
Abstract
Background:
To determine the impact of type-2 diabetes mellitus (T2DM) on the prevalence, clinical features, and outcome of common musculoskeletal disorders at the community level in Bangladesh.
Methods:
This comparative cross-sectional study was conducted among 3,464 individuals from June 2023 to May 2024 in 10 community hospitals of the Diabetic Association of Bangladesh (BADAS) among two population groups (1,732 participants in each group). Participants were selected by purposive sampling. Data were collected through face-to-face interviews and record reviews using a semi-structured questionnaire and a checklist. Data were analysed by using STATA software. Quality of data and ethical issues were strictly maintained.
Results:
The prevalence of musculoskeletal disorders among T2DM participants was 8.43% and among non-diabetics was 3.92%. Age (P < .001), education (P < .001) and occupation (P = .031) were significantly associated with musculoskeletal disorders in T2DM participants. Among T2DM participants, the most prevalent musculoskeletal disorders were osteoarthritis (41.1%), rheumatoid arthritis (17.8%), fibromyalgia (15.1%), prolapsed lumbar intervertebral disc (PLID) (14.4%), and osteoporosis (12.3%). Among non-diabetic participants, osteoarthritis (42.6%) was also prevalent. Other musculoskeletal disorders included PLID (25.0%), rheumatoid arthritis (19.1%), and fibromyalgia (14.7%).
Conclusion:
Present study findings will guide to development of a comprehensive approach and primary care setup for further evaluation and management of diabetic patients having musculoskeletal diseases.
Introduction
Type 2 diabetes mellitus (T2DM) has become an emerging epidemic globally, especially in lower- and middle-income countries. 1 The number of adults in the world with diabetes has increased almost five times in the last four decades, from 108 million in 1980 to 537 million in 2021, projected to be 783 million by the next two decades. 2 However, the relative increase in the prevalence of diabetes between 2021 and 2045 is estimated to be highest in developing countries (almost 21%) compared to developed countries (nearly 12%).1,2 Most of these countries are geographically situated in the Southeast Asian region, which is the residence of almost 90 million people with diabetes. 2 The prevalence of T2DM in this region is nearly 9%, the second highest prevalence after the Eastern Mediterranean region. 3 The prevalence of T2DM in different countries of the Southeast Asian region varies as follows: 6.3% in Nepal, 6.7% in the Maldives, 8.3% in India, 9.8% in Sri Lanka, 12.5% in Bangladesh, and 13.7% in Pakistan.4–9 Bangladesh is a lower-middle-income country in Southeast Asia with a population of almost 170 million. The country has one of the highest prevalences of T2DM, affecting more than 12% of the adult population, resulting in nearly 13 million people living with diabetes.4,7 Apart from demographic change and economic development, this high prevalence is contributed to by a parallel rise in the prevalence of overweight and obesity, the major risk factors for T2DM. 3 T2DM predisposes a wide variety of complications in patients, including renal disease, peripheral neuropathy, retinopathy, and vascular events. Due to its multisystemic nature, additional manifestations, such as musculoskeletal complications, are also possible. 10 Musculoskeletal diseases are a heterogeneous group of chronic conditions generally characterised by musculoskeletal pain, swelling, and reduced mobility. 11 These diseases may lead to multisystemic dysfunction that compromises the patient’s functional capacity, impairs the individual’s quality of life, and imposes a high socioeconomic burden. 12 Musculoskeletal diseases are more common among individuals with T2DM than healthy individuals. It is reported that almost 58% of the patients with T2DM suffer from different types of musculoskeletal disorders. 13 However, the underlying mechanism of most of these musculoskeletal alterations remains unclear. Glycosylation of proteins, microvascular changes, and accumulation of collagen in the skin and periarticular structures might result in changes in the connective tissue, which culminate in musculoskeletal pain, stiffness, and limitations of movements. 14 Despite being a common manifestation of T2DM, there is a lack of comprehensive evidence on the epidemiology of musculoskeletal diseases in patients with T2DM in Bangladesh. A recent study conducted among the general population reported that overall, 30.4% of the population had different musculoskeletal disorders, including low back pain (18.6%), knee osteoarthritis (7.3%), and soft tissue rheumatism (3.8%), the top three conditions. 15 However, this data does not represent the magnitude of musculoskeletal diseases among patients with T2DM. Considering the high burden of musculoskeletal diseases in general population in different countries, a comprehensive study investigating the impact of T2DM on the clinical presentation and outcome of musculoskeletal diseases is necessary. In this context, the community-oriented program for control of rheumatic diseases (COPCORD) model, which was introduced in 1981 by the International League of Associations for Rheumatology, could be used to understand the causes and consequences of chronic musculoskeletal diseases in patients with T2DM. 16 The model has been beneficial for preventing and controlling rheumatic diseases and involves multi-stakeholder efforts in rural, urban, and marginalised urban communities, particularly in low-resource settings. 17 The COPCORD model uses a simple diagnostic questionnaire validated and administered in multiple countries. However, studies based on the COPCORD methodology have shown variations in the prevalence of some rheumatic diseases associated with social stress, ethnicity, genetic characteristics, and geographical area.16,17 However, there is a lack of evidence regarding the prevalence, clinical manifestation, and outcome of these diseases among patients with T2DM. Hence, the purpose of the present study is to determine the impact of T2DM on the prevalence, clinical features, and outcomes of musculoskeletal disorders at the community level in Bangladesh, using the COPCORD methodology. To find out the purpose of this study, a research hypothesis is formulated, and the hypothesis is that patients with T2DM have a greater prevalence of musculoskeletal disorders compared to non-diabetic patients.
Methods
Setting and Program Description
The study was conducted in the community network of the Diabetic Association of Bangladesh (BADAS). BADAS is a countrywide community network for patients with diabetes mellitus (DM) in Bangladesh, which has activities in all 64 administrative districts of Bangladesh. The present study was conducted in two population groups: individuals with T2DM and the healthy population.
Study Design and Study Population
This comparative cross-sectional study was conducted from June 2023 to May 2024. Hence, the population of the present study was adult patients aged more than 18 years with T2DM in Bangladesh who were registered with the community of BADAS, and a similar number of healthy populations aged more than 18 years with no evidence of T2DM from the same community. Patients with type 1 DM, women who are pregnant, and patients with T2DM who have a severe complication need emergency hospitalisation, and patients who did not give consent to participate in the study are excluded.
Sample Size
The sample size for the present study was calculated by using the following formula: n = z2p (1–p)/d2, where z = 1.96 for a 95% level of confidence, p = prevalence of musculoskeletal diseases among patients with T2DM, and d = margin of error. A meta-analysis reported that the prevalence of musculoskeletal disease among patients with T2DM is 58%. 13 Using this information for a 3% margin of error, the formula provided the sample size of 1,040. Considering a 10% nonresponse rate and a design effect of 1.5, the final sample size was 1,732. As the present study had two groups, 1,732 individuals were included in each group of individuals with and without T2DM, resulting in a final sample size of 3,464.
Exposure Assessment
Information on background characteristics, various types of musculoskeletal diseases, and clinical presentation of musculoskeletal disease-related information was collected from eligible participants. Variables related to background characteristics included age (19–40 years, 41–60 years and >60 years), gender (male/female), religion (Islam, Sonaton and others), marital status (unmarried, married and ever married), education (illiterate/primary, secondary, higher secondary and above), occupation (student, service, business/self-employed, housewife, retired/unemployed and others), type of family (nuclear/joint), Body Mass Index (BMI) (Underweight/Normal/Overweight/obese I/obese II), tobacco use (non-user, present user and former user), type of tobacco (smoked tobacco, smokeless tobacco, and both), comorbidity (yes/no) and many more. Various types of musculoskeletal diseases included rheumatoid arthritis (yes/no), psoriatic arthritis (yes/no), gouty arthritis (yes/no), Systemic lupus erythematosus (SLE) (yes/no), osteoporosis (yes/no), fibromyalgia (yes/no), prolapsed lumbar intervertebral disc (PLID) (yes/no), frozen shoulder (yes/no), carpal tunnel syndrome (yes/no), dupuytren contracture (yes/no), stiff hand syndrome (yes/no), trigger finger (yes/no), tennis elbow (yes/no) and many more. Other clinical features of musculoskeletal disease information included clinical features of osteoporosis, osteoarthritis, fibromyalgia, rheumatoid arthritis, and many more.
Sampling and Data Collection Technique
A simple random sampling technique was used to select 10 BADAS community hospitals from among the 64 districts. After randomly selecting hospitals, the purposive technique was used to include patients with T2DM who met the inclusion and exclusion criteria from these community hospitals. This ensures that the sample accurately reflects the target population of interest. Since patients with T2DM were selected purposively, there is a risk of selection bias if the criteria or process favour certain subgroups (e.g., more accessible patients, those more willing to participate, or those from certain demographics), and for this, special attention was given in this regard. To mitigate this bias, all the patients attending these respective hospitals and their attendants were asked regarding their diabetes status, and only those with Type 2 diabetes were included in the study. In addition, a similar number of nondiabetic individuals from the same community were included in the study by household survey. A household listing was prepared with the aid of the BADAS community network, and then, through the systematic random sampling method, households were selected. Systematic random sampling offers a more unbiased approach for selecting households, provided the sampling frame is well-ordered without periodic patterns. Recognising and addressing these biases was crucial for ensuring the validity and generalizability of the study findings.
According to the modified COPCORD questionnaire form, the research team developed a semi-structured standardised questionnaire and a checklist. Data were collected through face-to-face interviews by a trained research associate to collect their socio-demographic and clinical information. The first phase of the interview aims at detecting the respondents with musculoskeletal pain, with some elaboration of the complaints. In the second phase, a clinical evaluation was conducted for all patients associated with a history of pain, and the medical examination was conducted on the same day of the interview; all positive cases underwent clinical assessment. This approach was for both groups. The subjects with suspected musculoskeletal disease were evaluated by specialist rheumatologists to confirm the diagnosis and to provide follow-up care. As the definition of prevalence encompasses both the old and new cases, among the study participants, those who were previously diagnosed with musculoskeletal diseases were also considered as patients with musculoskeletal diseases. Moreover, as the study participants were first interviewed by research associates, who were unaware of participants’ medical condition, participants were enrolled in the study only based on their diabetic status, not based on the presence or absence of musculoskeletal disorders. This process ensured the diagnostic blinding of the study. For the present study, common musculoskeletal disorders, such as osteoarthritis, rheumatoid arthritis, osteoporosis, fibromyalgia, and many more were considered.
Data were checked and verified at the field and central levels to ensure quality. Data were kept safely under the control of the principal investigator. All data were double-checked to ascertain their relevancy and consistency. Incomplete and missing data were excluded. Data were coded, categorised, cleaned, and entered into STATA software.
Statistical Methods
Data analysis was done using STATA software. Categorical variables were presented as frequencies and percentages. Comparisons between the two groups were made with the χ² (Chi-square) test. A P value < .05 was considered significant. All the two-sided statistical tests were performed at a significance level of α = 0.05.
Ethical Consideration
Ethical clearance was obtained from the ethical review committee (ERC) of BADAS. Informed written consent was taken from all participants before data collection.
Results
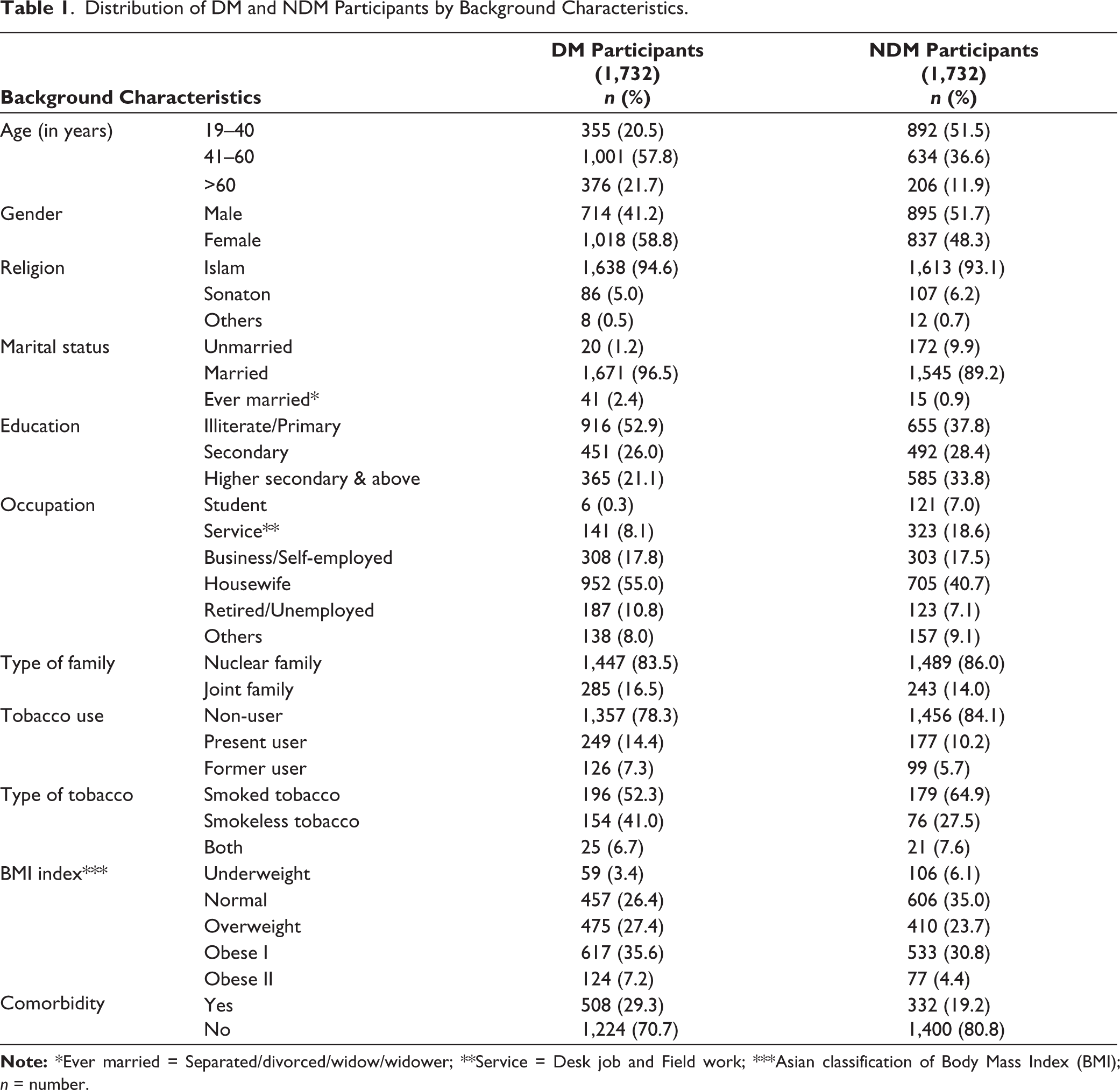
A total of 3,464 participants were interviewed: 1,732 participants with T2DM and 1,732 without T2DM. Among the 1,732 T2DM participants, the majority, 1,001 (57.8%), were 41–60 years old. On the other hand, among the 1,732 non-diabetic participants, the majority, 892 (51.5%), were in the age group of 19–40 years. In the diabetic group, 41.2% were male, and in the non-diabetic group, 51.7% were male. In both groups, a maximum number of participants (52.9% and 37.8%) were illiterate or had only a primary level of education, and most of the DM and non-diabetes mellitus (NDM) participants (55.0% vs. 40.7%) were housewives. Regarding tobacco use, most participants in both groups (78.3% vs. 84.1%) were found to be non-users. Most diabetic participants, 617 (35.6%), were detected as obese; on the contrary, most of the non-diabetic participants, 606 (35.0%), were found to be in the normal weight range. Regarding comorbidity, among the diabetic patients, 508 (29.3%) had some other comorbidity except diabetes (Table 1).
Distribution of DM and NDM Participants by Background Characteristics.
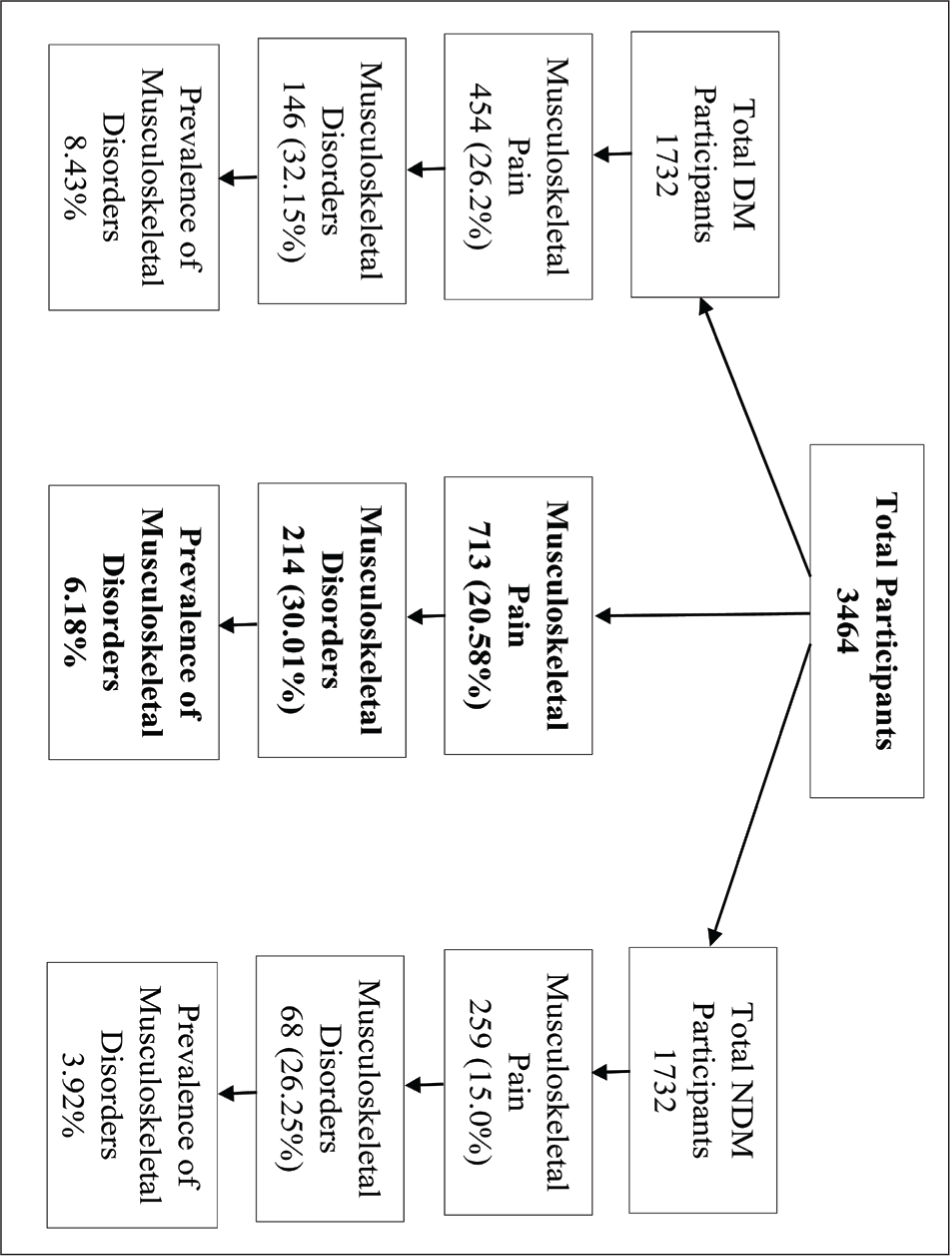
Among 3,464 participants, 713 (20.58%) had musculoskeletal pain, and 214 (6.18%) had musculoskeletal disease. Besides, in 1,732 diabetic participants, 146 (8.43%) had musculoskeletal disease; in contrast, in 1,732 non-diabetic participants, only 68 (3.92%) had musculoskeletal disease (Figure 1).
Flow Chart of Detecting Musculoskeletal Disorders within Diabetic and Non-diabetic Participants.
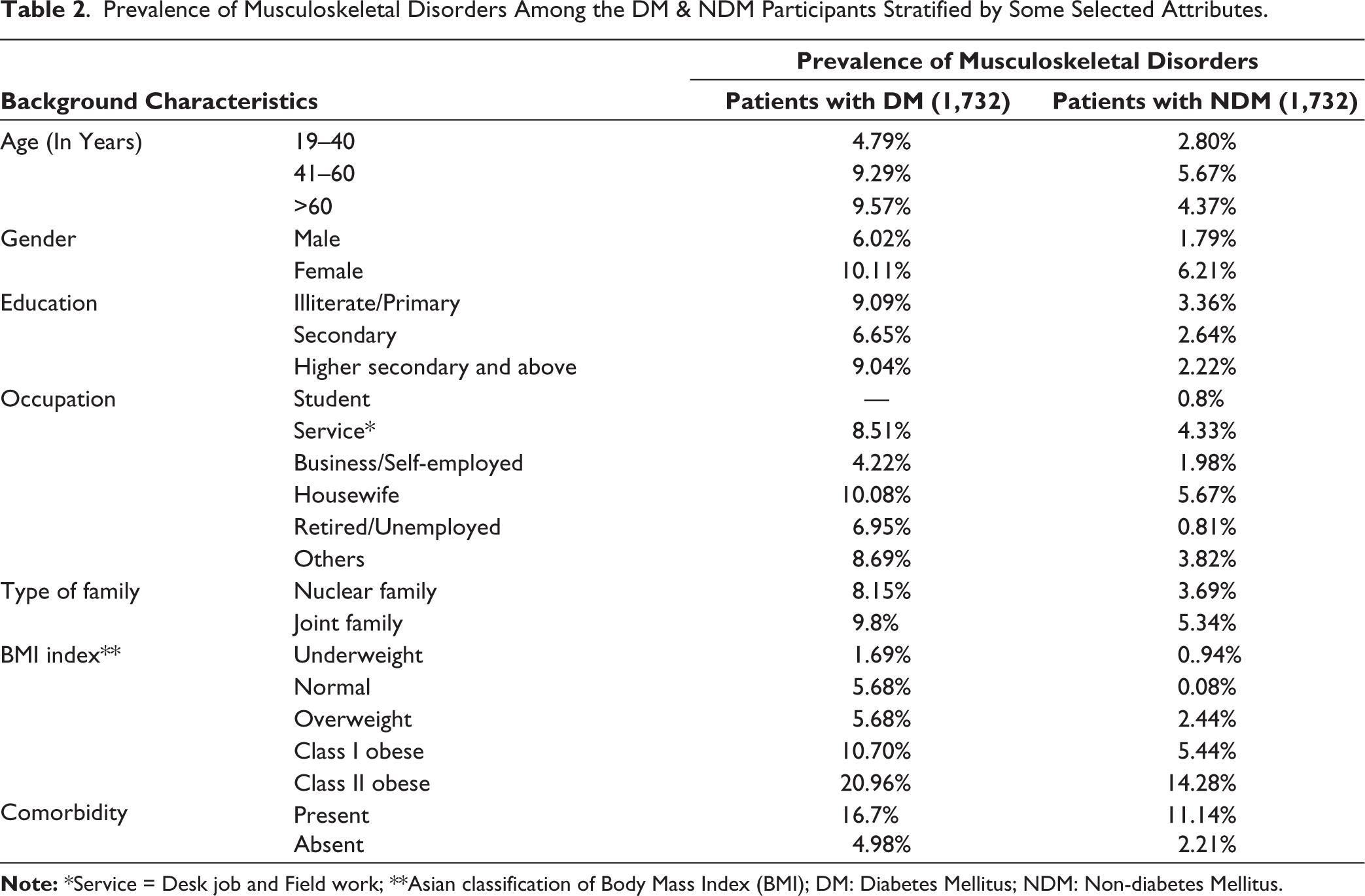
Females were found to have more musculoskeletal disorders in both diabetic and non-diabetic groups (10.11% vs. 6.21%). In the diabetic group, the prevalence of musculoskeletal disorders was high in patients more than 60 years of age (9.57%). Besides, in the non-diabetic group, the prevalence of musculoskeletal disease was high in the 41–60 years age group (5.67%). The prevalence of this disease was high among housewives in both groups (10.8% vs. 5.67%). The prevalence of musculoskeletal disorders was higher in the class II obese group in both DM (20.96%) and NDM (14.28%) participants (Table 2).
Prevalence of Musculoskeletal Disorders Among the DM & NDM Participants Stratified by Some Selected Attributes.
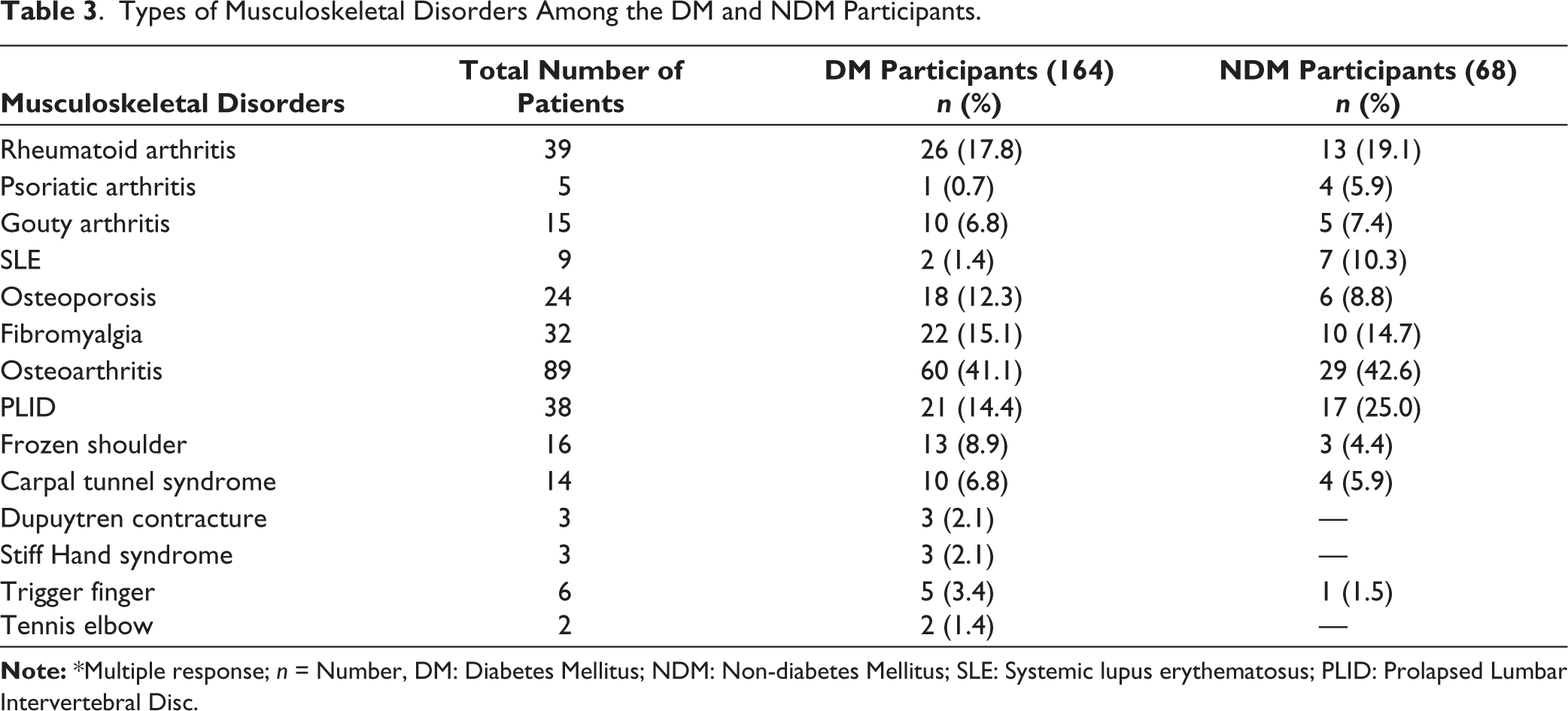
Among T2DM participants, prevalent musculoskeletal disorders were osteoarthritis (41.1%), rheumatoid arthritis (17.8%), fibromyalgia (15.1%), and PLID (14.4%). Among non-diabetic participants, prevalent musculoskeletal disorders were osteoarthritis (42.6%), PLID (25.0%), rheumatoid arthritis (19.1%), and fibromyalgia (14.7%) (Table 3).
Types of Musculoskeletal Disorders Among the DM and NDM Participants.
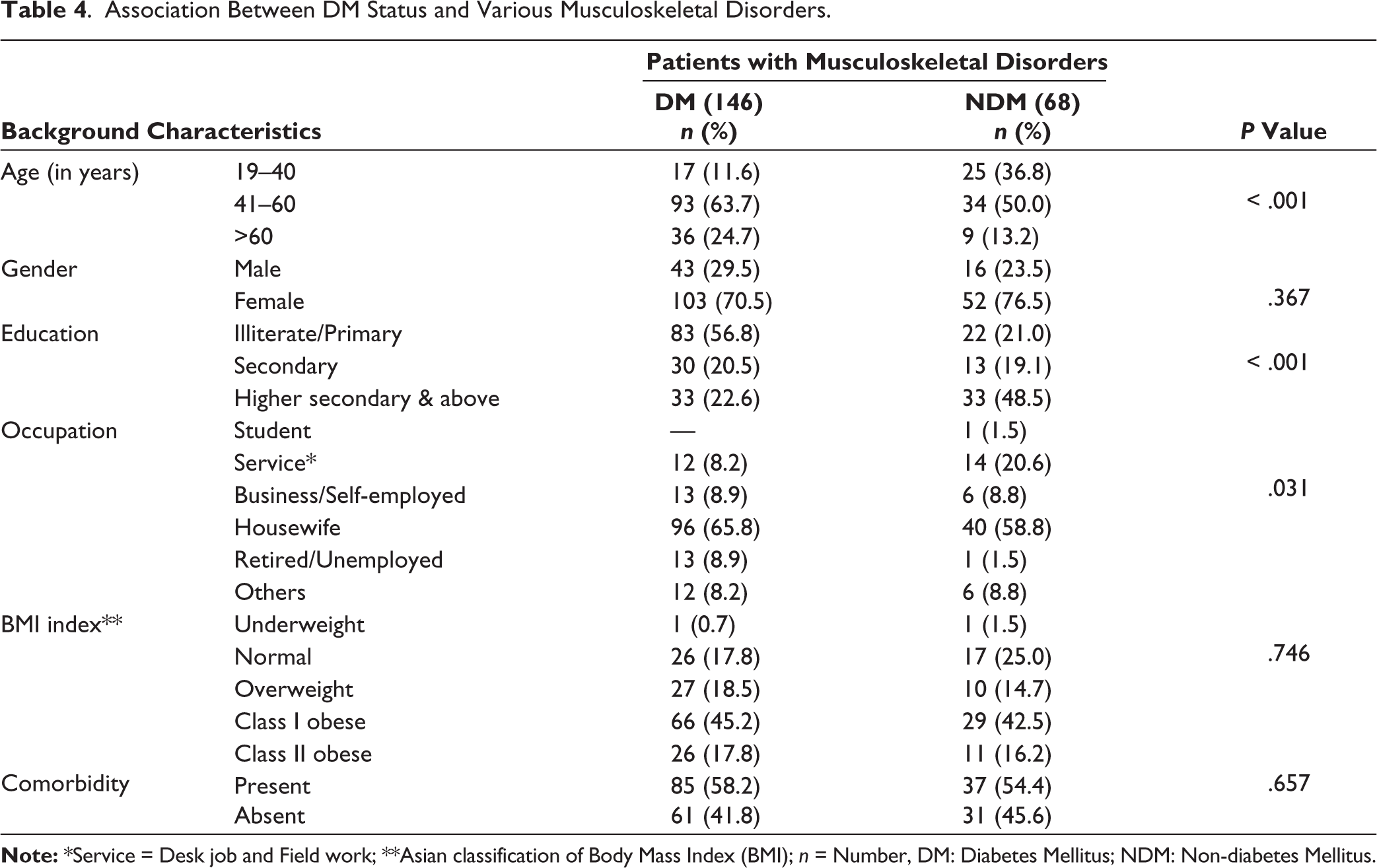
The present study revealed that the differences in developing the musculoskeletal disease among DM and NDM patients were significantly associated with age (P < .001), education (P < .001), and occupation (P = .031) of the participants (Table 4).
Association Between DM Status and Various Musculoskeletal Disorders.
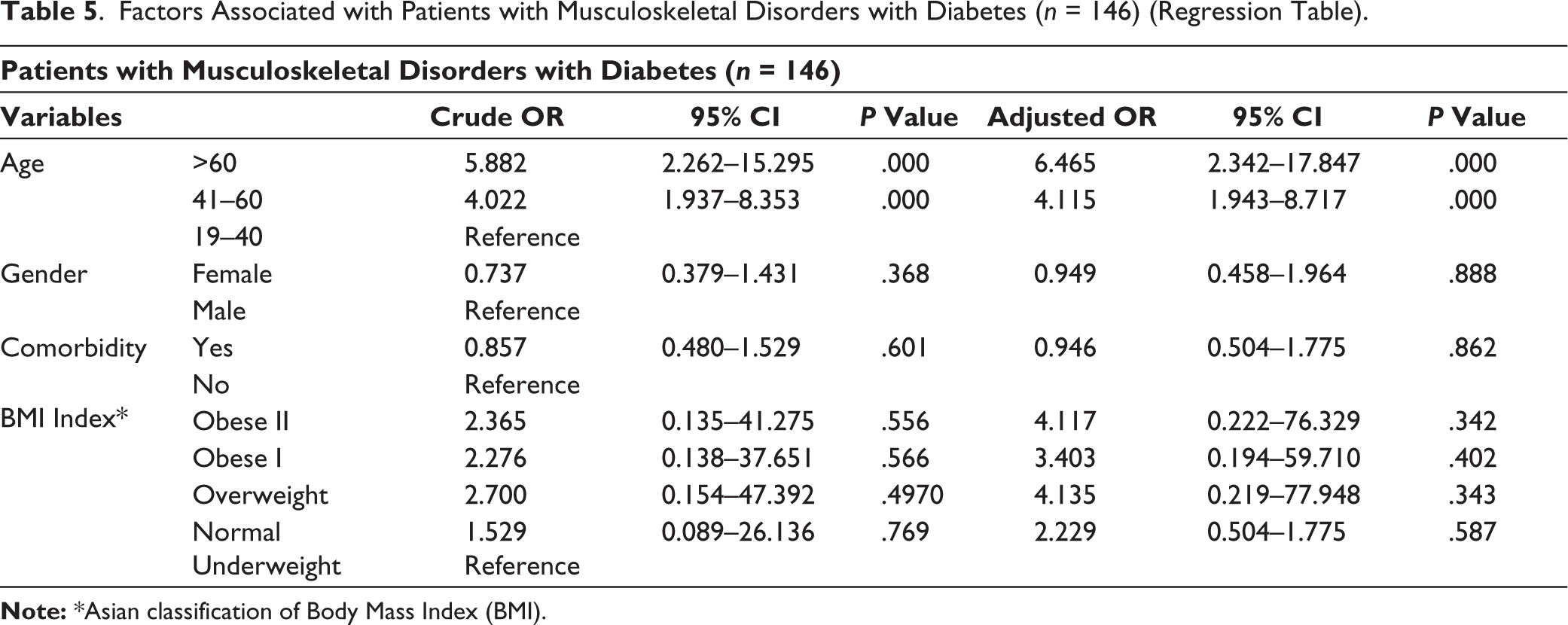
Both bivariate and multivariate analyses showed that age was observed to be a risk factor for having musculoskeletal disease among diabetic patients (P < .05). Though statistically insignificant, obesity or overweight could be a risk factor for having musculoskeletal disease in diabetic patients, as an adjusted odds ratio (AOR) of obesity or overweight was found to be high (Table 5).
Factors Associated with Patients with Musculoskeletal Disorders with Diabetes (n = 146) (Regression Table).
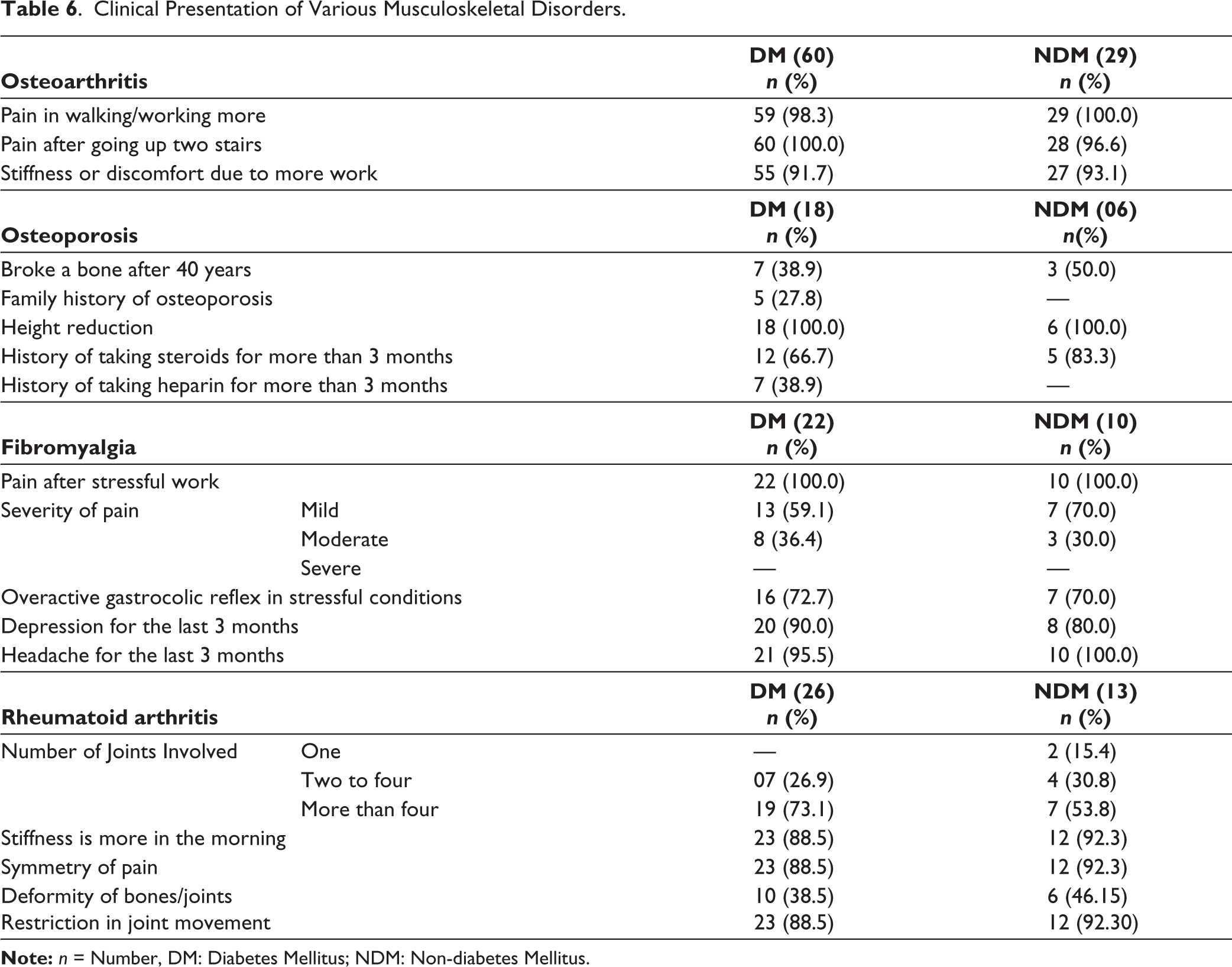
Regarding the clinical presentation, in osteoarthritis, almost all diabetic participants 100% and 96.6% of non-diabetic participants had pain after going upwards or climbing stairs, and mainly knee joints. In patients with osteoporosis, both DM and NDM patients had a history of height reduction, and 66.7% of diabetic and 83.3% of non-diabetic patients with osteoporosis had a history of taking steroids with different doses and duration. In patients with diabetes and fibromyalgia, 72.7% had Gastrointestinal (GI) symptoms. Also, 90.0% of diabetic participants had a history of depression. In rheumatoid arthritis, small joint involvement was more in diabetic patients (73.1%) than in non-diabetic patients (53.8%) (Table 6).
Clinical Presentation of Various Musculoskeletal Disorders.
Discussion
The present study aimed to assess the impact of T2DM on the prevalence, clinical presentation, and outcome of common musculoskeletal diseases at the community level in Bangladesh.
Among the total 3,464 participants, 1,732 were found to be diabetic participants, and 1,732 were found to be non-diabetic participants. Here, most diabetic participants were in the 41-60 age group. However, among the non-diabetic participants, mostly in the age group of 19-40 years. The mean age of the diabetic participants was quite similar to a study in Nigeria. 18 As primarily, Type 2 diabetes developed more frequently in the middle age group, the result of age-related variables might be similar for these two studies.
Furthermore, females (58.8%) were more in the diabetic group, whereas males (51.7%) were more in the non-diabetic group. A study in Nigeria 18 also found that females were more prevalent in the diabetic population. Though the data of the studies contradicts the global data stating DM prevalence is equivalent in people, the results might be similar for the studies due to similar socio-demographic backgrounds.
In the present study, diabetic participants’ occupational profiles indicated a higher prevalence of housewives, followed by businessmen or self-employed, like a similar pattern of study conducted in Ethiopia. 19 This similarity might be identical because the same kind of sedentary lifestyle and indoor activities make them more prone to developing diabetes.
In this study, of the DM population, 14% were current smokers, and 71% had ever smoked. A study in Jordan had similar findings, and in addition, diabetes might help people quit their smoking habit. 20
Regarding obesity, the percentage of obese participants was higher in the diabetic population. Another study conducted in Denmark 21 also found similar findings because obesity is a risk factor for diabetes. Comorbidity was also found to be higher in the diabetic population. Similar findings were found in a Nigerian study. 18 Since diabetes makes people vulnerable to other co-morbid disease conditions, the result might be almost identical.
Musculoskeletal disorders were significantly more prevalent among the participants with T2DM (8.43%) than the non-diabetic participants (3.92%). A study in Nigeria also shows the same finding. 22 These findings support the fact that inflammatory pathways engage in the pathogenesis of diabetes, which in turn increases the risk of the development of musculoskeletal disorders.
The study found that age was significantly associated with the difference in the development of musculoskeletal disorders among DM and NDM participants. A study also found that older age was more prevalent in diabetic people with musculoskeletal disease. 22 It was defined that older age might make people prone to developing musculoskeletal disorders with T2DM.
Education level was found to be significantly associated with the development of musculoskeletal disease. Here, primarily illiterate or having primary education level was high in DM with musculoskeletal disorders. A study found that people with diabetes with no formal education had higher musculoskeletal disease. 22 Illiteracy or lower-level education might make diabetes uncontrolled, and this un-checked diabetes might be the cause of developing musculoskeletal disorders frequently.
The occupation was significantly associated with the development of musculoskeletal disease. As most participants were housewives, their sedentary lifestyle might put them at risk of developing more musculoskeletal disorders with diabetes.
The present study found that there was no significant association between obesity and DM status in patients with musculoskeletal disease. Another study also revealed similar findings. 23
Here in this study, among T2DM participants, prevalent musculoskeletal disorders were osteoarthritis (41.1%), rheumatoid arthritis (17.8%), fibromyalgia (15.1%), and PLID (14.4%). Among non-diabetic participants, prevalent musculoskeletal disorders were osteoarthritis (42.6%), PLID (25.0%), rheumatoid arthritis (19.1%), and fibromyalgia (14.7%). This study shows that fibromyalgia was higher among diabetic patients than non-diabetic patients, and a similar study finding was found in another study. 24 The study shows that among diabetic patients, musculoskeletal disorders affecting with hand and shoulder were more frequent than in non-diabetic participants. A similar result was found in a study. 25 Diabetes might worsen the situation of musculoskeletal disease, particularly affecting the hand or upper extremity involvement. Though there are lack of study regarding the association of DM status with overall musculoskeletal disorders, some studies showed that insulin resistance was a risk factor for some musculoskeletal disease like atherosclerosis. 26 Hyperglycaemia promotes the pathology of musculoskeletal disorder through the formation of Advanced Glycation End-products (AGEs), cross-linking of collagen, microvascular damage, inflammation, and oxidative stress.27,28 Thus, these processes lead to tissue stiffening, fibrosis, impaired repair, and degenerative changes, resulting in the diverse musculoskeletal disorder manifestations observed in hyperglycaemic states, especially in diabetes mellitus. A study showed that chronic hyperglycaemia affected osteoarthritis by causing oxidative stress and low-grade chronic inflammation. 29 Besides, a study also revealed that rheumatoid arthritis and diabetes mellitus had a bidirectional causal chain, so bidirectional surveillance is needed to prevent these two diseases. 30
The present study revealed that the prevalence of musculoskeletal disorders was higher among diabetic patients than among nondiabetics. Age, education, and occupation were significantly associated with the development of musculoskeletal disorders among diabetic patients. So, it is high time to establish a standard clinical guideline for examining and diagnosing musculoskeletal disease among diabetic patients to prevent disability and improve the quality of life in the primary care setting.
With 3,464 participants (1,732 with T2DM and 1,732 without diabetes), this study provided sufficient statistical power to detect meaningful differences and associations and also allowed direct comparison between diabetic and non-diabetic groups, facilitating the assessment of the impact of T2DM on musculoskeletal disorders. As the study was conducted at the community level, the findings of the study enhanced the external validity and generalizability to the broader population in Bangladesh. But the study was conducted in a setting with limited time and resources. Moreover, as the study population was derived from diabetic centres, the results may not represent the overall scenario of the country, but the study results could be a basis for further large-scale studies. Some non-modifiable confounders, like ethnicity, genetic factors for DM, and many more, could not be included in the study. However, strict inclusion and exclusion criteria were used to minimise other biases.
Conclusion
Bangladesh is an overpopulated country, and as a non-communicable disease, diabetes is growing rapidly in our country. Moreover, the data of this study shows that the prevalence of musculoskeletal diseases is more with Type 2 diabetes and age, education, occupation, and many more also play a role in developing musculoskeletal diseases in diabetic people. As an over-burdened country with diabetes, primary prevention of the development of musculoskeletal disease in diabetes is essential. Findings of this study will help in the development of guidelines for lifestyle modification and for developing a screening protocol for at-risk populations of musculoskeletal disease with diabetes. These data will be the basis of further analytical research on diabetes with musculoskeletal disease among those participants who have diabetes and musculoskeletal pain but have not yet been diagnosed with musculoskeletal disease.
Footnotes
Acknowledgements
This research received a grant from the COPCORD Grant 2023. All authors contributed to the design and draft of the work, data collection, and analysis in preparation for this report and agreed to be accountable for all aspects of the job, special thanks to Dr. Jahid Hasan for helping with the protocol write-up. We are grateful to the following physicians of the BADAS for their active cooperation and support: Prof. Dr. Md. Jahangir Alam Sarker, Dr. Md. Abdul Awal, Dr. Umme Sadia Mili, Dr. Mohammad Shah Alam, Dr. Azmiri Zaman, Dr. Rubayat Islam, Dr. Kazi Nazmul Hossain, Dr. Shariful Alam Khan, Dr. Faysal Al Sams Malik, Dr. Rezaul Haider Chowdhury, Dr. Sumon Rahman Chowdhury, Dr. Md. Nurun Nabi, Dr. Md. Sikandar Abu Zafor, Dr. Md. Abdul Hamid Mollah, Dr. Most. Jannatul Ferdous, Dr. Md. Hedyetul Islam, Dr. Nurullah Al Masud. We are grateful to the honourable director general of BIRDEM General Hospital for his kind cooperation to conduct the study.
Authors Contribution
The conception and design of the study—SY, acquisition of data, analysis and interpretation of data—SY, SKM, SJA, RC, RSCS. Drafting the article—SY, SS, SAH; revising it critically for important intellectual content—SY, SAH. Final approval of the version to be submitted— SY, SKM, SJA, RC, RSCS, SS, SAH. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved—SY, SKM, SJA, RC, RSCS, SS, SAH.
Data Availability Statement
Data is not available online.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent Statements
Ethical approval was obtained from the ERC of the BADAS. All participants were informed about the goals and methods of the study. Informed written consent was taken from all patients before data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Community Oriented Program for the Control of Rheumatic Disease (COPCORD) Grant-2023.