
Abstract

Dear Editor,
A 28-year-old male, diagnosed with a case of Behçet’s disease since 2019, presented with recurrent oral and genital ulcers (with scarring), generalised papulonodular skin lesions and recurrent conjunctival congestion. Despite colchicine therapy, he experienced 2–3 episodes annually, each lasting 2–3 weeks. He was referred for persistent painful oral ulcers with dysphagia affecting oral intake and generalised skin lesions. Erythrocyte sedimentation rate and C-reactive protein were 68 mm in the first hour and 48 mg/L, respectively. The patient was not tested for HLA-B51. Given his severe disease activity, elevated acute phase reactants and male gender, he was screened for underlying vascular involvement.1,2 Common femoral vein (CFV) thickness was increased (0.7 mm; cut-off value ≥0.5 mm; Figure 1A), 3 prompting a computed tomography pulmonary angiography (CTPA), which revealed multifocal stenosis with intervening aneurysmal dilatations in the fourth- and fifth-order branches of the right and left pulmonary arteries, creating a ‘string of beads’ appearance without thrombosis (Figure 1B). These aneurysms were true stable pulmonary artery aneurysms (PAAs) in nature. 4 He was treated with oral steroids, colchicine and apremilast after 125 mg of methylprednisolone intravenously for three days. He showed a good response and is planned for long-term DMARD therapy. While a few studies suggest treatment of asymptomatic aneurysms due to the high-risk of progression, more research is necessary to determine whether cyclophosphamide or TNF blockers should be used aggressively to treat them. 5
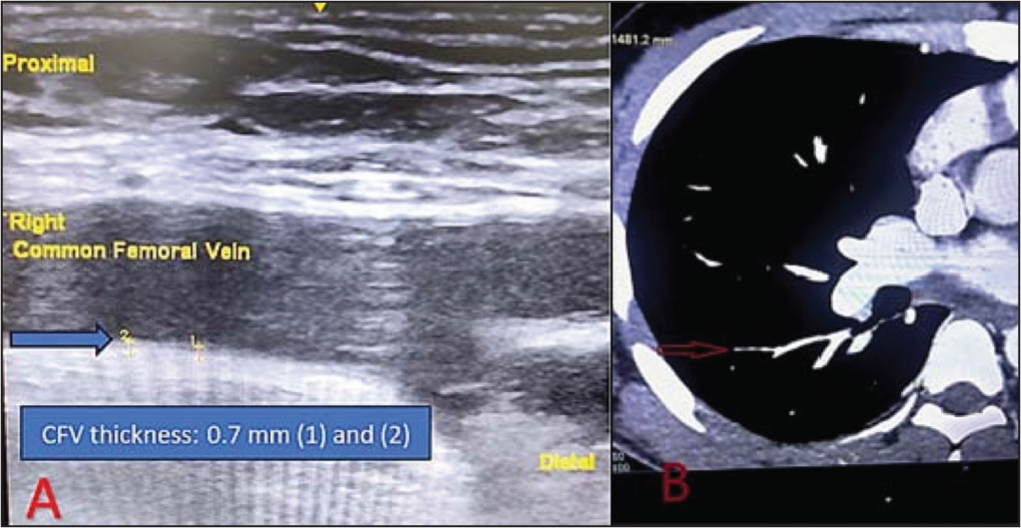
(A) Common femoral vein thickness (CFV- 0.7 mm) is increased (Blue arrow). (B) CT pulmonary angiography (CTPA) showing pulmonary artery stenosis with small sized aneurysms (Red arrow).
PAA in BD carries a mortality as high as approximately 25%. Therefore, early recognition of PAA is important. 6 An increase in vessel wall thickness has been correlated with organ involvement, particularly vascular involvement. 7 Increased CFV thickness is a sign of underlying vessel wall inflammation, a distinctive feature of BD, which may trigger thrombotic tendency. 8 Abacar et al. observed that mucocutaneous BD patients with higher baseline CFV thickness may have a higher risk of developing major organ involvement during follow-up. Similarly, our patient was a young male with severe mucocutaneous disease and elevated CFV thickness; hence, we proceeded with vascular screening. 9 The initial evaluation for vascular screening includes CFV measurement and assessment of acute phase reactants, followed by a CTPA to look for PAAs. 2 Pulmonary artery involvement (PAI) in Behçet’s disease is primarily isolated thrombosis, while aneurysms are rare. Studies suggest that one-fourth of male BD patients asymptomatic for vascular involvement may have subclinical PAI. Early detection of silent PAI through routine CTPA in high-risk patients could lead to improved outcomes. 10 Our findings highlight the importance of screening for vascular involvement in Behçet’s disease using CFV thickness measurement and CTPA, especially in high-risk patients. However, the use of routine CTPA to detect PAI in asymptomatic patients warrants further investigation, as the existing data are inconclusive.
Footnotes
Data Availability Statement
All data relevant to the study are included in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Clearance
Ethical clearance was not taken, as it was not required, since consent was obtained.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written consent has been obtained from the patient for publication