultimately, two RCTs provided suitable data for the meta-analysis. The complete literature search and screening process is illustrated in Figure 1.
Study Characteristics
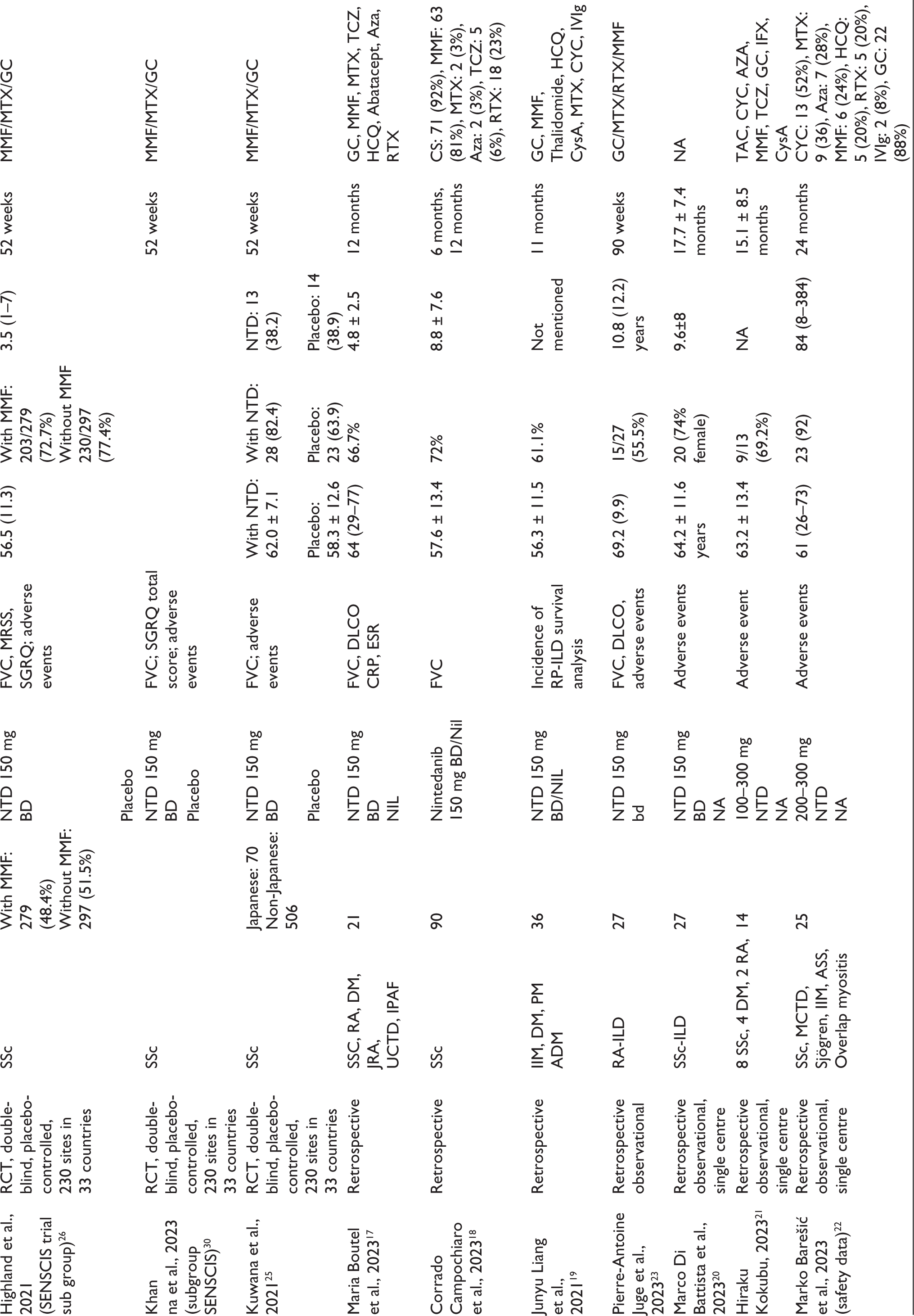
The final synthesis incorporated two primary RCTs, their corresponding six subgroup analyses, and seven observational studies.5,8,19–25 The detailed characteristics of these studies are provided in Table 1.
Baseline Characteristics of Included Studies.
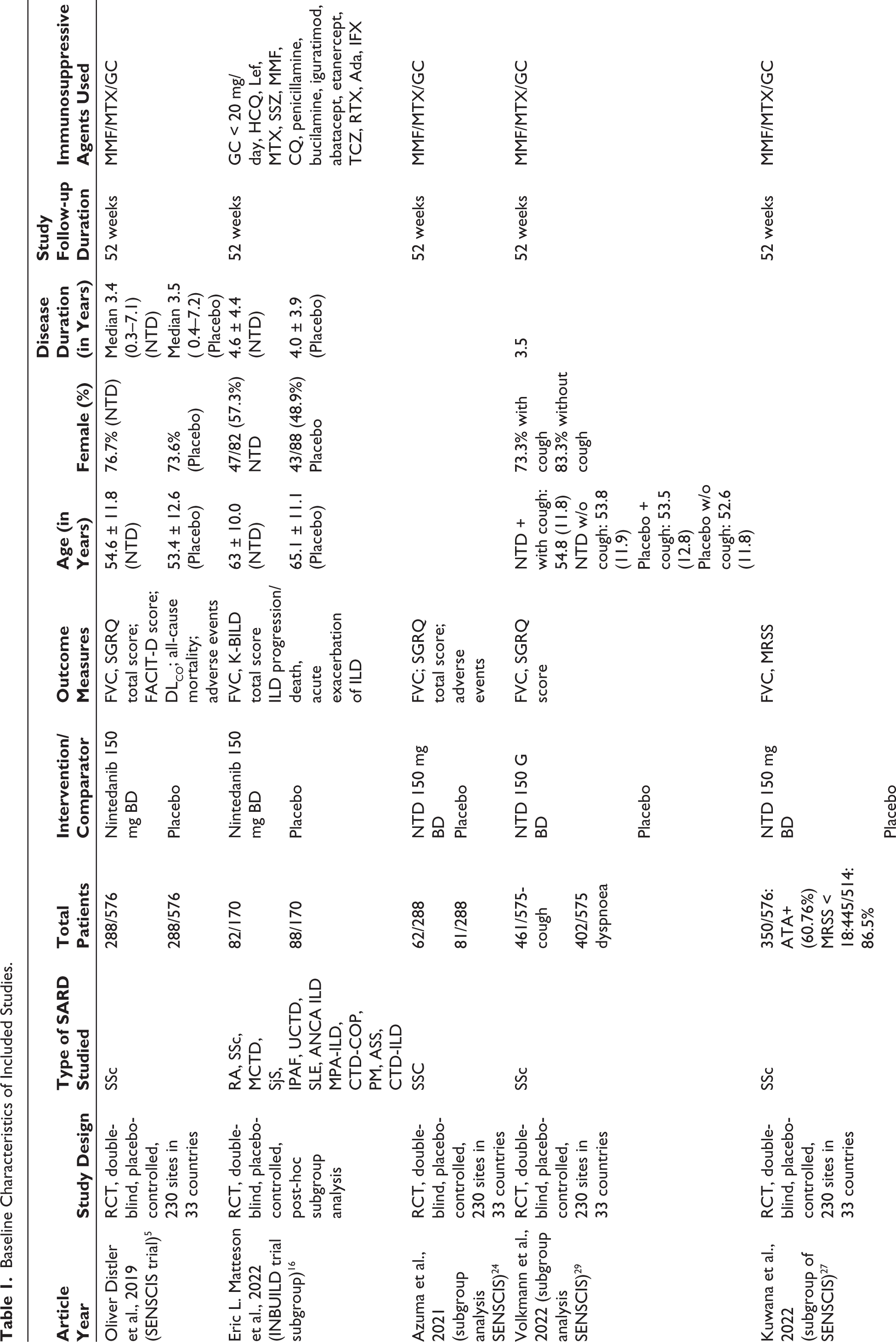
The SENSCIS trial 5 focused on SSc-ILD patients, assessing nintedanib’s efficacy, safety, and tolerability over 52 weeks. The study reported by Matteson EL et al. 8 was a post-hoc subgroup analysis of the INBUILD trial, specifically extracting data on SARD-ILD patients treated with nintedanib.
The remaining RCTs included were subgroup analyses of the SENSCIS trial, which investigated various specialised cohorts, including Asian versus non-Asian populations, 26 Japanese versus non-Japanese patients, 27 those receiving concomitant mycophenolate mofetil, 28 anti-topoisomerase one antibody status, 29 Modified Rodnan Skin Score (MRSS) subgroups (≤18 vs. >18), 29 SSc subtype (diffuse vs. limited disease), 30 and patients stratified by cough and dyspnoea symptoms. 31 Khanna D et al. 32 performed a separate analysis of SENSCIS participants, identifying subjects with risk factors for rapid ILD progression (e.g., early SSc, elevated inflammatory markers, or significant skin fibrosis) who experienced a more rapid FVC decline than the overall trial population.
The seven included observational studies provided relevant safety, tolerability, and pulmonary function data on SARD-ILD patients receiving nintedanib.19–25
Participant and Intervention Characteristics
A total of 1,101 patients were included in this systematic review, with 610 patients receiving nintedanib. Table 1 details the study and participant characteristics. The primary SARD classifications included: SSc-ILD (765 patients), RA-ILD (123), IIM-ILD (163), MCTD (22), SjS (9), CTD-ILD (5), ANCA ILD (2), SLE-ILD (2), overlap myositis (2), juvenile RA (1), and CTD-OP (1). Additionally, a small number of patients were classified as IPAF (6) in trials when specific SARD criteria were not fully met.
In the SENSCIS trial and its subgroup analyses, nintedanib was administered at 150 mg twice daily (BD). In some retrospective studies, the dosage was reduced to 100 mg BD due to AEs.21,23 In the study by Marko Barešić et al., 19 19 of 25 patients received 150 mg BD, while 6 were initiated on 100 mg BD, a protocol also reported by Maria Boutel et al. 24
Outcome Measures
Change in FVC
All included RCTs and three observational studies5,8,19,20,25 reported the annual rate of decline in FVC. Both the SENSCIS trial and the post-hoc INBUILD analysis described the effect of nintedanib on FVC decline.
The pooled analysis of the two RCTs demonstrated a significantly smaller annual FVC decline in the nintedanib arm compared to the placebo arm, with an MD favouring nintedanib of 52.49 mL/year (95% CI = 18.38–86.59).
SENSCIS trial 5 : Nintedanib slowed the annual rate of FVC decline by 40.90 mL/year (95% CI = 3.06–78.74) versus placebo.
Post-hoc INBUILD analysis 8 : Nintedanib slowed the annual rate of FVC decline by 102.70 mL/year (95% CI = 23.94–181.46) versus placebo (Figure 2).
While the overall result favoured nintedanib, the post-hoc INBUILD analysis indicated that the reduction in FVC decline was not statistically significant in specific subgroups: SSc-ILD (120.7 mL/year; 95% CI = −53.2 to 294.6), MCTD ILD (31.9 mL/year; 95% CI = −210.0 to 273.8), and other fibrosing ILD (72.5 mL/year; 95% CI = −134.1 to 279.0). 8
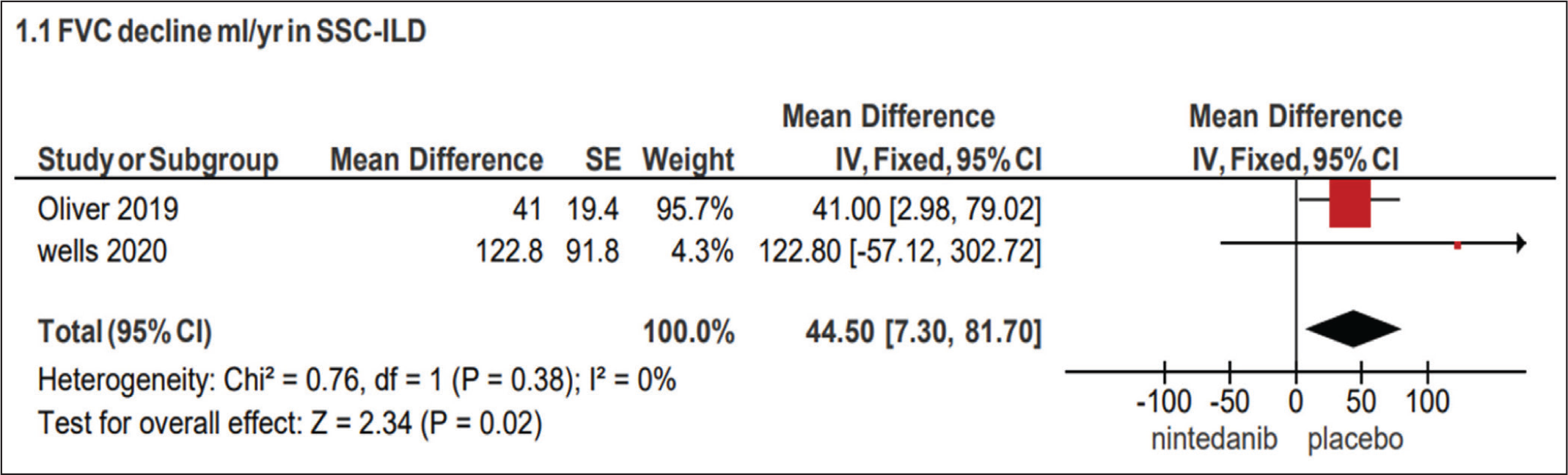
Subgroup analysis pooled across both RCTs focusing on SSc-ILD patients showed that the annual rate of FVC decline was significantly higher by 44.5 mL/year (95% CI = 7.3–81.7) in the placebo group compared to the nintedanib group (Figure 3).
Pooled analysis combining the two RCTs and subgroup data5,8,28 indicated that nintedanib was associated with a statistically significant lesser decline in absolute FVC of 51.43 mL (95% CI = 25.94–76.93) at 52 weeks versus placebo (e-Figure 2). However, the pooled analysis showed no significant difference in the absolute change in percent predicted FVC at 52 weeks (MD = 1.98; 95% CI = −0.01 to 3.97) (e-Figure 3).
Meta-analysis of the Annual Rate of Decline in FVC (mL/year) over 52 Weeks Across the SSC-ILD Subgroup.
Nintedanib was associated with a 36% lower rate of decline in FVC by >5% at week 52 compared to placebo (e-Figure 4). This protective effect was consistent across SENSCIS subgroups, including those treated with or without MMF and those with or without cough.5,8,28,31 Conversely, the meta-analysis for the proportion of patients with FVC decline of >10% at 52 weeks showed no significant effect (OR = 0.86; 95% CI = 0.70–1.06) (e-Figure 5). This non-significant result was consistent across all analysed subgroup populations.
Forest Plot Showing Association of Frequent Adverse Events with Nintedanib.
Change in Diffusing Capacity of Carbon Monoxide (DLCO)
The SENSCIS trial reported the change in the absolute value of DLCO (% of predicted value), finding no significant difference between the nintedanib and placebo groups (MD = –0.44; 95% CI = −1.94 to 1.06). 5
Adverse Events
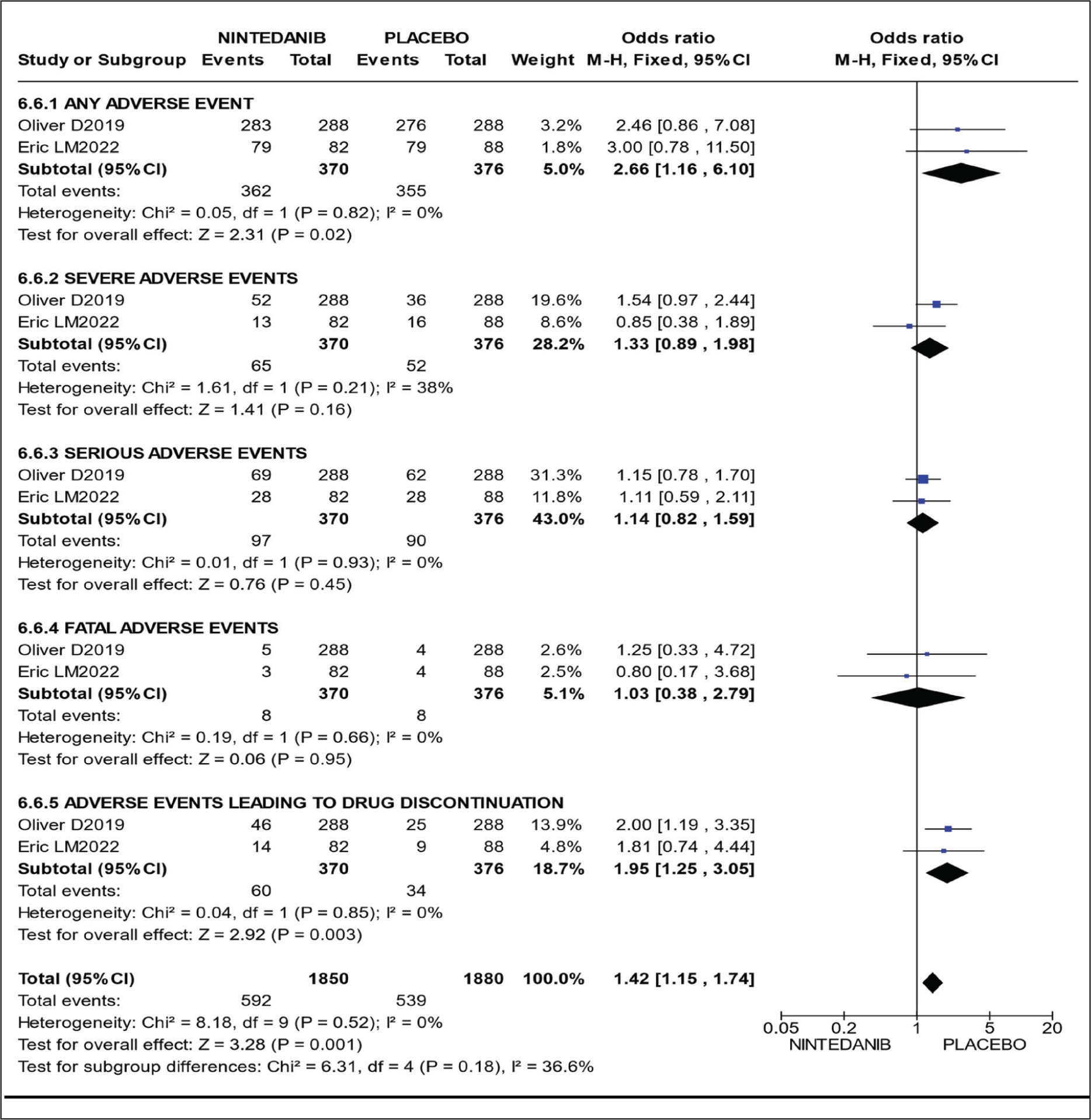
AEs were evaluated in both included RCTs.5,8 The forest plot summarising the meta-analysis for AEs is presented in e-Figure 6.
Heterogeneity: There was low heterogeneity for overall AEs (I 2 = 0%), serious AEs (I 2 = 0%), fatal AEs (I 2 = 0%), and AEs leading to treatment discontinuation (I 2 = 0%). Moderate heterogeneity was observed for severe AEs (I 2 = 38%).
Incidence: Pooling data from both studies showed that nintedanib treatment was associated with a statistically significant increase in:
Overall AEs (OR =2.66; 95% CI =1.16–6.10; P = .02). Treatment Discontinuation (OR =1.95; 95% CI =1.25–3.05; P = .003).
Nintedanib numerically increased the incidence of severe AEs (OR = 1.33), serious AEs (OR = 1.14), and fatal AEs (OR = 1.03) compared to placebo, but none of these differences reached statistical significance (online resource 5.pdf).
Most frequent AEs (Figure 4): No heterogeneity was observed for diarrhoea (I 2 = 0%), nausea (I 2 = 0%), vomiting (I 2 = 0%), and nasopharyngitis (I 2 = 0%). Moderate heterogeneity was observed for weight loss (I 2 = 35%).
Nintedanib significantly increased the risk of common gastrointestinal events:
Diarrhoea: 6.15 times higher rate (72.9% vs. 30.6%; OR = 6.15; 95% CI = 4.48–8.46; P < .00001). Nausea: 2.93 times higher rate (30.5% vs. 13%; OR = 2.93; 95% CI = 2.02–4.26; P < .00001). Vomiting: 2.81 times higher rate (22.9% vs. 9.6%; OR = 2.81; 95% CI = 1.85–4.29; P < .00001). Weight loss: 3.75 times higher rate (11.0% vs. 3.4%; OR = 3.75; 95% CI = 1.98–7.08).
Nintedanib was associated with a reduction in the risk of nasopharyngitis (OR = 0.72; 95% CI = 0.48–1.08; P = .12), although this finding was not statistically significant.
Discussion
Therapeutic Context and Rationale
ILD represents a principal cause of morbidity and mortality in patients with systemic autoimmune rheumatic diseases (SARDs), significantly curtailing life expectancy to potentially less than five years. 32 Management protocols for SARD-ILD are heterogeneous, dictated by the specific underlying autoimmune disorder, the extent of fibrosis, and the severity of respiratory impairment. Despite the historical scarcity of high-level evidence, the anti-fibrotic agent nintedanib has demonstrated established effectiveness in IPF, SSc-ILD, and other progressive fibrosing ILDs.5,6,33 Nevertheless, persistent concerns regarding its safety profile and tolerability necessitate thorough evaluation.
This systematic review and meta-analysis is the first to directly evaluate the efficacy and safety of nintedanib in the diverse SARD-ILD population compared to placebo. Our review incorporated eight RCTs (including their subgroups) and seven observational studies; however, due to the limited reporting of standardised outcomes across the majority of studies, only two studies could be included in the quantitative meta-analysis for FVC change and AEs.
Efficacy in Preserving Lung Function
The SENSCIS trial focused exclusively on SSc-ILD, 5 while the INBUILD trial included a distinct cohort where SARD-ILD patients constituted 25% of the total population, mainly comprising SSc, RA, and mixed connective tissue disease (MCTD). 34 Our analysis included the post-hoc analysis of the INBUILD trial, which specifically highlighted patients with progressive fibrosing autoimmune ILDs. Both pivotal trials consistently reported a significantly lower annual rate of FVC decline (measured in mL/year) in the nintedanib group compared to placebo,5,34 a finding that constituted the primary outcome of this review.
SARD-ILD represents a major fraction of patients developing Progressive Pulmonary Fibrosis (PPF). Specifically, ILD is a chief risk factor for SSc-related mortality, with 67% of SSc-ILD patients developing progressive pulmonary disease within five years, and 32%–35.5% meeting PPF criteria.35,36 Similarly, approximately 7.7% of RA patients develop ILD, with 25% being diagnosed at disease onset and another 25% progressing to severe ILD within five years. Of the RA-ILD patients, 53% progress, and an estimated 40% meet PPF criteria at five years.3,37
Our quantitative findings, demonstrating a reduced annual FVC decline, are consistent with prior systematic reviews confirming nintedanib’s effectiveness across connective tissue disease-associated ILD (CTD-ILD) and RA-ILD.27,38 Furthermore, several retrospective studies corroborate these results, reporting attenuated annual FVC decline with nintedanib among patients with CTD-ILD, RA-ILD, and IIMs-associated ILD.19,20,24 Notably, one study by Liang et al. reported improved survival rates in IIM-ILD patients treated with nintedanib, demonstrating a statistically significant survival benefit (HR = 0.268, P = .013) after adjusting for key clinical variables.
Combination Therapy and Safety Profile
The current standard of care for SARD-ILD combines glucocorticoids with various immunosuppressive agents, which may include conventional agents (e.g., cyclophosphamide, mycophenolate mofetil) or biologic agents (e.g., rituximab, tocilizumab). 39 All included RCTs and observational studies permitted the concomitant use of conventional immunosuppression alongside nintedanib. Although the INBUILD trial initially excluded patients on these medications at baseline, it permitted their initiation after six months in cases of clinically significant deterioration, raising questions regarding the optimal timing for introducing anti-fibrotic therapy. Current evidence supports the need for further RCTs to directly compare combination therapy (immunosuppressants plus anti-fibrotics) versus immunosuppressants alone to establish the most effective treatment regimen for SARD-ILD.
Our meta-analysis confirmed a significantly increased incidence of AEs in the nintedanib group compared to placebo, with diarrhoea being the most frequent complaint. This finding is consistent with prior literature5,34 and is thought to be mechanistically related to intestinal epithelial inflammation caused by nintedanib metabolites, which are predominantly eliminated via faeces.40,41 Strategies to mitigate AEs are necessary; for example, a study by Battista et al. reported that dose reduction to less than 100 mg twice daily was required in 15.3% of SSc-ILD patients (compared to 44.4% of IPF patients). 22
Limitations
The primary limitations of this systematic review are inherent to the current evidence base, including: a heavy reliance on observational studies due to the scarcity of RCT data specific to non-SSc SARD-ILDs, the lack of complete outcome measures reported across several observational studies, and the inclusion of patients with IPAF and CTD-Organising Pneumonia in our meta-analysis, which potentially limits the generalizability of results to all strictly defined SARD-ILDs. Despite these limitations, the robust reporting of the safety profile across all included studies is a notable strength.
Conclusion
The pooled analysis from this systematic review and meta-analysis conclusively highlights nintedanib’s efficacy in significantly reducing the rate of FVC decline in patients with SARD-ILD compared to placebo. This benefit is observed despite a higher incidence of non-serious AEs, principally diarrhoea, vomiting, nausea, and weight loss. However, the definitive demonstration of nintedanib’s efficacy may not yet apply to individual, less-studied SARDs beyond SSc-ILD and RA-ILD. Further dedicated, high-quality research is essential to fully establish the role and optimal combination regimen of nintedanib as an anti-fibrotic treatment across the entire spectrum of SARD-ILD patients.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We would like to acknowledge Dr Venkatesh S. Pai and Dr. Ravi Kant for their valuable research idea and guidance throughout this study. We extend our gratitude to Dr Prativa Sethi, Dr Avneet Gupta, Dr Aditya Sudan, Dr Rajat Ranka, and Dr Ashish Bawaja for their efforts in data extraction, analysis, and manuscript preparation. We also appreciate the critical and statistical analysis contributions provided by Dr Meenakshi Khapre and Dr Sukdev Manna. All co-authors have reviewed and approved the final version of this manuscript, and each author affirms that the content reflects honest and accurate work. On behalf of all the contributors, I will act as guarantor and will correspond with the journal from this point onward (including verification of proofs).
Clinical Trial Registration
PROSPERO Registration number: CRD42023430594.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval and patient consent were not required for this study as it is a systematic review and meta-analysis of previously published studies/data. PROSPERO registration number is CRO42023430594.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.
Notation of Prior Abstract Publication/Presentation
The contents of the manuscript have not been published or submitted for publication elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.