
Abstract
Inflammatory joint diseases, such as rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA), and osteoarthritis (OA), are leading causes of chronic pain and disability. Effective management is essential to prevent long-term joint damage and improve quality of life. This narrative review examines the role of intra-articular corticosteroid (IACS) injections, with a focus on triamcinolone hexacetonide (THA), in managing these conditions. THA has demonstrated superior efficacy in prolonging remission in RA and JIA in the injected joints, providing sustained relief from pain associated with OA, and offering a better safety profile compared to other corticosteroids, such as triamcinolone acetonide (TA) and methylprednisolone acetate (MPA). In RA, IACS such as THA, when combined with disease-modifying antirheumatic drugs (DMARDs), play a vital role in controlling disease activity and minimising comorbid risks. THA is preferred over TA in non-systemic JIA due to its longer duration of action and lower relapse rates. Similarly, in OA, THA provides sustained pain relief and functional improvement, offering advantages over other corticosteroids due to its slower systemic release and prolonged joint retention. By enhancing symptom control and reducing inflammation, IACS, especially THA, offer an important therapeutic strategy for patients with RA, JIA, and OA, helping to improve patient outcomes and quality of life.
Keywords
Introduction
Inflammatory joint diseases such as rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA) and osteoarthritis (OA) are leading contributors to severe, chronic pain and long-term disability globally. 1 RA is a formidable autoimmune condition impacting approximately 0.5%-1% of the population. Its far-reaching effects extend beyond joint inflammation, posing significant challenges due to extra-articular manifestations and associated comorbidities. 2 In India, the estimated prevalence of RA is 0.7%, surpassing the global prevalence of 0.46%. 3 RA is more prevalent in females than males, with the highest incidence occurring in the third and fourth decades of life. 4 In developing countries like India, patients with RA often delay seeking medical advice, adversely affecting their prognosis and increasing the disease burden. 5 JIA is a diverse group of inflammatory arthritis conditions that affect children under 16 years of age and persist for at least six weeks. It is the most common chronic rheumatic disease in children, leading to both short-term and long-term disability. 6 The inflammatory process in OA has been extensively studied, revealing that OA may behave like an autoinflammatory disease, driven by chondrocyte and synoviocyte responses. 7 Recent studies have shown elevated levels of inflammatory cytokines in the serum and synovial fluid of OA patients, underscoring the significant role of inflammation in the disease’s pathogenesis. 7
Effective RA management aims to minimise disease activity and achieve clinical remission in the short term, while long-term goals focus on slowing structural damage, preventing impairment, and controlling systemic symptoms. 8 Treatment options include conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) which act slowly, and faster-acting biological (bDMARDs) and targeted synthetic (tsDMARDs) medications. Glucocorticoids (GCs) may have disease-modifying effects in addition to rapid symptom-relieving effects.9,10 In India, 74% of physicians use GCs in initial RA treatment, and 95.4% use them during acute exacerbations. 4 Intra-articular corticosteroid (IACS) injections play a pivotal role in providing immediate relief from pain, and managing inflammatory arthritis, oligoarthritis and joints that are refractory and at risk of developing limb length or flexion deformities.11-12 Studies have shown that early and continued use of IACS is associated with less leg length discrepancy in young children with JIA. 13
This review compiles and synthesises current literature on the optimisation of IACS use in RA, JIA and OA focusing on key aspects such as efficacy, safety, and routes of administration. Drawing on clinical guidelines, expert consensus, and peer-reviewed articles, it provides a comprehensive overview aimed at enhancing clinical practice.
Additionally, the review traces the historical evolution of corticosteroid use, explaining its integration with DMARDs and detailing injection protocols. Clinical outcomes, patient demographics, and treatment protocols are examined through thematic analysis of data from various medical databases, offering valuable insights to inform clinical decision-making. While studies describe the efficacy of IACS in conditions such as psoriatic arthritis, spondylarthritis, and gout, these indications are not included here as they are beyond the scope of this review.
Intra-Articular Corticosteroids
IACS injections are a key therapeutic modality, furnishing rapid-onset anti-inflammatory effects and engendering remission in a noteworthy subset of early RA patients. 2 Notably, analyses from landmark trials such as the BeSt study (Dutch acronym for Behandel-Strategieen’s treatment strategies’) illuminate the transient yet impactful nature of these interventions, with a significant reduction in joint swelling observed in the short term. 14 Meanwhile, the Cyclosporine, Methotrexate, Steroid in RA (CIMESTRA) study underscores the synergy between IACS injections and step-up conventional synthetic DMARDs, underscoring their pivotal role in bolstering disease control and patient well-being. 15
Indications for IACS injection are as follows:
Mono-or oligoarthritis in RA.
16
When recently initiated systemic treatment has not yet taken effect or when systemic treatment proves to be ineffective, contraindicated, or can be reduced or avoided.
16
When other joints are under check effectively with systemic treatment.
16
To offer rapid relief from severe inflammatory pain.
16
To facilitate adequate physical therapy.
16
To prevent flexion deformities and damage secondary to persistent inflammation.
11
For pregnant women encountering a flare-up of RA, intra-articular administration is advised for corticosteroids to minimise systemic side effects. Nonsteroidal anti-inflammatory drugs (NSAIDs) offer an alternative option; however, their use demands caution, particularly during the third trimester of pregnancy.
17
Various corticosteroid preparations, including methylprednisolone acetate (MPA), triamcinolone acetonide (TA), and triamcinolone hexacetonide (THA), are commonly used in clinical practice for intra- or periarticular injections, each with differing concentrations, anti-inflammatory potency and duration of action.13,16
Hollander et al. observed that branched esters of hydrocortisone exhibited superior efficacy compared to hydrocortisone alone, leading to the development of esters of prednisolone, triamcinolone, and dexamethasone. 18 These esterified analogues, characterised by increased insolubility, exhibit prolonged retention at the injection site or within joints, offering potential advantages over their more soluble parent compounds. 19
Triamcinolone Hexacetonide
Chemical Structure and Properties
THA is a long-acting IACS having the least solubility of all the corticosteroid esters. Lower solubility agents exhibit slower systemic absorption and longer duration of action, leading to higher efficacy. THA, being 2.5 times less soluble in water than others, provides the longest duration of effect. Moreover, THA results in minimal systemic spillover, enhancing its safety profile. 16 Although TA and THA differ only by one side chain, their efficacies vary considerably. Multiple studies have demonstrated that THA provides a longer duration of clinical remission in patients with JIA compared to TA. This may be attributed to its slower absorption and release. Additionally, THA has been shown to specifically reduce synovial T cell lymphocytes and associated inflammatory cytokines. 20 The difference between THA and TA is given in Table 1.
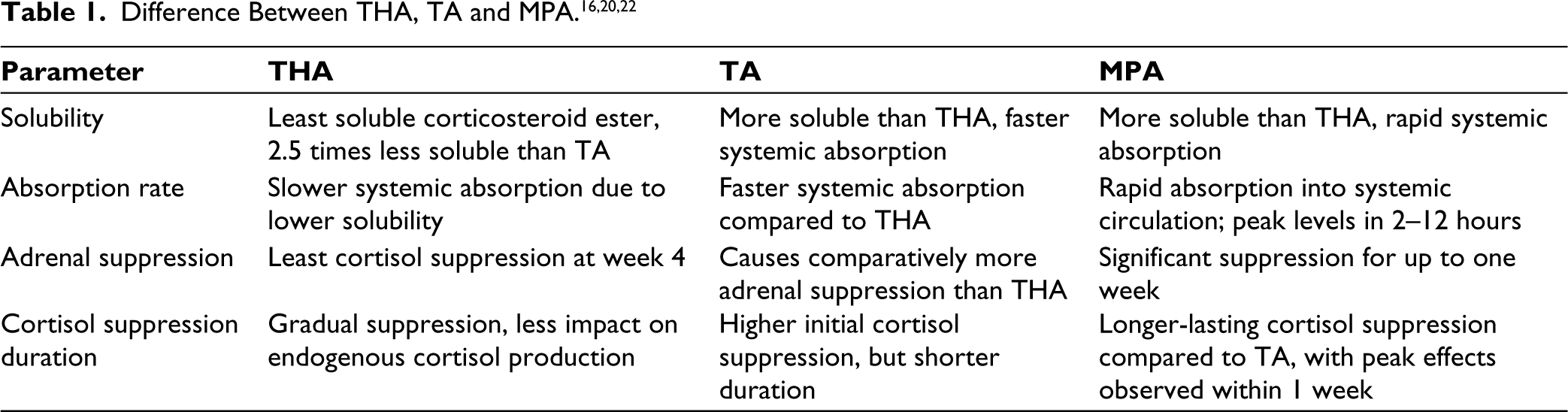
Blyth et al. found that THA provided extended pain relief in knee RA compared to hydrocortisone succinate or TA, 21 while Bird et al. reported thermographic improvement with prednisolone t-butylacetate, MPA, and THA in knee RA, with the longest-lasting effects observed with THA. The study also demonstrates the effect of these three drugs on adrenal suppression. Prednisolone t-butyl acetate showed the most significant initial suppression, while methylprednisolone had the longest-lasting effect. THA showed the least cortisol suppression at week 4 thereby offering advantage over the other two drugs. 22 Centeno and Moore surveyed members of the American College of Rheumatology, revealing varying preferences for IACS, with MPA, THA, and TA being the most favoured options. 23 Compared to MPA and TA, THA causes slower systemic absorption owing to its lower solubility. This slower absorption prolongs its presence in synovial fluid and results in lower systemic corticosteroid levels. In contrast, MPA is absorbed more rapidly into the systemic circulation. A study by Armstrong RD et al. demonstrated that in 21 patients with RA who received intra-articular MPA injections, peak serum levels of MPA were reached within 2–12 hours post-injection. Additionally, when 80 mg of MPA was administered as 40 mg into each knee, it produced consistently higher peak serum levels compared to a single intra-articular injection. Serum cortisol levels were significantly suppressed for up to one week, and this suppression was observed across all dose levels. The absorption of THA into the systemic circulation follows a first-order process, leading to a more gradual release of the steroid compared to MPA and TA. Consequently, THA’s slower absorption rate reduces its impact on the hypothalamic-pituitary-adrenal axis, resulting in less suppression of endogenous cortisol production. 24
Effect on Articular Cartilage
While corticosteroid therapy effectively alleviates joint symptoms associated with OA and other inflammatory disorders, there is a concern about its long-term negative effects on articular cartilage. In their review article, Wernecke C et al. summarised conflicting findings from basic science studies on triamcinolone. 28 While two in vitro investigations on chondrocytes suggest that triamcinolone exhibits chondrotoxic effects across all tested doses, in vivo animal and human clinical studies suggest a potential protective effect of triamcinolone on chondral tissues, particularly in the context of injury or OA. 28 The variability in findings may stem from diverse factors such as animal model variations, dosage differences, or treatment durations. 25 In a study by Weitoft T et al. 20 patients underwent intra-articular glucocorticoid treatment for knee synovitis, with half receiving post-injection rest. Each received a 20 mg injection of THA. Changes in cartilage and bone turnover were assessed using serum and urine markers over two weeks. Cartilage oligomeric matrix protein (COMP) measured cartilage turnover, osteocalcin assessed bone formation, and deoxypyridinoline (DPD) evaluated bone resorption. COMP levels decreased significantly in both groups (P < .001), with a more pronounced reduction in patients who rested post-injection. Serum osteocalcin levels decreased significantly (P < .001) with no difference between groups, while DPD levels remained unchanged. This suggests that intra-articular glucocorticoid treatment for knee synovitis may offer a protective effect on cartilage by reducing COMP levels. 26
Effect on Blood Sugar
Habib GS et al. investigated how different intra-articular triamcinolone preparations like THA and TA affect blood glucose levels in diabetic patients receiving knee injection. The study included diabetic patients who received knee injections with different triamcinolone preparations to assess blood glucose levels. Blood glucose measurements were taken before and after the injections to analyse any changes. With median peak blood glucose levels less than 300 mg%, IACI of depot preparation of either TAH or TA is not contraindicated in a patient with controlled diabetes with symptomatic OA knee. The median initial and peak blood glucose level observed with TA and THA are mentioned in Table 2.
Median Initial and Peak Blood Glucose Levels with TA and THA. 27
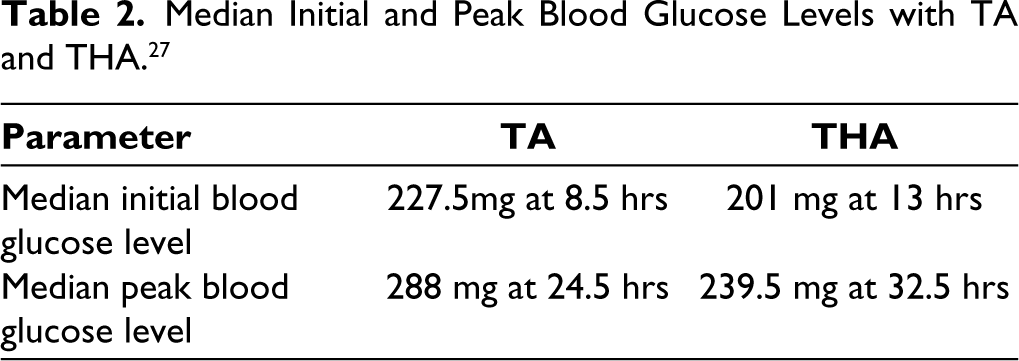
The study indicated that THA is associated with a more gradual rise in blood glucose levels compared to other triamcinolone preparations, resulting in significantly lower increases in blood glucose levels post-injection. Although there was no significant difference between the two triamcinolone groups, THA might be the preferred option for IACI in diabetic patients with symptomatic OA of the knee. 27
Habib GS et al. studied the impact of IACS MPA on glucose metabolism in patients with controlled type 2 diabetes and OA of the knee, as prior studies had not explored this relationship. Nine patients received 50 mg of MPA via knee injection and monitored their blood glucose levels before and after meals. All patients experienced a significant rise in blood glucose levels, with peak levels ranging from 300 mg/dL to 500 mg/dL, occurring as early as two to four hours in some and 12–26 hours in others. The elevated glucose levels persisted for two to three days in most patients and up to five days in a few. This suggests that IACS of MPA in diabetic patients can lead to a transient but significant increase in blood glucose, likely due to rapid absorption of the steroid into the bloodstream. 28
Evidence in RA Management
In 1961, Hollander et al. reported that THA exhibited significantly longer local remission of inflammation compared to other adrenocorticosteroids. 29 In 1971, McCarty DJ et al. conducted a study with 12 patients followed for 14–27 months, revealing prolonged (>1 year) reversal of inflammation in joints treated locally with THA resulting in improved grip strength and functional outcomes. Radiographic observations over a mean follow-up of 21 months showed fewer new lesions on the treated side, but some injected joints experienced arthritis recurrence and progression, both clinically and radiologically. Common adverse effects included soft tissue atrophy and periarticular calcification, although their true incidence and significance require further investigation. 30
Pereira DF, et al. conducted the study to compare the medium-term effectiveness of low and high doses of THA in intra-articular injections for medium-sized joints of RA patients. Conducted as a randomised double-blind trial, 60 wrists with painful refractory synovitis were randomised to receive either a low dose (20 mg) or high dose (40 mg). Assessments were performed at weeks 0, 1, 4, 8, and 12, evaluating pain and swelling via visual analogue scales, chronic disease activity index, goniometry, simplified Stanford Health Assessment Questionnaire, and side effects. Results showed no significant differences between groups in baseline values or outcomes, with both groups experiencing improvements in pain, swelling, disease activity, and function over time (P < .001). No serious side effects were reported. In conclusion, both low and high doses of THA demonstrated comparable effectiveness in intra-articular injections for RA patients’ wrists. 31
In this prospective case-control study conducted by Rocha RH et al. 262 joints in 158 rheumatic patients (mean age 60 ± 13.7 years) were evaluated following a single intra-articular injection of THA over 12 months. Remission rates were observed at 3, 6, and 12 months, with a mean duration of effect of 8 ± 4.0 months. RA patients exhibited longer remission (8.4 ± 3.9 months) compared to OA (6.9 ± 4.0 months), and smaller joints had a longer duration (10.4 ± 2.7 months) than medium and large joints. Predictors of longer duration included RA, smaller joints, female sex, lower pain/swelling scores, and leflunomide use, while receiving only one injection, hypertension, diabetes mellitus, and biological therapy were associated with shorter duration. 32
Furtado RNV et al. conducted a study evaluating joint function in RA patients after intra-articular injections with THA. They assessed metacarpophalangeal, wrist, elbow, shoulder, knee, and ankle joints at baseline and at 1, 4, 12, and 24 weeks post-injection. Outcome measures included pain at rest (VASR), pain during movement (VASM), joint swelling (VASSw), and joint flexibility (flexion and extension). Among 289 patients (635 joints), significant improvements were observed in swelling and rest pain at 4, 12, and 24 weeks across all joints. Movement pain improved at 4 weeks for all joints, and at 12 and 24 weeks for the metacarpophalangeal and knee joints. Flexion and extension also showed marked improvements, particularly in the metacarpophalangeal and knee joints, with significant gains lasting up to 24 weeks. 33
Evidence in JIA Management
In the management of non-systemic JIA, initial treatment is determined in part by the number of active arthritis joints. Polyarticular JIA, involving more than 4 joints, typically necessitates systemic therapy with methotrexate or a biologic DMARD, while oligoarticular JIA, involving 4 or fewer joints, is often treated with IACS injections. Refractory oligoarticular arthritis may require systemic treatment. The preference for IAS in children with fewer affected joints aims to minimise toxicity and cost associated with systemic therapy while reducing joint damage and long-term morbidity. 34
To date, most studies investigating IACSs in JIA have focused on THA, with documented evidence of its effectiveness and safety. 35
Allen RC et al. prospectively assessed the efficacy of intra-articular THA in 40 children with persistent knee arthritis unresponsive to nonsteroidal anti-inflammatory drugs. Among 49 injected knees, 63.3% maintained complete resolution of inflammation at 6 months, correlating with younger age, shorter disease duration, and higher triamcinolone dose. At 12 months, 45% of injected knees remained in remission. 36
In a retrospective review of 194 children with JIA treated with intra-articular THA subgroup-specific differences in efficacy and duration of benefit were assessed. A total of 1439 THA injections were administered, with a median duration of improvement of 74 weeks across all injections. Responses varied significantly among JIA subgroups (P = .0001), with varying durations of efficacy: 121 weeks for early-onset pauciarticular JIA type I, 47 weeks for late-onset pauciarticular JCA type II, 105 weeks for rheumatoid factor-negative polyarticular JIA, 63 weeks for rheumatoid factor-positive polyarticular JCA, and 36 weeks for systemic JIA. Side effects were rare, including skin and lipoatrophy, necrosis of the hip, luxation of shoulders, and periarticular calcification. Intra-articular THA proved effective across all JIA subgroups with low risk of major complications, with duration of improvement influenced by disease subgroup. 37
Prior research has extensively compared the long-term efficacy of THA versus TA in JIA patients receiving intra-articular joint injections (IAJI). Zulian et al. reported significantly higher response rates with THA compared to TA at 6 months, 12 months, and 24 months (60% vs. 33.3%, respectively). 38 Follow-up studies conducted by the same group showed consistent long-term outcomes, even in cases of symmetrical joint involvement, with THA outperforming TA despite TA being administered at double the dose (2 mg/kg vs. 1 mg/kg). 39 Another study by Eberhard et al. compared time to relapse over a 15-month follow-up period after THA or TA injection of 227 joints, showing a response rate of 76% versus 56% at 6 months, respectively. However, TA’s efficacy declined over time, with a response rate dropping to approximately 50% in the THA group versus 21% in the TA group after 12 months. Moreover, the hazard ratio associated with injection type was 1.8 (95% CI 1.05, 3.08), indicating a higher relapse risk with TA from the first month post-injection. 35
In the recent analysis by Chun A et al. retrospective chart review of 39 JIA patients who received IACS from September 2018 to September 2019 was conducted. Lifetime injections with either THA or TA up to 30 May 2021, were analysed, excluding patients initiating systemic therapy concurrently. The primary outcome, time to relapse, was defined by arthritis presence on physical examination by a rheumatologist. Kaplan–Meier curves and log-rank tests compared relapse probability between IACS injections, with mixed-effects Cox regression models adjusting for multiple injections per participant. Results indicated a longer median relapse time for THA compared to TA. TA joints had a higher relapse probability (P < .001), with THA showing reduced hazard of relapse in both unadjusted and adjusted models (unadjusted hazard ratio: 0.184; adjusted hazard ratio: 0.189). In conclusion, THA offers longer duration of action and fewer systemic side effects, making it the preferred choice for IACS injections in children with JIA. 22 In a study by Rubin et al. comparing the efficacy and safety of TA versus THA for JIA patients, similar recovery rates (~70%) were observed with both treatments. However, TA-injected joints had more than double the relapse rate compared to THA-injected joints. 40 THA is recommended by ACR guidelines 2019 for the treatment of JIA recommends over TA. 41
Evidence in OA Management
OA is one of the most common rheumatologic disorders in India with a prevalence ranging from 22% to 39%. 42 Knee OA is the predominant type. Disability-adjusted life years attributed to OA have increased substantially. It affects women more than men, with symptoms becoming more prevalent with age. Pain, exacerbated by weight bearing and exertion, is a key symptom leading to total knee arthroplasty. IACS, often prescribed for pain relief, have variable effectiveness depending on drug solubility. THA, globally approved for inflammatory joint diseases, provides prolonged pain relief due to its slower release of the active metabolite compared to TA. 43 In the United States, a comprehensive survey found that over 95% of rheumatologists utilise IACS injections for knee OA treatment. However, there is ongoing debate regarding the most effective steroid formulation. THA and MPA are the most used and researched preparations. However, only one trial has directly compared both agents, revealing that THA demonstrated greater efficacy at week 3, whereas MPA showed superiority at week 8. These findings prevent a definitive conclusion regarding the preferred choice between the two. Considering this Lomonte ABV, conducted the study aimed to compare the efficacy of intra-articular THA and MPA in patients with defined knee OA. 44 Patients with knee OA (Kellgren-Lawrence grade II or III) received either intra-articular THA or MPA. Assessment at 4, 12, and 24 weeks demonstrated significant pain improvement with both treatments, sustained up to 24 weeks, with no difference observed between groups in pain relief, patient, and physician global assessments, WOMAC score, or Lequesne index. Secondary outcomes remained improved throughout the study. Both intra-articular therapies are equally effective, maintaining pain relief and function for 24 weeks. 29 A prospective study conducted by Buyuk AF et al. evaluated the efficacy of THA and MPA in 126 patients, demonstrating that both MPA and THA provide similar effectiveness in pain relief and functional improvement. 45
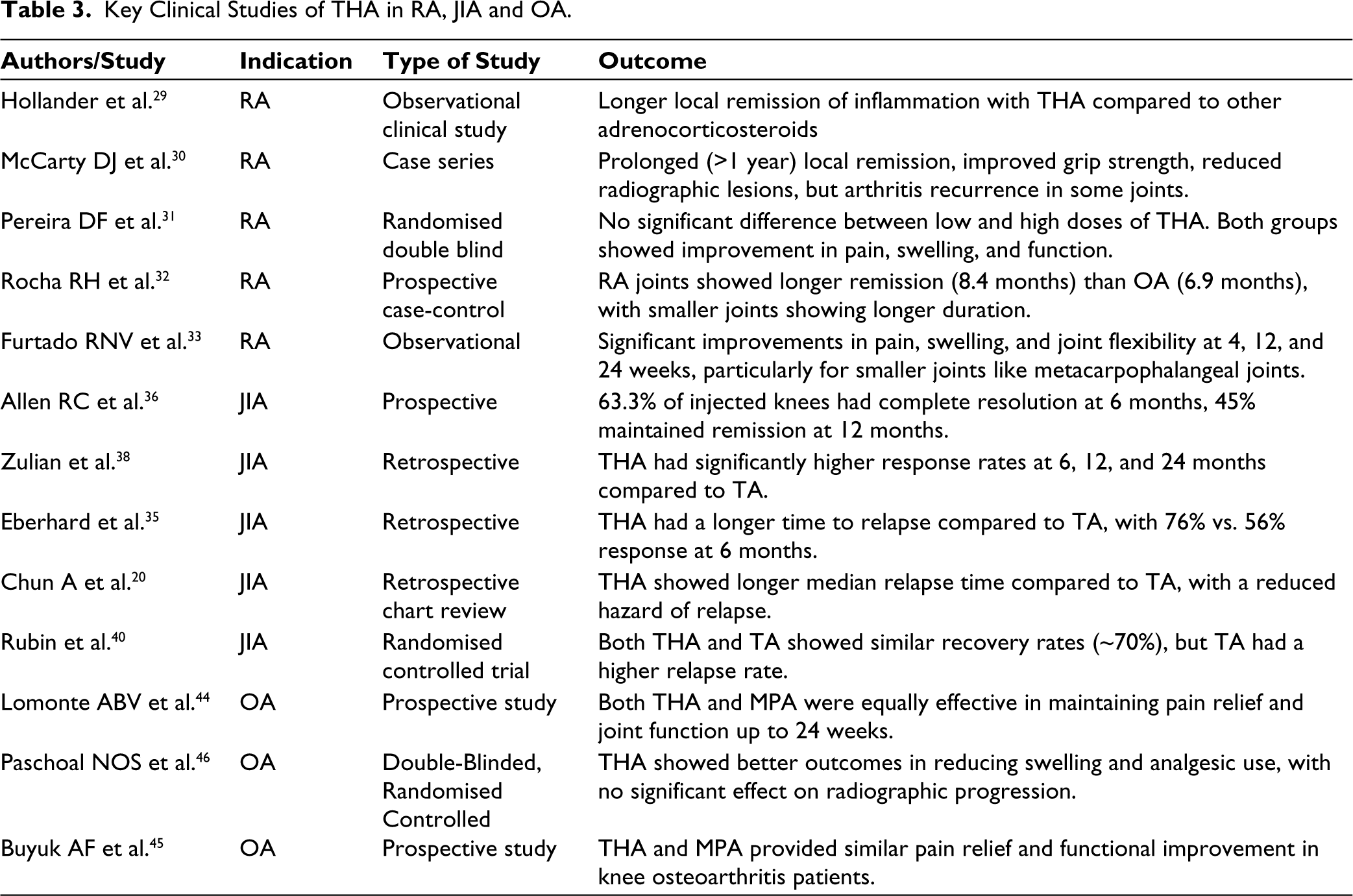
Paschoal NOS conducted a double-blinded randomised controlled trial with a one-year follow-up to evaluate the effectiveness of THA intra-articular injection in hand Interphalangeal Joints (IP) of OA patients to improve pain and joint swelling; improve function, goniometry, and grasping force, and assess intra-articular injection influence on radiographic evolution over 1-year. In this randomised, double-blind study, 60 patients with symptomatic OA of the IP joints were randomly assigned to receive either intra-articular THA plus lidocaine (LD) or LD alone. Over a 1-year period, patients were assessed for variables including pain, swelling, functional status, grip strength, joint mobility, and radiographic changes. While both groups exhibited similar outcomes at 48 weeks, the TH/LD group demonstrated superior improvements in joint swelling and reduced acetaminophen usage (P = .04 and P < .001, respectively). Importantly, the radiographic assessment showed no significant differences between the groups, indicating that IAI treatment did not influence OA progression in the injected joints. These findings highlight the efficacy of intra-articular injection therapy of THA in managing IP joint OA, particularly in reducing swelling and analgesic consumption, while ensuring its neutral impact on radiographic evolution. 46 Table 3 describes the clinical studies of THA in RA, JIA and OA.
Key Clinical Studies of THA in RA, JIA and OA.
Thus, THA exhibits distinct advantages in managing RA, JIA, and OA due to its prolonged duration of action and reduced systemic absorption. THA’s efficacy, particularly in RA and JIA, is well-documented, with studies highlighting significant improvements in disease activity, symptom relief, and joint function. In RA, THA is effective as IACS for significant and prolonged symptom relief, especially beneficial in early RA and flares. Similarly, in JIA, THA demonstrates better efficacy and longer remission durations compared to TA, making it the preferred choice for managing oligoarticular JIA. For OA, THA provides sustained pain relief and functional improvements, with evidence supporting its use over other corticosteroids due to its slower systemic release and prolonged joint retention. Despite concerns about potential cartilage damage with long-term corticosteroid use, THA’s favourable safety profile, particularly its minimal systemic spillover and reduced hypothalamic-pituitary-adrenal axis suppression, underlines its therapeutic value. Thus, THA represents a potent, well-tolerated option for managing various inflammatory joint conditions, balancing efficacy and safety effectively.
Summary and Conclusion
Inflammatory joint diseases, mainly RA, JIA, and OA, are significant contributors to chronic pain and long-term disability. While RA is a common autoimmune disorder and JIA primarily affects children, OA has emerged as a more complex disease with inflammatory features. RA patients face increased risks of comorbidities, highlighting the importance of effective disease management. The use of DMARDs and IACS injections, including THA, is central to reducing disease activity and preventing long-term damage. In JIA, IACS injections, particularly THA, are effective in managing oligoarticular cases, offering prolonged remission with minimal side effects. Similarly, in OA, THA provides prolonged pain relief due to its slower release profile, making it a valuable option. Insights from clinical guidelines, expert consensus, and peer-reviewed studies underscore the critical role of IACS, particularly THA, in managing these diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was not obtained from the local Ethics Committee or Institutional Review Board as it was a review article.
Funding
Editorial assitance for writing was provided by Parv enterprises through funding received from Abbott Healthcare Pvt. Ltd.
Patient Consent
Consent was not needed/not applicable as this did not include any patient-related data.