
Abstract

Introduction
Ankylosing spondylitis (AS) is a chronic multisystem inflammatory disorder affecting the axial skeleton, most commonly involving the sacroiliac joints. It is seen more frequently in males between the second and third decades, out of which around 90% turn out to be HLA-B27 positive. 1 Andersson lesion (AL) is a well-known but rare complication of AS, the incidence of which ranges from 1.5% to 28% of all cases of AS. 2 In the late stages of the disease, the spine demonstrates progressive ossification of the annulus fibrosus, anterior longitudinal ligament, apophyseal joints, interspinous and flaval ligaments, resulting in a complete ankylosed spine, also called ‘bamboo spine’. 2 This serves as a predisposing factor for the development of AL. The exact aetiology of these lesions is unknown but is stipulated to be due to several causes like inflammation, trauma, and pseudoarthrosis. 2 Due to this uncertainty, and the absence of definitive diagnostic criteria, the diagnosis of this condition is often missed. Here is a case series showcasing four patients having AS presenting with ALs at different vertebral levels and its subsequent workup, management and outcome.
Case 1
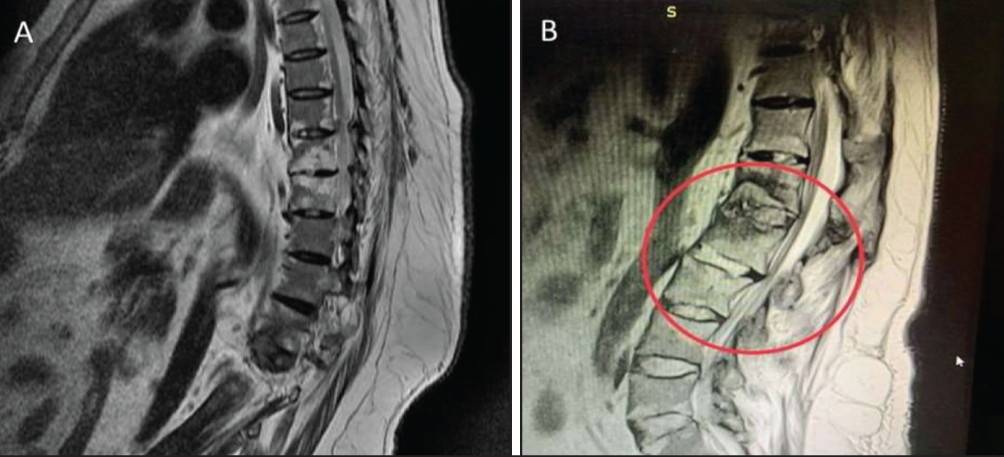
A 53-year-old man presented with low back pain for one year which was insidious in onset, dull in nature, accompanied by early morning stiffness, and not relieved on rest. The patient also complained of restriction of movement. There was no history of fever, night sweats, weight loss, joint pain, skin lesions or trauma. The patient was a known case of hypertension, hypothyroidism, and Type II Diabetes Mellitus. The patient was kyphotic, with tenderness over L1, L2 vertebra. Spine examination was not done due to pain. He was treated empirically with anti-tubercular drugs with suspicion of TB Spine after initial lab and radiological investigations at a primary health care centre. Six months later, the patient had no symptomatic relief. On evaluation ESR was elevated (60 mm/1 hr) and CRP was 136 mg/l (6 mg/L). His hemogram, liver and renal function tests were normal. MRI of dorso-lumbar spine showed erosion of L1 and L2 vertebrae, and destruction of intervertebral disc with peripherally enhancing collection and persistence of lesions even after completion of ATT regimen (Figure 1). A surgical procedure was carried out for D12-L2 stabilisation along with D12-L2 laminectomy and fixation. Histopathological examination of L1-L2 vertebral lesions, the specimen showed abundant fibrin-rich exudates, with foci of inflammatory granulation tissue, containing inflammatory cells and fibroblasts. There was no evidence of suppuration, caseation, granulomata, infective growth, or malignancy. Routine gram stain, AFB stain and cultures for pyogenic and TB were negative. Tissue TB PCR was negative. Based on the histopathology, radiological findings and ruling out infection (both pyogenic and Tuberculosis), final diagnosis of AL with AS was made. The patient was started on Tofacitinib 11 mg once daily and Etoricoxib. He had relief during follow up four weeks later. In this case AL was the presenting feature of AS.
(A) MRI Spine Showing Erosion of L1, L2 Vertebrae, Destruction of Intervertebral Plate. (B) MRI Dorsal Spine Showing Persistence of Lesions After Completion of ATT.
Case 2
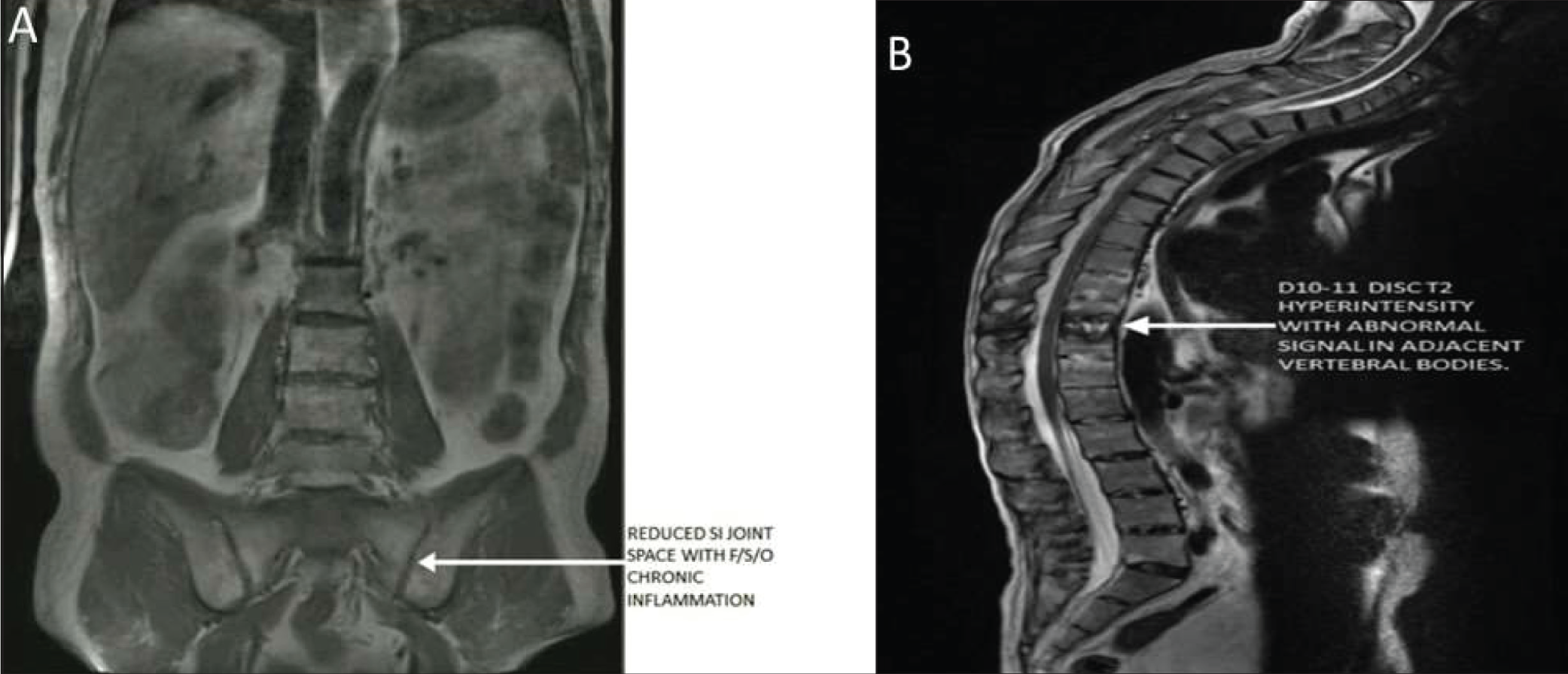
A 45-year-old man who was a known case of AS for 15 years and had been treated with nonsteroidal anti-inflammatory drugs and sulfasalazine (2 g/day) for the same previously, presented with subacute-onset, dull pain over the mid-back region not relieved by rest. On examination, he had kyphosis with restricted neck movement and tenderness over the mid-thoracic region without a history of trauma. Investigations revealed an erythrocyte sedimentation rate of 8 mm/1st h (10 mm/h-20 mm/h), and C-reactive protein of 2.35 mg/L (0 mg/l-6 mg/l). MRI spine showed ossification of the anterior longitudinal ligament, shiny corners of the lower dorsal and lumbar vertebrae, and healed inflammatory changes of the bilateral sacroiliac joints as seen in Figure 2. D10-11 disc appeared hyperintense on T2 weighted images and hypointense on T1 weighted images with no paraspinal collection, suggestive of non-infective spondylodiscitis, that is, AL. Blood culture, procalcitonin, Mantoux test, and TB quantiFERON tests were negative. Chest X-ray was normal. He was started on Injection Etanercept 50 mg subcutaneously, once weekly and after four weeks he showed significant improvement in pain and mobility. This case was previously published as an image in rheumatology. 3
(A) MRI Imaging Revealing Reduced SI Joint Space and Chronic Inflammation Suggestive of Sacroiliitis. (B) MRI Imaging Revealing Hyperintensity in D10-11 Disc with Abnormal Signal in Adjacent Vertebral Corpus on T2 Weighted Images Suggestive of Andersson Lesion.
Case 3
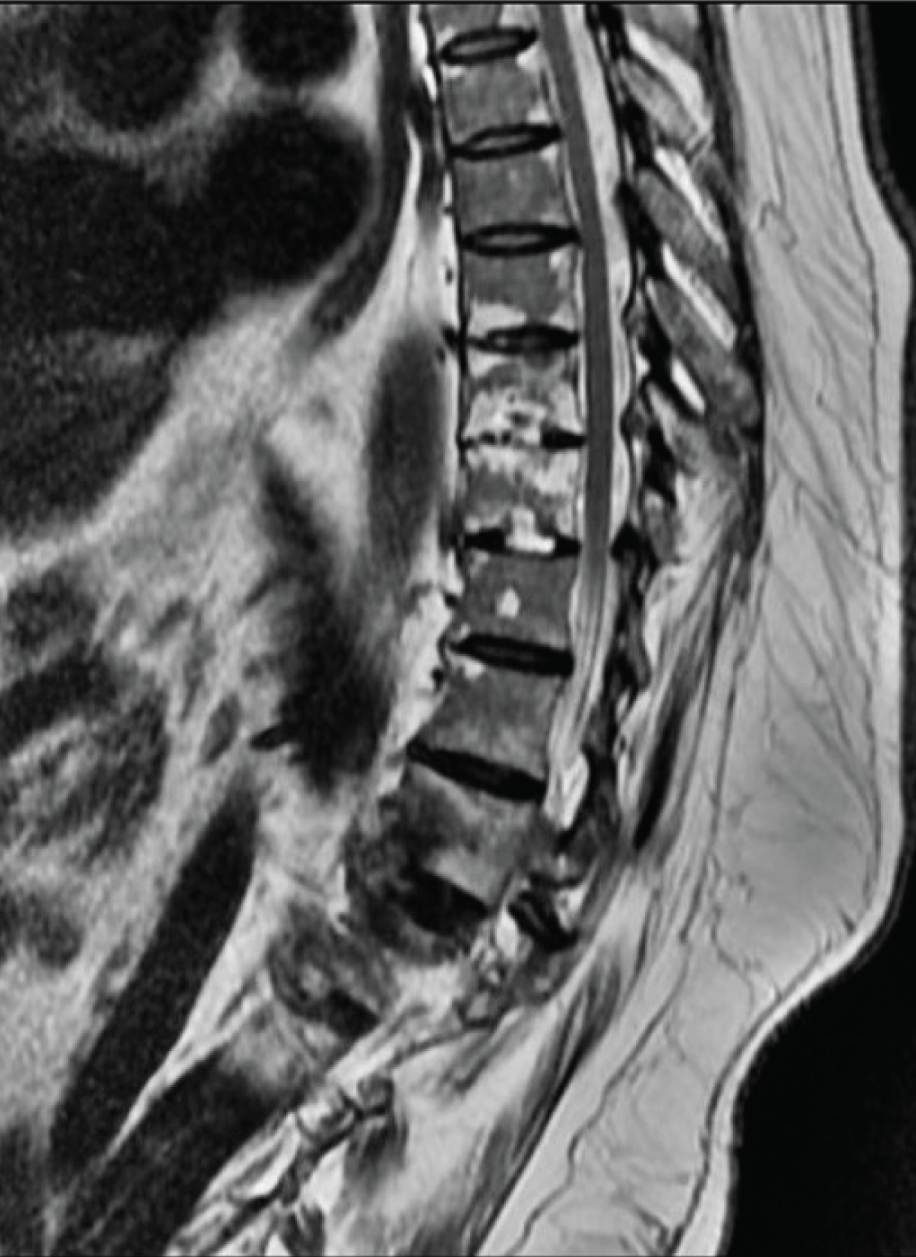
A 31-year-old male presented with complaints of insidious, dull aching, continuous lower back pain since one year associated with morning stiffness that worsened as the day progressed with no relief on rest. He was diagnosed with AS nine years back and was treated for the same. He reported increasing difficulty with ambulation and activities of daily living. There was no peripheral joint involvement or history of trauma, fever, weight loss or night sweats. Movement of the spine was restricted along with tenderness over the T12-L1 segment of the dorso-lumbar spine. ESR was 80 mm/1st hr and CRP was 70 mg/L, hemogram, liver and renal function tests were normal. Mantoux and QuantiFERON gold tests were negative. MRI spine showed hyperintensity in T12/L1 disc with erosion in adjoining endplates in T2 weighted images along with intervertebral disc destruction and disc space narrowing suggestive of AL (Figure 3). The patient was treated with Tofacitinib 11 mg once daily and Tablet Etoricoxib. He responded well and reported symptomatic relief during subsequent follow-ups.
MRI Imaging Showed Hyperintensity in T12/L1 Disc with Erosion in Adjoining Endplates Along with Intervertebral Disc Destruction and Disc Space Narrowing Suggestive of Andersson Lesions.
Case 4
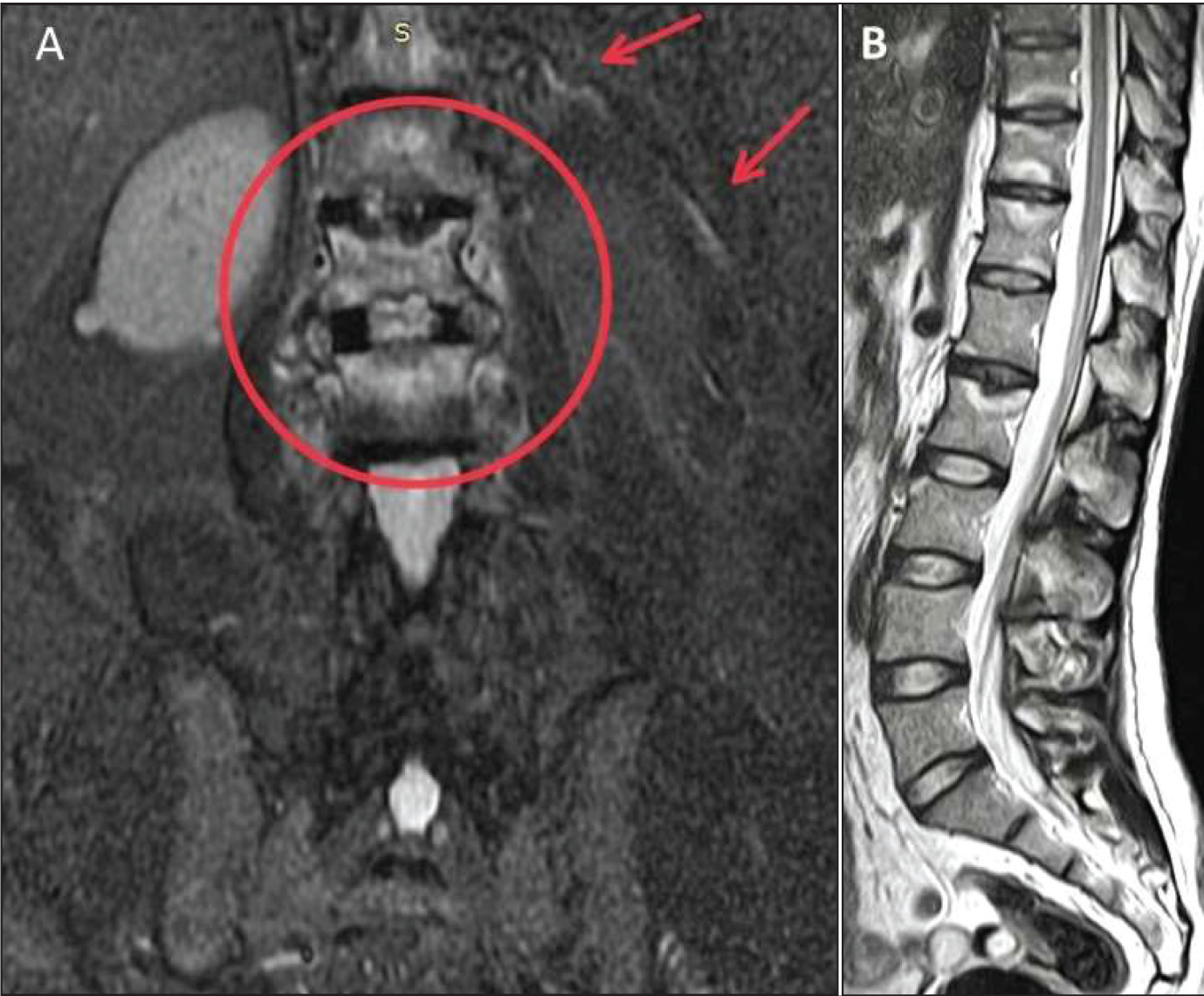
A 45-year-old male with no known co-morbidities presented with complaints of persistent low back pain for two years with progressive worsening over the last six months along with stiffness in the hip joint which was interfering with his daily activities and mobility. There was no history of trauma, recent infections, rashes, fever, or peripheral joint involvement. He reported having minimal to no relief in symptoms with NSAIDs or with rest. He was previously diagnosed as AS 10 years back. On examination, he was found to have kyphosis, decreased spinal mobility, especially lumbar flexion and tenderness over the dorso-lumbar spine and sacroiliac joints. ESR was found to be 40 mm in one hour and CRP was 13.8 mg/l. CT Pelvis showed bilateral sacroiliitis and sclerosis and Schmori’s nodes at dorso-lumbar vertebrae. MRI Spine showed focal erosion and end plate changes appearing hyperintense on T2 weighted images in the anterior aspect of end plates of cervical, thoracic, and lumbar vertebrae at multiple levels consistent with Romanus lesion and end plate depressions at multiple levels with minimal adjacent marrow edema in lower thoracic and lumbar vertebrae, consistent with AL (Figure 4). Based on clinical suspicion, lab findings, and radiological evidence, he was diagnosed with ALs and was managed conservatively with tablet tofacitinib, injection methylprednisolone pulse and tablet etoricoxib. On subsequent follow-up four weeks later, he reported pain relief and regression of symptoms.
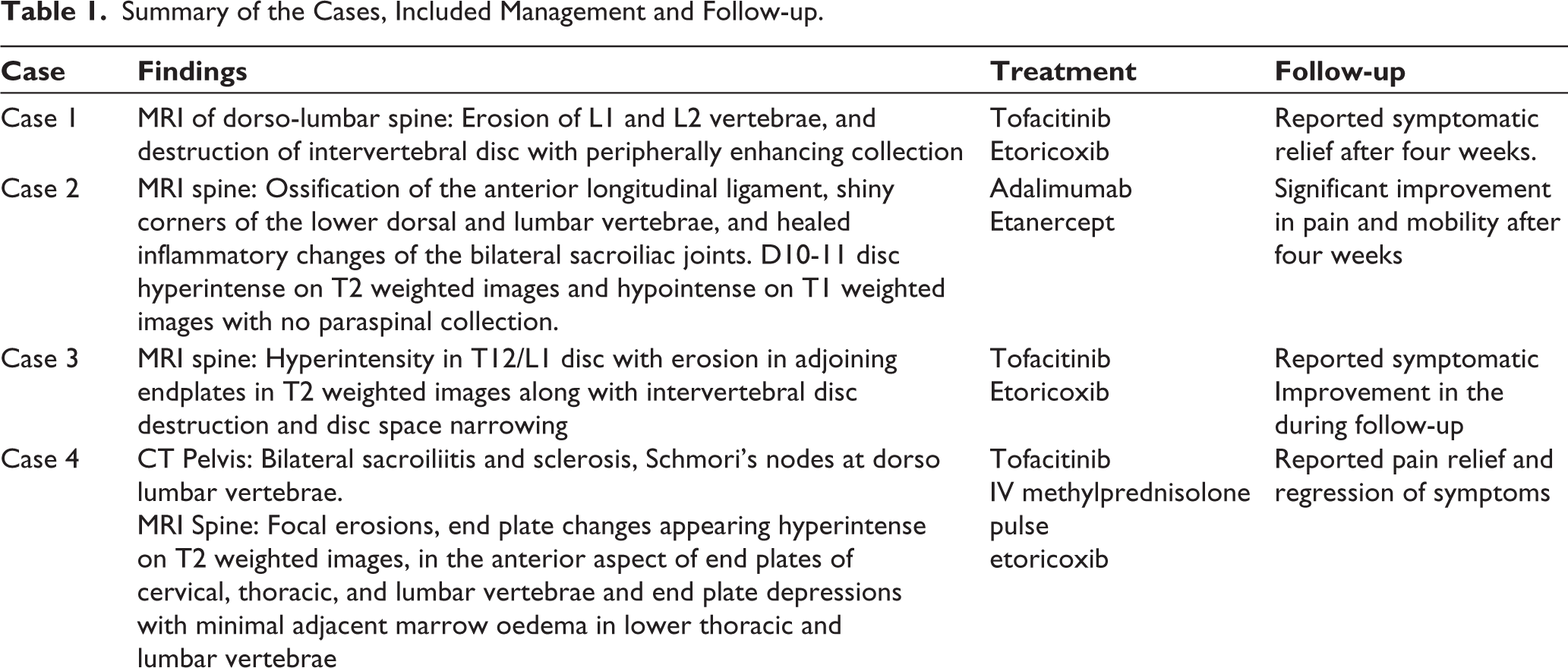
Radiological findings, management and outcome has been summarised in Table 1.
(A) Coronal and (B) Sagittal Section Revealing Focal Erosions, End Plate Changes Appearing Hyperintense on T2 Weighted Images Adjacent Marrow Oedema in Lower Thoracic and Lumbar Vertebrae With Sacroiliitis.
Summary of the Cases, Included Management and Follow-up.
Discussion
Seronegative spondyloarthropathies are a group of joint disorders consisting of AS (most common), IBD-associated arthritis (e.g., Crohn’s disease or Ulcerative colitis), reactive arthritis, Psoriatic arthritis, and undifferentiated variety. ALs characteristically show disc space narrowing, destruction of vertebral end plate and sclerosis of adjacent bone on radiological imaging and appear hyperintense on STIR images and hypointense on T1-weighted images. The significance of AL is that it occurs frequently in AS of longer duration and mimics infection and malignancy. Since the first such case reported by Andersson, 4 there have been various theories about the aetiology of these lesions including inflammation, infection, mechanical stress, or trauma. Lohr et al., described a patient with AS who had a history of intravenous drug abuse and was diagnosed with T11-T12 spondylodiscitis. The patient underwent a right thoracotomy, but no histology or lesions were obtained post-surgery. 5 Similarly, biopsies have been performed in patients with an AL in many studies, but positive cultures have never been found and tuberculosis was never detected.6-8
Inflammation
AS is characterised by spinal inflammation, which has led many authors to focus on an inflammatory aetiology for AL. Romanus was the first to describe ‘anterior spondylitis’, which involves marginal erosions of the anterior vertebral corners, linked to inflammation of the anterior annulus fibrosus in patients with AS, which was noted in a few of our reported cases.9,10 Fragments of necrotic bone and cartilage are frequently observed along the vertebral border. Mild inflammatory changes may also be present, characterised by the infiltration of plasma cells, lymphocytes and, less commonly, macrophages. Other factors supporting an inflammatory origin of ALs include the development of lesions early in the course of AS, before the spine becomes fully ankylosed, as well as the presence of multiple lesions within a patient. Other contributing factors are the occurrence of asymptomatic lesions and the lack of a trauma history in many patients. 2 Pseudoarthrosis could be caused due to either localised lesions that always have an inflammatory origin or extensive lesions with or without fractured posterior elements resulting from mechanical factors.
Trauma or Mechanical Stress
In many patients, AL develops following trauma and is associated with spinal fractures. The ankylosed and osteoporotic spine in individuals with AS is particularly prone to fractures due to the loss of spinal mobility.10,11 In a long ankylosed thoracolumbar kyphotic spinal column, local stresses near the thoracolumbar junction are increased exponentially. Besides the thoracolumbar junctions, areas that are affected by increased stresses are the levels proximal to the lumbosacral junction, where conditions like disc degeneration and spondylolisthesis occur in the non-rigid spine. The thoracolumbar and lumbar regions of the spine are more susceptible to shearing or distractive forces due to the effects of gravity on a kyphotic spine. Traumatic fractures of the cervical spine are also common in patients with AS, but the development of an AL is less frequently observed at this location owing to less severe mechanical loading in this area of the spine.12-14
Surgical Resection
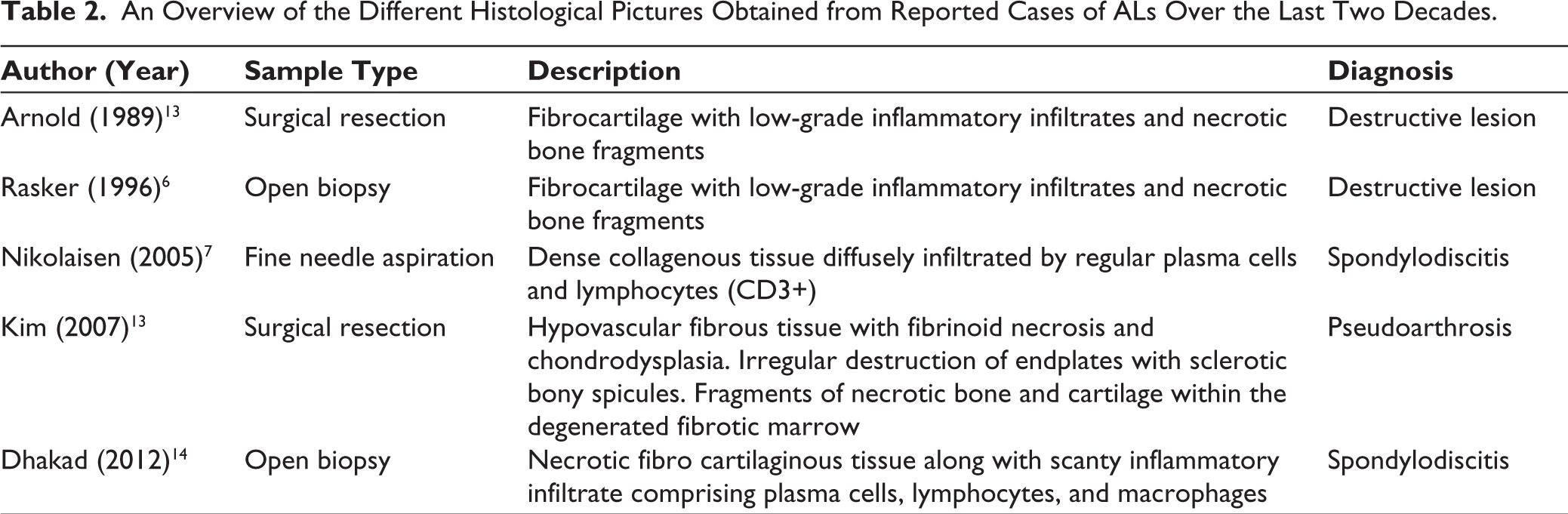
In the first case of the present series, the specimen was obtained by surgical resection and showed abundant fibrin-rich exudates, with foci of inflammatory granulation tissue, containing inflammatory cells and fibroblasts. This is similar to the previously published literature. We have compared the different studies that underwent surgical procedures and their histopathological pictures (Table 2).6,7,13-15
An Overview of the Different Histological Pictures Obtained from Reported Cases of ALs Over the Last Two Decades.
Investigations
While conventional radiographs are the first choice for initial imaging, CT and MRI provide more detailed and sensitive information about AL in AS. Conventional radiographs help locate the exact location of the lesion. Angular Kyphosis and spondylolisthesis are common features. Key findings include osteolytic destruction, reactive sclerosis, vertebral osteophytes, and potential fractures of the posterior elements. CT offers better details as compared to conventional radiographs and identifies osteolysis, fractures, non-fusion of facet joints, vacuum phenomena, and paraspinal swellings. 2 A study found that 77% of lesions missed by conventional radiographs were detected by CT scans, although radiation exposure still poses a significant risk. 16 MRI is considered the best option for detecting AS. ALs characteristically show disc space narrowing, destruction of vertebral end plate and sclerosis of adjacent bone on radiological imaging and appear hyperintense on STIR images and hypointense on T1-weighted images. This lesion is often misdiagnosed as Pott’s spine or malignancy due to lack of awareness and similar appearance on MRI. 17 Bone scintigraphy may be useful but has limited documentation and sensitivity.
Treatment
Conservative management without surgical intervention is the mainstay of treatment in this condition as reported in most of our cases. Non-steroidal anti-inflammatory drugs (NSAIDs) are commonly used during active phases of AS, but newer therapies like anti-TNF-α drugs, for example, infliximab, etanercept, adalimumab are being used these days. 2 There are not many studies reporting definitive management for ALs, however, recently biologics have gained popularity in treating such cases. Role of new drugs like Tofacitinib in AL is yet to be proved. Three of our patients were given Tofacitinib out of which two responded to the treatment. The previously published case is being maintained on Tofacitinib. Surgical treatment is considered for patients with severe pain, worsening symptoms, kyphotic deformities, or neurological deficits and is done for spinal decompression, stabilisation and fusion.
Conclusion
AL is a late manifestation of AS. One of the patients presented with AL as a diagnostic feature of AS. A diagnosis of AS with AL, makes it an unusual presentation. This case series sheds light on the importance of imaging, biochemical as well as histopathological investigations in clinching the diagnosis of AL. We have outlined the workup and treatment discourse of four patients with AS and comprehensively compared and contrasted the same with other work published about AS with AL previously.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.