
Abstract

Dear Editor,
Since the beginning of this millennium, several workers, mainly led by Paul Ridker, have shown a close relationship between inflammation, especially chronic inflammation, as detected by high sensitivity C-reactive protein (CRP), and atherosclerotic cardiovascular disease (ASCVD). 1 Several studies have highlighted the critical link between chronic inflammation and premature or increased risk of ASCVD in patients with ankylosing spondylitis (AS) and other spondyloarthritis (SpA) conditions.2-9
Nonsteroidal anti-inflammatory drugs (NSAIDs) are a cornerstone in managing SpA due to their efficacy in reducing inflammation and pain. There are a series of high-class publications that provide strong evidence supporting the continuous use of NSAIDs in AS and SpA as a strategy to slow radiographic progression and act as disease-modifying agents compared to on-demand use.
Wanders et al., evaluated the effects of continuous versus on-demand use of NSAIDs on radiographic progression in AS and showed that continuous NSAID use significantly slowed the progression of spinal radiographic damage compared to on-demand use, suggesting disease-modifying properties. 10
The INFAST trial demonstrated that patients with AS who used NSAIDs continuously had significantly less radiographic progression compared to those using NSAIDs on-demand. The study concluded that continuous NSAID use has a disease-modifying effect in AS by reducing inflammation and preventing new bone formation. 11
Dougados et al., in their review discussed the role of NSAIDs not only as symptom-relievers but also as potential disease-modifying agents in AS. They reviewed evidence from clinical trials that support continuous NSAID use for reducing radiographic progression and highlight the mechanisms behind their effects on bone formation. 12
In the OASIS Cohort study, continuous use of NSAIDs was associated with a significant reduction in radiographic progression of AS, particularly in patients with elevated CRP. This study supports the disease-modifying role of NSAIDs in patients with higher inflammatory activity. 13
Sieper et al., in their review, explore the potential of NSAIDs in modifying disease progression in SpA and AS. The authors discuss the findings from several key studies and trials that indicate continuous NSAID treatment reduces radiographic progression, compared to on-demand use, and highlight the mechanisms of action in bone metabolism and inflammation control. 14
The DESIR cohort study investigated radiographic progression in patients with early axial SpA and confirmed that continuous NSAID use reduced progression compared to on-demand use. This study underscores the importance of NSAID therapy in managing early-stage disease to prevent structural damage. 15
The GESPIC Cohort, long-term observational study, evaluated NSAID use over eight years and confirmed that continuous NSAID therapy significantly reduces radiographic progression in patients with axial SpA, adding further evidence for their disease-modifying potential. 16
NSAID use, however, has been associated with cardiovascular (CV) risks, which vary among different NSAIDs. Gurkirpal Singh was the earliest worker to draw attention to the adverse CV effects of prolonged NSAID use, with a specific focus on COX-2 inhibitors.17,18 His work has played a significant role in shaping our understanding of the balance between the benefits of NSAIDs and their potential CV harms. Since then, several additional studies (like meta-analysis by Trelle S et al., McGettigan P et al., Bally et al., Coxib and Traditional NSAID Trialists’ (CNT) Collaboration, review by Nissen et al., Ray et al., Helin-Salmivaara et al.) have been published that underscore the adverse CV effects of prolonged NSAID use, particularly in terms of increasing the risk of myocardial infarction, heart failure, and stroke.19-25
This association is stronger with COX-2 inhibitors and certain non-selective NSAIDs like diclofenac.
General CV risks of NSAIDs in SpA patients:
Increased CV events: NSAIDs have been linked to a heightened risk of CV events in the general population. In SpA patients, the relationship is less clear. Some studies suggest a possible beneficial effect of NSAIDs concerning CV events in axial SpA patients, while others indicate potential risks. A systematic review did not find an increased CV risk for NSAIDs, including COX-2 inhibitors, in AS patients. Notably, COX-2 inhibitor use was associated with a reduced risk of all CV events (RR 0.48 [95% CI: 0.33–0.70]).
26
Dose-dependent risks: Higher doses of NSAIDs may correlate with an increased risk of CV disease in AS patients.
27
Diclofenac: This NSAID has been associated with a significant increase in vascular and coronary risks. Studies indicate that diclofenac may elevate the risk of major adverse CV events, including heart attacks and strokes.
28
Etoricoxib: Research from the MEDAL program, which compared etoricoxib to diclofenac, found similar rates of thrombotic CV events between the two drugs. However, the choice of diclofenac as a comparator has been criticised due to its own associated CV risks.
29
Rofecoxib (withdrawn): This COX-2 inhibitor was withdrawn from the market after studies revealed a significant increase in the risk of myocardial infarction compared to naproxen. The VIGOR study highlighted a fourfold increase in heart attack risk among rofecoxib users.
30
Comparative CV risks among specific NSAIDs:
Literature review informs us about the comparative CV risk associated with different NSAIDs. The traditional NSAIDs, like diclofenac and some COX-2 inhibitors, have been associated with increased CV risks, including heart attacks and strokes.
Hierarchical List of NSAIDs Ranging from the Most Cardio-neutral to the Most Cardiotoxic, Based on Available Evidence.
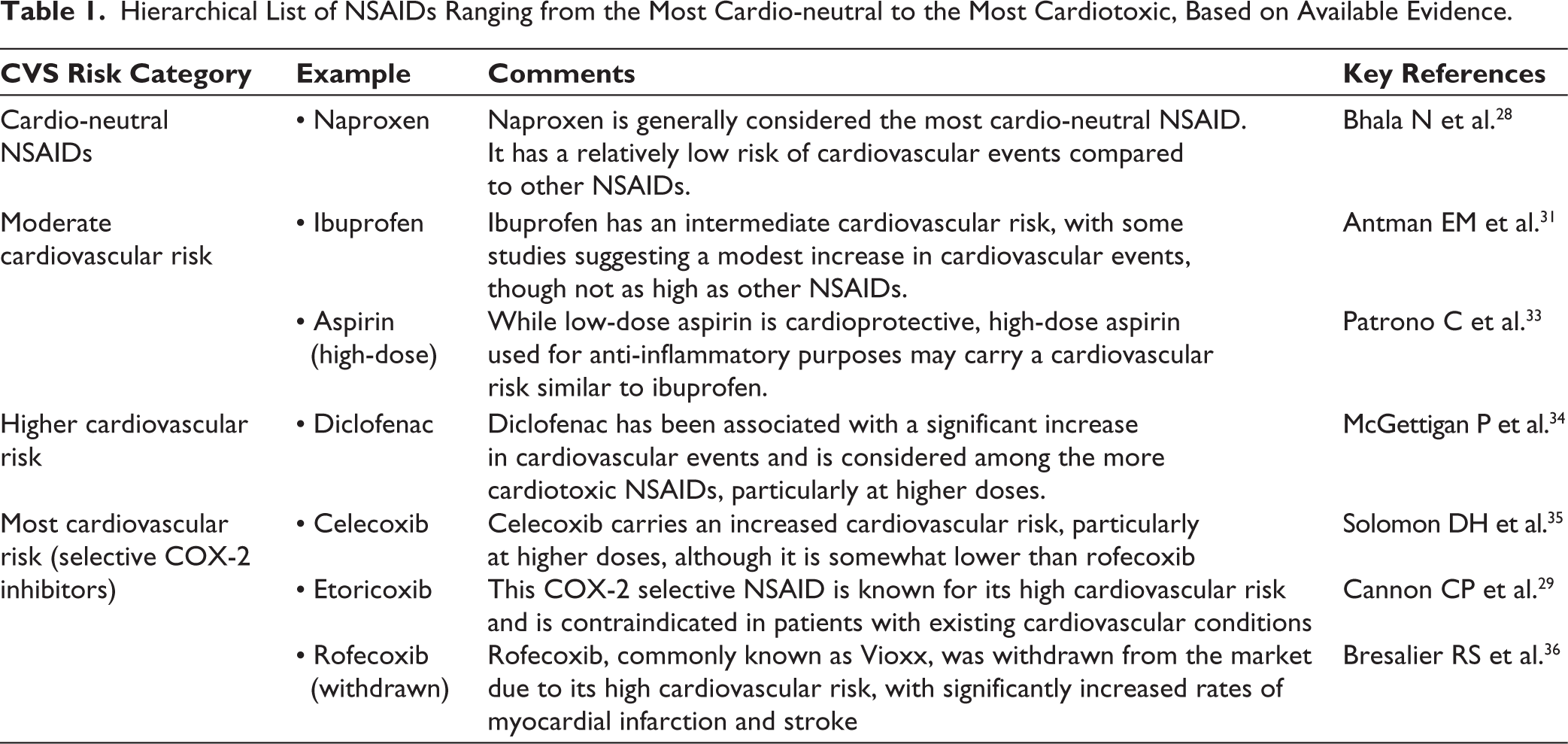
In contrast, cardioneutral NSAIDs like naproxen, ibuprofen and, to some extent celecoxib, are thought to avoid these risks and can be safer options for patients with a history of or risk factors for CV disease.
Bhala N. et al., in their meta-analysis highlights the varying CV risks of NSAIDs and identifies naproxen as having a more favourable CV profile. 28
Antman EM et al., gave an update for clinicians: a scientific statement from the American Heart Association, published in Circulation, which emphasised naproxen and ibuprofen as the safer choices among NSAIDs regarding CV risk. 31
FitzGerald GA in their review published in Nature discussed the mechanisms by which COX-2 inhibitors and other NSAIDs can affect CV risk, providing insights into why certain NSAIDs, like naproxen, may be cardioneutral. 32
Summary of CV risk hierarchy (discussed in Table 1)27–36
Naproxen (cardio-neutral) Ibuprofen, Aspirin (high-dose) (moderate risk) Diclofenac (higher risk) Etoricoxib, Rofecoxib (highest risk)
Interestingly, the Federal Drug Administration (FDA) of the United States has categorised celecoxib as comparatively safer NSAID (FDA)
In the year 2023, two papers appeared at an interval of only a few months in two leading journals in the field of rheumatology that reported the effect of continuous use of NSAIDs in patients with AS/SpA on the CV system. One was by French workers 37 and the other from the Korean workers. 27 Both studies examined the long-term effects of continuous use of NSAIDs in AS/SpA and its effect on the CV system. These studies were very similar in design and studied insurance claims data. Yet, the conclusion reached by them was exactly the opposite. While the French study found a protective role of NSAIDs in CV risk in these patients, significant reduction in ASCVD risk in patients on prolonged use of NSAIDs, the Korean study reported increased risk of ASCVD on prolonged use of NSAIDs in AS.
Obviously, these contradictory reports have caused confusion among rheumatologists, including the author of this article. In this context, the analysis of Kim et al.’s Korean paper 27 by two leading rheumatologists from the EULAR region, Robert B.M. Landewé and Maarten Boers, is of great interest. 38 They have raised several relevant questions about Kim et al.’s data derived from the insurance claims database. Firstly, such data is closely tied to financial incentives (reimbursement of medical care). Therefore, ‘exposure’ and ‘outcome’ will be picked only if it has resulted in an insurance claim. Such data also has an inbuilt issue of doubt about whether the prescribed drugs were actually taken. Also, in Kim et al.’s paper, there was the lack of direct information regarding the drugs being taken, neither by their physicians nor by the patients themselves. Therefore, Landewé and Boers opine that the calculations about the exposure to ‘high dose’ versus ‘low dose’ are inherently imprecise. Their major criticism, however, is related to confounding by indication (CBI). In Kim et al.’s study population, the choice between low-dose or high-dose NSAIDs was intentional, and not determined by randomisation or a chance occurrence. Based upon these, and several additional statistical criticisms of Kim et al.’s paper, Landewé and Boers reassure readers that in the context of axial spondylitis that is usually seen in relatively young patients who may experience large benefits from an optimal NSAID dose when they have active AS, contrary to the conclusion drawn by the authors, these data on continuous use of NSAIDs, are rather reassuring.
One of the authors of this letter brought to the notice of Landewé (the first author of the above-mentioned paper) a similar paper by French workers that had appeared a few months earlier but in another rheumatology journal. This paper also reports on the use of NSAIDs in AS/SpA and its effect on the occurrence of CV disease with a similar study design using insurance claims data. Landewé’s comments were:
This French study … Potentially suffers from the same shortcomings. It perfectly illustrates how careful one should be with interpreting big-data-analyses stemming from (claims) databases with different purposes than the research question under study. In the end, and after two publications, we still are similarly uncertain about whether NSAIDS in AS cause CV harm or protect against it. My opinion: the real effects, if any, are very modest and clinically irrelevant. (Personal communication [email message], with one of the authors, 4 September 2024).
In summary, AS/axSpA patients must continue to be treated as per the ACR/EULAR guidelines that recommend NSAIDs in patients with active disease who respond well to these drugs, preferably with ‘continuous’ as against ‘on demand’ use. 39 Regarding the choice of which NSAID, as discussed above, it hardly matters as their adverse effect on CV disease seem to balance out; anti-inflammatory effects would protect against CV disease while their inherent cardiotoxic effect would enhance the risk. In those with a strong family history of CV disease, it would be prudent to use safer NSAIDs, for example, naproxen, ibuprofen, rather than indomethacin or etoricoxib. As mentioned earlier, the FDA of the United States has categorised celecoxib as comparatively safer NSAID. Based on the evidence discussed, the author prefers to use either naproxen or celecoxib for patients with AS/axSpA with active disease and show good response to these drugs.
Clinical Implications
When prescribing NSAIDs for SpA patients, clinicians should carefully consider the individual patient’s CV risk profile. While NSAIDs are effective for symptom management, their potential CV risks necessitate a personalised approach, balancing therapeutic benefits against possible adverse effects. It is essential to note that while some studies provide insights into the comparative CV risks of various NSAIDs, more research is needed to draw definitive conclusions, especially concerning their use in SpA patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.