
Abstract
Background:
Rheumatoid arthritis (RA) is a persistent polyarthritis with unknown aetiology. The articular structures are destroyed by locally produced degradative enzymes, including aggrecanases, serine proteases and metalloproteinases, that break down the extracellular matrix (ECM). The expression of MMP-2 and MMP-9 occurs mostly in synovial fibroblast and articular cartilage degeneration in RA is influenced by these MMPs. MMP-2 plays an important role in the removal of recruited immune cells, which is essential for reducing inflammatory responses. On the other hand, MMP-9 regulates the invasion and survival of synovial fibroblast cells.
Material and Method:
QIAmp DNA blood mini kit (Qiagen) was used to isolate the genomic DNA. PCR-RFLP method was followed for genotyping MMP-2-735 C/T and MMP-9-1562 C/T gene polymorphisms. GraphPad Prism (version 8.0.2) and SPSS (version 27.0) were used for data analysis.
Results:
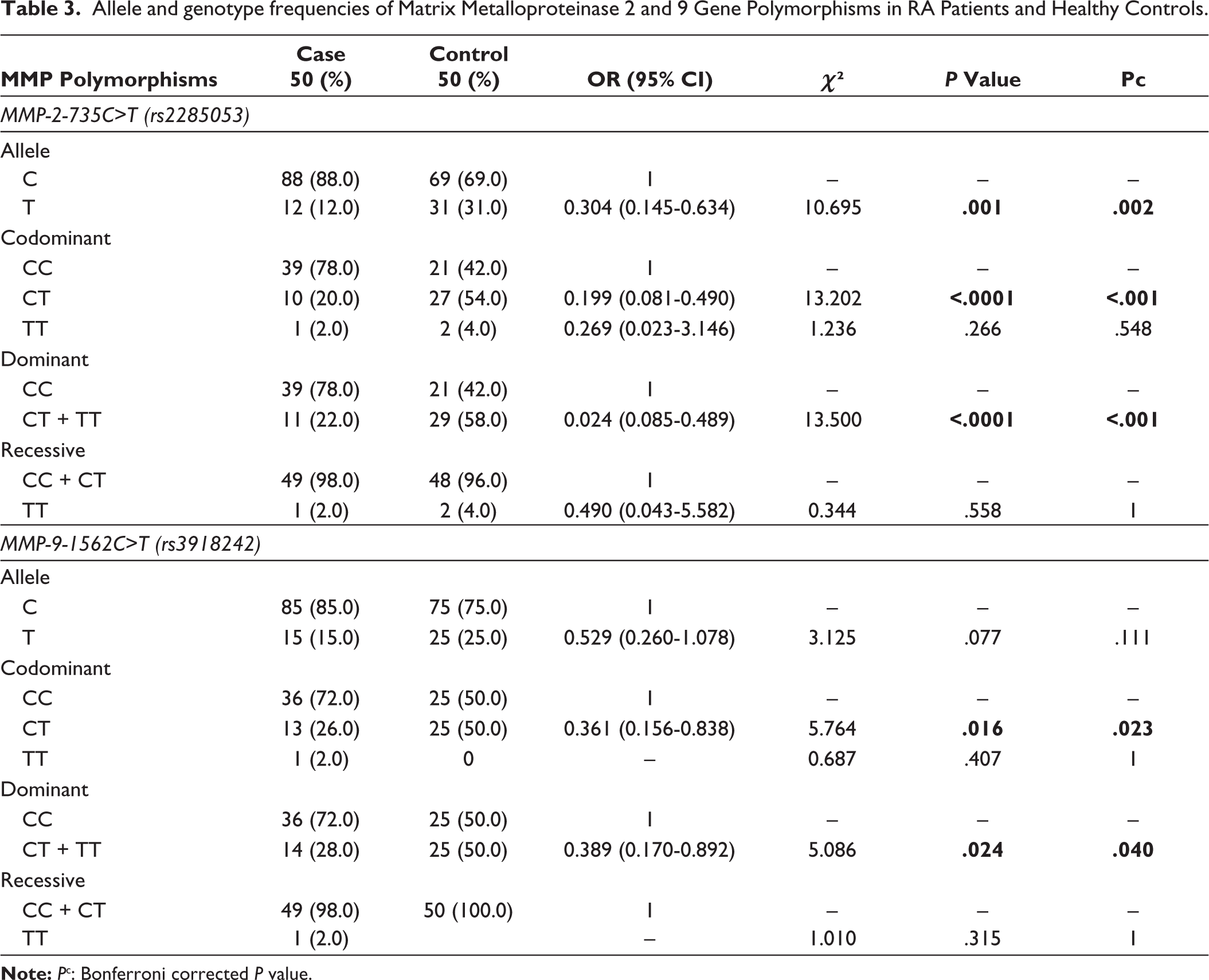
Genotyping analysis revealed significant association between MMP-2 735C/T (rs2285053) gene variant and protection against RA under allele (C vs. T: OR: 0.304; 95% CI: 0.145–0.634; P = .001); codominant (CC vs. CT: OR: 0.199; 95% CI: 0.081–0.490; P = .0001) and dominant (CC vs. CT + TT: OR: 0.024; 95% CI: 0.085–0.489; P = .0001) inheritance models. Further, MMP-9-1562 C/T (rs3918242) variant was also found to be associated with protection against RA under codominant (CC vs. CT: OR: 0.361; 95% CI: 0.156–0.838; P = .016) and dominant (CC vs. CT + TT: OR: 0.389; 95% CI: 0.170–0.892; P = .024) inheritance models.
Conclusion:
The finding of this preliminary study suggests the protective effect of MMP-2 735C/T (rs2285053) and MMP-9-1562 C/T (rs3918242) gene variants against RA in our study population.
Introduction
Rheumatoid arthritis (RA) is a complex autoimmune condition with undefined aetiology. It affects the joint synovium, leading to destruction and deformities of joints. 1 Many cell types, such as lymphocytes, macrophages, etc., surround the synovium. The articular structures are destroyed by locally produced degradative enzymes, including aggrecanases, serine proteases, and metalloproteinases, that break down the extracellular matrix (ECM). 2 Autoantibodies like anti-cyclic citrullinated peptide (anti-CCP) and rheumatoid factor (RF) are considered as the diagnostic markers for RA. 3 An abundance of activated leucocytes containing macrophages, B cells, CD4+/CD8+ T cells, dendritic cells (DCs), natural killer (NK) and mast cells are found in the interstitial tissues underneath the macrophage and fibroblast-rich lining that covers the synovial lesion in RA. 4 The polymorphisms in genetic loci, including HLA-G, 5 soluble HLA-G level, 6 RF and anti-CCP antibodies are the critical determinants of disease progression in RA. Although the aetiology of RA remains unclear, immunologically permissive microvascular or biomechanical elements play a considerable role in RA.
Matrix metalloproteinases (MMPs) comprise over 20 distinct zinc-dependent endopeptidases with diverse physiological functions, including a breakdown of ECM and remodelling of connective tissue. MMP family is involved in the secretion of proteolytic enzymes by an inflammatory synovial tissue, which mediates the destruction of bone and cartilage in RA. 7 MMPs mediate the inflammatory response, and it is shown that variations in MMP gene expression precede several autoimmune diseases, including RA. 8 MMP-2 and MMP-9, belonging to the gelatinase family of matrixins, are thought to be important factors in the articular cartilage degradation through promotion of angiogenesis and direct matrix degradation in RA.9,10 A significant correlation exists between RA and MMP-9 in rheumatoid tissues and cells, and increased synthesis of MMP-9 is believed to originate from synovial cells.11,12 The present study was carried out with the objective to find out the possible association of MMP-2 and MMP-9 gene variants with susceptibility/protection to RA.
Materials and Methods
Study Subjects
In this case-control study, 50 subjects with RA and 50 healthy controls were recruited from Malda Medical College and Hospital, Malda, West Bengal, India. The Institutional Ethics Committee, University of Gour Banga (UGB/IEC (Human)/001–17, Dated: 13.02.2017) approved the study, and all subjects provided their informed consent.
Diagnosis of RA Patients
RA cases were confirmed following the 2010 criteria of the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR). Age and sex matched healthy subjects from the same geographic region without any clinical symptoms and/or history of RA in their families were included as controls.
Collection of Peripheral Blood Samples
A peripheral blood sample (3–4 mL) was collected from each participant by the vein puncture method in anticoagulant-free vacutainer tubes from the Department of Orthopaedics, Malda Medical College & Hospital, West Bengal, India. Sample processing and genotyping experiments were carried out at the Molecular Immunology Laboratory, Department of Zoology, University of Gour Banga, West Bengal, India.
Genomic DNA Isolation
The commercially available QIAamp DNA Blood Mini Kit (Qiagen, Germany, Cat No: 51304) was used for the isolation of genomic DNA from blood samples.
Genotyping of MMP-2-735 C/T and MMP-9-1562 C/T Variants
MMP-2-735 C/T and MMP-9-1562 C/T variants were genotyped by the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method as described previously.13,14 PCR reaction for genotyping these gene variants was comprised of 25 µL reaction mixture containing 10 µL GoTaq Green PCR Master Mix (Promega, Madison, USA, Cat No: M7122), 1 µL each of forward and reverse primer (Eurofins, India, details furnished in Table 1), 2 µL (~50 ng) genomic DNA, and nuclease free water was added to make the final volume. The PCR condition applied was comprised of 95°C pre-denaturation five minutes, followed by 35 cycles of 94°C denaturation 30 seconds, 61°C (MMP-2-735 C/T) and 65°C (MMP-9-1562 C/T) annealing 10 seconds, 72°C extension 30 seconds, and 72°C final extension seven minutes. PCR-amplified products were electrophoresed in 1.5% pre-stained agarose gel (0.5 mg/mL ethidium bromide). For RFLP analysis, 10 µL PCR product of MMP-2 gene was digested with five unit HinfI (Promega, Madison, USA; Cat: R6201) at 37°C for 2.5 hour and 10 µL PCR product of MMP-9 gene was digested with two unit SphI (NEB, Ipswich, Massachusetts, USA; Cat: R0182S) at 37°C for one hour. The digested products were electrophoresed in 3% pre-stained agarose gel, and the gene fragments were visualised and imaged using GelDoc system (GelDoc EZ Imager, Bio-Rad).
Primer Sequence, Annealing Temperature, Restriction Enzyme and Product Size of MMP-2 and MMP-9 Gene Variants.

Statistical Analysis
Data were analysed using GraphPad Prism (version 8, San Diego, California, USA) and SPSS (version 27, Armonk, NY: IBM Corp). Hardy-Weinberg equilibrium (HWE) was determined using STATA (version 13, College Station, TX: StataCorp LLC). χ2 test or Fisher’s Exact test was employed to compare allele and genotype frequencies of MMP-2-735 C/T and MMP-9-1562 C/T variants between the study groups. Odds ratios (ORs) were calculated and reported within the 95% confidence limit. For all analyses, P < .05 was considered to be statistically significant.
Results
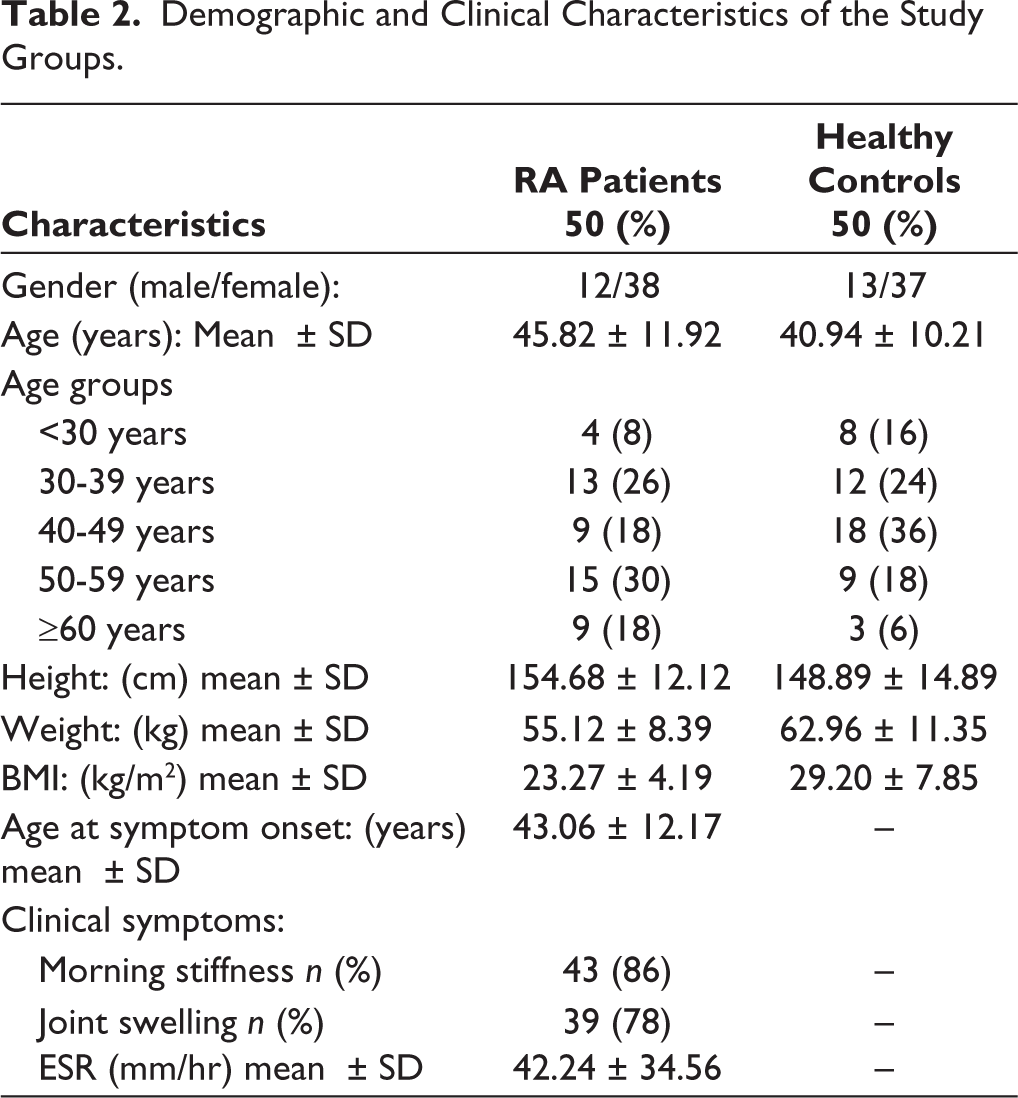
This case-control study included 100 subjects (50 RA cases and 50 unrelated healthy controls) aged ≥20 years with a mean age of 45.82 ± 11.92 years and 40.94 ± 10.21 years for cases and controls, respectively. The RA case group were comprised of 12 (24%) male and 38 (76%) female subjects, and the control group was comprised of 13 (26%) male and 33 (74%) female subjects. The clinico-demographic profiles of the study subjects are summarised in Table 2.
Demographic and Clinical Characteristics of the Study Groups.
MMP-2-735 C/T (rs2285053) Variant
The gel image of the restriction fragments of MMP-2-735 C/T (rs2285053) gene variant is shown in Figure 1. The genotype distribution of MMP-2-735C/T gene variant is presented in Table 3. The frequencies of the C allele (wild type) were 88% versus 69%, and that of the T allele (mutant allele) were 12% versus 31% in RA cases and healthy controls (χ2 = 10.695, P = .001), respectively. The cumulative genotype frequencies of CC, CT and TT were 78% (n = 39) versus 42% (n = 21), 20% (n = 10) versus 4% (n = 27) and 2% (n = 1) versus 4% (n = 2) in RA cases and healthy control subjects, respectively. The result showed that MMP-2 gene 735C/T (rs2285053) variant is associated with protection against RA under allele (C vs. T: OR: 0.304; 95% CI: 0.145–0.634; P = .001); co-dominant (CC vs. CT: OR: 0.199; 95% CI: 0.081–0.490; P = .0001) and dominant (CC vs. CT + TT: OR: 0.024; 95% CI: 0.085–0.489; P = .0001) inheritance models. However, there is a lack of significant association of this gene variant and RA susceptibility/protection under the recessive (CC + CT vs. TT: OR: 0.490; 95% CI: 0.043–5.582; P = .558) inheritance model.
Gel image of MMP-2 735C>T variant by PCR-RFLP method. T allele was digested by HinfI restriction enzyme and produced 338bp and 53bp fragments while C allele remained undigested with 391bp band. Lanes 3, 6 and 7 show homozygous (CC) genotype and lanes 2 and 5 show heterozygous (CT) genotype. Lane 4 shows homozygous (TT) genotype. 50 bp DNA ladder (Promega, USA) was loaded in lane 1.

Allele and genotype frequencies of Matrix Metalloproteinase 2 and 9 Gene Polymorphisms in RA Patients and Healthy Controls.
MMP-9-1562 C/T (rs3918242) Variant
The gel image of the restriction fragments of MMP-9-1562 C/T (rs3918242) gene variant is shown in Figure 2. The genotype distribution of this gene variant is presented in Table 3. Analysis revealed that the frequencies of the C allele (wild type) were 85% versus 75% and that of the T allele (mutant) were 15% versus 25% in RA cases and healthy controls, respectively (χ2 = 3.125, P = .077). The cumulative frequencies of the homozygous dominant (CC), heterozygous (CT) and homozygous recessive (TT) genotypes were 72% (n = 36), 26% (n = 13) and 2% (n = 1) versus 50% (n = 25), 50% (n = 25) and 0 in RA cases and healthy control subjects, respectively. The result showed that MMP-9-1562 C/T (rs3918242) gene variant also provides protective effect against RA under co-dominant (CC vs. CT: OR: 0.361; 95% CI: 0.156–0.838; P = .016) and dominant (CC vs. CT + TT: OR: 0.389; 95% CI: 0.170–0.892; P = .024) inheritance models. Conversely, there was no discernible association between the MMP-9-1562 C/T variant and RA risk/protection under allele (C vs. T: OR: 0.529; 95% CI: 0.260–1.078; P = 3.125) and recessive (CC + CT vs. TT: P = .315) inheritance models.
Gel image of MMP-9 1562C>T polymorphism by PCR-RFLP method. T allele was digested by SphI restriction enzyme and produced 247bp and 188bp fragments while C allele remained undigested with 435bp band. Lanes 3, 4 and 5 show homozygous (CC) genotype and lanes 2, 6, 7, 8 show heterozygous (CT) genotype. 50 bp DNA ladder (Promega, USA) was loaded in lane 1.

HWE Test
The genotype distribution of MMP-2-735C/T and MMP-9-1562C/T gene variants were tested for HWE (Table 4). The genotypes of both MMP-2-735C/T and MMP-9-1562C/T variants were found to exist in HWE (χ2 = 0.129; P = .72 and χ2 = 0.020; P = .89, respectively) in the case group. However, both gene variants deviated from HWE (χ2 = 3.806; P = .05 and χ2 = 5.556; P = .02, respectively) in control group.
Hardy-Weinberg Test for MMP-2-735C>T (rs2285053) and MMP-9-1562C>T (rs3918242) SNPs.

Discussion
The family of endopeptidases that hydrolyse peptide bonds from nonterminal amino acids includes matrixins, also known as MMPs. ECM is mainly composed of type IV collagen, an important constituent of basement membrane (BM), which is degraded by MMP-2 and MMP-9.15,16 It is observed that MMP-2 and MMP-9 are involved in acute inflammatory reaction. 17 MMP-2 comes under the family of gelatinase A, which codes for a 72KD protein, while MMP-9 belongs to gelatinase B family and encodes a 92KD protein. 18 MMP-2 has an impact on clearance of recruited immune cells, which is important for reducing inflammatory responses. 19 MMP-9 accelerates inflammatory cell invasion, migration, and vascular endothelial dysfunction, which are connected to an intensified inflammatory response.15,16 MMP-9 is highly responsive to growth factors and cytokines, while MMP-2 is constitutively produced and comparatively insensitive to them. 9
This study aimed to assess the possible association between MMP-2-735C/T and MMP-9-1562C/T gene variants and susceptibility and/or protection to RA. The finding of our study revealed the protective effect of both gene variants against RA. It is evident that a polygenic component is highly probable to contribute to the susceptibility and severity of RA. 7 Studies have demonstrated the association of MMP genes with RA, but there is paucity of data on MMP-2-735C/T (rs2285053) variant and RA risk/protection. de Rooy et al. reported a significant association of rs11908352 variant of MMP-9 gene with RA. 20 Similarly, Scherer et al. observed a significant correlation between MMP-3 gene variant and RA risk. 7 Furthermore, the genotypes of MMP genes such as MMP-3, MMP-7, MMP-12, may influence the functional condition of RA. 21 Nemec et al. reported an association of MMP-2-790T/G variant with RA but did not find any association of MMP-2-735C/T with RA risk or protection. 22
Although the results of the association studies are inconsistent, it is reasonable to believe that polymorphisms in the promoter region of MMP genes may have some effect on RA. However, this effect may be minimal or confined to a certain disease phenotype. Notwithstanding the contentious evidence about MMP expressions, our findings revealed that the minor allele T of MMP-2-735C/T (rs2285053) and MMP-9-1562C/T (rs3918242) gene variants confers protection against RA. The HWE test revealed deviation of both MMP-2 and MMP-9 gene variants from HWE in control group. Although the exact reason for this deviation is unclear, it may be assumed that the small sample size and random changes in allele frequencies could be the probable causes in our study population. The current study has undoubtedly certain shortcomings, the selection bias was inevitable as the individuals in this hospital-based case-control study were not entirely the representatives of the population under study. In the current study, analysis of genetic polymorphisms with respect to demographic characteristics, environmental and comorbid conditions was not within the scope. Furthermore, the findings of association between MMP-2-735C/T (rs2285053) and MMP-9-1562C/T (rs3918242) variants and protection to RA is limited with a small sample pooled from a single region. To validate our findings, further study in an adequately large sample size of both case and control groups is warranted. Lastly, the RA pathogenesis could be influenced by several factors, such as gene-gene vis-à-vis gene-environment interactions, as there may be subtle differences in genetic and environmental factors for various ethnic populations. It is possible that the MMP-2-735C/T (rs2285053) and MMP-9-1562C/T (rs3918242) gene polymorphisms are coupled to varying levels of genetic risk with the etiopathogenesis of RA in various ethnicities and environmental contexts.
Conclusion
In conclusion, the finding of this preliminary study suggests the protective effect of MMP-2-735 C/T (rs2285053) and MMP-9-1562 C/T (rs3918242) gene variants against RA in our study population. Further, an extensive large-scale case-control study will help to affirm our finding.
Footnotes
Acknowledgements
The authors acknowledge the help received from Laboratory Technicians (MT Lab.) and Paramedics students of Malda Medical College and Hospital, Malda, for providing the blood samples, demographic and clinical data.
Authors’ Contribution
Animesh Chowdhury, MSc, PhD Research Scholar, performed laboratory experiments & statistical analysis and was responsible for the interpretation of the data and drafting of the manuscript.
Ms Sabana Arju, MSc, performed laboratory experiments like DNA extraction, polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP).
Mr Tarun Barman, MSc performed laboratory experiments like DNA extraction, polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP).
Dr Rajat Sarkar, collected blood samples, demographic & clinical data, and also helped in writing manuscript.
Dr Manoj Lama, PhD, Principal Investigator, was responsible for the conception, study design, and interpretation of final data and editing the manuscript. All authors read the final manuscript and approved it for communication.
Availability of Data
The data underlying this article cannot be shared publicly due to the privacy of individuals that participated in the study and the ethical restrictions from the Institutional Ethics Committee, University of Gour Banga. The data will be shared upon reasonable request to the corresponding author with appropriate ethical permission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee (IEC), University of Gour Banga (vide Ref. No. UGB/IEC (Human)/001-17, Dated: 13.02.2017), and Malda Medical College and Hospital (vide Memo no P/MLD-MC/1590).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the participants included in the study.