
Abstract

Abbreviations
Glycated Hemoglobin
U1 Ribonucleoprotein
Sjogren Syndrome A antigen
RO 52 Antigen
Intravenous Immunoglobulin
Cyclophosphamide
Sjogren Disease
Cerebrospinal Fluid
Adenosine Deaminase
Acid Fast Bacilli
Anti Nuclear Antibodies
Random Blood Sugar
Introduction
Sjogren disease (SjD) is a chronic progressive autoimmune disease characterised by lymphocytic infiltration of the lacrimal and salivary glands, leading to loss of secretory function.1,2 SjD can present with extra-glandular manifestations. It is called primary when not associated with other autoimmune conditions and associated SjD when present alongside other autoimmune diseases. 3 Neurological disorders are seen in 10%–60% cases of SjD.4,5 Neurological involvement could be central or peripheral, with the latter being the predominant manifestation. 6 Cranial neuropathy is an uncommon symptom in SjD; any cranial nerves from I to XII could be involved, though trigeminal sensory neuropathy is most common. 7 Herein, we are reporting a case presenting as cranial neuropathy in primary SjD.
Case Report
A 38 year old female, a known case of hypertension and type 2 diabetes mellitus since 1.5 years on irregular treatment and hypothyroid for six months presented to a neurologist with history of high-grade fever two months ago which lasted for two days followed by numbness of the left half of the face and decreased sensation over the anterior two-thirds of the left half of the tongue, which was insidious in onset and gradually progressive. There is a history of difficulty in chewing from the left side of the mouth and dribbling of saliva from the left angle of the mouth. No history of difficulty in swallowing, nasal regurgitation, visual symptoms, seizures, cough or shortness of breath. Patient’s vitals were stable and the documented physical examination was also normal except for decreased pain, touch and temperature sensations on the left half of the face and impaired taste sensation over the anterior two-thirds of the tongue bilaterally. Contrast-enhanced MRI brain showed bilateral superior cerebellar arteries closely abutting the bilateral trigeminal nerves (right > left) at their cisternal part. Cerebrospinal Fluid (CSF) analysis showed total cells <5, all lymphocytes, sugar 85.9, protein 156 mg/dL; Adenosine Deaminase (ADA) level was normal, Acid Fast Bacilli (AFB) and GeneXpert were negative; viral panel was negative and negative for fungal elements. CSF oligoclonal bands were negative. The patient was given methylprednisolone pulse therapy for five days and was referred to us after six days.
On detailed history taking, the patient revealed a history of bilateral upper and lower limb pain with paraesthesia in the bilateral soles of the feet and reduced sensations over the left half of the face and loss of taste sensation over the anterior two-thirds of the tongue were persistent. On further enquiry patient gave a history of ocular and oral sicca for 2–3 months. No history of other features suggestive of connective tissue diseases and family history was not significant for any autoimmune disease. On examination, the patient was conscious and oriented; pulse 100 beats/min, blood pressure 124/76 mm Hg and random blood sugar (RBS) 109 mg/dL. No pallor, icterus, clubbing or lymphadenopathy. Reduced sensation over the left half of the face and impaired taste sensation in the anterior two-thirds of the tongue; the rest of the cranial nerves were normal. Motor examination was unremarkable. Both knee and left ankle reflexes were diminished. Schirmer’s test was 0 mm in both eyes; unstimulated whole salivary flow rate was 0.2 mL/5 min (normal rate: 0.1 mL/min). HbA1c was 6%. Patient was investigated on lines of SjD with neurological involvement. Antinuclear antibodies (ANA) (HEp-2) were 4+ speckled. Extractable nuclear antigen profile showed U1RNP 3+, SSA 3+ and RO52 3+. The nerve conduction study was suggestive of bilateral sural nerve sensory axonal neuropathy. C-reactive protein was 20 mg/L. Minor salivary gland biopsy was suggestive of focal lymphocytic sialadenitis with a Focus score of 5. Patient was diagnosed as primary SjD with neurological involvement (cranial nerves V, VII; sural sensory axonal). For cranial neuropathies, the use of corticosteroids, cyclophosphamide, rituximab and plasma exchange has been proven to be effective. After shared decision making, the patient was started on 0.5 mg/kg prednisolone and was given the first induction dose of inj rituximab 1 g along with symptomatic treatment such as pregabalin and oxcarbazepine. Her paresthesias of both feet and numbness over the left half of her face reduced by approximately 25% after six weeks of therapy and facial neuropathy recovered completely.
Discussion
Neurological manifestations of primary SjD are seen in 10%–60% of patients with SjD. 3 The most common form is pure sensory neuropathy. 3 Rarely, cranial neuropathy can be the initial manifestation of SjD. 8 There can be involvement of the facial nerve and rarely the oculomotor nerve.4,5,7 The pathophysiology of cranial neuropathies is not well known yet. Two mechanisms have been proposed: A vascular cause leading to damage of the vasa nervorum and an immunological cause leading to lymphocytic infiltration of the nerve. 3 Aseptic meningitis also contributes to multiple cranial neuropathies. 9
Less than 1% of diabetic patients are affected by overt cranial neuropathies, but there is a four-to seven-fold increased risk of cranial neuropathies in diabetes. 10 This patient had well-controlled glycaemia and did not have third cranial nerve palsy. Anti-U1RNP positivity can be seen in primary SjD and they have a lower median age at onset of SjD symptoms; more frequent constitutional symptoms, muscle weakness and pulmonary involvement. 11 Though the patient has anti-U1RNP antibodies, she did not have any clinical features suggestive of overlap or mixed connective disease.
Cases reported of primary SjD presenting as cranial neuropathy are summarised in Table 1. In a large cohort of 92 patients with SjD, 15 (17%) patients had pure sensory trigeminal neuropathy, nine patients with unilateral involvement and six with bilateral involvement. 12 Our patient also had unilateral pure sensory trigeminal neuropathy. Most trigeminal neuropathies occur initially or appear later in patients with sensory ataxia or painful small-fibre sensory neuropathy. Trigeminal neuropathy may be due to myelin sheath loss, axonal degeneration or vasculitis. Lymphocytic infiltration of the trigeminal ganglion leading to trigeminal denervation has also been reported.4,12,109
Reported Cases of Cranial Nerve Involvement in Primary Sjogren Disease.
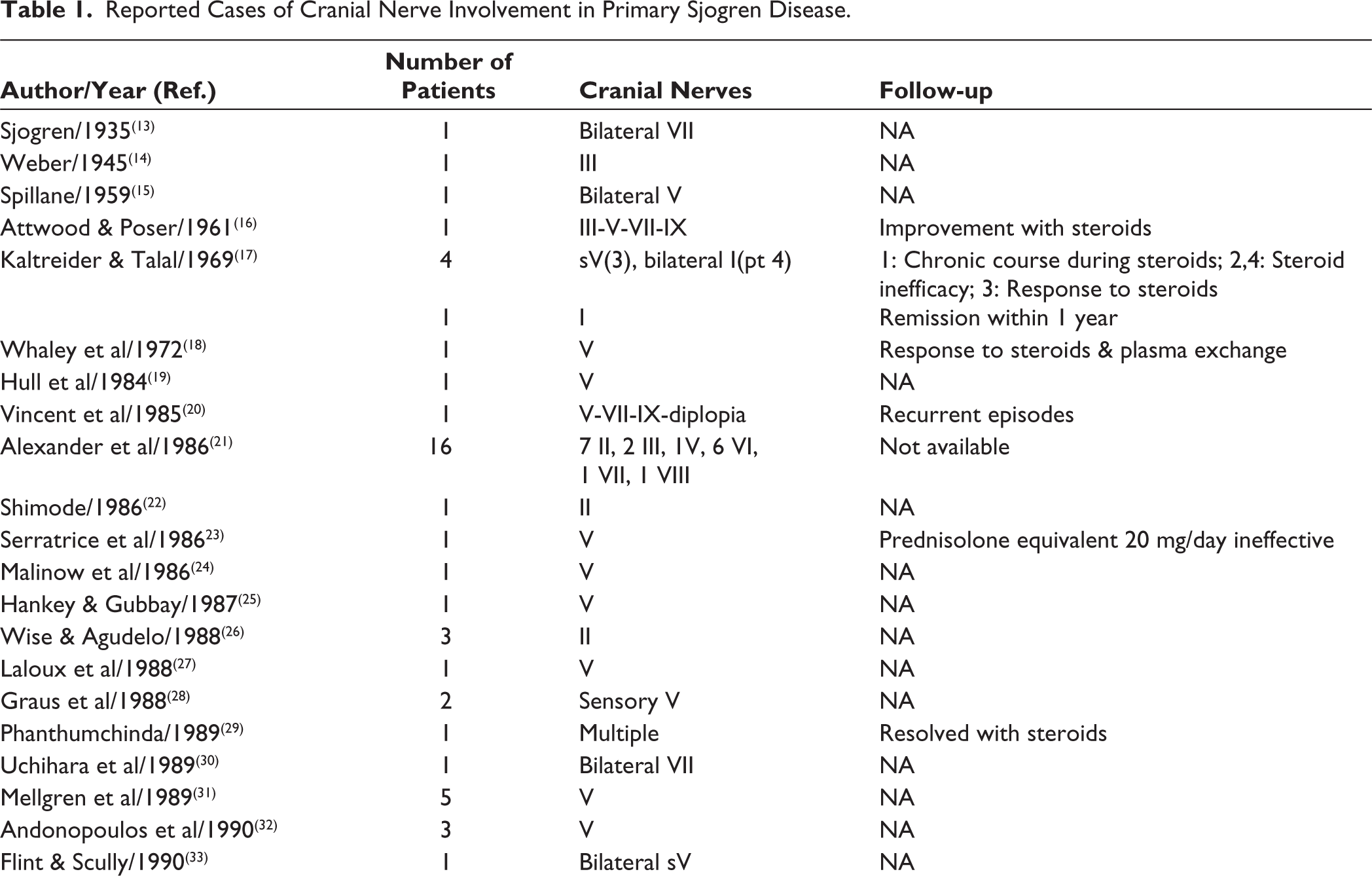

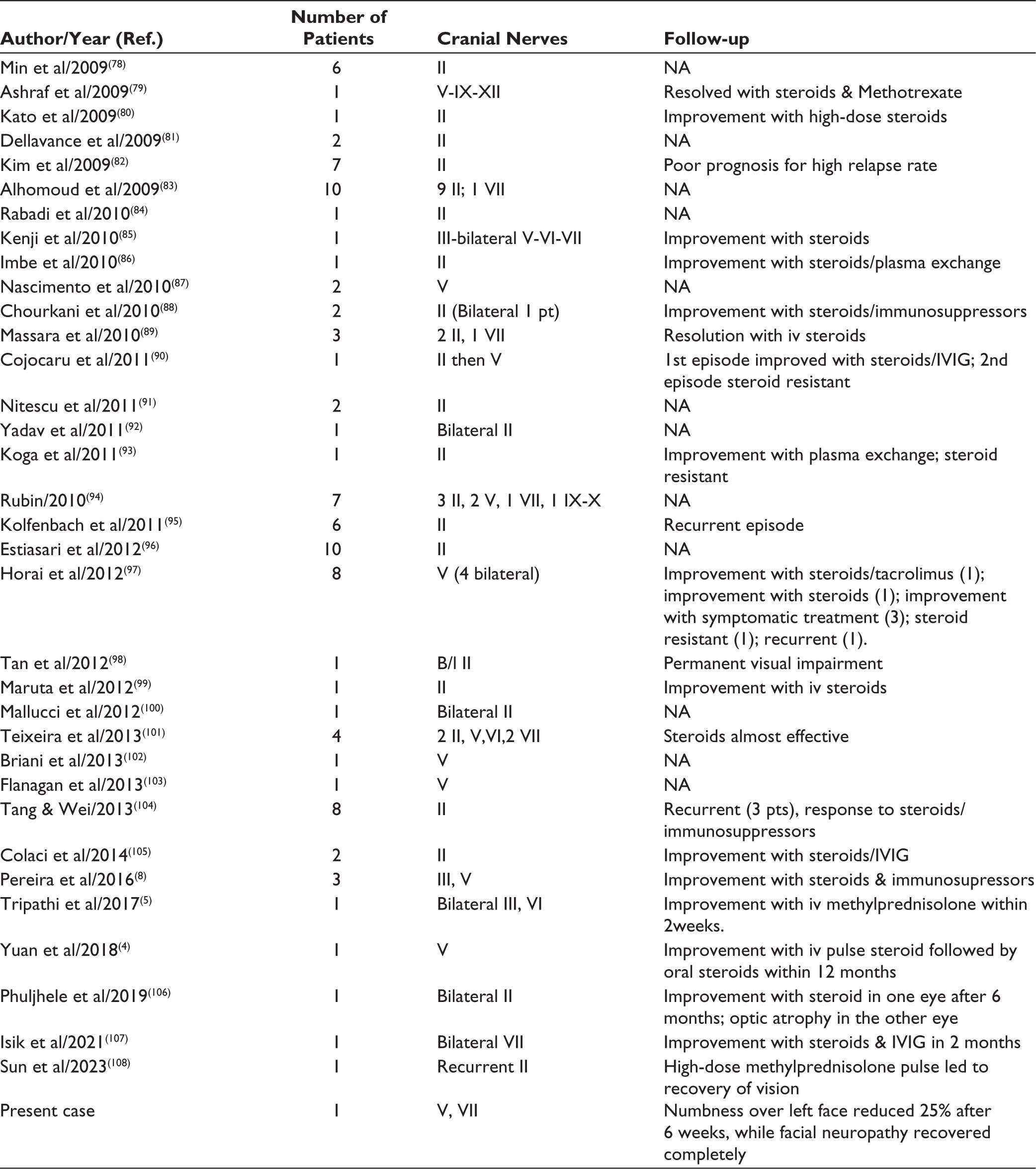
Only 10 cases with third cranial nerve involvement and 21 cases with involvement of the abducens nerve have been reported in the literature. 105 SjD-related optic neuritis is seen in 5.8%–6.3% of reported cases of optic neuritis; it can be unilateral or bilateral, progressing rapidly or insidiously to chronic optic atrophy or evolving as part of the spectrum of neuromyelitis optica. 108 Another study described eight cases of SjD with optic neuritis; all of them were women and four of the eight cases had bilateral optic neuritis. 106
After searching published English literature on cranial neuropathy in SjD, facial paralysis was seen in 23 patients. Ten cases had facial paralysis as part of multiple cranial neuropathies, while 13 had pure facial paralysis; two of them were bilateral. 107
The therapeutic management of primary SjD has not changed considerably. The use of corticosteroids, cyclophosphamide, rituximab and plasma exchange for cranial neuropathies has been proven to be effective.4,110,111 If there is a lack of improvement in immunosuppression, surgical intervention for vascular compression to the nerve may be attempted. 112
Conclusion
Primary SjD should be considered as the underlying aetiology of cranial neuropathy, after excluding common causes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Not Applicable.
Patient Consent
Informed consent was obtained and signed from the patient regarding the use of patient health information for the purposes of writing a case report publication.