
Abstract

Introduction
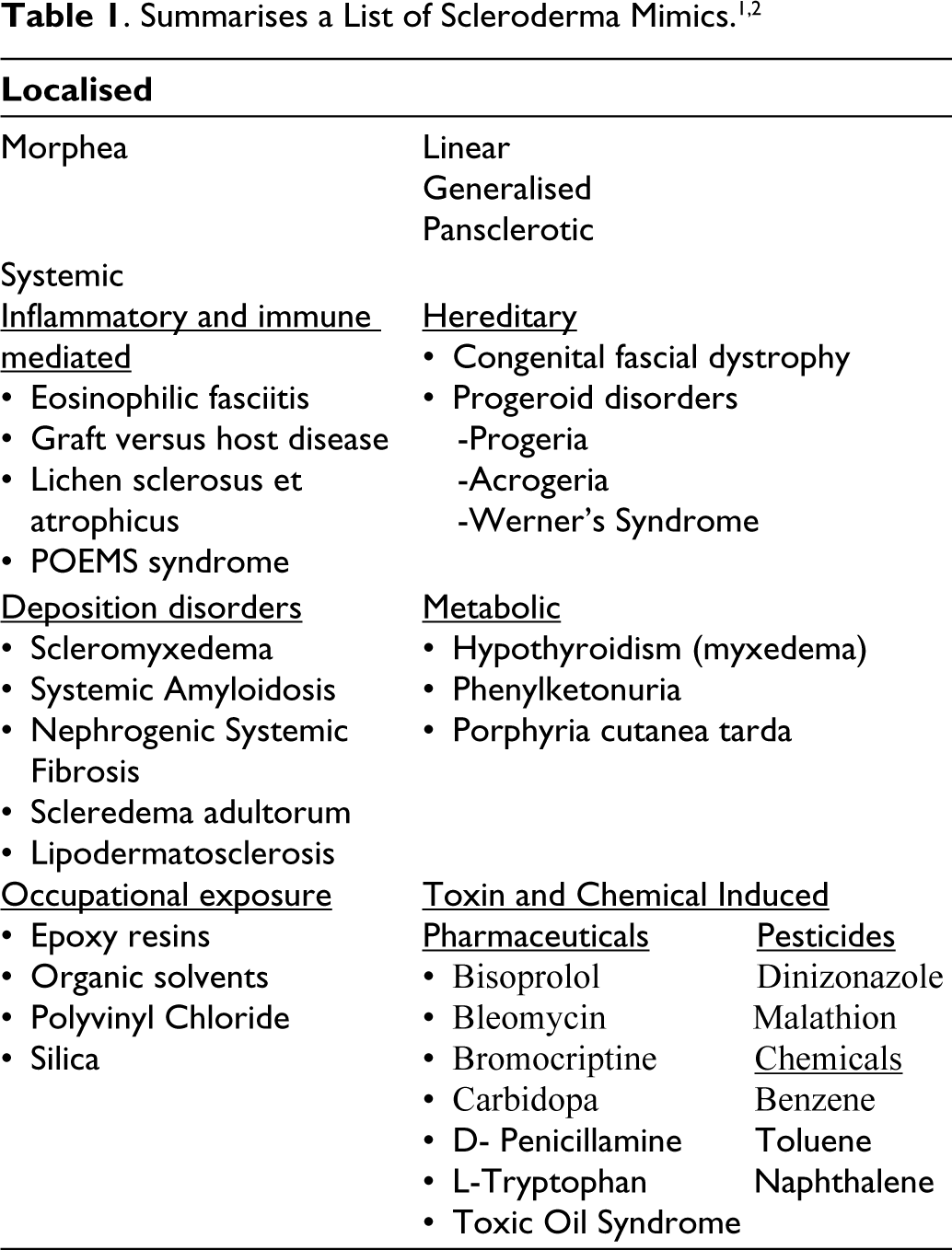
Systemic sclerosis (SSc) is a rare autoimmune disorder characterised by diverse clinical manifestations and multiorgan involvement due to fibrosis of the skin and internal organs. 1 However, there are other conditions which can cause hardening and thickening of skin (Table 1). These conditions can mimic SSc and can potentially lead to a misdiagnosis. 2 Scleredema Adultorum of Buschke is one such mimic and was first described by Curzio in 1752. It was well defined later by Abraham Buschke in 1902 who described skin tightening in a 46-year-old carriage varnisher following an episode of influenza which started in the neck and spread to involve all over the body sparing regions distal to the palms and thighs.3,4
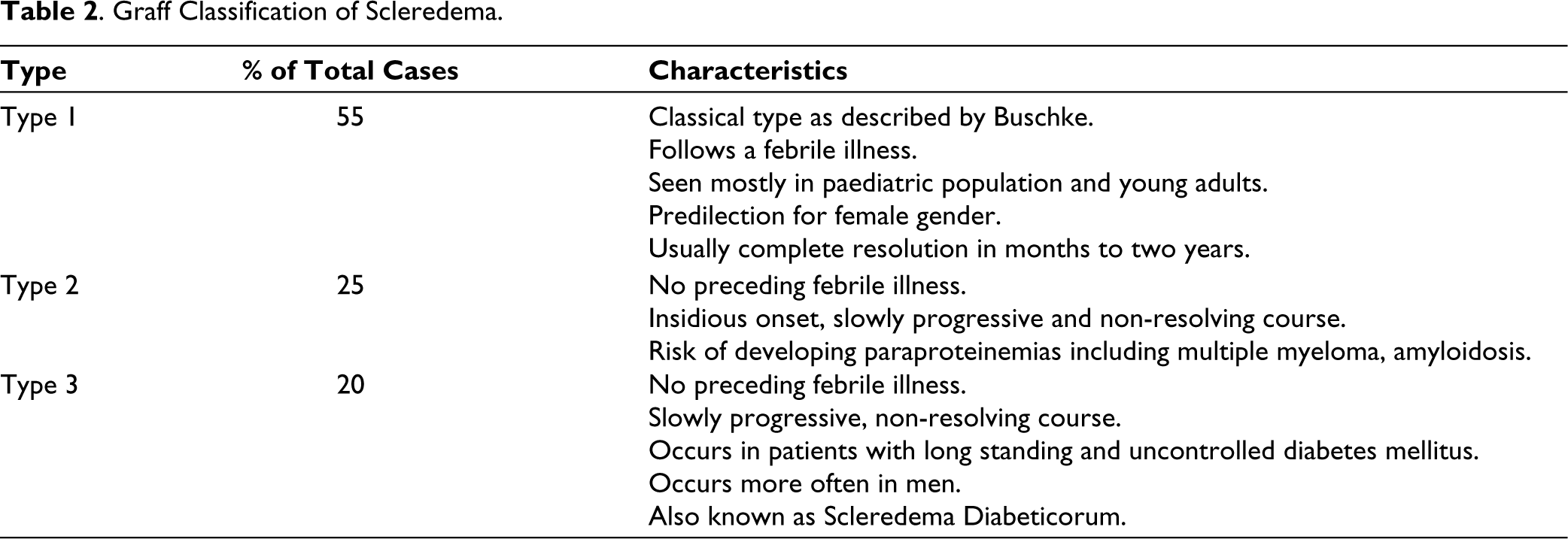
Scleredema is an uncommon fibro mucinous connective tissue disorder with unknown aetiology. It is characterised by increased production of Type 1 collagen and glycosaminoglycans by fibroblasts of the reticular dermis and it clinically presents with firm, non-pitting oedema that usually begins in the neck and extends to the face, scalp, shoulders, and trunk. The hands and feet are conspicuously spared.2,3 In addition, it is not associated with other features like Raynaud’s phenomenon, abnormal nail fold capillaries and is also devoid of autoantibodies. 1 In 1968, Graff described three types of scleredema adultorum, which are summarised in Table 2. 4 Scleredema, irrespective of the subtype, causes asymptomatic, woody, non-pitting induration of the skin on the neck, upper back, shoulders and arms. The indurated skin can have a peau d’ orange appearance. Extra cutaneous involvement is rare, especially seen in Type 2 and Type 3 Scleredema. It affects mostly the tongue, heart, lungs, skeletal muscles, oesophagus, parotid glands, liver, spleen, pleura and eyes. Complications include restricted motility, dysphagia, sicca syndrome, pleural or pericardial or peritoneal effusions. 3 The diagnosis of Scleredema is both clinical and histological characteristics. 2 The pathogenesis of Scleredema diabeticorum (Type 3) remains unclear. One hypothesis suggests that high glucose levels induce non-enzymatic glycosylation of dermal collagen. Another hypothesis proposes that glucose stimulates fibroblast proliferation and synthesis of extracellular matrix components. Immunological response has also been postulated since patients have ameliorated following treatment with cyclosporine. The lack of lymphocytic infiltrates in the dermis rules out a T-cell-mediated etiologic mechanism. 5
Graff Classification of Scleredema.
Distinguishing scleredema adultorum from scleroderma is very important due to significant differences in their clinical presentation, progression, treatment and prognosis. Scleredema affects the upper body with sparing of the hands and feet while scleroderma typically affects the hands, arms and face with indurated skin. Scleroderma can involve internal organs while Scleredema usually does not. In addition, scleroderma carries a higher mortality risk due to organ involvement while scleredema adultorum is generally benign. Misdiagnosing scleredema adultorum as scleroderma can lead to unnecessary aggressive treatment and patient anxiety. Accurate distinction between the two ensures appropriate management, treatment and patient counselling, ultimately improving outcomes.
Here, we present five cases of scleredema adultorum of Buschke, their presentation, evaluation and management.
Description of Cases
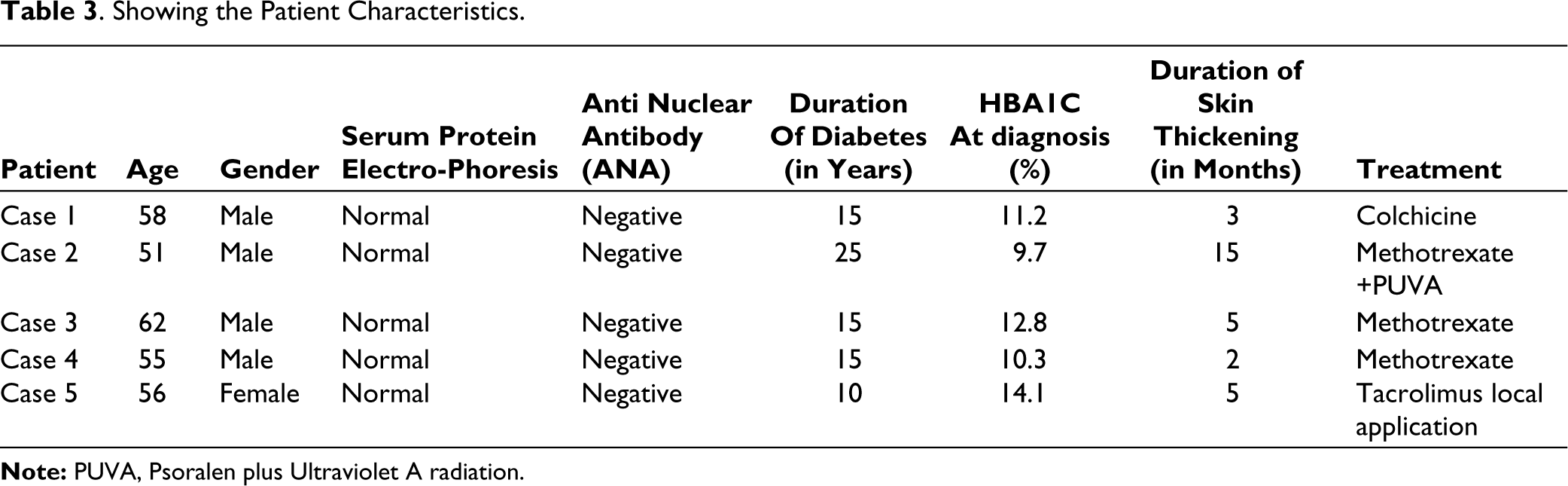
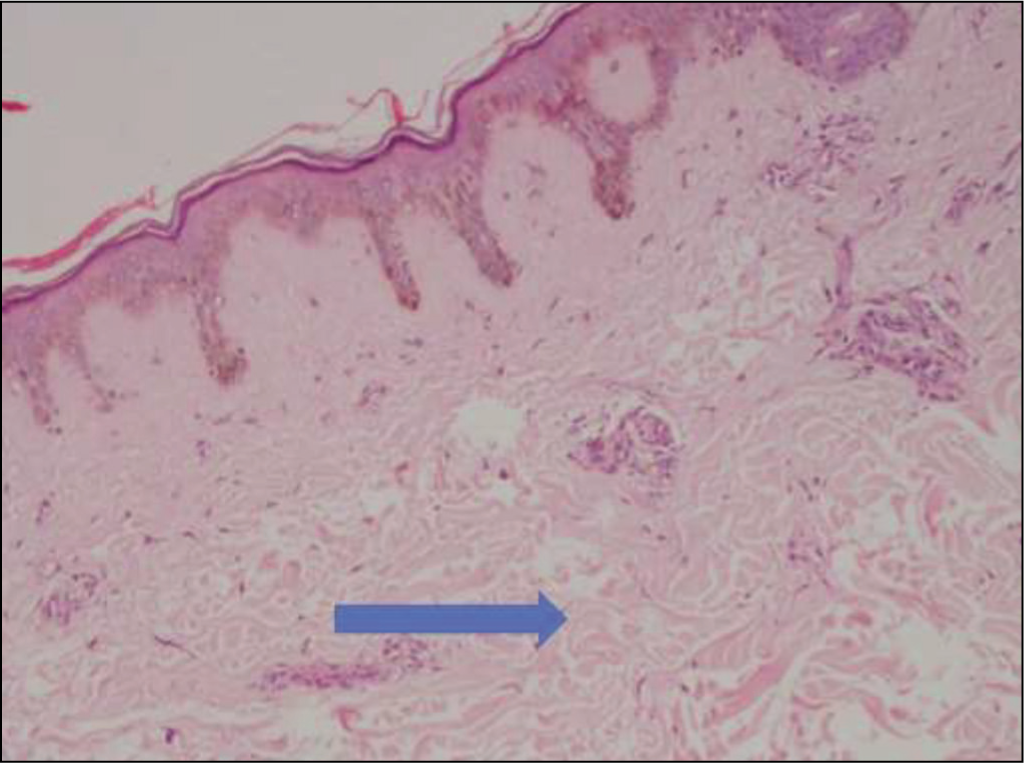
Details of the cases are given in Table 3. There were four male patients and one female patient with a median age of 56 (range 51-62) years. All of them presented with gradually progressive thickening of the skin over the back extending from neck to upper arm and up to lumbar region (Figure 1). None of the patients had a history of previous infections. All of them had diabetes mellitus, with a median duration of 15 (range 10-25) years before diagnosing Scleredema and had uncontrolled diabetes mellitus. Two patients also had features of end-organ damage in the form of Diabetic Retinopathy. There was no Raynaud’s phenomenon, digital tip ulcers, joint pain, salt and pepper pigmentation of the skin. They had no constitutional symptoms, loss of appetite or loss of weight. Complete Blood Count, liver function test, renal function test, chest X-ray and echocardiogram were normal. All patients were evaluated for Systemic diseases like autoimmune disease SSc. There were no clinical features and all were negative for ANA. They were also evaluated for myeloma and were negative for monoclonal gammopathy. Skin biopsy was performed on all these patients. Histopathology revealed epidermis unremarkable with dermis showing thick collagen bundles with increased spaces in between the bundles. There was minimal inflammatory reaction and sweat glands appeared to be pulled up due to increased collagenisation of the deeper dermis (Figure 2). Alcian blue staining revealed increased mucin and collagen. These features are consistent with Scleredema.
Showing the Patient Characteristics.
Clinical Picture of Scleredema Patient Revealing Thickening of the Skin on the Back and Sparing the Fingers with Biopsy Site.

Skin Biopsy 10X Magnification H&E Staining Revealing Thick Collagen Bundles in the Dermis.
Treatment options considered were low doses of steroids, immunomodulators and a good control of diabetes mellitus. The immunomodulator preferred was Methotrexate in three patients and Tacrolimus local application in another. Colchicine was also used in one of them. One patient, who had diffuse involvement and rapid progression received phototherapy with Psoralen + ultraviolet A (PUVA), along with Methotrexate. They were followed up for a median of 18 months (range 15-24), but no decrease in skin thickening was observed in any of them. There was an increase in the skin thickening.
Discussion
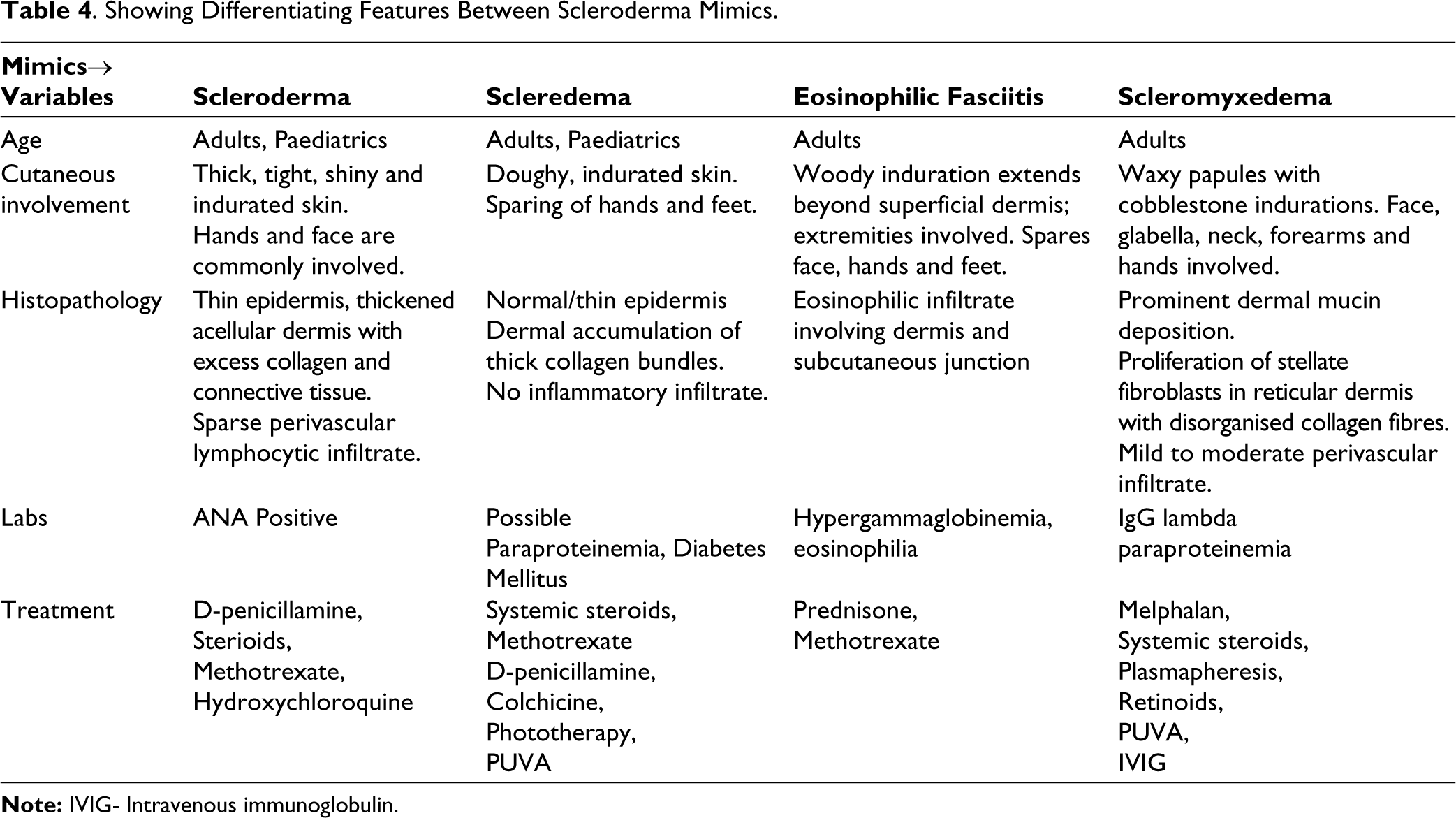
We have described five cases of Scleredema. They had typical presentation, histopathology and response to the treatment as described in the literature. It is prudent to distinguish between the mimickers of SSC as a definitive diagnosis may foretell a favourable or a poor prognosis, guide further screening and thus direct us towards the appropriate therapy. Table 4 compares and contrasts some of the key features of common scleroderma mimickers.
Showing Differentiating Features Between Scleroderma Mimics.
We reviewed the previous publications and compared them with our cases. The largest series on Scleredema was reported in 1984 which described 33 patients from the Mayo Clinic where it was observed that the disease was of insidious onset with a prolonged course. The patients were divided into two groups based on the presence or absence of diabetes. Diabetes when present, was typically late onset, Type 1 and difficult to control. 6 Another study from China published in its original language included 67 patients and another retrospective study from Martinique included 49 patients enrolled. The study was published in French where the median age at diagnosis was 50 years and it was mostly associated with obesity, diabetes and monoclonal gammopathy. 7 Another retrospective multicentre study involving 44 patients was conducted by F. Rongioletti et al. where the mean age of diagnosis of Scleredema was 53.8 years and the most commonly associated disease was diabetes mellitus, that too Type 2 diabetes seen in 30 patients and monoclonal gammopathies were present in five cases. 8
Treatments either with combination or sequential were used. The outcomes are also variable. Phototherapy was associated with a higher but partial response. Our study confirms some of the previously described features of typical Scleredema, such as the mainly affecting adults in their fifties or sixties, marked association with diabetes with male predominance.
Management of Scleredema is not well defined. When a preceding infection is suspected, antibiotics can be used. Penicillin use in documented recent streptococcal infections has been suggested. UV light, Radiation therapy, and immunosuppressants such as corticosteroids, Methotrexate, and immunoglobulin (IVIg) have been advocated for use in the treatment of Scleredema variable therapeutic benefit. 2 Topical and intra-lesional corticosteroids, injection with hyaluronidase, Factor XIII, Cyclosporine, and other therapies such as pentoxifylline, Colchicine, interferon-gamma and D- penicillamine have been tried but to be unsuccessful. 9 Extracorporeal photopheresis involving the exposure of 10%-20% of the body’s leucocytes being photoactivated 8-methoxypsoralen and their re-infusion to the patient has been reported to be successful in a report by Stables et al. There was a regression of skin lesions in a patient with Scleredema and paraproteinaemia after six months of treatment. 9 In Scleredema diabeticorum, Diabetic control has been the initial management. In one series of four cases of Type 1 diabetes, a significant decrease of glycated haemoglobin from 9.3% to 7.9% showed an improvement in skin thickening. 10 In another series, five out of eleven, Scleredema lesions improved partially with good glycaemic control. 11 However, some other reports did not show improvement of the Scleredema after improving glucose control. 5 As for treatment, the majority of reports on therapy modalities seem to be arbitrary. Our data suggests initial treatment with phototherapy, ideally Ultraviolet A1 for patients with disabling manifestations. Oral Psoralen plus ultraviolet A (PUVA) therapy has also been reported effective in patients with Scleredema. The mechanism of the action of PUVA appears due to increased production of collagenase synthesis by fibroblasts and by inhibiting de novo synthesis of Type 1 collagen. 12
Electron beam radiation therapy can be used in the treatment of Scleredema because of its ability to induce apoptosis in abnormal dermal fibroblasts and interfere with cell signalling by decreasing collagen and mucin production. 13 Treatment with electron beam radiation therapy may be a viable option for Scleredema patients with limited treatment options as reflected in a case series by Bowen et al. where he observed varying degrees of improvement in three patients with diabetes and severe forms of Scleredema treated with radiation. 13
There are some case reports showing the use of Colchicine along with PUVA in the successful treatment of scleredema adultorum of Buschke.14,15 PUVA can decrease Type I and III collagen formation and collagen mRNA levels in a dose-dependent manner. UVA can stimulate collagenase synthesis by human dermal fibroblasts and further potentiate the degradation of sclerotic tissue. Colchicine by interfering with the transport and secretion of collagen, has an inhibitory effect on collagen. It also suppresses the TGF-ß-induced upregulation of Type I collagen mRNA expression and basal level of Type I collagen mRNA in human dermal fibroblasts. Hence, a combination of these two methods might have a synergistic effect in the treatment of Scleredema. 14 Due to concern for adverse effects, Systemic corticosteroids and immunosuppressive drugs may be reserved for patients with persistent, debilitating diseases who have phototherapy failed or for patients with scleredema-associated gammopathies. Treatment of primary disease with strict glycaemic control and in combination with physical therapy in patients with motion or respiratory disability should be considered. Specific guidelines for the management of Scleredema are not available and the therapy is based on published case reports, small case series and retrospective studies reporting unsuccessful outcomes. It is recommended that the therapy for scleredema adultorum be individualised, taking into account the associated conditions of the patient, severity of Scleredema, and potential trigger factors.
Conclusion
SSc mimics like Scleredema adultorm of Buschke must be suspected in patients presenting with diffuse skin thickening, especially of the upper body and sparing the hands and feet. Prompt diagnosis, evaluation for monoclonal gammopathy, underlying autoimmunity and prompt control of diabetes must be the mainstay in the management of these cases. Treatment modalities are still not effective and need to be evaluated.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Approval from the Ethical Committee was obtained (Letter No. AIMS/IEC/20/2024; EC Registration No. EC/NEW/INST/2023/KA/0383).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.