
Abstract

POS001
Choice of Disease Modifying Drug in RA Patients Refractory/Intolerant to Methotrexate: Has Tofacitinib Replaced Others – Single Center Study
To find out which DMARD was prescribed in our patients with MTX refractory/intolerant disease and to look for reasons for the same. To compare diagnostic delay/whether seen by other specialists before coming to us etc with another series.
Data was collected from the outpatient summaries recorded at the IQVIA EMR software at our tertiary care centre. Informed consent was taken.
Studies from recent study from theWest showed tofacitinib usage in 13.6% as 2nd line and 0.8% in another (2), (3).
Image and Bar Table 1

Image and Bar Table 2

POS002
Glycome Profiling of Serum IgG Antibodies in Active and Remission Rheumatoid Arthritis Patients: Role in Disease and Clinical Implications
POS003
Efficacy of Upfront Low Dose Rituximab in Treatment Resistant Rheumatoid Arthritis
POS004
Clinical Global Assessment and Psychiatric Morbidity with Effects on Disease Burden in Patients of Rheumatoid Arthritis- A Multicentric Study
POS005
To Study the Effects of Disease Control on Lipid Profile in Rheumatoid Arthritis -A Prospective Observational Study
POS006
Prevalence of Anaemia of Chronic Disease in Rheumatoid Arthritis and It’s Correlation with Disease Duration and Severity
POS007
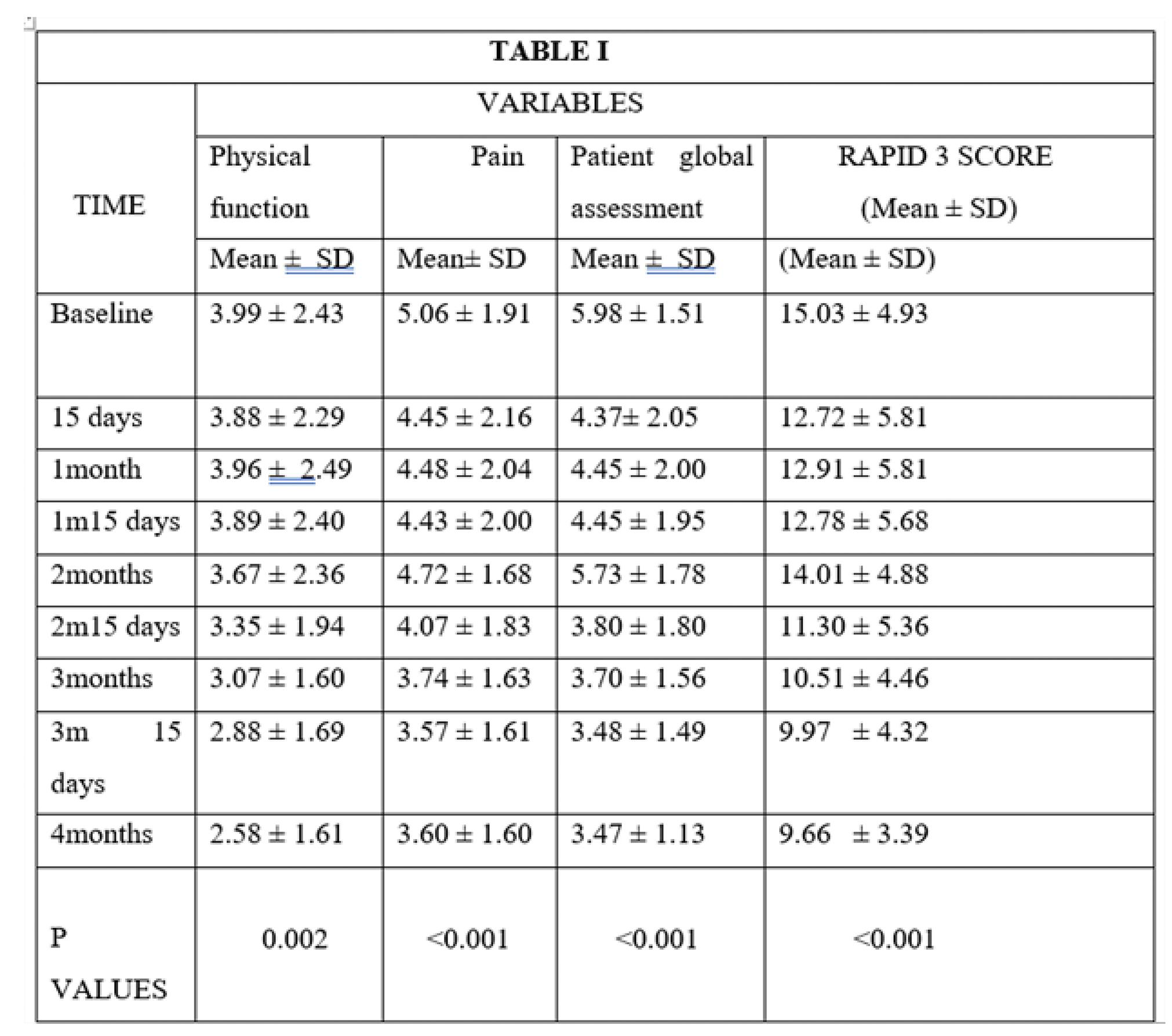
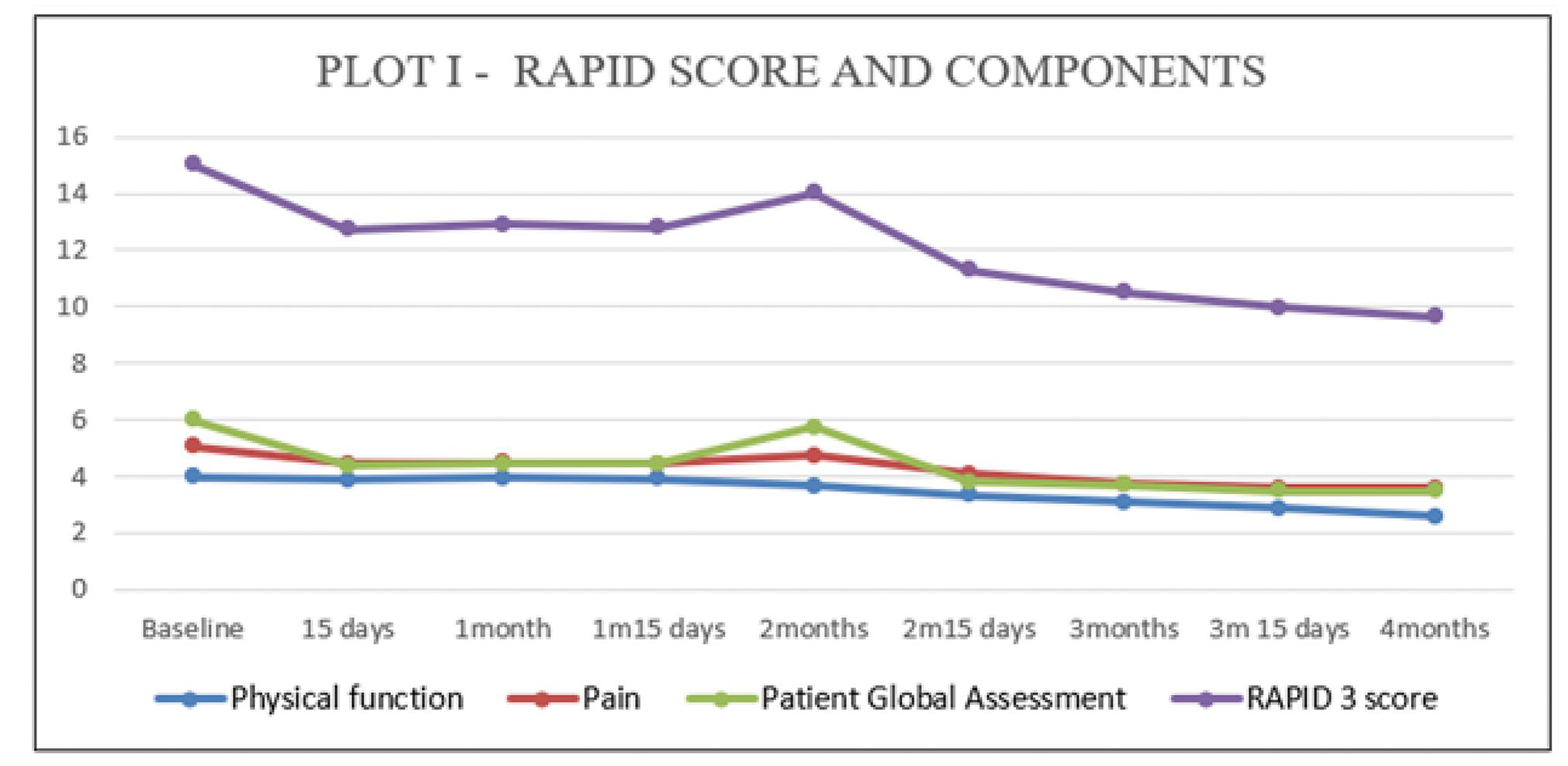
Domicillary Clinical Followup for Rheumatoid Arthritis Patients for Disease Severity Using Rapid 3 Score
Image and Bar Table 1
POS008
Serial Changes in P-Glycoprotein Expression on Peripheral Blood Lymphocytes in Patients with RA Following Immuno Suppressive Therapy - Longitudinal Study
To compare p glycoprotein and MRP 1 expression and function on lymphocytes with newly diagnosed treatment naïve RA at baseline and 3 months after DMARDS.
Image and Bar Table 1

Image and Bar Table 2

POS009
Predictors of Cardiovascular Risk in Rheumatoid Arthritis
1. Jagpal A, Navarro-Millan I. Cardiovascular co-morbidity in patients with rheumatoid arthritis: a narrative review of risk factors, cardiovascular risk assessment and treatment. BMC Rheumatol. 2018; 2:10.
2. Cox JH, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ 2017; 357:j2099
Image and Bar Table 1

Image and Bar Table 2

POS010
Impact of Disease-Modifying Antirheumatic Drugs on Inflammation in Patients with Rheumatoid Arthritis: A Retrospective Analysis of Long-Term Follow-Up in A Kazakhstani Cohort
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by inflammatory polyarthritis and the involvement of internal organs. RA is a socially and economically significant condition due to frequent disability and high treatment costs. The prevalence of RA varies between 0.5-2% of the adult population worldwide and is associated with premature mortality, with an average reduction in life expectancy of 3-10 years. In the Republic of Kazakhstan, the prevalence and incidence of RA are 0.37% and 0.086%, respectively.
This was a retrospective cohort study performed at a tertiary public hospital between 2015 and 2023. Patients were adults (age >18 years) who regularly attended an outpatient RA clinic. Patients with other systemic inflammatory conditions were excluded, as were patients from the original cohort whose follow-up duration was less than 12 month. The study protocol was approved by the institutional Research Ethics Committee. In compliance with the Declaration of Helsinki, all patients gave informed consent for the T2T strategy, and investigators signed a data use agreement.
At the time of inclusion in the study, 16 patients out of 142 died. The mean life expectancy from onset to death was 125 months. The mean age at death was 66, 5 years. Causes of death were: chronic renal failure due to secondary amyloidosis-6, 25%, cardiovascular diseases (primarily cerebrovascular disorders and myocardial infarction) -31, 25%, oncological diseases-25%, side effects of therapy (gastrointestinal bleeding) -12, 5%, complication of COVID-19 (heart failure) -12, 5%.
Patients in remission were all female, mean age 49.6 years, mean disease duration 24 months, positive RF and ACCP (+). In 2 patients the duration of therapy with csDMARDs (MTX-15 mg) was 30 months and 1 csDMARDs (MTX-15) with GC (4 mg) was 132 months.
The probability of achieving remission was higher in patients with fewer comorbidities, absence of EAM, early diagnosis and T2T strategy of RA.
The study data demonstrated a statistically significant reduction in disease activity. The mean value of DAS28 was 3, 9±0, 64. Remission or low activity was achieved in 24, 5 %, remission -3, 1% patients during the study.
Image and Bar Table 1


POS011
Endothelial Dysfunction and QRISK3 in Rheumatoid Arthritis
Image and Bar Table 1

Image and Bar Table 2

POS012
Exploring Knowledge Gaps Among RA Patients-A Single Center Cross Sectional Questionnaire Based Study
John Britto S1, Anna C Das2, Ramya Janardana3, Sumithra Selvam4, Prem Mony5,
To identify socio-demographic determinants for knowledge barriers among RA patients.
Image and Bar Table 1

Image and Bar Table 2

POS013
Comparing Efficacy of Combination Therapy: Leflunomide, Sulfasalazine or Tofacitinib with Methotrexate in Rheumatoid Arthritis with Methotrexate Inadequate Response -Randomised Open Label Study
Image and Bar Table 1


POS014
Efficacy of Upfront Low Dose Rituximab in Triple Therapy Resistant Rheumatoid Arthritis
Ashaq Parrey1, Adarsh Lakshman, Mohd Ismail, Ajaz Kariem; 1Government Medical College Srinagar.
POS015
The Consequences of Delayed Referrals and Inadequate Access to National Health Service- A Questionnaire Based Cross-Sectional Study from Karnataka Chapter of Indian Rheumatology Association (KRA)
Median expenditure incurred prior to referral to rheumatologists was INR 35000/- (IQR 5000-40000) which amounted to catastrophic expenditure (>20%) of their annual income for 585 (27.2%) patients. Seventy three percent of our cohort (n=1565) took > 6 months for a Rheumatologist referral and mean of 3 (0-36) non Rheumatological consultations before consulting the Rheumatologist (Table1).
There was a non-significant positive relationship between rural/urban population and the money spent before specialist consultation, negative relationship between amount spent before specialist consultation and disability index, and DAS-28 score was observed (p > 0.05) using logistic regression analysis. Multiple linear regression models did not show significant correlation between pre-referral expenditure, annual expenditure, HAQ-DI and DAS-28 scores (p>0.05).
Image and Bar Table 1

Image and Bar Table 2

POS016
Comparison of FIB-4 Score with FibroScan for the Assessment of Liver Fibrosis in Patients of Rheumatoid Arthritis on Long Term Methotrexate
Mean treatment duration with methotrexate was 9.1 years (4-27), with mean cumulative dose of 6.3g (1.9-14.4).
FibroScan showed mean liver stiffness measurement (LSM) of 6.06 kPa (2.2-24.3), mean Controlled attenuation parameter (CAP) of 242.7 (108-387). The METAVIR scoring of fibrosis showed F0-F1 in 162 (81%), F2 in 20 (10%), F3 in 10 (5%) and F4 in 6 (3%) of patients.
FIB-4 score was calculated using the formula (Age x AST) /(Platelets x √ (ALT)). The mean FIB-4 score was 1.37 (0.17-4.82).
Abnormal liver parameters in the form of elevated SGOT or PT levels were 23 (11%), FibroScan of >=F2 in 36 (18%), FIB-4 values >1.3 in 78 (40%) and >2.67 in 15 (7.7%).
The correlation coefficient between FIB-4 scores and LSM values yielded a moderate positive correlation (R=0.53) (Figure 1).
The correlation between FIB-4 scores and CAP values of FibroScan yielded a weak positive correlation (R=0.07).
One study of FIB-4 in RA showed FIB-4 >1.45 in 29%, vs 40% >1.3 in our study.
Another study on 56 patients demonstrated 18% prevalence of fibrosis by Fibroscan but 2% by FIB-4. However, correlation was not studied.
Image and Bar Table 1

Image and Bar Table 2

POS017
Study of Comorbidities and Extra Articular Manifestations in Patients of Rheumatoid Arthritis and their Prevalence with Seropositivity
Mahin O.S, Jyotsna Oak,
To investigate the prevalence of comorbidities in RA patients and their association with positive rheumatoid factor and anti-CCP antibody status. To examine the extra-articular manifestations in RA patients and their prevalence among seropositive and seronegative individuals. To assess the relationship between disease severity, as measured by the DAS28-ESR score, and the presence of extra-articular manifestations.
POS018
Assessment of Vitamin D in Patients with Rheumatoid Arthritis and Its Correlation with Disease Activity
1. Deluca HF, Cantorna MT. Vitamin D: Its role and uses in immunology. FASEB J. 2001;15:2579–85. [PubMed] [Google Scholar]
2. Cantorna MT. Vitamin D and autoimmunity: Is Vitamin D status an environmental factor affecting autoimmune disease prevalence? Proc Soc Exp Biol Med. 2000;223:230–
3. [PubMed] [Google Scholar]
POS019
Assessment of Caregiver Burden in Primary Caregivers of Patients with Rheumatoid Arthritis – A Cross-Sectional Study (Interim Analysis)
Image and Bar Table 1

POS020
The Function of Platelet to Lymphocyte Ratio (PLR) and Neutrophil to Lymphocyte Ratio (NLR) in Assessing Disease Activity in Rheumatoid Arthritis Patients
Image and Bar Table 1

Image and Bar Table 2

POS021
Efficacy and Safety of Tofacitinib in Rheumatoid Arthritis Associated Interstitial Lung Disease (RA-ILD): A Systematic Review and Meta Analysis
Naitica Darooka1, Khadeejah Hussain2, Sachi Kalawadia3, Tithi Wade4, Adarsh Kawalkar5, Aniruddh Bansal6,
Image and Bar Table 1

Image and Bar Table 2

POS022
Effect of Disease Activity on Neutrophil -Lymphocyte Ratio and Platelet - Lymphocyte Ratio in Newly Diagnosed Rheumatoid Arthritis Patients
Sindhu Rao Malla,
NLR and PLR are simple hematological parameters which can be employed to monitor thedisease activity in rheumatoid arthritis patients. There is a need for multi-centre, large sample studies to use NLR and PLR as surrogate markers of inflammatory activity in rheumatoid arthritis patients in comparison with DAS28, ESR and CRP.
Image and Bar Table 1

POS023
Assessment of the Anti-Rheumatoid Properties of Curcuma Caesia Through In-Silico, In-Vitro, and In-Vivo Approaches
POS024
Quantifying Indirect Cost of Rheumatoid Arthritis: A Comprehensive Analysis of the Cost of Productivity Loss from A Multicenter Cohort
To assess the cost of productivity loss from absence or inefficiency at paid or unpaid work due to Rheumatoid arthritis. To determine disease-related and demographic contributors to significant productivity loss.
The cost of lost unpaid work was more than the cost of absenteeism, which was more than the cost of presenteeism (Table 1). Comparison of disease severity with cost showed significant association between high DAS-28 and unpaid work loss, whereas high CDAI also incurred significant costs from work-absenteeism, loss of paid work and total cost (Table 2). High HAQ-DI was significantly associated with all forms of indirect cost. Among socio-demographic parameters, those belonging to lower Kuppuswamy socioeconomic class had significant costs from loss of unpaid and paid work, whereas those with higher education suffered significant losses from paid work.
Image and Bar Table 1


POS025
Prevalence of Metabolic Syndrome Among Patients with Rheumatoid Arthritis
Metabolic syndrome involves risk factors like abdominal obesity, high triglycerides, low HDL cholesterol, elevated blood pressure, and high fasting glucose, which increase cardiovascular morbidity. The National Cholesterol Education Program Adult Treatment Panel III defines metabolic syndrome by the presence of three or more of these factors. This study aims to evaluate the prevalence of metabolic syndrome in RA patients in an urban hospital in Bangalore, helping identify those needing additional management to reduce cardiovascular risks.
Primary: To determine the proportion of RA patients with metabolic syndrome. Secondary: To study associated factors for metabolic syndrome in RA patients.
POS026
Assessment of Nutritional Status, Nutrient Adequacy & Musculoskeletal Strength in Subjects with Rheumatoid Arthritis
POS027
Sleep Quality in Patients with Rheumatoid Arthritis and It’s Association with Pain, Disease Disability and Disease Activity
To identify sleep issues and their relationship with pain thresholds, disease activity, and functional impairment in RA patients. To examine the correlation between sleep quality and inflammatory markers in RA.
Correlation of different sleep scale with age, pain Intensity, CRP, CDAI, ESR, HAQ-DI score in RA.

POS028
Assessment of Dietary Intake and Body Composition in Subjects with Rheumatoid Arthritis
POS029
Clinical Characteristics and Associations of Interstitial Lung Disease in Rheumatoid Arthritis- A Retrospective Cohort Study
Harikrishnan Gangadharan,
Interstitial lung disease (ILD) is a major cause of morbidity and mortality in Rheumatoid arthritis (RA).
Symptomatic ILD was seen in 37 patients (8.1%), 83.7% were female. The mean age of ILD patients was 57.4 ± 9.9 years and median disease duration was 72 (24-180) months. 89.1% of ILD patients were RF positive. The most common patterns were organising pneumonia (26.6%), definite UIP (20%) and fibrotic NSIP (20%) On follow up, 13 patients underwent a serial HRCT Thorax to assess ILD progression and radiological progression was noted in 6 patients (46.15%). On univariate analysis, older age (57.14 ± 9.94 vs 51.14 ± 10.9, p<0.001) and longer disease duration (97.4 vs 36 months, p <0.026) were associated with RA-ILD. On binomial logistic regression, older age and longer disease duration were significantly associated with RA-ILD (Table 1).
Image and Bar Table 1

POS030
Efficacy, Safety and Immunogenicity of A Biosimilar Adalimumab Advixa→ Compared with the Reference Product Humira→ in Patients with Rheumatoid Arthritis in Bangladesh
No significant difference between the groups was found with regard to the 6 serious and 105 non-serious AEs. There was no significant intergroup difference in the change in anti-adalimumab antibody titers from baseline to week 12 (P > 0.2).

POS031
Efficacy and Safety of Tofacitinib in the Management of Rheumatoid Arthritis: A Real-World Multicenter Study in India
Dr Nishikant Madkholjar, Dr Roshan Pawar and Dr Akhilesh Sharma are full-time employees of Alkem Laboratories. No any other conflict of interest.
POS032
Economic Burden of Rheumatoid Arthritis: A Cross-Sectional Study at A Tertiary Healthcare Center
Rheumatoid arthritis (RA) imposes a substantial economic burden and severely affects quality of life. Globally, the financial impact of RA is well-documented, but in India, the situation is compounded by unique social dynamics. Most patients are women with limited financial independence, and inadequate healthcare coverage for autoimmune diseases exacerbates the economic strain. The inability to perform household duties further disrupts family stability. Understanding the economic burden and social dynamics of RA in India is essential for addressing these challenges and informing healthcare policies.
Direct medical costs, including RA medications and lab tests, accounted for significant annual expenses, averaging ₹36,094± 8,522 per patient which was 78% of total annual health expenditure. Non-medical costs such as travel and other expenditures (₹7,476+ 8,147) added to this financial strain. Cost of medication (₹23,417 ± 6, 777) accounted for 65 % of Direct cost of illness of RA. (Table2) Although the annual expenditure on RA in India, at about $558, seems low compared to higher-income countries, the relative financial burden is significant 20.4% of GDP per capita.
Image and Bar Table 1

Image and Bar Table 2

POS033
Translation of Rheumatoid Arthritis Disease Activity Index-5 (RADAI-5) to Punjabi Language Version and Its Correlation with Disease Activity Score 28 (DAS28) and Clinical Disease Activity Index (CDAI)
Ravreet Pal Kaur1,
POS034
Tofacitinib Safety in Inflammatory Arthritis (Rheumatoid Arthritis, Seronegative Arthritis, and Psoriatic Arthritis): A Real-World Cross-Sectional Large-Number Study
Image and Bar Table 1

Image and Bar Table 2

POS035
Evolving Therapies in Rheumatoid Arthritis: A Systematic Review of Disease Modifying Anti Rheumatic Drugs
The inclusion criteria were randomized controlled trials (RCTs) and cohort studies that evaluated efficacy and safety of DMARDs in adults diagnosed with rheumatoid arthritis.
A total of 15 studies met inclusion criteria and were analyzed.
Image and Bar Table 1

Image and Bar Table 2

POS036
Familial Clustering and B27 Positivity Indicate that Diffuse Idiopathic Skeletal Hyperostosis is a Spondyloarthritis-Spectrum Condition: Results from A Clinical Study/Case Series
Image and Bar Table 1


POS037
Renal Involvement in Spondyloarthritis: Case Series
1. He D, Wang R, Liang S, Liang D, Xu F, Zeng C, et al. Spectrums and Prognosis of Kidney Disease in Patients with Ankylosing Spondylitis. Kidney Dis. 2020 Nov;6 (6):444–52.
Image and Bar Table 1

Image and Bar Table 2

POS038
Mapping the Clinical Profile of Ankylosing Spondylitis Patients Prescribed Etanercept in India
Most of the patients had a medication history of taking some or other NSAID (95%). Other drugs which were previously consumed by the patients included DMARDS (73.7%) & steroids (32.1%). Most common comorbid disorders reported among the patients were hypertension (30%) and diabetes (14.1%). Anxiety, depression and sleep disturbance were present among 26.2%, 20.4% and 43% patients respectively.
Involvement of peripheral joint, hip or shoulder joint and stiffness or pain in neck were seen among 35%, 32% and 63% patients respectively. Erythrocyte Sedimentation Rate (ESR) was done in 472 patients with a mean value of 45.3±19.11 mm/hr. Among patients who were subjected to HLA-B27 testing, 70.2% were HLA-B27 positive while the rest of 24.98% patients were HLA-B27 negative.
81.6% of the patients were prescribed ETN in dose of 50mg/week while 15.8% of patients received ETN dose of 25mg twice weekly. Etanercept was utilized for up to 3 months among 50.0% patients and up to 6 months in another 27.7% of patients. 4.1% of patients received ETN for more than a year. Methotrexate, NSAIDS, Sulfasalazine & glucocorticoids were commonly co-prescribed with ETN.
POS039
Comparing Efficacy of Tofacitinib V/S Adalimumab in Axial Spondyloarthritis.
Image and Bar Table 1


POS040
Multi Centric Case Series on Incidence of Thrombosis in Patients Using Tofacitinib for Rheumatological Diseases on Behalf of SIG on Spondyloarthritis -IRA
After this event, tofa had been stopped and disease had been well controlled with ORAL DMARDs, that included methotrexate, iguratimod, sulfasalazine and prednisolone.
No CV risk in our patients except two had well controlled diabetes and hypertension. Further studies are required.

POS041
Sequential Therapy with TNF Inhibitors and Tofacitinib in the Management of Radiographic Axial Spondyloarthritis
Image and Bar Table 1

POS042
Utility of a Biomarker HLA B27 in the Diagnosis of Spondyloarthritis: A Retrospective Study
Image and Bar Table 1

Image and Bar Table 2

POS043
Prevalence of Sexual Dysfunction in Male Patients of Ankylosing Spondylitis and Its Correlation with Disease Activity
Avdesh Giri,
Image and Bar Table 1

Image and Bar Table 2

POS044
Total Hip Arthroplasty in Patients with Axial Spondyloarthritis: Clinical Features and Risk Factors
Image and Bar Table 1

POS045
Normal Versus Elevated CRP Spondyloarthritis - are both these Subgroups Same or Different? A Descriptive Study from A Single Centre
Image and Bar Table 1


POS046
Impact On Work Productivity Among Patients with Axial Spondyloarthritis in A Rheumatology Specialized Care Centre in Sri Lanka
Image and Bar Table 1

Image and Bar Table 2

POS047
Real World Data of Tofacitinib in the Patients of Spondyloarthritis
Age >16 years Patients fulfilling ASAS criteria for axial and/or peripheral disease, non-responded to NSAIDs and CsDMARDs ASDAS ESR or CRP score > 2.1 for predominant axial disease or Active peripheral arthritis
Age >50 years Psoriatic Arthritis IBD
After 3 months of Tofacitinib therapy, this study observed significant difference in all the disease parameters. The mean difference of SJC, TJC, MASES, BASDAI, BASFI, BASMI, ASDAS-ESR, ASDAS-CRP from baseline to 3-month tofacitinib therapy was - 0.73, - 1.92, - 0.37, - 2.03, - 1.77, - 0.83, - 1.44, - 1.63 (p < 0.05). 63% achieving BASDAI 50 response, ASDAS-CRP, MCID & MI was noted in 70% & 42%. ASDAS-CRP LDA & Inactive disease states were seen in 65% & 31% respectively. URTI were more commonly reported (41 events). Other side effects in our study population were headache (31 events), diarrhoea (9 events), 1 event each of pneumonia, abdominal pain and uveitis. Three events of mild transaminitis, Weight gain is seen in 17% of patients and no cases of herpes zoster infection during the treatment period.
Treating SpA patients with Tofacitinib can reduce the need of Anti-TNF therapy, in financially constrained population.
In areas with limited resources, it can be utilized cost-effectively as a next line of therapy for patients who are not responding to NSAIDs & CsDMARDs.
Image and Bar Table 1

Image and Bar Table 2

POS048
Efficacy and Safety of Tofacitinib and Its Comparison with TNF Inhibitors in Axial Spondylarthritis Patients
To assess the safety of tofacitinib in the treatment of axial spondyloarthritis.
POS049
Impact of Gender Differences on Clinical Spectrum of Spondyloarthritis Patients: A Real World Study
Male patients receiving bDMARDs at baseline had higher remission rates at 6 months (74.54% vs. 50%, p value 0.06) and females had more refractory disease, as 37.5% of patients had HDA or VHDA as compared to only 7.27% in males (p = 0.002). Of the 123 patients receiving csDMARDs at baseline, 62 patients (48 males and 14 females) had achieved remission, and 34 patients (27 males and 7 females) were switched to bDMARDs over course of 6 months.
Image and Bar Table 1

POS050
Exploring the Utility of Generative Artificial Intelligence for Aiding Literature Review in Rheumatology Using Psoriatic Arthritis Treatment Guidelines as a Test Case
We also fine-tuned another model- DistilBert; training it to assess quality of evidence presented within an article. This was then used to classify the forty-nine articles under study into grades of ‘strong’, ‘moderate’, ‘neutral’, and ‘poor’. The results generated by it were compared with manual labelling of the same articles based on the universally accepted hierarchal grades of evidence.
Image and Bar Table 1

POS051
Efficacy of Ixekizumab (IXE) In Psoriatic Arthritis (PsA) and Psoriasis (PsO) - Real World Data
Patients were mandatorily assessed by our rheumatologist at baseline and subsequent follow-up visits. Descriptive statistics were represented as percentages and proportions. Group differences were carried out using paired t-test (differences at baseline and post-treatment) a p-value less than 0.05 was considered statistically significant. Statistical tests were carried out employing Jamovi. Data was collected using an approved CRF.
Image and Bar Table 1


Image and Bar Table 2

POS052
Genome-Wide Genotyping Yields New Susceptibility Loci in An Indian Cohort of Psoriatic Arthritis Patients
Table 1 describes the genes found to have a suggestive association with susceptibility to PsA.
Image and Bar Table 1


POS053
Liver Abnormalities in Patients with Psoriatic Disease: Experience from A Tertiary Care-Teaching Hospital
To identify prevalence and predictors of liver abnormalities in patients with psoriatic arthritis.
We identified PsA patients who had developed elevated serum transaminase or alkaline phosphatase level during the period 2022-2024 august.
Transaminitis was defined as elevated ALT and or AST more than upper limit of normal (ALT >41, AST >41). Persistent transaminitis was defined as elevated ALT and or AST for more than 3 consecutive visits.
Patients who had fatty liver or coarsening of echotexture in liver were also included. ARFI values >1.2 were taken as abnormal. Changes in therapy due to subclinical liver abnormalities were also noted.
Patients who developed transaminitis, fatty liver, cirrhosis on ultrasound and abnormal ARFI values were taken as cases. Controls were patients with psoriatic arthritis from the same cohort who never had such abnormalities or liver disease during the study period.
Data was analysed using SPSS 41.
51 patients had developed transaminitis, while persistent transaminitis was seen in 13 of them.
Of the patients who had developed transaminitis, ultrasound abdomen showed abnormalities in 28 and ARFI showed deranged values in 23.
Male patients were more seen to develop liver abnormalities. Presence of obesity, higher BMI, history of alcohol intake, lower HDL levels, higher cumulative dose of methotrexate were significantly associated with liver abnormalities. There was no difference between the two groups with regards to age at diagnosis of psoriasis or PsA, or duration of disease, use of leflunomide or complementary alternative medicine. 21 patients were switched to biologics in view of persistent transaminitis or abnormal imaging.
Image and Bar Table 1

Image and Bar Table 2

POS054
Subclinical Atherosclerosis in Relation to Ultrasonographic Enthesopathy in Psoriasis Patients, A Single Center Case Control Study
We have compared the total entheseal score with CIMT, BMI, Serum Total cholesterol, Serum LDL, HDL, VLDL, and Triglycerides. These results were compared with age-matched controls by standard t-test.
Image and Bar Table 1


POS055
Time Interval Between Psoriasis and Psoriatic Arthritis Onset: Clinical and Demographic Correlations in A Clinic-Based Cohort
Image and Bar Table 1

POS056
Unveiling the Hidden Load: Exploring the Impact of Psoriatic Arthritis Among Psoriasis Patients
Image and Bar Table 1

Image and Bar Table 2

POS057
Nail Entheseal Complex Ultrasonography and Nailfold Capillaroscopy in Psoriatic Arthritis and Rheumatoid Arthritis
POS058
Adverse Effect Profile of Tofacitinib: A Real-World Scenario
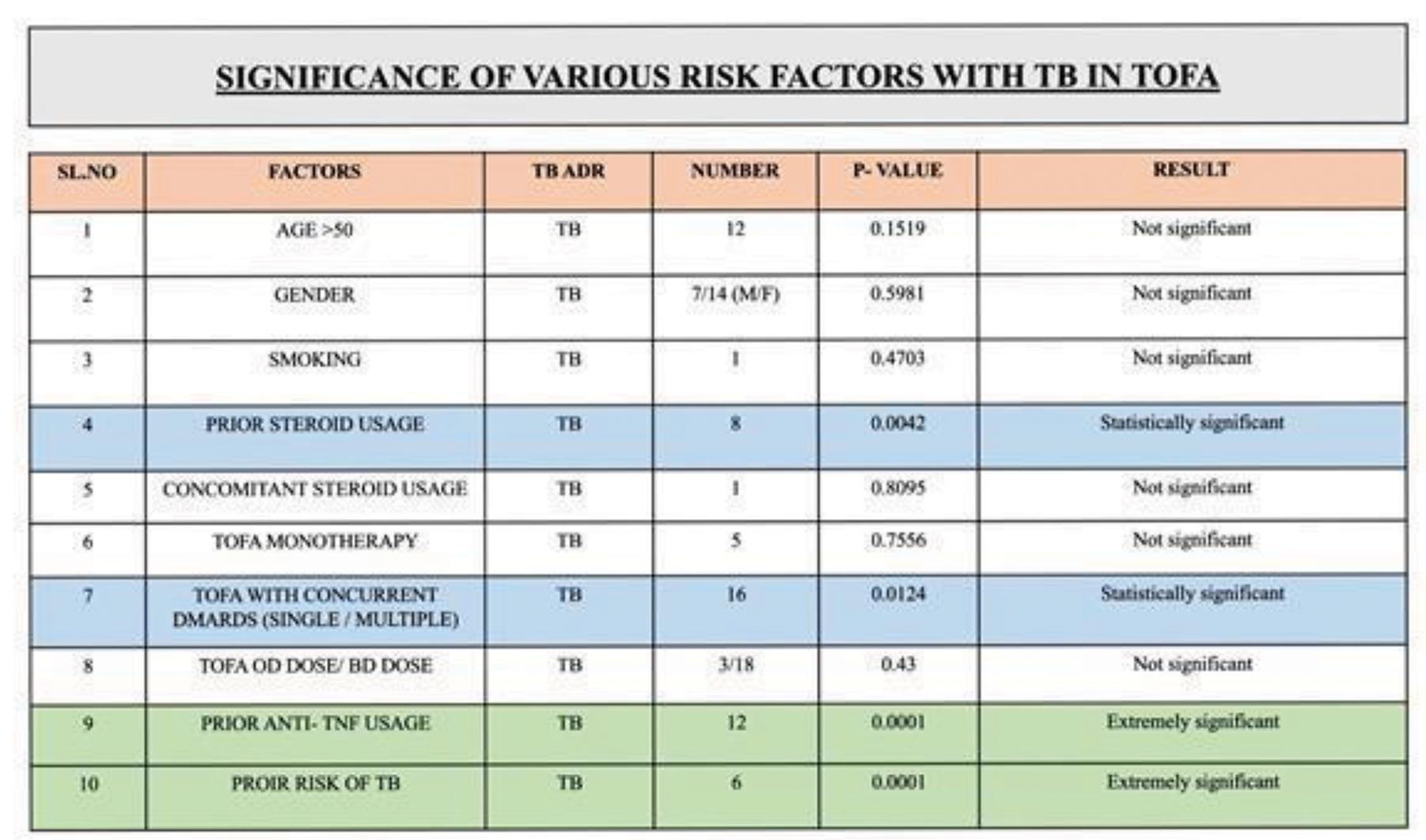
During Tofa treatment, 11 patients (2.8%) developed herpes zoster after an average of 32.9 weeks, all had single dermatomal involvement and one had recurrent episodes. TB was observed in 3 patients (0.8%), with an average onset of 25.3 weeks following the initiation of Tofa. Pulmonary TB was observed in 2 and TB lymphadenitis in 1. TB reactivation was noted in one patient. Furthermore, 3 patients were hospitalized for severe pneumonia, including one case attributed to Burkholderia cepacia. In all of them, Tofacitinib was stopped.
Image and Bar Table 2

POS059
Predictors of Response to Intra-articular Glucocorticoids in Primary Osteoarthritis of the Knee
Primary outcome was the change in WOMAC at 3 months while secondary outcomes were WOMAC scores at 1 and at 6 months. Predictors assessed by univariate regression included age, sex, BMI (body mass index), disease duration, FRAX (Fracture Risk Assessment Tool), PainDETECT questionnaire, presence of fibromyalgia, CCI (Charlson comorbidity index), laboratory parameters and baseline WOMAC score. Variables with p<0.1 were included in the multivariate analysis using Generalized Linear Modelling (GLM).
The median WOMAC score improved from 40 (IQR:34.75-44) to 32 (28-36) at 1 month (p<0.001), 32 (28-36) at 3 months (p<0.001), 34 (28-36) at 6 months (p<0.001) [Figure 1A]. The primary outcome, WOMAC at 3 months was significantly lower than the baseline WOMAC score [Figure 1B]. Similarly, WOMAC-pain, WOMAC-stiffness and WOMAC-function were all improved at 3 months [Figure 1C-E].
In the univariate models, BMI (p=0.074), CCI (p=0.06), presence of hypertension (p=0.021), erythrocyte sedimentation rate (p=0.016), creatinine (p=0.096), fibromyalgia (p=0.085), and baseline WOMAC (p=0.004) were predictors of change in WOMAC by 3 months. However, age, sex, disease duration, Diabetes mellitus, CKD, tender points, PainDETECT, haemoglobin, C-Reactive protein, alkaline phosphatase, Kellgren Lawrence (KL) grade on radiographs, FRAX score of hip or spine were not associated with improvement in WOMAC.
In the multivariate model, age, BMI, presence of hypertension, haemoglobin and creatinine levels, and baseline WOMAC were independently associated with changes in WOMAC at 3 months, while the associations of fibromyalgia and radiological KL grade were borderline. Findings for WOMAC-pain, WOMAC-function were similar. WOMAC-stiffness was not assessed due to low variations (figure 1D).
Image and Bar Table 1

Image and Bar Table 2

POS060
Efficacy and Safety of Polmacoxib 2 mg in Adult Patients with Idiopathic (Primary) Osteoarthritis of Hip/Knee - A Randomized, Double Blind, Active-Controlled, Phase III Clinical Study
Image and Bar Table 1


POS061
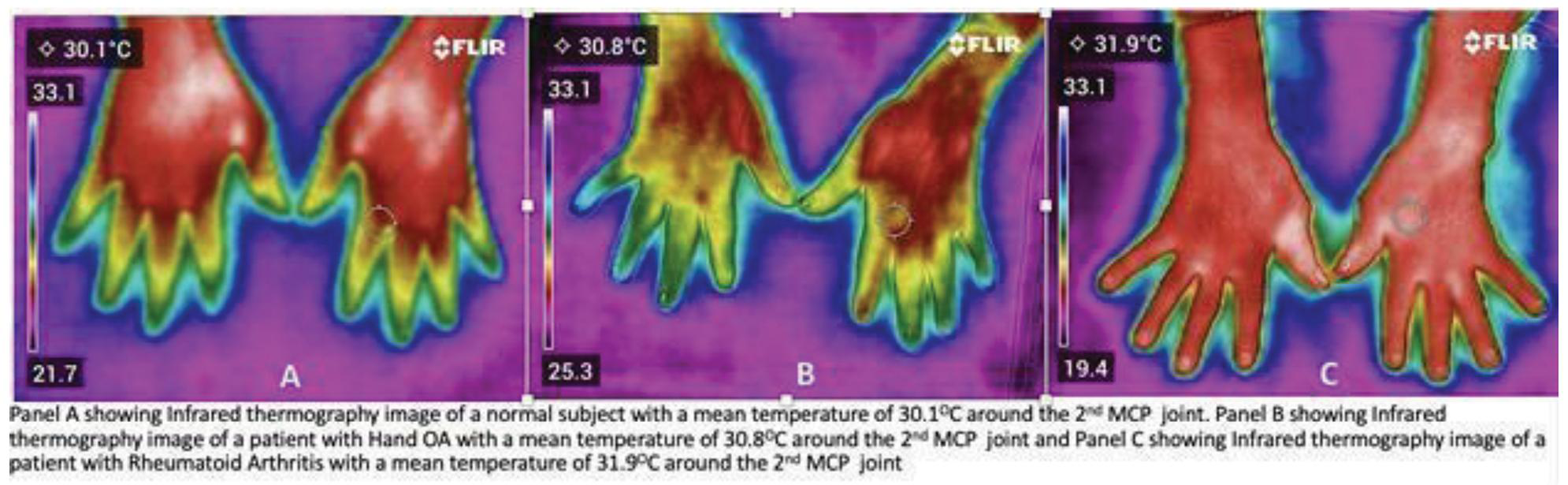
The “I” to look for Inflammation: The Role of Infrared Thermography to Differentiate Hand OA and RA
We also found that the mean temperature (T mean) at the hand joints of Osteoarthritis patients were more than the T mean in normal subjects indicating the possibility of low grade inflammation occurring in patients with Osteoarthritis.
Infrared thermography imaging shows increased temperature in patients with Rheumatoid Arthritis when compared to patients with Hand Osteoarthritis. Infrared thermography could be utilized as a potential tool to discriminate Rheumatoid Arthritis from Hand Osteoarthritis and further larger studies are required to validate these findings.
POS062
The Effect of Oral Nigella Sativa Capsule on Symptoms and Serum Levels of Tenascin C in Knee Osteoarthritis Patients: A Triple-Blind Randomized Clinical Trial
POS063
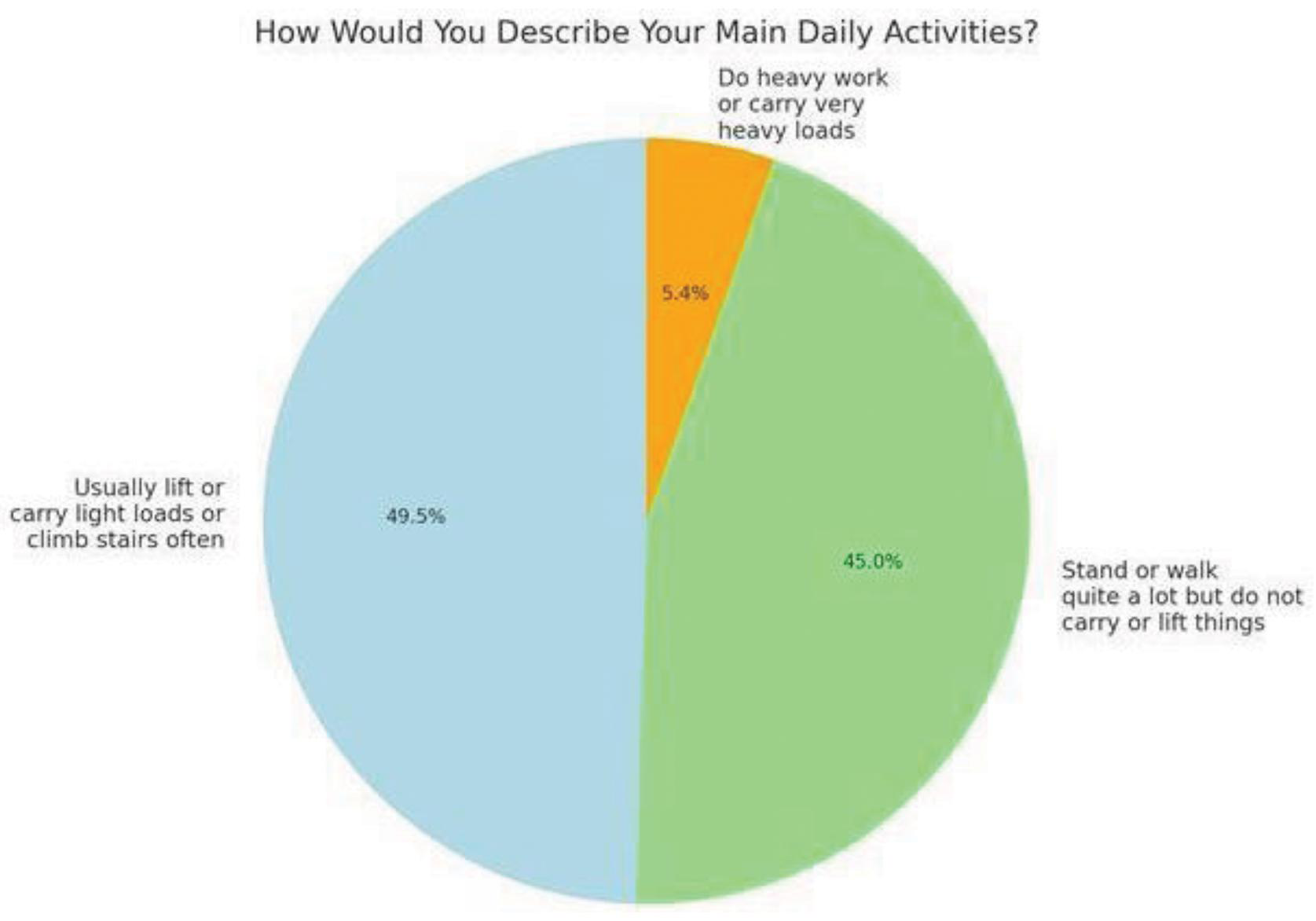
Survey on Dietary Intake, Physical Activity, Occupational Risk, and Other Modifiable Factors Influencing Osteoarthritis Progression in Sri Lanka
Daily physical activity was reported by 88% of participants, yet only 37% had a diet rich in Vitamin D. Occupational heavy lifting was uncommon, with 78% not engaged in such activities. Although higher physical activity was linked to slightly lower pain scores, this association was not statistically significant. Interestingly, participants with a lower BMI (<30) reported significantly fewer functional limitations compared to those with a higher BMI, suggesting that weight management may play a critical role in functional outcomes.
Image and Bar Table 1

Image and Bar Table 2
POS064
An Observational, Immunogenetic, Pilot Study, of Contrasting Forms of Rheumatic Diseases; Coexisting in an Individual Patient or First-Degree Relatives: Identification of the “Overlap Musculoskeletal Disease
Image and Bar Table 1


POS065
First DMARD in Palindromic Rheumatism – A Retrospective Analysis
Image and Bar Table 2

POS066
Introductory Results from the Pregnancy Registry for Indian Women with Autoimmune Diseases (PRIWA) Project - A Single Centre Prospective Pregnancy Registry
Mean (SD) age of enrolled subjects is 26.3 ± 3.9 years. Majority of patients (n=43) already had a diagnosis of rheumatic disease and were on treatment. 11 patients were diagnosed with rheumatic disease in their current pregnancy. Majority women (34/54) had history of at least one previous poor pregnancy outcome (miscarriage/ IUD/ IUGR/ preeclampsia).
Mean gestational age at enrolment was 15.26 ± 8.8 weeks. Till date 18 pregnancies are completed. Mean (SD) period of gestation was 35.7 ± 5.9 weeks. Maternal and foetal outcomes are presented in table 1. Two patients (SLE) had a disease flare during and post pregnancy.
Image and Bar Table 1

POS067
Chikungunya Arthritis: A Systematic Review
MeSH terms used for the search were chikungunya, arthritis, polyarthritis, joints, infection, virus, and management. A total of related 494 articles were found. The search was made concise using PubMed Advanced Search Builder.
1. Rodríguez-Morales AJ, Cardona-Ospina JA, Fernanda Urbano-Garzón S, Sebastian Hurtado-Zapata J. Prevalence of Post-Chikungunya Infection Chronic Inflammatory Arthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res (Hoboken). 2016.
2. Bouquillard E, Combe B. A report of 21 cases of rheumatoid arthritis following Chikungunya fever. A mean follow-up of two years. Joint Bone Spine. 2009.
3. Amaral JK, Bingham CO 3rd, Schoen RT. Successful Methotrexate Treatment of Chronic Chikungunya Arthritis. J Clin Rheumatol. 2020.
4. Manimunda SP, Vijayachari P, Uppoor R, Sugunan AP, Singh SS, Rai SK, Sudeep AB, Muruganandam N, Chaitanya IK, Guruprasad DR. Clinical progression of chikungunya fever during acute and chronic arthritic stages and the changes in joint morphology as revealed by imaging. Trans R Soc Trop Med Hyg. 2010.
Image and Bar Table 1

POS068
Safety and Effectiveness of Intraarticular Injection in Rheumatological Diseases in a Single Centre in Central India
Vivek Kattel1, Neetu Gupta2,
POS069
Challenges Faced by Female Rheumatologists in India: A Survey Based Cross-Sectional Study
Image and Bar Table 1

Image and Bar Table 2

POS070
Vaccination Status, Knowledge, and Acceptance of Adult Vaccinations Among Patients Receiving Immunosuppressive Therapy
Yathish GC,
Assess the vaccination status of patients receiving immunosuppressive therapy. Evaluate their knowledge of recommended adult vaccinations. Investigate the factors influencing their acceptance or hesitancy toward vaccinations. Identify potential barriers to vaccine uptake and suggest strategies for improving vaccination rates.
Image and Bar Table 1

Image and Bar Table 2

POS071
Disease Burden in Inflammatory Arthritis: An Unsupervised Machine Learning Approach of the COVAD-2-E-Survey Dataset
Vincenzo Venerito1, Sergio Prieto González2, Marco Fornaro3, Florenzo lannone4, Lorenzo Cavagna5, Masataka Kuwana6, Vishwesh Agarwal7, Jessica Day8, Mrudula Joshi9, Sreoshy Saha10, Kshitij Jagtap11, Wanruchada Katchamart12, Phonpen Akawatcharangura Goo13, Binit Vaidya14, 15Tsvetelina Velikova, Parikshit Sen16, Samuel Katsuyuki Shinjo17, Ai Lyn Tan18, Nelly Ziade19, Marcin Milchert20, Abraham Edgar Gracia- Ramos21, Carlo Vinicio Caballero- Uribe22, Hector Chinoy23,
To compare disease burden among patients with RA, PsA, and AS using Patient-Reported Outcome Measurement Information System (PROMIS) scores. To identify distinct patient clusters based on comorbidity profiles and PROMIS outcomes.
However, in inactive disease, PROMIS Global Physical Health score was significantly higher in the AS group (13.13 ± 2.95) compared to PsA group (12.43 ± 3.27, p=0.016). PROMIS Global Mental Health scores were similar across all groups. PROMIS Fatigue 4a score was significantly higher in inactive PsA (10.58 ± 4.22) and RA (10.45 ± 4.08) compared to inactive AS (9.4 ± 4.13, p=0.016 for RA, p<0.01 for PsA). PROMIS Physical Function SF10 score was significantly higher in the inactive AS group (41.13 ± 7.39) compared to inactive PsA group (39.27. ± 9.01, p<0.001).
The mean VAS pain scores were significantly lower in the inactive AS group (3.34 ± 2.39) compared to inactive PsA (4.04 ± 2.50, p=0.016) and RA groups (3.87 ± 2.45, p=0.016). Clustering analysis identified four distinct patient clusters: Clusters 2 and 4 had higher comorbidities, frequent depression, and poorer patient-reported outcomes (PROs), whereas Clusters 1 and 3 had less frequent depression and better PROs.
POS072
Adherence to Medication in Patients Diagnosed with Systemic Lupus Erythematosus: Cross-Sectional Study in A Rheumatology Specialized Care Unit, Sri Lanka
1. Feldman, C. H., Yazdany, J., Guan, H., Solomon, D. H., Costenbader, K. H., & Chibnik, L. B. (2017). Medication nonadherence is associated with increased subsequent acute care utilization among Medicaid beneficiaries with systemic lupus erythematosus. Arthritis Care & Research, 69 (11), 1706-1713. doi:10.1002/acr.23195
POS073
A Study of Clinical and Investigative Profile of Patients with Fibromyalgia in A Tertiary Care Centre in Central India
Mean age group of the study population was 47.07±14.062. Fatigue and musculoskeletal pain were seen in all 45 patients.
Majority of patients did not suffer from any co-comorbidities (n=29, 64.4%). Out of the remaining 16 patients, type 2 diabetes mellitus is the most common comorbid illness (n=5, 11.1%).
Out of 45 patients, 3 patients (6.7%) had RF positive and 7 patients (15.6%) are ANA positive and 4 (8.9%) had HLA B27 positive. All 4 HLAB27 scored into severe FIQR category. 14 out of 45 patients (31.1%) scored in-between 64 to 82 landing them in the severe category of FIQR severity group. 10 out of 14 (71.4%) who scored into severe group had secondary fibromyalgia secondary to associated rheumatological conditions. Of this 14 individuals, 8 had a history of single comorbidity whereas 5 had history of 2 or more comorbidity, indicative that people with associated comorbidities have severe disease (p<0.0001). 11 out of the 14 individuals (78.60%) in the severe group were overweight while 2 were obese indicating that patients who are obese (BMI more than equal 30) and overweight (BMI of 25.0-29.9) had severe disease than patients who are normal weight (BMI of 18.5-24.9) had low disease (p<0.0001).
POS074
Profile of Juvenile Systemic Lupus Erythematosus Patients with A Special Reference to Monogenic Lupus and Lupus Nephritis: A Cross-Sectional Study
Image and Bar Table 1

Image and Bar Table 2

POS075
A Study of Monogenic Autoinflammatory Diseases in Southern India: Clinical Features, Genetic Findings, and Therapeutic Responses
Among the 81 patients, 18 patients (22.2%) had Periodic Fever, Aphthous Stomatitis, Pharyngitis, Adenitis (PFAPA) and 36 patients were diagnosed with 14 kinds of monogenic AIDs including 10 patients (28%) with inflammasomopathies, 20 patients (55%) with non-inflammasome related conditions, and 6 patients (17%) with type 1 interferonopathies.
Diseases affecting inflammasomes included NLRP1 associated autoinflammation with arthritis and dyskeratosis (2 patients), FMF (1 patient), Hyper IgD syndrome (1 patient), MWS (2 patients), NOMID (1 patient), Majeed syndrome (3 patients).
Blau syndrome (8 patients), COPA (1 patient), DADA2 (8 patients), H syndrome (2 patients), Sharpin (1 patient) were categorized as non-inflammasome related conditions.
Type1 interferonopathies identified in the cohort included patients with Aicardi-Goutières syndrome (2 patients), TRAPS (1 patient), monogenic lupus (3 patients).
Laboratory findings and treatment strategies varied depending on the specific condition. Corticosteroids and immunosuppressive agents were used as per availability and convenience.
A follow-up of 30 patients over a median duration of 60.5 months revealed, 7 patients (19.4%) showing good response while active disease persisted in 12 patients (33.3%). There were 2 reported deaths (5.5%).
Image and Bar Table 1


POS076
Measuring Disease Activity and Psychological Burden in Juvenile Idiopathic Arthritis: A Prospective Observational Study
During evaluation, 32 patients had active disease activity (Table 1). These patients included 17 patients from SJIA group, 14 patients from ERA group, five patients from Oligoarticular JIA group, one patient each from RF Positive Polyarticular JIA and RF Negative Polyarticular JIA group. Mean delay of diagnosis was maximum in the ERA group while it was least in SJIA group. Highest mean JADAS27 score was recorded in polyarticular JIA group (24), followed by SJIA group (20.9) and ERA group (17.3). Major depressive episode was the predominant psychiatric burden seen in six patients, followed by attention deficit hyperactivity disorder seen in one patient. One patient had severe depression and suicidal ideation. SJIA had a significant association with psychiatric morbidity (Table 2). Mean delay of diagnosis, age at presentation, gender, duration of disease, number of relapses, and disease activity at time of diagnosis did not have any relation to the psychiatric co-morbidity.
Five patients with psychiatric co-morbidity remained under follow up. Three patients with depression improved with psychological counselling, while one patient with severe depression improved after psychiatrist intervention. One patient with ADHD is under follow up.
Image and Bar Table 1

Image and Bar Table 2

POS077
Clinical Profile of Kawasaki Disease–Experience from A Tertiary Care Center in South India
POS078
Study of Clinico-Immunological and Treatment Profile in Children with Non-Renal Manifestation of Systemic Lupus Erythematosus
POS079
Prospective Indian Childhood Lupus Nephritis Registry: Analysis of One Year Data
C Ravali Pratima Goud1,
Image and Bar Table 1

Image and Bar Table 2

POS080
Identifying Predictors of IgA Nephritis in Pediatric IgA Vasculitis: A Retrospective Analysis
Image and Bar Table 1


POS081
Progressive Pseudo Rheumatoid Dysplasia – JIA mimic – Case Series
Image and Bar Table 1

Image and Bar Table 2

POS082
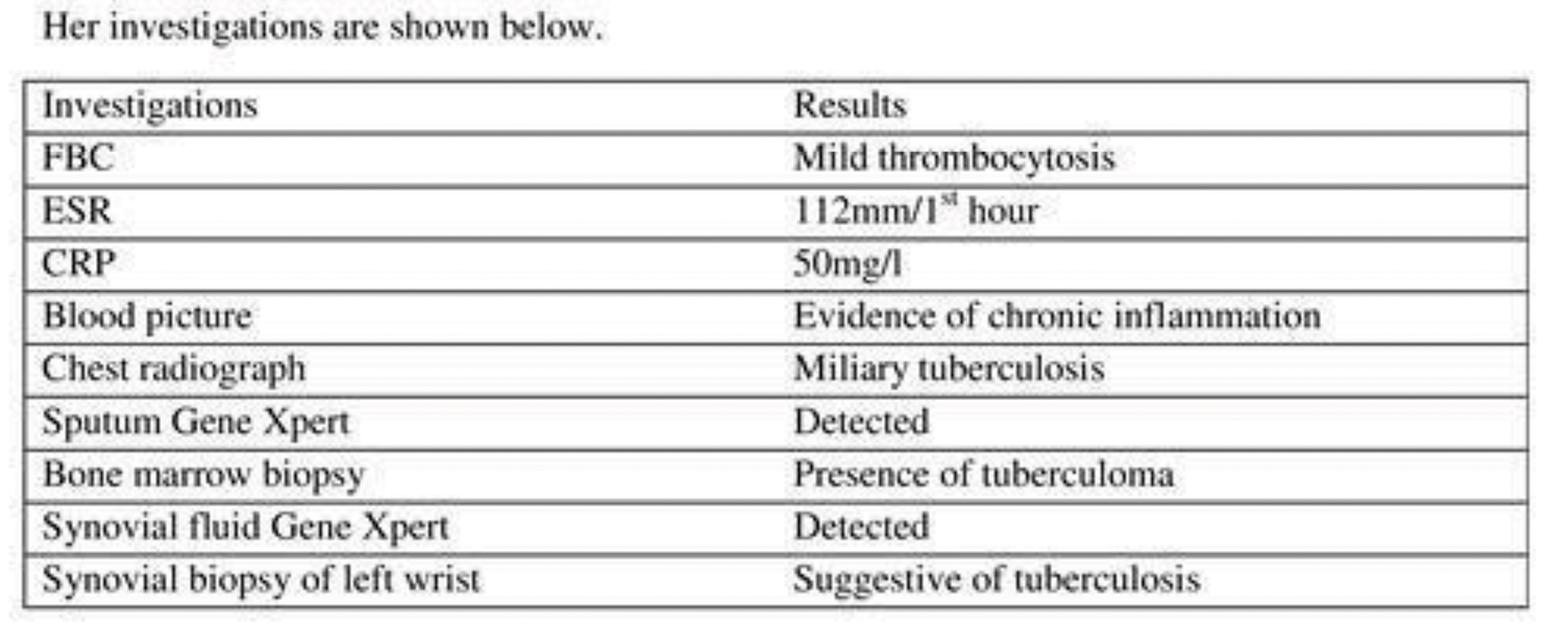
The Eye Openers in Diagnosis: Musculoskeletal Tuberculosis Mimics Juvenile Idiopathic Arthritis in A Child from A Developing Country
Thus the diagnosis of disseminated tuberculosis involving musculoskeletal, pulmonary and hematological system was made and started on category 1 anti-tuberculosis treatment with good clinical response within one month of treatment and being followed up at both pulmonology and rheumatology clinics.
Left wrist showing synovitis

Her investigations are shown below.
POS083
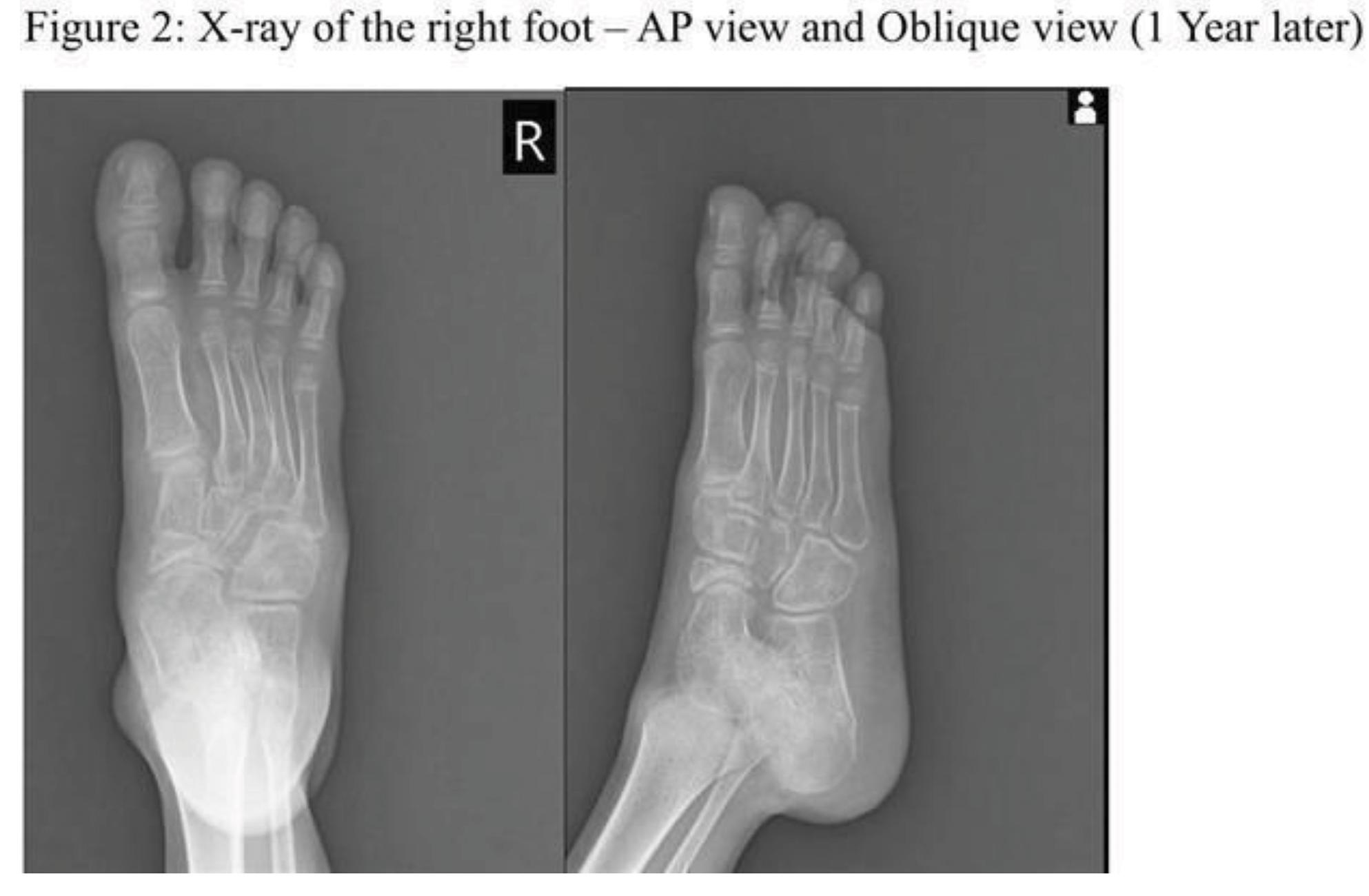
Navigating Navicular Necrosis: Steroid Side Effect in Juvenile Idiopathic Arthritis
Image and Bar Table 1

POS084
Clinico-Demographic Profiles and Treatment Responses in Juvenile Idiopathic Arthritis: A Prospective Study from a South Indian Tertiary Care Center
Polyarticular JIA was the most common subtype, affecting 44.4% (12/27) of patients, followed by ERA at 25.9% (7/27). Methotrexate was the first-line therapy for 81.5% of patients, with 18.5% receiving sulfasalazine. Four patients required escalation to tofacitinib or TNF inhibitors. Rheumatoid factor (RF) was positive in 22.2% of patients, ANA in 29.6%, and HLA-B27 in 14.8%. JADAS scores improved from 31.75 (SD = 14.19) to 14.38 (SD = 6.88) between visits. Nine patients showed worsening JADAS, five due to treatment discontinuation related to medication apprehension and poor disease knowledge.
Image and Bar Table 1

POS085
Whole Exome Sequencing (WES) for Diagnosis of Monogenic Disorders in Children at A Tertiary Level Pediatric Rheumatology Centre: a Tool of Utility or Futility?
Clinical features: Common symptoms identified in these children were undifferentiated arthritis 23 (33%), intermittent fever 22 (31%), and rash 21 (30%).
Differential diagnosis: Autoinflammatory disorders form the major group of suspected diagnoses (57 patients, 81%) followed by Inborn errors of Immunity (3, 4.3%) and JIA mimics (4, 5.7%).
Suspected autoinflammatory disorders included DADA-2, Inflammosomopathies, Blau syndrome, Interferonopathies, Early complement deficiencies, HA-20, PAPA spectrum disorders, and COPA syndrome. Pathogenic gene was identified in 13 (23%) and correlated with phenotype to establish the diagnosis.
PIDs including DOCK-8 deficiency and CVID were suspected in 2 different patients however pathogenic genes could not be detected.
Among JIA mimics, 1 case each of MONA syndrome, H syndrome, CACP syndrome, and MPS-1h was identified using WES.
21 had pathogenic genes identified: Genotype-phenotype correlation was seen in 18 (25.7%). Variants of uncertain significance (VUS) were identified in 22 patients (31.4%). Parental genotyping was done in one case (Trio).
Image and Bar Table 1

POS086
Transcriptome Sequencing Reveals Gene Signatures Implicated in the Pathogenesis of Juvenile Onset Systemic Sclerosis
Heatmap showing expression for top 25 and bottom 25 significantly differentially expressed protein coding genes.

This volcano plot displays the differential gene expression analysis of juvenile systemic sclerosis (jSSc) patients versus healthy controls. Upregulated genes are shown in green and downregulated genes in red based on p-value < 0.05 and fold change ≥ 2 or ≤ –2.

POS087
Autoimmunity and Immune Dysregulation in Inborn Errors of Immunity: Experience from A Tertiary Care Center in South India
Autoimmunity was observed in 120 (25.5%) patients. The ‘autoimmune cohort’ experienced a mean delay in diagnosis of 8.5 years, significantly higher than the rest of the study population (p < 0.002). The most prevalent autoimmune manifestations included inflammatory colitis (n=30), autoimmune cytopenia (n=27), autoimmune endocrinopathy (n=10), and arthritis (n=9). Skin manifestations included pyoderma gangrenosum (n=7), alopecia areata (n=4), vitiligo (n=3), bullous pemphigoid (n=1), dermatitis herpetiformis (n=1), and cutaneous vasculitis (n=1). Others included systemic lupus erythematosus (n=7), Kawasaki disease (n=4), lymphoproliferation (n=15), autoimmune hepatitis (n=3), CNS vasculitis (n=2), systemic vasculitis (n=1), nephritis (n=1), nephrotic syndrome (n=2), oral aphthosis (n=1), sarcoidosis (n=1), and uveitis (n=1).
Patients were treated with various immunomodulatory agents, including steroids (n=40), methotrexate (n=12), colchicine (n=6), cyclosporine (n=3), sirolimus (n=6), mesalamine (n=3), leflunomide (n=2), thalidomide (n=2), tofacitinib (n=2), mycophenolate mofetil (n=3), azathioprine (n=6), and dapsone (n=1). Biologics used were rituximab (n=3), anakinra (n=2), tocilizumab (n=1), adalimumab (n=1), and infliximab (n=1). 38 patients received immunoglobulin replacement therapy. Five patients with C1q deficiency were given fresh frozen plasma infusions.22 underwent Hematopoietic stem cell transplant. The overall survival rate in the ‘autoimmune’ cohort was 89%.
POS088
Profile of Systemic Autoinflammatory Diseases-Experience from A Tertiary Care Center in South India
Treatment included corticosteroids (n=22), NSAIDS (n=12), methotrexate (n=12), colchicine (n=8), leflunomide (n=3), thalidomide (n=2), and cyclosporine (n=1). Eleven patients (TRAPS, Otulin deficiency, DADA2, NOMID, CRMO, SPENCD, Blau syndrome, IL6ST mutation) were treated with biologics (Infliximab n=1, Tocilizumab n=2, Adalimumab n=6, Tofacitinib=2, Baricitinib n=1, Rituximab n=1, Anakinra n=2, Etanercept n=1). Five patients with PFAPA remained well on intermittent steroids, whereas three of them were treated with colchicine. Five CRMO patients were treated with pamidronate, however, one of them failed to respond warranting adalimumab. Refractory uveitis in one patient with Blau syndrome required weekly adalimumab. The child with IL6ST mutation presented with granulomatous sarcoid-like inflammation involving the eyes, lungs, liver, and lymph nodes. He continued to run high fevers that failed to respond to TNF blockers, Rituximab, Tocilizumab, and Jak inhibitors and is currently maintained on weekly adalimumab and low-dose steroids. 34 patients under close follow-up.
Image and Bar Table 1
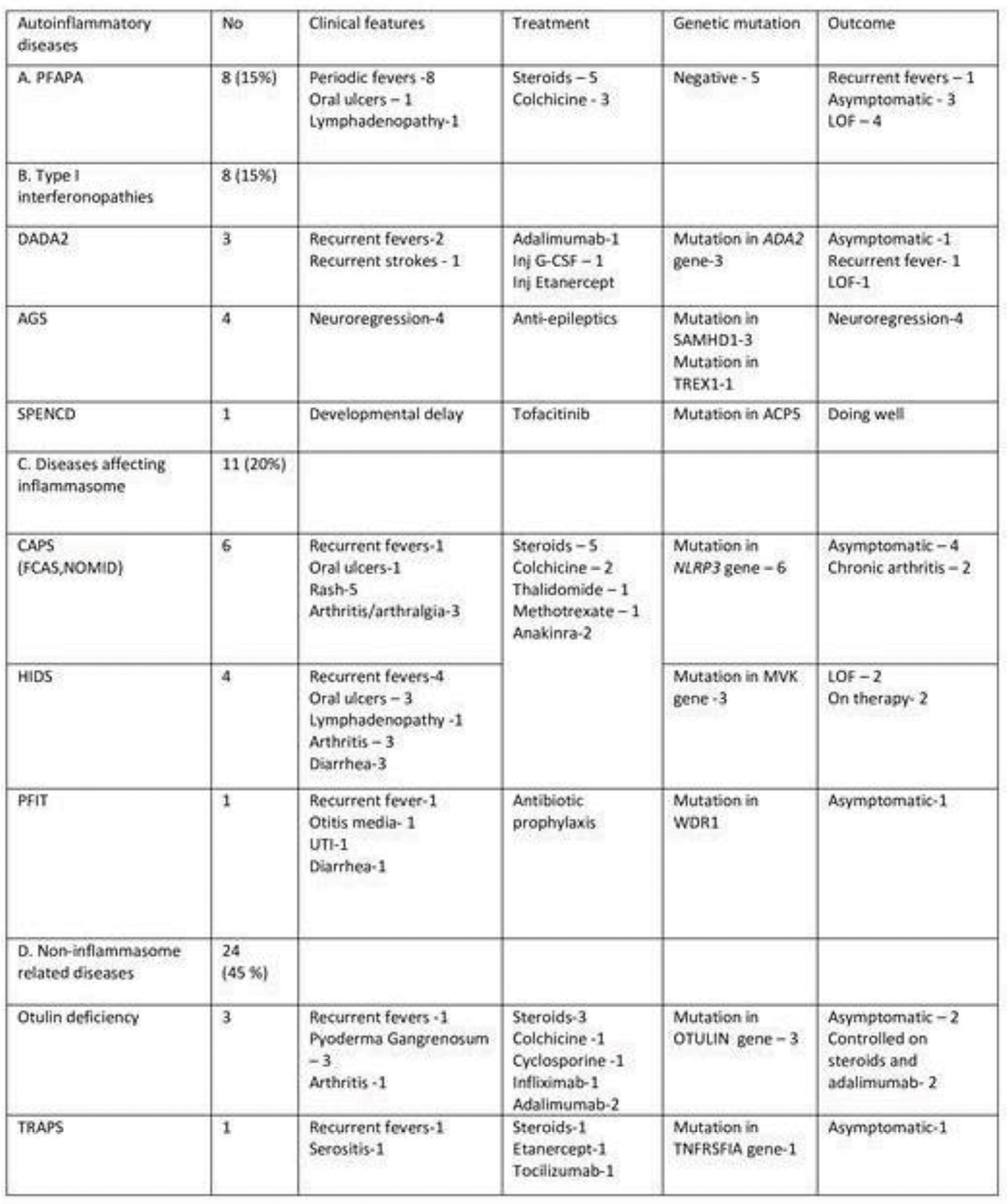
Image and Bar Table 2

POS089
A Tertiary Center Based Retrospective Study on Juvenile Dermatomyositis: Clinical Spectrum, Treatment Response, Complications and Outcome
POS090
Use of Tofacitinib in Juvenile Idiopathic Arthritis: Experience from Two Centres in Eastern India
Study the response to tofacitinib in patients with JIA Document side effects of Tofacitinib in these patients.
Other biological DMARD like anti TNF agents were used in 22% prior to initiation of tofacitinib and in 8% was used concurrently. There was transient transaminitis in 2 patients, Herpes zoster infection in 2 patients and 1 patient experienced increase in serum LDL cholesterol after 3 months, hence tofacitinib was stopped.
POS091
ADA2 Deficiency: Clinical Manifestations and Outcome in Children
Clinical manifestations of children with ADA2 deficiency. Treatment response and outcome of children with ADA2 deficiency.
Image and Bar Table 1

POS092
Changing Epidemiology of Kawasaki Disease: Data from a Tertiary Referral Centre in Eastern India
March 2020 to March 2022: This period was majorly affected by COVID 19. A total of 54 patients were diagnosed as Kawasaki disease this period. 16 (30%) were less than one year of age, 3 (6%) were more than 5 years of age, 27 were males, 10 were incomplete KD (19%), 4 (7%) had intravenous immunoglobulin (IVIG) resistant who received infliximab (IFX) after IVIG. 15 (28%) had CAA none giant.
April 2022 to August 2023: 64 patients were diagnosed as KD, 20 (37%) were less than one year of age, 1 (2%) was more than 5 years of age, 63 were males, 21 were incomplete KD (39%), 6 (11%) had intravenous immunoglobulin (IVIG) resistant who received infliximab (IFX) after IVIG. 23 (43%) had CAA, none giant. One had intraluminal thrombus formation.
POS093
Infection Associated Hyperinflammation: Retrospective Observational Data from a Tertiary Referal Centre in Eastern India
POS094
Juvenile Dermatomyositis Outcome Prediction Using Magnetic Resonance Imaging STIR Sequences
Image and Bar Table 1

Image and Bar Table 2

POS095
ANCA Associated Vasculitis in Children-Experience Over 11 Years in A Tertiary Centre in South India
The M/F ratio was 1:3, the median age was 14, the median disease duration at presentation was age was 7.4 months (range 2-13 months) and the median follow up duration was 12.8 months. Among systemic manifestations arthralgia, fever and weight loss were present in 8, 6 and 5 patients respectively. Respiratory manifestations include lung cavities and infiltrates in 2 each, diffuse alveolar haemorrhage and interstitial lung disease in 1 each. ENT manifestations include sinusitis in 6, CSOM & hearing loss in 2 each, and saddle nose in 1. Cutaneous manifestations were present in 4. Renal manifestations in 2 and periorbital swelling was present in 1. Total white cell count and CRP was elevated in all but one patient each. ESR was elevated in all patients. Proteinuria was present in 1 patient and elevated creatinine with renal failure in 1 patient. C ANCA was positive in all GPA patients P ANCA in renal AAV and was negative in the 2 EGPA patients. Steroids were used in all patients, rituximab in 3, cyclophosphamide in 2 and MMF in 2 patients as induction agents. 1 patient declined treatment. MMF was used as maintenance therapy in 4, Methotrexate in 2 and azathioprine in 1 patient.
POS096
Tracing the Roots of An Autoinflammatory Disease – 15 Members with Blau Syndrome in a Family
Anitha Manoharan1, Sudharshan Sridharan2,
Eight of the family members had proven NOD 2 mutation. All these patients were detected using a next-generation sequencing panel to carry a c. 1000C >T/p. Arg334Trp (R334W) heterozygous variant in the NOD2 gene. The other patients had clinical manifestations of Blau syndrome. Three of the patients had expired.
Methotrexate was used as a first-line agent for the management of uveitis and arthritis. Oral prednisolone was used as bridging agent initially in addition to topical steroids and cycloplegics. Oral methotrexate alone was used in 4 patients (26.6%); Combination of Methotrexate and mycophenolate mofetil in 2 patients (13.3%); oral tofacitinib in 2 patients (13.3%) along with oral methotrexate; and adalimumab in combination with oral methotrexate in one patient (6.6%). There were multiple episodes of recurrences despite immunosuppressive therapies in the majority of patients.
Image and Bar Table 1

POS097
Immune Regulatory Defects: Insights from A Tertiary Care Rheumatology Centre in Northern India
Primary manifestations included fever in 13 patients, hepatosplenomegaly, lymphadenopathy and inflammatory Bowel Disease (IBD) in 7 patients each. Notably, 12 patients experienced at least one infection and 11 had cytopenia, 11 exhibited failure to thrive, 4 had HLH and 2 had interstitial lung disease. Diagnoses varied from Autoimmune Lymphoproliferative Syndrome (ALPS), Immune Dysregulation, Polyendocrinopathy, Enteropathy, X-linked (IPEX) syndrome, SOCS1 haploinsufficiency, to familial Macrophage Activation Syndrome (MAS) (Table 1).
Regarding treatment response, 12 patients received immunosuppression, 4 received chemotherapy according to HLH protocol and 3 patients underwent HSCT. 14 patients positively responded, while 3 succumbed to the illness, and 4 were lost to follow-up.
Image and Bar Table 1

POS098
Nailfold Capillaroscopic Findings in Healthy Children
POS099
Profile of Kawasaki Disease with and Without Coronary Artery Aneurysms: Data from A Tertiary Care Centre in Eastern India
Image and Bar Table 1
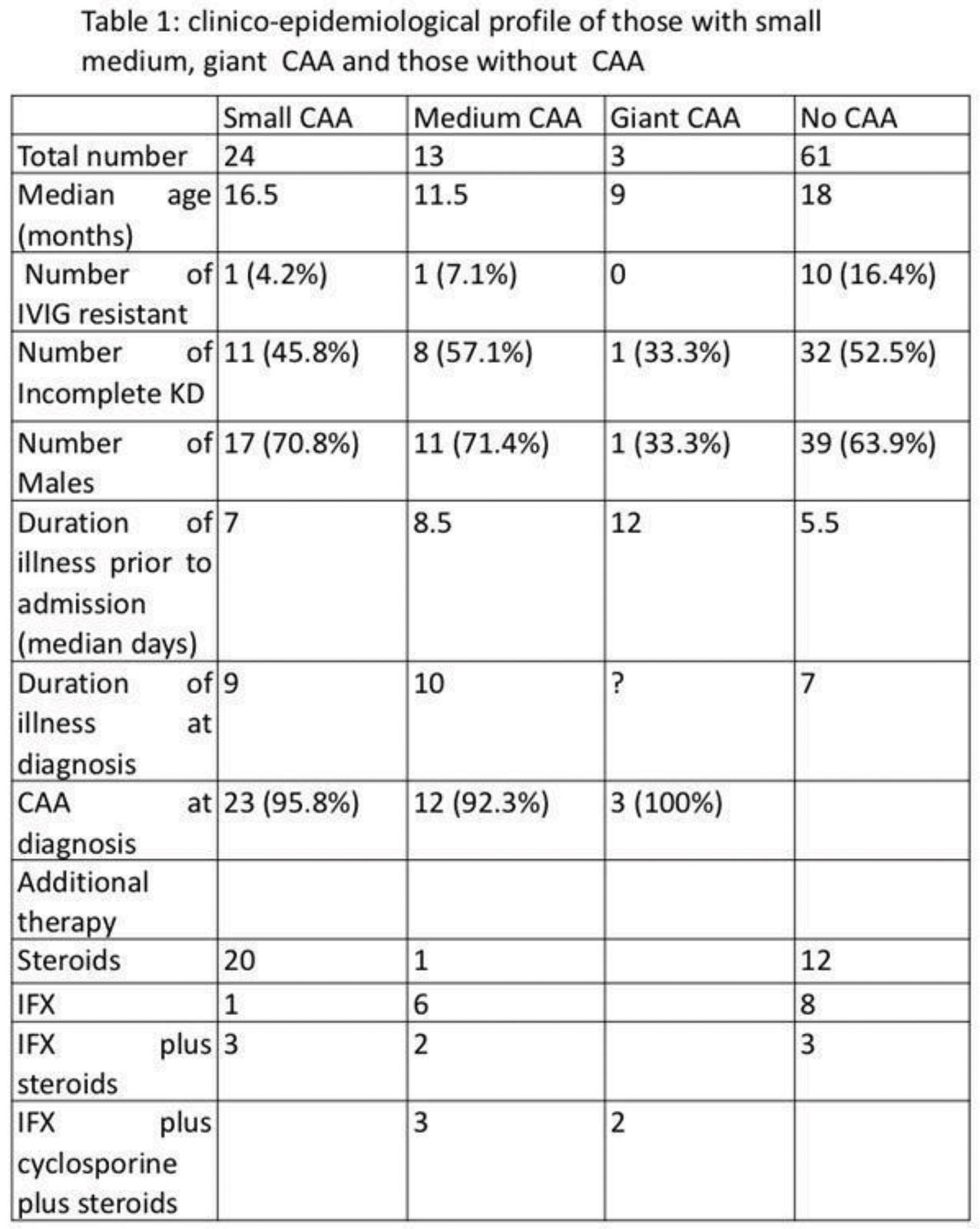
Image and Bar Table 2

POS0100
Association of Single Nucleotide Polymorphisms of TGF-Beta Pathway in North Indian Children with Kawasaki Disease: The First Study from the Indian Subcontinent
Image and Bar Table 1

Image and Bar Table 2

POS101
Use of Infliximab in Infants with Kawasaki Disease
To evaluate the response to IFX in terms of fever defervescence and normalization of inflammatory markers in infants diagnosed with IVIG resistant KD. Evaluate the response to IFX in terms of regression in size of aneurysms, for those with CAA at diagnosis or with increasing CAA following IVIG therapy. Document side effects of IFX in these infants.
12/32 in this cohort received IFX for IVIG resistance, 2 infants had both IVIG resistance and CAA at presentation.
15/32 infants received IFX for CAA at presentation.
All small and 9 medium aneurysms completely regressed on follow up. 3/9 giant aneurysms regressed, 4 reduced to small aneurysms, 1 continues to have persistent giant aneurysm. One infant with giant aneurysm and 1 with medium aneurysm have been lost to follow up. Median time for regression was 3 months.
There were no adverse reactions to IFX.
POS102
Unravelling the Mysteries of Childhood FUO (Fever of unknown origin): A Retrospective Journey Through FDG-PET-CT and MRI at Tertiary Centre in Kerala
The most common diagnoses were lymphoma/leukaemia (31%, n = 7), followed by Langerhans cell histiocytosis (22%, n = 5), large vessel vasculitis (13%, n = 3), and systemic juvenile idiopathic arthritis (5%, n=1). Other diagnoses included Kikuchi lymphadenitis (9%, n = 2), Ewing sarcoma (4%, n=1), ganglioneuroma (4%, n=1), and septic left knee arthritis with coexistent pneumonia (4%, n=1). In one case (4%), the study revealed only reactive lymphadenopathy, with no obvious cause, but the patient recovered uneventfully. All children survived except one, who succumbed to sepsis.
POS103
Spectrum of CHAPLE Disease in Children
POS104
In the Shadows of Symptoms: Decoding a Complex Pediatric Illness
Physical examination revealed dilated abdominal veins, hepatosplenomegaly, and joint swelling. Initial investigations showed iron deficiency anemia (Hb: 10.0 g/dL), elevated ESR (55 mm/hr), and mild transaminitis. Ultrasound confirmed mild hepatosplenomegaly. A bone marrow aspiration ruled out hemophagocytic lymphohistiocytosis (HLH). Rheumatological workup revealed elevated serum complement (C3: 2.231 g/L), ANA positivity with a speckled pattern (2+), and strong Ro60 positivity, suggesting juvenile systemic lupus erythematosus (SLE). The patient was started on glucocorticoids and azathioprine, but difficulties tapering prednisolone prompted a reevaluation.
POS105
Juvenile Idiopathic Arthritis Mimics: A Case Series on Pseudo-Rheumatoid Dysplasia and CACP Syndrome in Pediatric Patients from a Tertiary Center in South India
Image and Bar Table 1

Image and Bar Table 2

POS106
Implications of PD-1/PD-L1 Pathway as a New Immunological Paradigm for Juvenile Idiopathic Arthritis
POS107
Clinico-Pathological Profile of Renal Involvement in IgA Vasculitis in Pediatric Population–A Prospective Study From Tertiary Care Centre in Eastern India
Renal biopsy findings include mesangial hypercellularity in 94%, endocapillary proliferation in 33%, cellular crescents in 33%. Biopsy was consistent with IgAVN in all of them. Initial immunosuppressants used methyl prednisolone low dose 11%, pulse dose 27%, oral prednisolone 50%. DMARDs mycophenolate mofetil was given in 22%. IV single dose cyclophosphamide was given in 33% for GI bleeding manifestations along with nephritis at onset, multiple doses of cyclophosphamide 33% for renal manifestations only. ACEI were given in all of them. Antihypertensives were given in 27%.
POS108
Study on Response to Intraarticular Triamcinolone Hexacetonide in Patients with Juvenile Idiopathic Arthritis: Prospective Observational Study from a Tertiary Care Centre in Eastern India
POS109
Enteric Fever Induced Hemophagocytic Lymphohistocytosis (HLH): A Case Series
POS110
Chronic Recurrent Multifocal Osteomyelitis: Experience from a Tertiary Care Center in Western India
Image and Bar Table 1

Image and Bar Table 2

POS111
Kimura’s Disease: Enigmas and Dilemmas
C Ravali Pratima Goud,
POS112
Unveiling the Enigma: A Challenging diagnostic journey to oculocutaneous sarcoidosis
Image and Bar Table 1

Image and Bar Table 2

POS113
Anca Associated Vasculitis Developing in Pre-Existing Rheumatological Diseases
POS114
Posterior Reversible Encephalopathy in Juvenile Lupus: Case Series of Varied Clinical Presentations
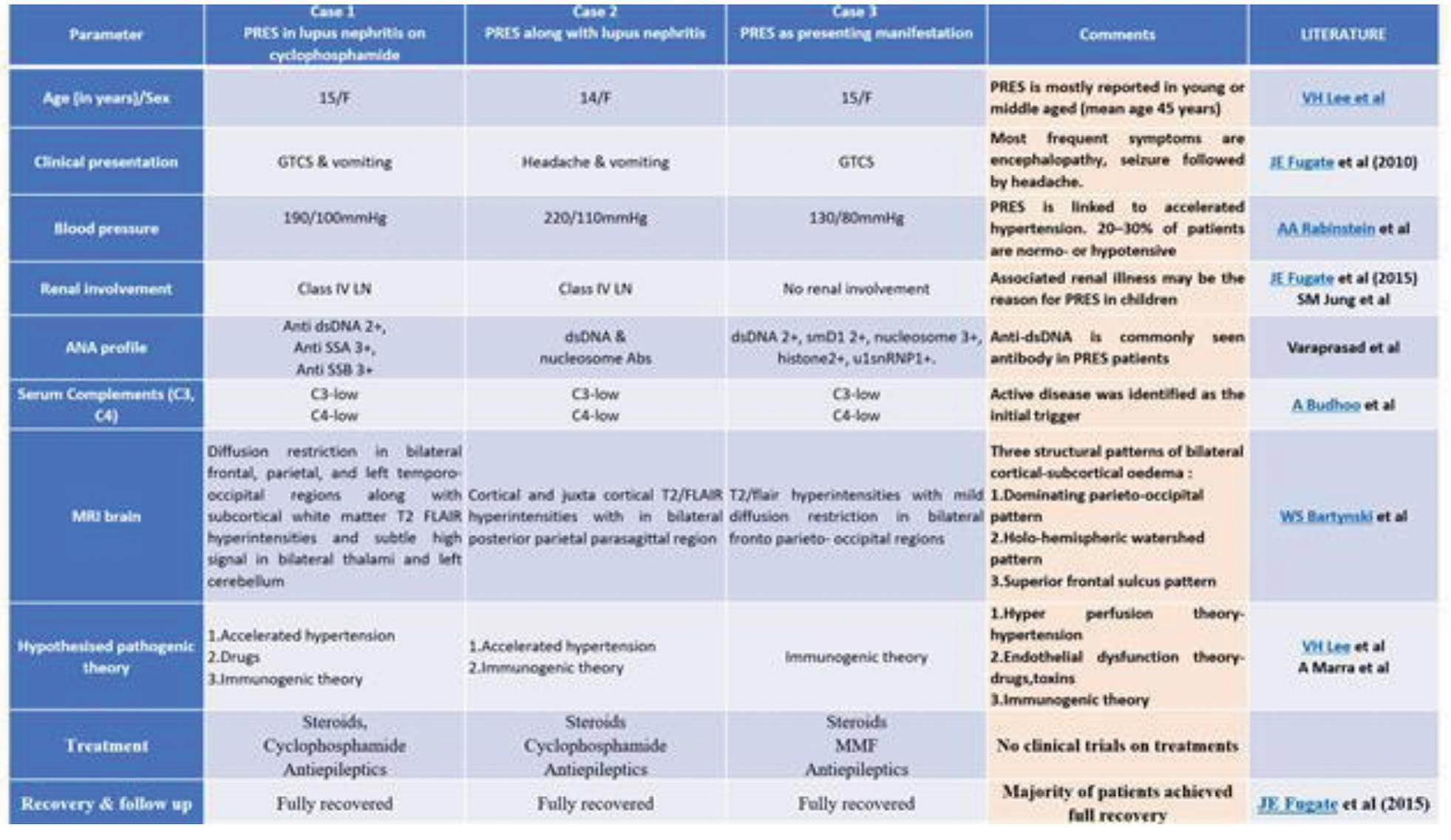
Case 1 - a 15-year-old female with generalized tonic-clonic seizures (GTCS), vomiting, and severe hypertension (190/100 mmHg) in an already diagnosed Class IV lupus nephritis who was on cyclophosphamide induction.
Case 2 was a 14-year-old female with headache, vomiting, and severe hypertension (220/110 mmHg), also associated with concomitant active Class IV lupus nephritis.
Case 3, a 15-year-old female, presented with GTCS and was normotensive (130/80 mmHg), with no renal involvement, marking an isolated PRES presentation which is unique and rare.
All patients had positive anti-dsDNA antibodies as a common autoantibody even though their immunological profiles were different and had low serum complement levels (C3, C4), indicating active disease. MRI findings revealed characteristic patterns of cortical-subcortical edema (figure 1: MRI brain of case 1). Multiple pathogenic theories such as endothelial dysfunction, hyperperfusion, and Immunogenic theories were hypothesized. All patients had a good prognosis.
This study also sheds light on the possible hypothesized pathogenic theories and appropriate treatment protocols and raises the question of whether to consider PRES as a manifestation of NPSLE.
Image and Bar Table 1

Image and Bar Table 2
POS115
From Griscelli Syndrome to Inflammatory Myositis: A Rare Pediatric Case of Multisystem Challenges and Successful Interventions
In 2019, the patient presented with fatigue and vomiting, and tests revealed elevated liver enzymes and hepatitis C infection. He was treated with direct-acting antivirals (DAAT), leading to negative HCV RNA and recovery. After three asymptomatic years, the patient presented in 2024 with muscle weakness, difficulty rising from a seated position, and elevated creatine kinase levels (CK-8233 IU/L). Viral markers and myositis profile were negative. Infectious panels for myositis were negative. MRI showed diffuse hyperintensities in the lower limbs and a muscle biopsy suggested inflammatory myositis. Steroid therapy led to significant improvement, and his creatine kinase levels normalized.
Image and Bar Table 1

Image and Bar Table 2

POS116
Systemic Juvenile Idiopathic Arthritis with Diffuse Alveolar Opacities—A Case Report
In the ED, the child has SpO2-65% (RA) with bilateral crepitations and chest retractions, grade 4 clubbing and mild hepatosplenomegaly. She was shifted to PICU and put on HHFNC. CXR revealed left lung consolidation with bilateral patchy opacities. HRCT thorax showed multiple patchy areas of consolidation, GGO and atelectasis, suggestive of ILD. On day 6 of admission, the child developed high spiking fever with worsening respiratory distress-- diagnosed as MAS, pulsed with MP and then Tofacitinib (JAK inhibitor) was started. The child improved but continued to have around SpO2-80-85% (RA). Again after 10 days the child had another episode of MAS with severe respiratory distress. She was intubated but she expired within 24 hours thereafter.
POS117
MDR TB Myositis Purulanta Tropica
12-year-old girl known case of systemic lupus erythematosus (SLE diagnosed at the age of 4 years with only musculoskeletal and mucocutaneous involvement presented with fever for 7 days. She was on Mycophenolate 1gm/day, Methotrexate and 1mg/kg steroids for 4months. She had high grade fever, headache and swelling at multiple sites.
She had no oral ulcer, rash or joint pain. There was no documented weight loss or recurrent infection.
On examination she had multiple tender fluctuating nodules over fingers, back, face and foot. She had cushingoid features. There was no rash, oral ulcer or tender joints. She had no hepatosplenomegaly.
On investigation she had high CRP and ESR. She had normal dsDNA and complements. Local sonography revealed pyomyositis.
Blood culture and pus cultures were sterile.
Considering possibility of Staph aureus infection oral Linezolid was initiated and steroid converted to stress dose hydrocortisone, Mycophenolate and methotrexate discontinued Hydroxychloroquine was continued, her fever improved ESR, CRP also improved only to recur after 7 days so Pus was drained and Sent for Gram staining, routine culture, AFB smear, GeneXpert and MGIT culture. Her GeneXpert s/o Mycobacterium Tuberculosis detected high with Rifampicin resistance detected. Pt was started on Bedaquiline based regimen including linezolid, levofloxacin, Clofazimine and Cycloserine. Child was symptomatically better. She was on deflazacort 3mg once daily and hydroxychloroquine for SLE.
She was evaluated for primary immunodeficiency (PID). Her DHR, NBT, lymphocytic subset analysis and serum immunoglobulins were normal. Whole exome sequencing did not reveal any genes associated with PID however it detected SPINK1 variant associated with SLE.
She was in regular follow up and developed rash, oral ulcer and alopecia after stopping bedaquiline. There was no fever, nodules or joint pain. SLEDAI was 6. she was Initiated on methotrexate. Steroids were increased to deflazacort 12mg twice daily (1mg/kg).
Improvement was not satisfactory and on tapering steroids there was recurrence along with transaminitis. IVIG was given 1mg/kg. symptoms slowly improved she had one UTI episode with candida growth in culture. At present asymptomatic on deflazacort 6mg per day, hydroxychloroquine. There are still some unsolved issues such as short stature and delayed puberty. Can we use growth hormone in this patients is an unexplored area. MDR TB Pyomyositis in juvenile SLE is a very rare presentation. There is no reported case of MDR TB Pyomyositis. Early diagnosis can decrease morbidity and mortality in these patients.
Image and Bar Table 1

POS118
Early-Onset JIA with Unique LACC1 Gene Mutation: Case Report
Image and Bar Table 1

Image and Bar Table 2

POS119
Vasculitis/Vasculopathy or Both?
We present a case of ELN (Elastin) mutation-associated aortic, cardiac, intracranial and pulmonary vasculopathies associated with suspected vasculitis, which is an unusual combination.
He presented with recurrent fever for 6 months, significant weight loss, with a background history of dyspnea, cough and recurrent epistaxis for 5 years. Despite thorough infection screening and antibiotic courses, his symptoms did not abate, with persistently high inflammatory markers.
IL-6: 42.9 pg/mL (<7).
PET/CT (Figure 1): Wall thickening with focal FDG uptake in left common carotid and ascending aorta; Non FDG avid diffuse wall thickening and narrowing of arch, descending aorta, Pseudoaneurysms across tibioperoneal vessels, ostial narrowing of pulmonary arteries.
He was started on Mycophenolate Mofetil and steroids, with temporary relief, but developed progressive headache and seizures. Brain imaging revealed SAH secondary to MCA aneurysm and ICA narrowing with vasculitic features. Hence, started on IV Tocilizumab. There was a significant improvement in headache, and decreased levels of CRP (28 mg/dL).
However, after his 3rd dose of Tocilizumab, he succumbed to a massive intracranial hemorrhage, despite surgical intervention.
Image and Bar Table 1

Image and Bar Table 2

POS120
A Case of PAAND (Pyrin Associated Autoinflammation with Neutrophilic Dermatosis) with Nephritis – First Reported Case from India
We present a 7-year-old girl from West Bengal with history of persistent papular urticaria like skin lesions from infancy[picture] and treated with multiple short courses of immunosuppressants for Chronic recurrent multifocal osteomyelitis which was diagnosed at the age of 3 years, came to the emergency department with hematuria of 1 week duration which progressed to Acute kidney injury [AKI] and hypertension. After ruling out initial suspects like PSGN, and SLE with appropriate blood workups, renal and skin biopsy was done. She needed 6 days of hemodialysis and renal function improved. She had evidence of persistent glomerulonephritis with associated hypertension and this required prolonged inpatient management. In search of a diagnosis linking early onset skin, joint and kidney disease, a whole genome exome sequence was done and that revealed heterozygous mutation of pyrin-associated autoinflammation with neutrophilic dermatosis. She was started on corticosteroids after pulse therapy. Considering the genetic diagnosis, she was started on Adalimumab which was initially given every 15 days while simultaneously reducing the dose of steroid. Six months into treatment she has no relapse of skin or joint issues and proteinuria and haematuria resolved. Her Adalimumab dose has been spaced out to three weeks and she is on 2.5mg alternate day of oral prednisolone.
Image and Bar Table 1
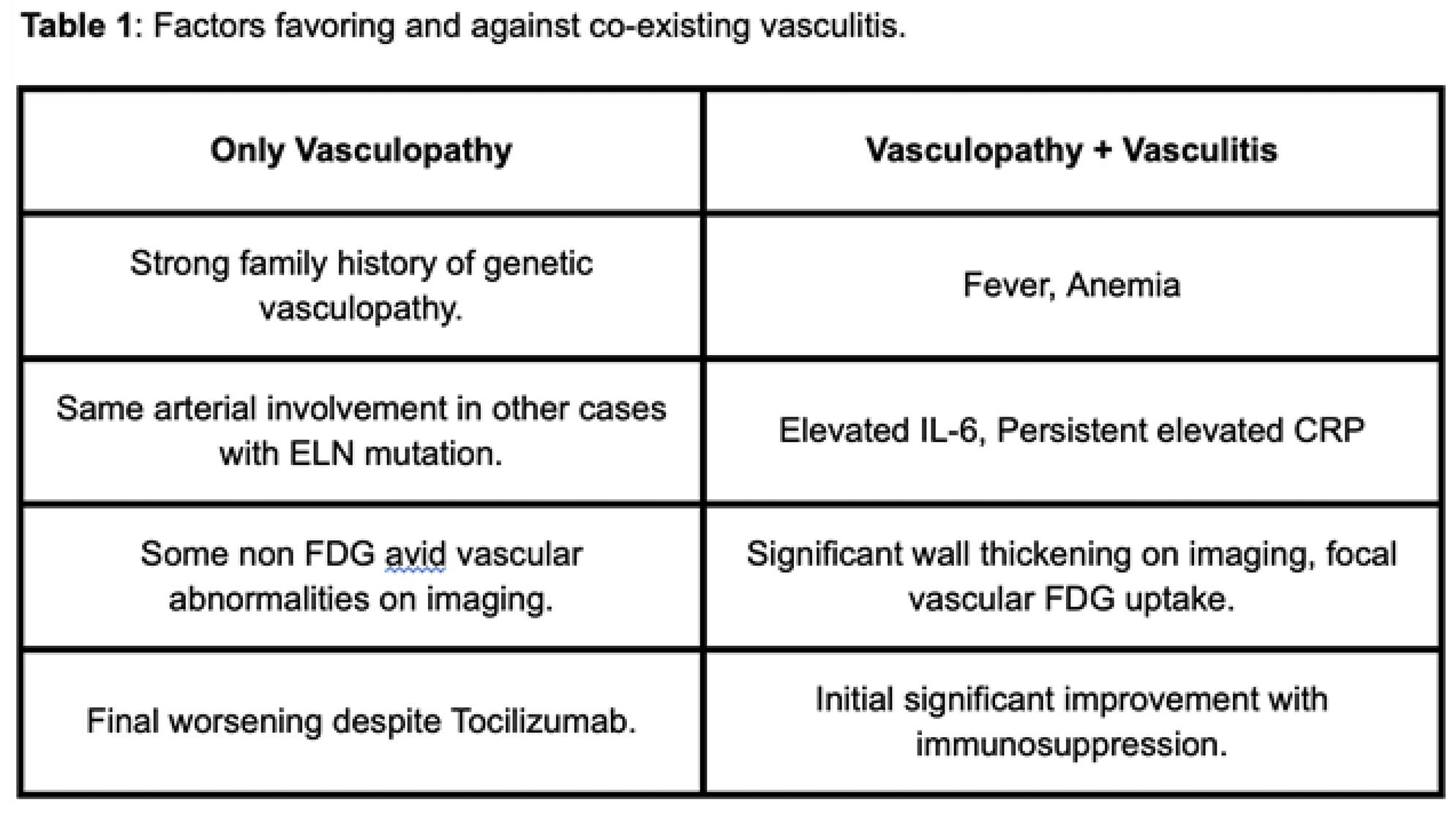
Image and Bar Table 2

POS121
X-Linked Agammaglobulinemia Presenting as Inflammatory Arthritis
Image and Bar Table 1

Image and Bar Table 2

POS122
Peripheral Gangrene in Kawasaki Disease: A Clinical Conundrum
POS123
Covid Associated Interstitial Pneumonitis with Autoimmune Features: Clinicaland Immunoradiological Features from South India
1. Fischer A, Antoniou KM, Brown KK, et al.: An official European Respiratory Society/American Thoracic Society research statement: interstitial pneumonia with autoimmune features. Eur Respire J. 2015, 46:976-87. 10.1183/13993003.00150-2015
2. American Thoracic Society, European Respiratory Society: American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2002, 165:277-304. 10.1164/ajrccm.
3. Cottin V. Interstitial lung disease: are we missing forme frustes of connective Tissue disease? Eur Respir J. (2006) 28:893–6. Doi: 10.1183/09031936.00101506
POS124
Unmasking the Invisible: A Compelling Series of Cases on Antiphospholipid Syndrome Emphasizing Diagnostic Vigilance
POS125
A Rare Manifestation of Apla Syndrome
Cerebral vein thrombosis is a rare form of cerebrovascular accident and an uncommon APS manifestation. Signs and symptomps rely upon the location of the thrombus, clinical manifestations includes headache (90%). followed by focal deficit, altered mental status, nausea, vomiting, seizure.
Image and Bar Table 1

Image and Bar Table 2

POS126
A Case of Spontaneous Vertebral Artery Dissection in a Young Male with Primary Antiphospholipid Antibody Syndrome
A Case of Spontaneous Vertebral artery dissection in a young male with Primary Antiphospholipid antibody syndrome.
Antiphospholipid antibody syndrome (APS) is an autoimmune disorder commonly associated with recurring thrombosis, obstetric complications, and non-thrombotic manifestations. It is characterized by persistently elevated antiphospholipid antibodies (aPL) and is often linked with systemic lupus erythematosus (SLE), where lupus anticoagulant (LAC) is a significant predictor of thrombotic risk. Though a few APS-related arterial dissections are documented, almost all cases were females. This report details a rare case of a 46-year-old male presenting with vertebral artery dissection, cerebellar stroke, and persistently elevated LAC titers.
A 46-year-old male with a history of dyslipidemia and testicular cancer presented with dizziness, nausea, neck pain, and headache after jujitsu training. Neurological examination revealed horizontal nystagmus, left upper extremity ataxia, and cervical tenderness. CT-angiography showed a right vertebral artery dissection extending from the V1 segment with varying patency and a distal segment occlusion. MRI indicated a moderate infarct in the medial right cerebellum.
He was promptly started on dual-antiplatelet therapy (aspirin and clopidogrel). Initial thrombophilia workup, including antiphospholipid antibodies, identified elevated LAC titers, confirmed by repeated testing after 12 weeks. APS was subsequently diagnosed.
This case represents an unusual presentation of isolated LAC-positive primary APS with vertebral artery dissection in a male patient. Cervical artery dissection, though rare (approximately 2.6 cases per 100,000), accounts for a significant percentage of ischemic strokes in younger populations. The exact pathogenesis of arterial dissection remains unclear, but LAC is known to promote a prothrombotic state by impairing endothelial function and enhancing coagulation. The dissection in this patient is hypothesized to result from thrombosis of the vasa vasorum, leading to medial necrosis and subsequent arterial dissection.
Both MR angiography (MRA) and CT angiography (CTA) are effective for diagnosing cervical arterial dissection, with CTA showing higher sensitivity for vertebral dissection. Treatment options include mechanical thrombectomy, thrombolysis, and anticoagulation. While dual- antiplatelet therapy has been shown to be effective, warfarin remains the standard for APS due to its superior efficacy in preventing arterial thrombosis. This case underscores the need for continued vigilance and individualized treatment strategies in APS patients presenting with unusual thrombotic events.
POS127
Double Climax in a Case of Recurrent CVA-Intersection between Autoimmunity and Infection
POS128
What Caused The Gangrene? Ionotrope or Antibody
He was then referred to our hospital with blackish discoloration and dried skin over distal ends of multiple digits of all the 4 limbs.
The painful digital gangrenes developed over a week. Radial and dorsalis pedis artery pulsations were present. CT Angiography detected smooth tapering with short segment luminal narrowing involving bilateral subclavian arteries, at the costoclavicular space.
The prothrombin time was 15.4 sec, activated partial thromboplastin time was 29.3 sec, INR was 1.16. Further laboratory investigations revealed a positive Lupus Anticoagulant with Dilute Russel’s Viper Venom Time (DRVVT) of 75 sec (reference range: 31-42 sec). Anti-Cardiolipin IgM Antibody was reactive. Other vasculitis disorders were excluded (ANCA was nonreactive). ANA was nonreactive and serum C3, C4 levels were normal. A diagnosis of Anti Phospholipid Antibody Syndrome was made.
Management was started with Alprostadil, Aspirin, Unfractionated heparin.
Anti Phospholipid Antibody syndrome is an autoantibody mediated thrombophilia with characteristic recurrent arterial and venous thrombosis.
Septic shock with disseminated intravascular coagulation (DIC) can cause peripheral gangrenes by coagulation activation that is not balanced by the physiological anticoagulant system. Ionotrope administration can further aggravate the situation by causing distal vasoconstriction.
Image and Bar Table 1

Image and Bar Table 2

POS129
Vasculitis in Antiphospholipid Syndrome: A Cause of Ischemia and Monomelic Neuropathy Responding to Corticosteroids
Vasculitis associated with APS has been linked to necrotizing inflammation within blood vessels, leading to the destruction of vessel walls and subsequent ischemic injury in affected tissues. Neuropathy, particularly mononeuritis multiplex, can occur due to ischemia of the vasa nervorum, reflecting the systemic effects of vasculitis on peripheral nerves. The other cause would be the direct ischaemia due to thrombus occlusion, called monomelic neuropathy which is rare.
We report a case of a 51-year-old female with a history of primary subfertility and previous miscarriages, who presented with acute limb ischemia and monomelic neuropathy.
Nerve conduction study revealed mononeuritis multiplex. ANA and ANCA were negative.
POS130
An Unusual Presentation of Late Onset Systemic Lupus Erythematosus Case Presented with Life Threatening Mononeuritis Multiplex due to Lupus Related Vasculitis (Biopsy Proven) and Complicated by Antiphospholipid Antibody Syndrome Resulting in Multiple Cerebral Infarcts
We present an 70 years female with mononeuritis multiplex due to SLE complicated by APS.
Over the next month, she progressively worsened with severe distal upper and lower extremity weakness, pain, paresthesias and gait instability.
Nerve conduction and electromyography showed evidence of vasculitic neuropathy and sural nerve biopsy showed features consistent with a diagnosis of vasculitis.
She was treated with methyl-prednisolone and pulsed cyclophosphamide as per Euro-Lupus regimen.
Patient developed steroid induced psychosis after 3rd cycle as she developed confusion and hallucinations and hence steroids were rapidly reduced over 3 days following which patient deteriorated and became stuperus with GCS of 8/15, needed ITU admission. CSF studies ruled out viral meningitis or encephalitis and MRI brain was done to rule out any lupus neuritis or stroke.
MRI head, showed multiple cerebral and cerebellar infarcts. 2-D echocardiogram ruled out any Libmann Sack’s endocarditis and CT thorax and CT aortogram ruled out any atherosclerotic disease as a source of emboli.
She had positive lupus anticoagulant and Beta2 glycoprotein antibodies positive and anti-cardiolipin antibody was negative. She was started on warfarin following her MRI scan.
She gradually improved with continued cyclophosphamide and oral prednisolone and anticoagulation and was discharged from hospital following her cyclophosphamide 6th cycle.
Taking mycophenolate mofetil 1.5 gm daily and prednisolone 5mg daily.
1. Late-onset systemic lupus erythematosus: a personal series of 47 patients and pooled analysis of 714 cases in the literature, Jacques Boddaert et al. Piette, Medicine (Baltimore), 2004 Nov;83 (6):348-359. doi: 10.1097/01.md.0000147737.57861.7c
POS131
Acute Budd-Chiari Syndrome In Catastrophic Apla
CT pulmonary angiography showed embolism in right trunk of main Pulmonary artery. Patient was started on heparin infusion adjusted according to aPTT. she also had 2 spontaneous abortions in third trimester. APLA profile showed presence of Lupus anticoagulant, IgG Anti cardiolipin, IgG Anti-β2 glycoprotein. ANA was negative. Color Doppler of bilateral lower limb revealed distal DVT in both the limbs. CDHPVS showed occlusion of left and middle hepatic veins.
Final diagnosis of Probable Catastrophic APLA (Pulmonary embolism + lower limb DVT + acute Budd-chiari syndrome + renal failure+ livedo reticularis.
Therapeutic anticoagulation was continued long with steroid and aspirin. Patient underwent 2 sessions of plasmapheresis after which AKI resolved and abdominal distension and lower limb swelling was decreased. She was discharged on Warfarin (target INR 2.5-3.5) Prednisone and Aspirin.
After 6 weeks, repeat CTPA and Color Doppler of lower limb showed resolution of thrombus. However CDHPVS showed paucity of blood flow in hepatic veins and ascites. PT-INR was 18/3.2. Fibroscan showed no fibrosis. She was planned for hepatic vein angioplasty. Warfarin was switched to LMWH before procedure, and she underwent hepatic vein angioplasty. After 12 weeks APLA profile h showed presence of antibodies which confirms the diagnosis of APLA syndrome. On follow up Ascites has resolved.
POS132
Cardiac CAT-in SLE/APLA – Successful Pregnancy Outcome-Post Surgery
She had a past history of abortion at the 6th month due to absent fetal heart rate at which point her routine ECHO showed atrial mass or thrombus. Her APLA and SLE were in remission. She was on anticoagulation too. After intense discussion, she was Anticoagulanted for 6 months, however no resolution of mass. Hence, she underwent cardiac surgery - (median sternotomy) was done on 25/11/22. Biopsy features suggested the possibility of calcified amorphous tumor. (CAT)
But there were lot of discussions during the 10 months of confinement with pimary care nurses, district OG team, National health mission team, Obstetric team, Cardiothroacic surgeons and of course family too.
1. Choi EK, Ro JY, Ayala AG. Calcified amorphous tumor of the heart: case report and review of the literature. Methodist Debakey Cardiovasc J. 2014 Jan-Mar;10 (1):38-40. doi: 10.14797/mdcj-10-1-38. PMID: 24932362; PMCID: PMC4051333.
Image and Bar Table 1

POS133
Early Onset Systemic Lupus Erythematosus: A Case Series of Five Patients with C1Q Deficiency from a Tertiary Care Center in South India
Image and Bar Table 1

Image and Bar Table 2

POS134
Different Attires of APS
Her medical history was significant for coronary artery disease (CAD) with a previous non-ST elevation myocardial infarction (NSTEMI), and hypothalamic-pituitary-adrenal axis suppression secondary to long-term steroid use. APS had been diagnosed 10 years earlier, confirmed by persistently elevated levels of beta-2 glycoprotein and anti-cardiolipin antibodies. She had been closely followed up for immune thrombocytopenia, although she had not experienced any major thrombotic events in the past.
The patient was managed initially with intravenous fluids, antibiotics, and dialysis for acute kidney injury (AKI). However, despite multiple hemodialysis sessions, her renal function did not improve. Renal biopsy was performed, revealing findings of thrombotic microangiopathy with mesangiolysis, fibrin thrombi formation within the glomerular capillaries, and focal fibrinoid necrosis. These findings were consistent with APS nephropathy, a rare but serious complication of APS leading to acute kidney injury.
The patient was started on plasma exchange to reduce circulating antiphospholipid antibodies and received intravenous pulse methylprednisolone to control inflammation. Due to persistent anuria, she was also initiated on hemodialysis. Over ten sessions of plasma exchange combined with dialysis, the patient’s renal function gradually improved, with her creatinine levels decreasing to 6.6 mg/dL at discharge. Long-term warfarin therapy was prescribed to prevent further thrombotic events.
POS135
TRIAD: Trisomy 8 Associated Autoinflammatory Disease– MDS with Behcet Like Disease
POS136
IgG4 related Renal Pseudotumour Mimicking Renal Cell Carcinoma - A Rare Presentation
Immunoglobulin G4-related disease (IgG4-RD) is a systemic condition characterized by unique clinical, serologic and pathologic features.
Tubulointerstitial nephritis is the most common renal manifestation. Renal mass-like lesions is a very rare presentation, which often pose a diagnostic challenge, since they mimic malignancy. We report one such rare case.
A 75-year-old male presented with history of pedal edema, ascites, weight loss of 15kg over 4months and left foot drop.
Serum creatinine was normal. Blood count was normal except eosinophilia (30%).
Abdominal ultrasound showed a hyperechoic Right renal mass. CT scan revealed a Right renal pelvic mass encasing the collecting system and renal vessels, and multiple enlarged abdominal and inguinal lymphnodes (Fig.1) PET scan showed uptake in right kidney and lymphnodes.
Bone marrow done for eosinophilia showed cellular marrow with increased plasma cells (21%), eosinophils and no light chain restriction.
Serum IgE was high (2711mg/dl). In situ hybridization for hypereosinophila and myeloma panel were negative.
Serum IgG (3120mg/dl) and IgG4 (3050mg/dl) levels were very high. Immunofixation electrophoresis was suggestive of IgG kappa monoclonal gammopathy.
Renal mass biopsy revealed lymphoplasmocytic infiltrate with intervening stroma showing storiform fibrosis without evidence of malignancy. Lymphnode biopsy showed sheets of histiocytes and numerous mature plasma cells with patchy fibroblastic proliferation.
IHC demonstrated positivity for IgG4 in plasma cells within kidney (>50/HPF), lymphnode (90-100/HPF) and BM (10-15/HPF). The IgG/IgG4 ratio was 40-50.
Nerve conduction study showed sensory and motor axonal neuropathy involving both lower limb and ulnar nerves.
The concordance of all these findings led to the final diagnosis of IgG4-related Renal inflammatory pseudotumor with Bone marrow and lymphnode involvement with mononeuritis multiplex. He was treated with oral prednisolone 1mg/kg/day, later tapered and also given Inj. Rituximab (2g total).
At 3months, serum IgG4 decreased to 350mg/dl. CT scan showed reduction in size of renal mass and lymphnode (Fig 2A).
A repeat CT scan at 6months showed near complete resolution of renal mass (Fig 2B) with IgG4 of 383mg/dl. Right foot power recovered to normal.
He is planned for maintenance Rituximab.
Image and Bar Table 1
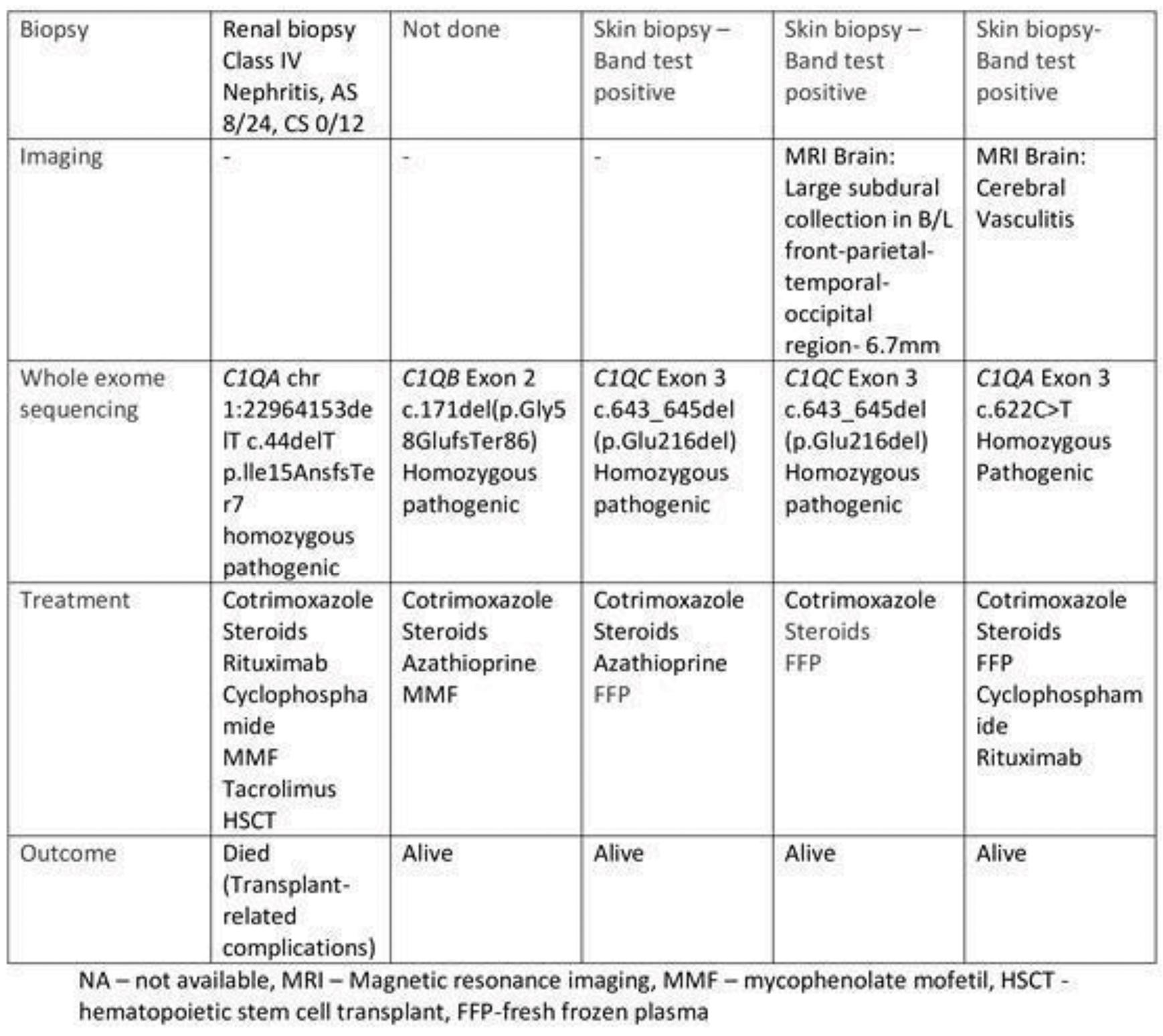
Image and Bar Table 2


POS137
Hemophagocytic Lymphohistiocytosis (HLH) in Interstitial Lung Disease (ILD): Insights from Two Compelling Cases
While Epstein-Barr virus (EBV) is a common trigger of HLH, determining the exact etiology is often challenging. These case reports underscore the importance of considering HLH in ILD patients presenting with unexplained haematological abnormalities and worsening respiratory symptoms.
POS138
Recurrent Infections and Autoimmunity in A Primary Immune Regulatory Defect
Lekshmi Minikumari Rahulan,
Five months later, she developed acute gastroenteritis, painful esophageal ulcerations, dehydration, and acute kidney injury (creatinine 2.3 mg/dL, 24-hour UPCR 387 mg/220 mg, creatinine clearance 22 ml/min). She also had extensive oral candidiasis. She improved with hydration, fluconazole and intravenous acyclovir. CMV PCR came positive with a viral load of 215,000 copies/ml. During her hospital stay, she developed severe abdominal pain, and imaging showed acalculous cholecystitis and bladder wall edema. She improved with valganciclovir and 1 mg/kg prednisolone.
A month later, she developed abdominal pain and new-onset bilateral iliac vein thrombosis, likely related to CMV. Valganciclovir was continued for another month, with subsequent resolution of pain and thrombus. Renal biopsy showed class III+V lupus nephritis with mesangial proliferation and a full house immunofluorescence pattern. Her IgG was 1760 mg/dl, IgA 251 mg/dl, IgM 85.2 mg/dl, with CD4/CD8 reversal, increased TEMRA cells in the CD8 compartment (41%), increased naïve cells in the CD4 compartment (32%), and αβ double-negative T cells (3.53%). Once CMV DNA was not detectable she was started on mycophenolate along with 1mg/kg/day prednisolone for lupus nephritis and has good response.
A regulatory defect was suspected, and whole exome sequencing revealed a heterozygous IKZF1 c.427 C>T p.Arg143Trp (autosomal dominant) partial dominant negative mutation. As she is an adopted child, parental genetic analysis was not feasible. She is currently planned for hematopoietic stem cell transplantation (HSCT).
This mutation causes a defect in the zinc finger 2 in the N-terminal DNA binding domain of IKAROS and results in a partial dominant negative phenotype due to inability of IKAROS to bind to the pericentromeric DNA as it usually would. HSCT is currently considered as the best possible treatment for this condition.
POS139
Unraveling Schnitzler Syndrome: Diagnostic Challenges and Treatment Insights
1. Srivatsav V, Milne A, Hofeld K, Abbas M. Case Report on the Rare Diagnosis of Schnitzler’s Syndrome Lipsker D. The Schnitzler syndrome. Vol. 5, Orphanet Journal of Rare Diseases.2010
Image and Bar Table 1

Image and Bar Table 2

POS140
The Double Jeopardy of Autoimmunity: Lupus-Dermatomyositis presenting as Macrophage Activation Syndrome
Image and Bar Table 2

POS141
Navigating Treatment Resistance in Relapsing Polychondritis
In view of macrocytic anemia, possibility of MDS/ VEXAS syndrome (MDS+RP) was considered; hence bone marrow biopsy and UBA1 mutation was done which were negative. Initial treatment with steroids and methotrexate (MTX) showed decreasing trend in inflammatory markers but the patient experienced worsening symptoms, including new-onset scleritis and polyarthritis, especially upon tapering steroids, which led to the addition of mycophenolate mofetil (MMF).
In view of recurrent relapses and development of new-onset sensorineural hearing loss (SNHL) he was considered for escalation of immunosuppression to tocilizumab (600 mg). He had initially good response to treatment, however it was short lived as he started developing flares. He was hence considered as TCZ failure and bDMARD (biological DMARDs) was switched to TNF inhibitors, Adalimumab, to which the patient responded well, with resolution of joint, eye and skin manifestations.
POS142
Amyloidosis
Image and Bar Table 1

Image and Bar Table 2

POS143
Phenotypic Variability and Novel Cutaneous Manifestations of Majeed Syndrome in Two Siblings
Bone marrow aspirate showed dyserythropoiesis in patient 2. Imaging revealed CRMO in the first patient, while the second had no radiological signs of bone inflammation. Genetic testing later confirmed a shared missense mutation in the LPIN2 gene, specifically in exon 17. Due to the lack of IL-1 inhibitors in India, the patients were managed with glucocorticoids, NSAIDs, and colchicine. While patient 2 responded well, patient 1 showed only partial improvement.
POS144
An Orphan Amongst the Lot - Pyoderma Gangrenosum, Acne and Hidradenitis Suppurativa (PASH) Syndrome
The patient was initially treated with high-dose prednisolone and dapsone, but the response was suboptimal. He was then switched to subcutaneous adalimumab 40 mg, with a good response. However, due to affordability issues, adalimumab was replaced with cyclosporine. The dose of cyclosporine could not be optimized due to hypertension and elevated creatinine levels. Tofacitinib was also attempted, but without improvement. Due to persistent symptoms, the patient was restarted on prednisolone 40 mg with a tapering schedule, alongside adalimumab 40 mg fortnightly (provided through hospital supply). After two weeks, new lesions developed, prompting an increase in the adalimumab dose to 80 mg fortnightly, as per PIONEER trial recommendations, along with the reintroduction of cyclosporine. This resulted in an excellent resolution of lesions. (1b, 2b, 3b)
Given that PSTPIP1 mutations increase IL-1 ß activity, TNF-alpha inhibitors, anakinra combined with cyclosporine, and IL-17 inhibitors have shown effectiveness in treatment. This case underscores the importance of dose escalation in achieving effective resolution of symptoms in complex autoinflammatory conditions like PASH syndrome
Image and Bar Table 1

Image and Bar Table 2

POS145
A Rare Case of Chronic Variable Immunodeficiency With Growth Harmone Deficiency
POS146
“Brucellosis with Musculoskeletal Manifestations: Insights from Five Clinical Cases”
Image and Bar Table 1

Image and Bar Table 2

POS147
Recurrent Sinopulmonary Infections and Non Resolving Pneumonia – An Ongoing Uncertainty
1. Cunningham-Rundles C, Bodian C. Common variable immunodeficiency: clinical and immunological features of 248 patients.
2. Bonilla FA, Barlan I, Chapel H, Costa-Carvalho BT, Cunningham-Rundles C, de la Morena MT, Espinosa-Rosales. International Consensus Document (ICON): Common Variable Immunodeficiency Disorders.
3. Chapel H, Cunningham-Rundles C. Update in understanding common variable immunodeficiency disorders (CVIDs) and the management of patients with these conditions.
4. Resnick ES, Moshier EL, Godbold JH, Cunningham-Rundles C. Morbidity and mortality in common variable immune deficiency over 4 decades.
Image and Bar Table 1

POS148
“Chronic Infections and Gingivitis in a Young Male: The Importance of Early Diagnosis and Treatment”
Image and Bar Table 1

Image and Bar Table 2

POS149
Unusual Case of Lipodermatosclerosis Presenting as Polyarthritis Following Gastric Bypass Surgery
Image and Bar Table 1

Image and Bar Table 2

POS150
A Novel Case of Hereditary Angioedema – is there a Genotype-Phenotype Correlation? – A Case Report
Genetic testing is usually not essential since the biologic tests are relatively accurate after the age of 1 year and there is no correlation between the genotype and phenotype expression so far. More than 150 different mutations have been identified in patients with HAE and can serve as potential modifiers of disease expression.
POS151
An Unusual Cause of Psoas Abscess in a Patient with Systemic Lupus Erythematosus
Image and Bar Table 1

Image and Bar Table 2

POS152
Syphilis: The Persistent Mimicker - A Case Series
Image and Bar Table 1
Image and Bar Table 2

POS153
Eosinophilia: Delving into the Unseen
On examination power was 3/5 in bilateral forearms and arms; 2/5 in bilateral lower limbs tone reduced in all limbs; thenar hypothenar atrophy, loss of functions of hand muscles. Fine touch lost distal to wrist and below knees.
Management focused on hyper eosinophilic vasculitis and pancreatic tuberculosis concurrently giving glucocorticoids, intravenous immunoglobulins, anti-tuberculosis therapy, and rituximab later.
Image and Bar Table 1

Image and Bar Table 2

POS154
A Neuropathic Riddle with Unseen Answers
Her nerve conduction study revealed sensory polyneuropathy. Erythrocyte sedimentation rate (ESR) was elevated (80mm in first hour). Autoimmune work up including anti- nuclear antibody, anti-neutrophil cytoplasmic antibody, complement, serum cryoglobulin, slit skin smear came to be negative. Vitamin B12 and blood sugar was within normal range. Sural nerve biopsy was done and revealed the diagnosis of leprosy related neuritis.
Retiform purpura of bilateral lower limb

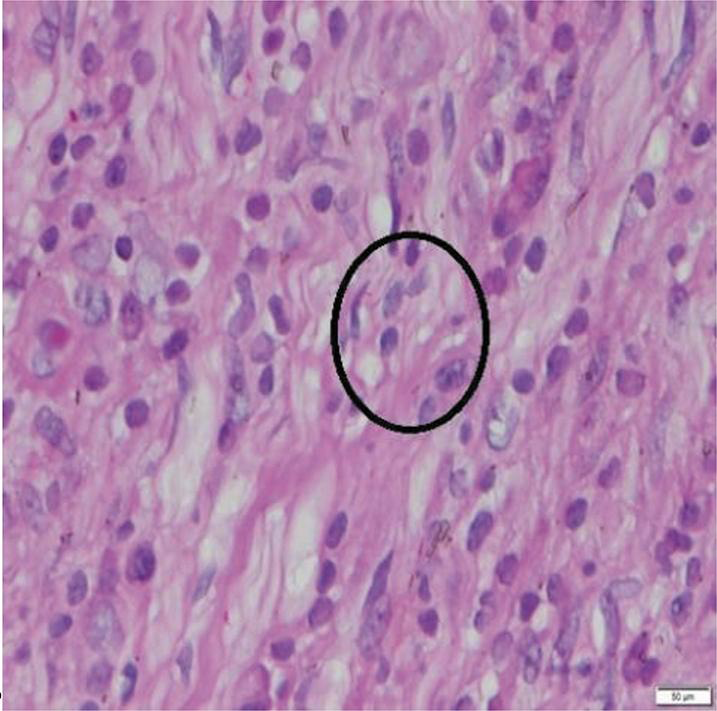
POS155
Tuberculosis Causing Secondary HLH: Uncommon Presentation of a Common Disease: A Case Series
We highlighted two cases of secondary HLH in adults with varying presentations with underlying triggers as Mycobacterium tuberculosis (MTb). These cases were referred to our centre as PUO. The first patient was a 68 years male who was diagnosed as HLH on bone marrow findings and he succumbed to his illness due to lack of definitive ante mortem diagnosis and rapid downhill progression of the disease. In second case, the prompt diagnosis and timely initiation of ATT in the early course of disease helped in significant improvement of patient outcome. Both patients with TB-HLH showed disseminated disease, manifested by extra-pulmonary TB, lung, pleural, splenic, liver and bone marrow involvement.
HLH is associated with high mortality and TB-HLH is no different. The prompt ATT was associated with survival independent of steroid therapy and was proven modifiable factor associated with lower mortality. The challenges in clinical medicine with patients of confirmed TB diagnosis was first to confirm secondary HLH, as TB alone can lead to fever, cytopenias and other similar characteristics of HLH. The presence of Low ferritin or even normal ferritin doesn’t exclude TB-HLH. The catch was rarity to see leukopenia and thrombocytopenia in Tb. The exact prevalence of TB-HLH is not well established, but it is estimated to comprise less than 2% of tuberculosis cases in immunocompetent adults based on case series and other literature reported on TB-HLH. In literature it is mentioned that TB-HLH, was often misdiagnosed, had high mortality and that early diagnosis and treatment were crucial for improving outcome. Incidence of anergy, defined by the absence of interferon–gamma mediated T-cell memory. A lack of response to M tuberculosis antigens and mitogen stimulation is associated with development of TB-HLH. Defective adaptive immune responses to MTb may facilitate persistence and dissemination of tb to the bone marrow. Removal of MTb antigen through ATT may be a key step in attenuating pathologic hyperinflammation in TB-HLH.
Therefore, it is reiterated that in endemic countries like India, TB-HLH is likely under reported and the diagnostic workup of patients with HLH should include bone marrow investigations for evidence of Mycobacterium tuberculosis like PCR based test on Marrow in addition to comprehensive search in lymph nodes or granulomas in RAS. The prompt initiation of ATT is crucial in improving survival in TB-HLH.
Image and Bar Table 1

POS156
Asymmetry: The Hidden Trigger of Suspicion
Case Details
September 2022
36/F presented with Inflammatory Polyarthritis and recurrent oral ulcers
ANA +4 (Speckled), dsDNA negative, Complement- N
Diagnosed as Incomplete Lupus – Started on Methotrexate
Was doing well for 7 months.
May 23
Presented with proximal lower limb muscle weakness.
Normal Muscle enzymes.
Myositis profile- Ro52 +3
Muscle biopsy- Type 2 fibre atrophy, No evidence of inflammatory myositis
Hiked Methotrexate in v/o myositis
Patient was doing well till July 23
Then she developed worsening proximal muscle weakness in right lower limb with static power in the left Lower limb- no improvement
MRI Thighs
Hyperintensities involving vastus lateralis, intermedius, semi membranous and semi tendinous.
Hyperintensities along the Hamstrings muscle
Evidence of active inflammation in muscles- dose of steroids /Methotrexate hiked.
Improvement in muscle power on follow up –2 weeks later – continued on same medication.
September 23
New onset S/c nodules on the the right leg, upper back, bilateral arms, face- lipoatrophy with skin hyperpigmentation
Also she developed new onset Left Upper limb weakness
Suspicion of progression in disease with disease related panniculitis versus alternate causes.
Skin Biopsy was done from left upper arm-
Dermis- Perivascular inflammatory infiltrate composed of Lymphocytes, histiocytes, plasma cells.
Sub cutaneous tissue- necrosis/septal inflammation comprised of neutrophils, lymphocytes and aggregates of histiocytes.
Vague granulomas in both dermis and subcutaneous tissue
ZN for AFB- Highlights clusters of bacilli
Further management
Post starting of ATT- patient developed worsening skin lesions with fever spikes, arthritis and myositis
Paradoxical IRIS
Hiked dose of steroids after which the fever spikes reduced and patient improved.
With the presence of false positive antibodies too.
In case of any deviation – like asymmetric involvement should raise the suspicion of an alternative diagnosis.
Image and Bar Table 1

Image and Bar Table 2

POS157
The Wolf and The Lamb: A Dilemma
More common in women.
Dermatomyositis is rarely reported in HIV population and associated with AIDS.
Presented with fever for 3 months
Proximal>distal Bilateral upper limb and Lower limb weakness for 2 months
Painful diplopia for 15days
Mother: Expired of HIV infection. Brother-PLHA on ART therapy.
Painful restriction of right medial rectus, left abductor and inferior rectus
Upper limb and lower limb -both proximal and distal weakness.
Peri-fascicular atrophy and necrosis
Orbital Myositis in MRI
Initial improvement on steroids but later worsening of symptoms with new onset bulbar, respiratory weakness and myocarditis after initiating ART-required IVIG.
Patient succumbed to death.
Paradoxical worsening of myositis after ART initiation in AIDS has fatal outcome.
Image and Bar Table 1

Image and Bar Table 2

POS158
“Beneath The Shadow of The Malevolent Meiloid: A Tale of Vengeance”
Investigations revealed neutrophilic leucocytosis, high serum procalcitonin (92.52mg/L), normal C3 and C4 levels, hyperferritinemia (301ng/ml), high CRP (101.7mg/dl), normal serum CPK; dengue profile, malaria card test, brucella IgG and IgM were negative. X-ray both knees were normal. USG showed collection (7to8cc) in vastus intermedius and medialis muscles with surrounding edema in left thigh. Blood culture showed significant growth of Burkholderia cepacia. STIR hyperintensity in lower part of vastus medialis, intermedius, short head of biceps femoris and adductor magnus muscles with intermuscular and periosteal edema noted along with bone infarcts in distal shaft of femur and medial femoral condyle with mild knee joint effusion on MRI.
Synovial fluid from left knee was inflammatory and no organisms isolated from culture or gram stain. Infectious disease specialist opinion was sought following which ceftazidime switched to cefoperazone-sulbactum and minocycline.
In view of persistent left thigh pain, recurrent fever and weight loss she was further investigated. Interval increase in size of altered signal intensity in mid and distal left femur shaft and medial femoral condyle with cortical break, interval appearance of altered marrow signal intensity proximal left femur, proximal tibia and fibula noted in repeat MRI.
PET CT showed metabolically active areas in distal metaphysis and shaft of left femur, medial condyle, bilateral proximal tibia and sclerotic area in head of right fibula likely multifocal osteomyelitis. CT guided multiple core biopsies were obtained from left distal femur and vastus medialis muscle.
Necrotic bony tissue with mixed inflammatory infiltrate was seen on histopathology. Tissue culture showed moderate growth of Burkholderia pseudomallei. AFB stain and TB Gene expert were negative. Treatment was escalated to Meropenam and Doxycycline following which patient improved symptomatically. Physiotherapy and rehabilitation has been initiated to prevent contractures of left lower limb. She has been restarted on Azathioprine.
Image and Bar Table 1

Image and Bar Table 2

POS159
Polymyositis Manifesting as Acute Inflammatory Vasculitis—A Rare Presentation
In summary, presentation of polymyositis with acute inflammatory vasculitis is rare and poses diagnostic challenges. A high index of suspicion is needed in such cases.
1. Conticini E, d’Alessandro M, Al Khayyat SG, et al. Inflammatory muscle involvement in systemic vasculitis: A systematic review. Autoimmun Rev. 2022;21 (3):103029. doi:10.1016/j.autrev.2021.103029
Image and Bar Table 1

Image and Bar Table 2

POS160
Pneumomediastinum & Vocal Cord Involvement in A Case of Anti-MDA5 Antibody-positive Clinically Amyopathic Dermatomyositis
Cluster 1, MDA-5 RP-ILD type, presents with lung disease.
Cluster 2, MDA-5 rheumatic DM type, presents with myositis and inflammatory arthritis.
Cluster 3, MDA-5 vasculopathy DM type, with the cutaneous vasculopathy findings of Raynaud’s phenomenon, digital necrosis.
Our case appears to be an overlap between Clusters 1, 2, and 3. Initial hyperferritinemia suggested a poor prognosis for ILD. Deterioration of her lung disease even after 2 months of immunosuppressive therapy with cyclophosphamide and ciclosporin led us to upscaling her regimen to rituximab and tofacitinib.
Image and Bar Table 1

Image and Bar Table 2

POS161
Polymyositis Affecting Distal Musculature Masquerading as Cellulitis in A Patient with Acute Lymphoblastic Leukemia
Image and Bar Table 1

POS162
A Case of MDA-5 Dermatomyositis with Refractory Cutaneous Disease
He was finally considered for repeat B cell depletion in view of progressive ILD as well and received 2 doses of 1g Obinutuzumab each in view of past non response to Rituximab.
1. Nombel Anaïs, Fabien Nicole, Coutant Frédéric. Dermatomyositis With Anti-MDA5 Antibodies: Bioclinical Features, Pathogenesis and Emerging Therapies. Frontiers in Immunology (2021). doi=10.3389/fimmu.2021.773352
2. De Santis M, Isailovic N, Motta F, Ricordi C, Ceribelli A, Lanza E, et al. Environmental Triggers for Connective Tissue Disease: The Case of COVID-19 Associated With Dermatomyositis-Specific Autoantibodies. Curr Opin Rheumatol (2021) 33:514–21
Image and Bar Table 1

Image and Bar Table 2

POS163
Immune-Mediated Necrotizing Myositis (IMNM): A Case Series of Atypical Presentations
Atorvastatin was stopped and pulse methylprednisolone was given. Since dysphagia progressed, IVIG (100g), corticosteroid (CS) taper and methotrexate (MTX) (15 mg/week) were given. She improved and CPK reduced (667mg/dl).
In our study of 3 patients, two were HMGCR antibody-positive with statin-induced myopathy. One required pulse MPS, IVIG, and MTX, while the other responded to high-dose CS and maintenance MTX. The 2nd patient had the cervicobrachial variant, needed pulse MPS, IVIG, and maintenance MMF.
The 3rd patient had HMGCR-related IMNM despite having two MSAs. With treatment, all 3 showed clinical improvement and declining CPK levels.
Image and Bar Table 1

Image and Bar Table 2

POS164
Dutasteride Induced Reversible Acute Necrotising Myopathy
An 80-year-old male presented with painful thighs after commencing dutasteride 5 days earlier for benign prostatic hyperplasia. Medical history included previous bypass surgery, chronic kidney disease (baseline creatinine 119 umol/L), hyperlipidaemia and urolithiasis. Medications were dutasteride (with tamsulosin) aspirin, candesartan, isosorbide mononitrate, pantoprazole and rosuvastatin. Examination revealed mild weakness in left hip flexors (4+/5) and normal power (5/5) in other muscle groups. There were no dermatological manifestations of myositis. Laboratory tests showed elevated creatinine kinase (CK) 7089, alanine transferase (ALT) (172 g/L), aspartate transferase (AST) (305 g/L), creatinine (430 umol/L) and mild pigmenturia. Magnetic resonance imaging (MRI) showed symmetrical diffuse muscle oedema in the lower limb muscle groups (Image 3). Myositis blot and HMGCR antibodies were negative. CT chest and upper abdomen ruled out solid tumours. Muscle biopsy showed features of active necrotising myopathy without inflammatory cell infiltrate (Images 1 and 2). Patient received intravenous fluid therapy while dutasteride and statin were discontinued. Patient did not receive any steroids. Patient made a complete recovery within four weeks. A repeat MRI showed complete resolution of myositis signs (Image 3). Statin was recommenced without recurrence of symptoms.
Image and Bar Table 1

Image and Bar Table 2
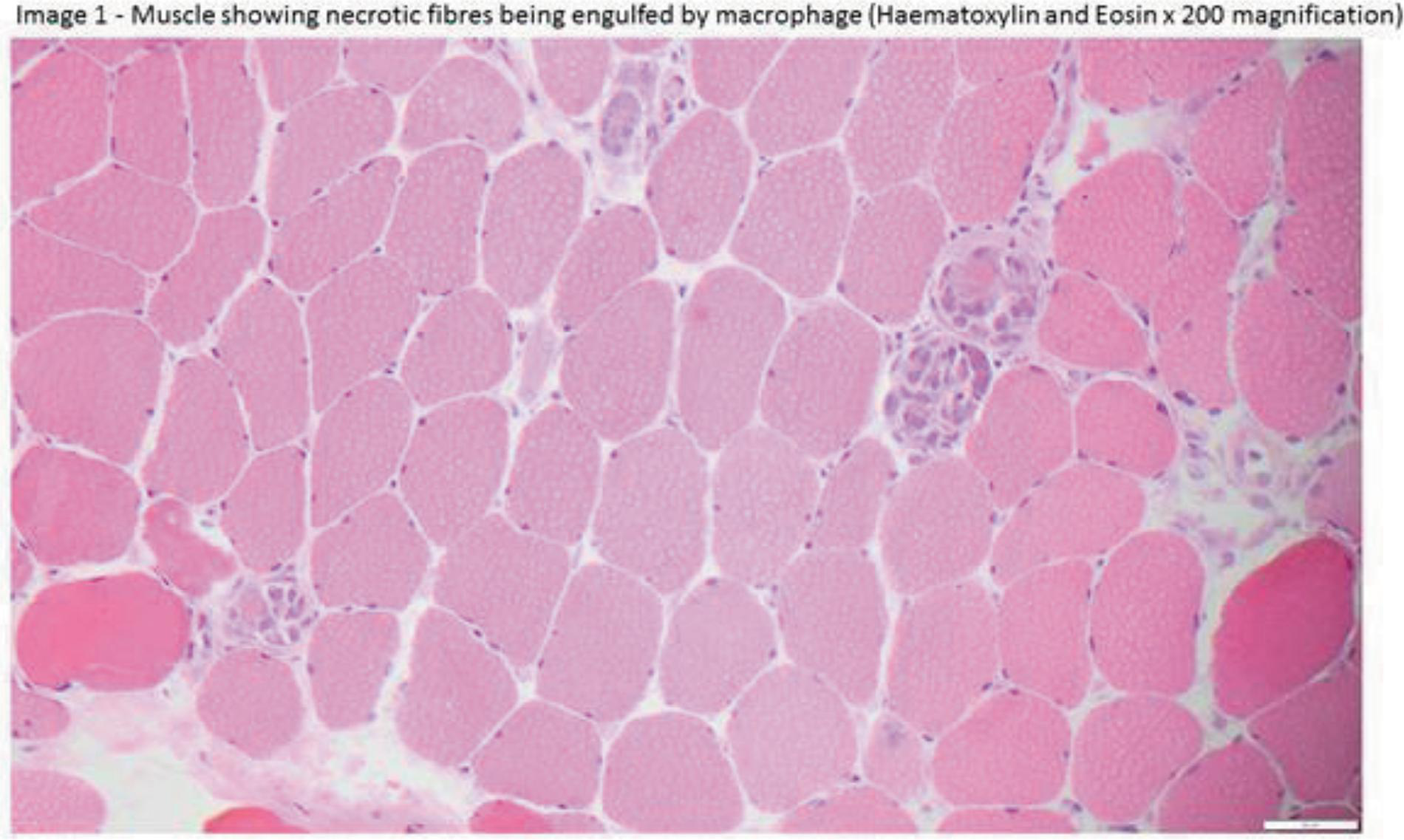
POS165
“Unveiling the Rare Coincidence: Idiopathic Inflammatory Myopathy with Pyomyositis in A Young Adult”
Investigations showed elevated muscle enzymes (CPK: 3600 U/L, LDH: 1157 U/L, ALT/AST: 244/101 U/L). ANA by IIF showed an AC-4 nuclear fine-speckled pattern, with line immunoassay positive for MI-2α and MI-2β antibodies. Serum IgG was elevated (26.3 g/L) with normal complement levels. Mantoux, TB Gold QuantiFERON, and antiphospholipid antibodies were negative. MRI of the thighs and muscle biopsy confirmed myositis. FDG-PET CT revealed extensive FDG-avid muscle lesions in the chest wall, shoulder girdle (right > left), bilateral upper limbs (SUVmax 9.15), right tibialis anterior, and bilateral abductor digiti minimi, along with fat stranding and edema. The abscess pus was negative for gram and ZN staining, culture, and GeneXpert. A biopsy of the skin surrounding the abscess revealed non-necrotizing granulomas
Image and Bar Table 1
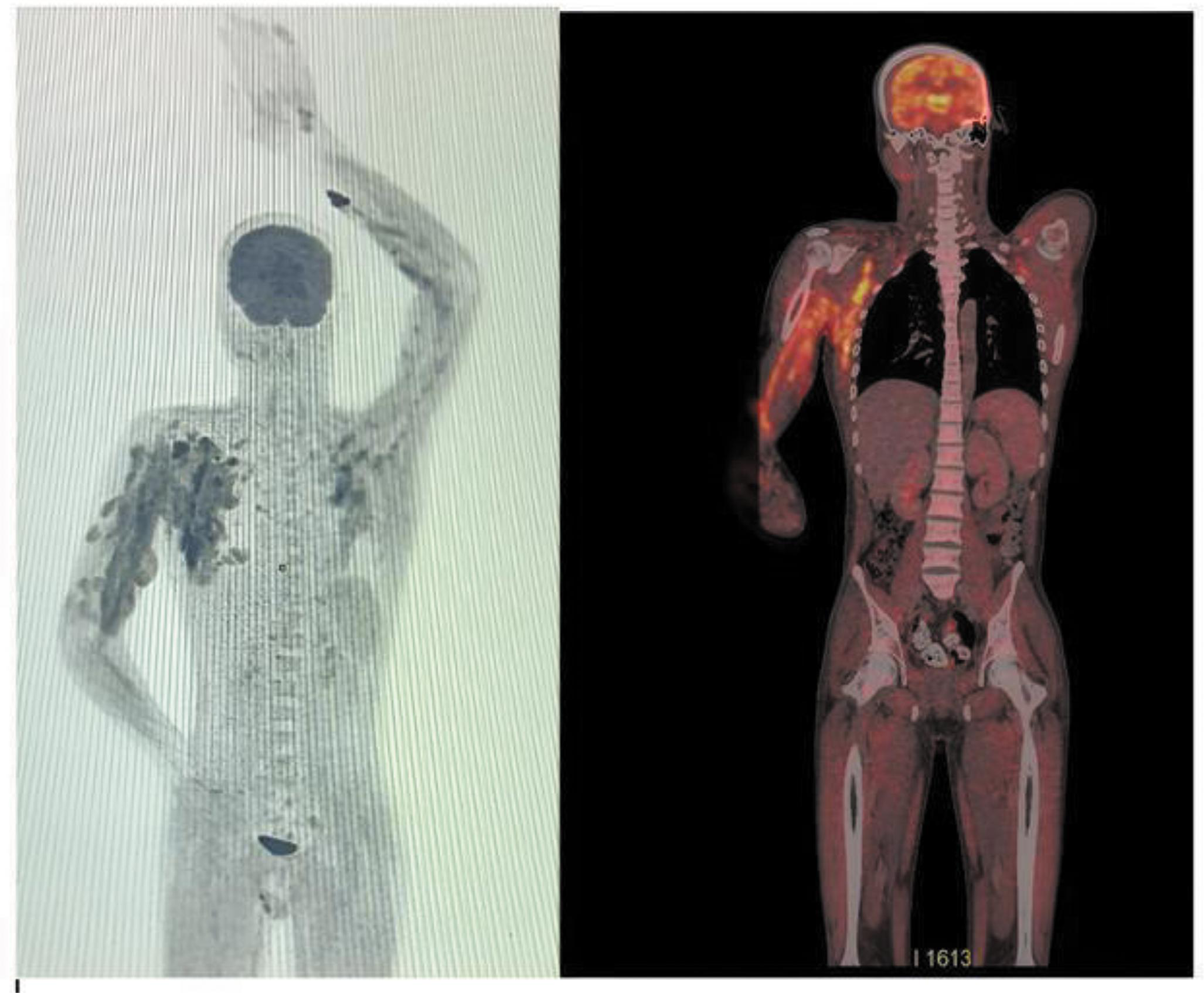
Image and Bar Table 2

POS166
Dermatomyositis - A Case Report
Image and Bar Table 1

Image and Bar Table 2

POS167
A Rare Case of Paraneoplastic Dermatomyositis Associated with Thymoma
Examination revealed hyperpigmentation over face, ears and neck. Proximal muscle power was 3/5 in all limbs. He did not demonstrate bulbar weakness, fatiguability or diurnal variation of weakness.
Baseline blood investigations were normal. Creatinine phosphokinase was 3115 IU/L. Contrast enhanced CT scan of chest revealed a synchronous thymoma in anterior mediastinum and right cardio phrenic angle.
He underwent thymectomy and 20 cycles of radiotherapy. Histology showed type B1 thymoma. Three weeks after surgery he demonstrated marked improvement with normal proximal power and gradual reduction of facial pigmentation. Azathioprine and Prednisolone were tailed off gradually and completely stopped six months after surgery. Two months after stopping immunosuppressants, he sustained remission and CPK was normal at 110 IU/L.
Image and Bar Table 1

Image and Bar Table 2

POS168
Spectrum of Cardiac Involvement in Idiopathic Inflammatory Myositis
Image and Bar Table 1

Image and Bar Table 2

POS169
Difficult to Treat Cutaneous Manifestations of Myositis: Case Series of 3 Patients
Image and Bar Table 1

Image and Bar Table 2

POS170
When in Doubt Rely on Gold
Roopa Tekkatte,
POS171
Podocytopathy in Anti-Mi-2 Dermatomyositis: A Newly Emerging Renal Manifestation – Case Report
Renal biopsy was done because of proteinuria and light microscopy and immunofluorescence study were suggestive of minimal change disease (figure 1) and electron microscopy confirmed podocytopathy. Imaging studies supported the diagnosis of inflammatory myositis. He was started with high-dose steroids and mycophenolate mofetil and he symptomatically improved and proteinuria resolved over three weeks.
Image and Bar Table 1

POS172
Unveiling Lupus Through Muscle Weakness: A Unique Case of Proximal Myopathy as Presenting Manifestation of SLE
Globally, the prevalence of SLE is estimated to range between 20-150 cases per 100,000 individuals[1, 2] with an Indian prevalence of approximately 3.2-4.5 cases per 100,000 individuals [2]. While myopathy affects about 7-15% of SLE patients during the disease course, proximal myopathy as the initial presentation is extremely rare. [2]. Limited epidemiological data exist on the incidence and prevalence of proximal myopathy as a primary manifestation of SLE, but it has been reported sporadically in clinical practice and case reports worldwide.
1. Kaul, A., et al. (2016). “Systemic lupus erythematosus.” *Nature Reviews Disease Primers*, 2, 16039.
2. Hochberg, M. C. (1997). “Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus.” *Arthritis & Rheumatism*, 40 (9), 1725.
Image and Bar Table 1
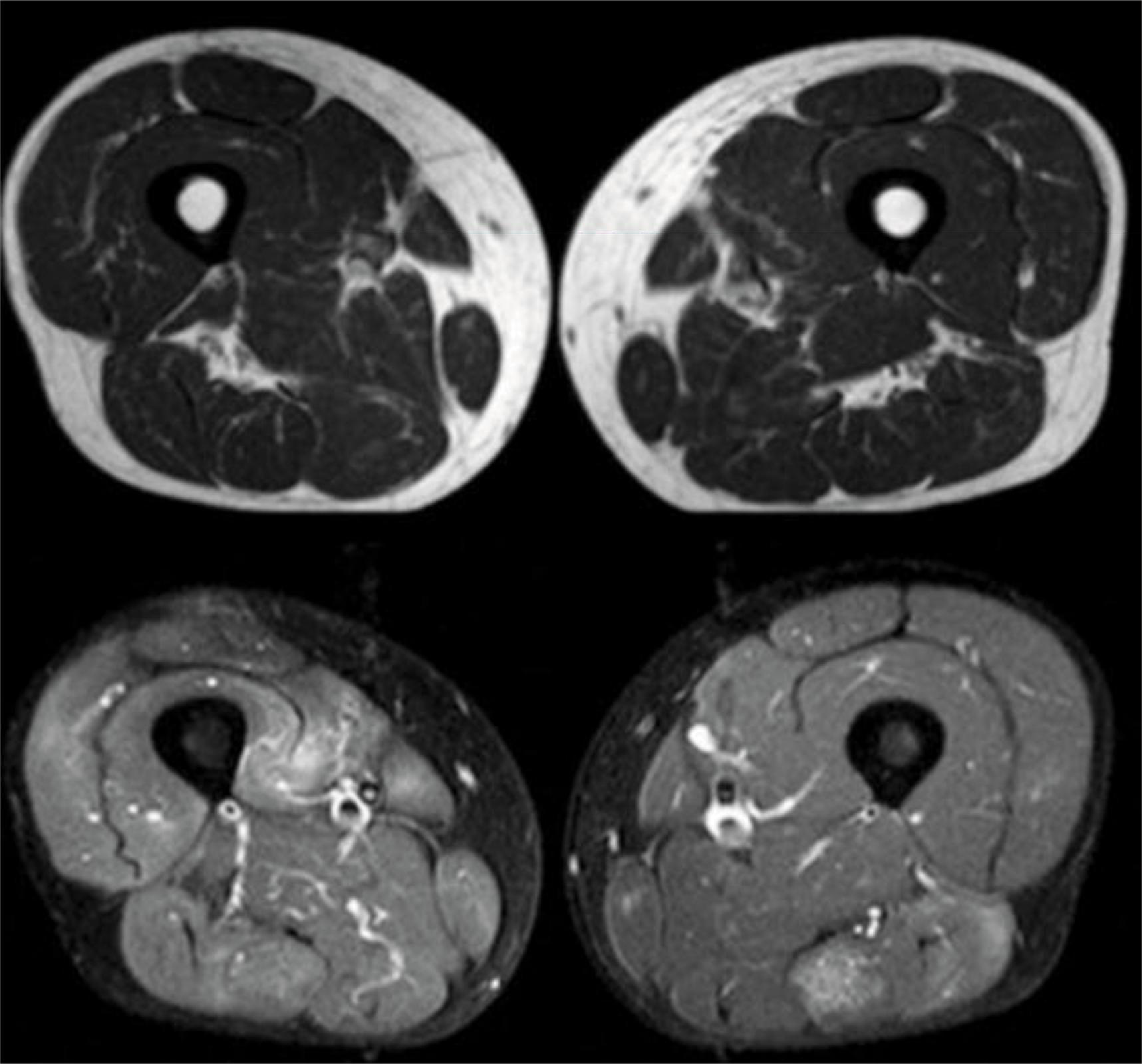
Image and Bar Table 2

POS173
Fatal Outcome in Anti-Mda5 Antibody Positive Dermatomyositis- A Case Report
POS174
Tackling Severe ILD: Case Series on Rapidly Progressive Interstitial Lung Disease
Padmanabha Shenoy, Sreekanth Anu, Nalianda Kaveri, vijayan Anuroopa,
Image and Bar Table 1

Image and Bar Table 2

POS175
Protean Manifestations of Dermatomyositis in South India Tertiary Care Centre
Mi2 alpha antibody is the common DM antibody seen.
Classical skin presentation is more commonly seen with anti Mi2 DM antibody positive patients.
Anti Mi2 antibody positive myositis can have unfavorable outcome.
In a patient with inflammatory arthritis with ILD, myositis has to be ruled out.
Knuckle ulcers may not always be associated with malignancies.
Anti NXP2 is not associated with malignancy.
Screening for gynaecological malignancies especially patients with TIF 1 gamma is mandatory.
Anti SAE did not develop cardiac involvement early in the disease.
Image and Bar Table 1


Image and Bar Table 2
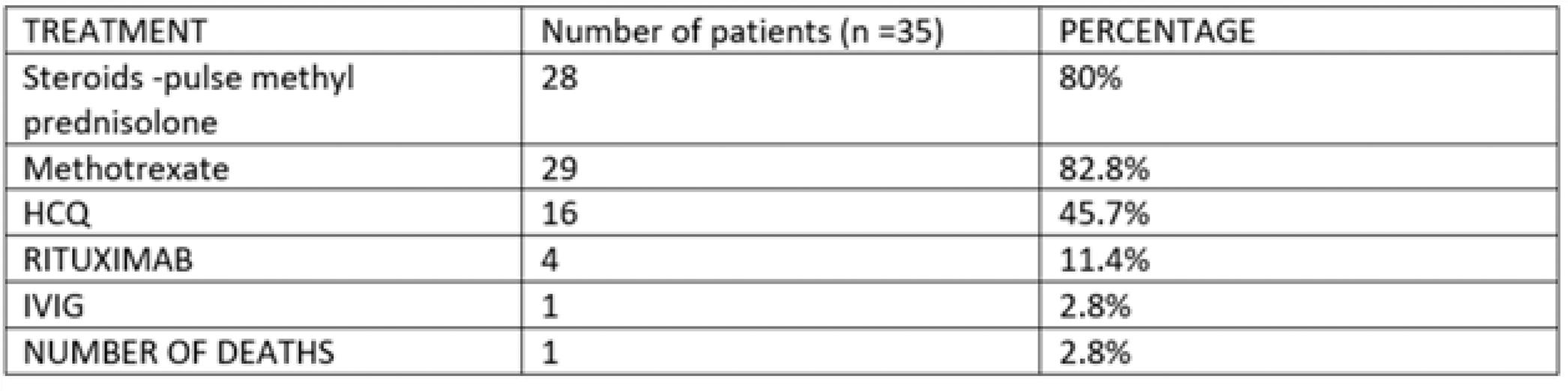
POS176
When Muscles and Rhythm Fail: Complete Heart Block in Dermatomyositis – A Rare Presentation
Accelerated atherosclerosis and atherosclerotic cardiovascular disorders. Cardiac inflammation from inflammatory cell tissue infiltration. Acquired channelopathies via modulated expression of myocardial ion channels from systemically released autoantibodies and cytokines. Autonomic dysfunction.
There are couple of case reports where in patient had suffered bradycardia post rituximab infusion. In our patient persistent bradycardia with asystole happened after 1 week of infusion, however it is difficult to say definitely its because of primary disease itself or due to rituximab.
Image and Bar Table 1

Image and Bar Table 2

POS177
Dual Pulmonary Infections in A Case of Anti-SAE Positive Dermatomyositis: A Clinical Challenge
High-resolution computed tomography (HRCT) of the thorax suggested pulmonary tuberculosis. Bronchoalveolar lavage (BAL) was performed, which showed a positive galactomannan index (GMI 6.14) and fungal culture revealing Aspergillus growth. Additionally, BAL CBNAAT was positive for rifampicin sensitive Mycobacterium tuberculosis. The patient was initiated on voriconazole for invasive aspergillosis and anti-tubercular therapy. Steroid therapy was gradually tapered without the introduction of any additional immunosuppressants. The patient showed significant symptomatic improvement, with follow-up chest X-ray demonstrating notable clearing of pulmonary opacities.
1. Nandy A, Gaini S, Sore P. Rapidly progressive interstitial lung disease in a patient with anti-MDA5-positive amyopathic dermatomyositis. Scand J Rheumatol. 2018;47 (4):334.
2. Muro Y, Sugiura K, Akiyama M. Low prevalence of anti-small ubiquitin-like modifier activating enzyme antibodies in dermatomyositis patients. Autoimmunity. 2013;46 (4):279.
Image and Bar Table 1

Image and Bar Table 2

POS178
Cases That Don’t Go by the Book. (Challenging Cases Seen in 6 Months of Fellowship at Centre of Rheumatic Diseases)
(1) 62 year old female (62/F) with elderly onset RA. Typical features (T) of inflammatory arthritis and atypical features (AT) of bilateral AVN of medial condyle of the Tibia. (2) 38/F with (T) Dermatomyositis and diffuse cutaneous scleroderma without organ involvement since 7 years (PM-SCL and SSA/RO 52) and (AT) of Bilateral ptosis, skin thickening, suboptimal response to DMARDS, cavitatory foci in lung on PET scan, incomplete resolution of ptosis post RITUXIMAB. (3) 63/F with elderly onset (T) Antisynthetase syndrome [PL-7, PL-12] (dysphagia 3 years before proximal muscle weakness) and (AT) no pulmonary involvement, suboptimal response to Rituximab but good response to DMARDS and Acute interstitial pneumonia. (4) 27/F with (T) rapidly evolving inflammatory polyarthritis and (AT) non tender nodules (elbows, wrist and back) - synovial biopsy of elbow - Teno Synovial Giant Cell Tumour (Pigmented Villonodular Synovitis), suboptimal response to DMARDS (RF, ACCP, ANA-Negative and ANA WB-u1snRNP, SSB/LA, Mi-2 positive) (5) 72/F EGPA with (T) severe eosinophilia, mononeuritis multiplex, nasal polyposis and a known case of bronchial asthma with diabetic neuropathy and retinopathy. ANA positive, ANCA (P and C) negative. (6) 37/M with (T) psoriatic arthritis, undifferentiated connective tissue disorder (RP, GERD, PAH) and (AT) Protein C deficiency, DVT, vasculitic ulcers on lower limbs (Sm/nRNP, SSA/RO52 positive). (7) 62/M with (T) Gout and (AT) polycystic kidney disease. (8) 40 year old female with (T) DISH, OA Knee and (AT) rapidly evolving GOUT (8) 2 cases of bilateral AVN HIP (1-spondyloarthropathy, 1-UMN lesion) (AT) no history of alcohol, tobacco or covid vaccine (2 males) (9) 22/F with (T) GPA (saddle nose, recurrent URTI, CSF rhinorrhoea) and (AT) subacute appendicitis due to vasculitis (ANA, cANCA positive). (10) 77/F with (T) elderly onset RA, left popliteal artery thrombosis leading to below knee amputation, (AT) RA vasculitis on right feet. (11) 42 year old male with (T) Spondyloarthropathy and (AT) vasculitis. Biopsy-Necrotizing leucocytoclastic vasculitis. (12) 65/F with (T) RA, ILD on Tofacitinib suffered from HERPES ZOSTER for 1.5 months (bilateral C5-C8 dermatome involvement). (13) 19/M with (T) Dermatomyositis with ulcer at PIP flexor aspect. (MDA-5, PM-SCL, PL7, SSA-Ro-52, u1snRNP).
POS179
The Calcified Mystery: A Tale of Unusual Arterial Aneurysms and Mineral Deposits
Examination revealed bilateral supraclavicular hollowing, subclavian artery pulsations, a pulsatile carotid aneurysm, left lower motor neuron facial palsy, Jaccoud’s arthropathy, multiple nodular swellings on the legs, high-arched palate, and calcinosis on the left forearm. Musculoskeletal findings included tenderness in bilateral MCPs and ankles, pes planus, left foot valgus, and fanning of toes. Neurological examination showed proximal muscle weakness (4/5) in the upper limbs and more pronounced in the lower limbs (3/5 proximally and 4/5 distally).
Laboratory tests revealed normal CBC, renal and liver function, with elevated ESR (45 mm/hr) and CRP (2.5 mg/dL). Rheumatoid factor and ANA were negative. Serum calcium was slightly elevated at 10.3 mg/dL, and phosphorus was markedly high at 8.5 mg/dL, with normal alkaline phosphatase.
Imaging, including CT angiography, revealed diffuse aneurysmal dilation of the bilateral subclavian arteries, multifocal aneurysms throughout the vertebral arteries, and multiple fusiform aneurysms in the cervical internal carotid arteries. Echocardiography showed a sclerosed aortic valve with trivial aortic regurgitation. Genetic testing identified a novel homozygous variant in the FGF23 gene, c.269G>A (p.Ser90Asn), which was classified as pathogenic upon reanalysis, consistent with the patient’s phenotype of hyperphosphatemic familial tumoral calcinosis. The patient was started on sevelamer and a phosphorus-restricted diet.
POS180
Role of Alprostadil in Patients of Severe Vasculopathy Despite Full Dose of Vasodilators
The 5th patient with a diagnosis of SSc SLE overlap presented with grade IV dyspnea, raised JVP, tender hepatomegaly, pedal edema with Severe PAH (mPAP - 63mm hg, TR jet velocity 3m/sec). CT pulmonary angiography was normal. Alprostadil 50mcg infusion was given in 50ml NS over 8 hours for 5 days every 3 weekly with total 6 doses till now.
All refractory RP with non-healing ulcer stopped progression after 1 week and healing of ulcer started after 6 weeks. DUCAS score and Raynaud’s condition score (RCS) improved. The 5th patient with overlap syndrome had a tremendous improvement in Dyspnea, mPAP, Po2, PCo2, and proBNP. LTOT was advised due to persistent Po2 of 61mm hg.
Image and Bar Table 1

Image and Bar Table 2


POS181
Ehlers Danlos Syndrome – A Rare Case Report from Central India
1. India. (2014). Rare Diseases India - Ehlers-Danlos syndrome. Rarediseasesindia.org.
2. Mathew T, Sinha S, Taly AB, Arunodaya GR, Srikanth SG. Neurological manifestations of Ehlers-Danlos Syndrome. Neurol India. 2005;53 (3):339-341. doi:10.4103/0028-3886.16938.
3. Ferreira O Jr, Cardoso CL, Capelozza AL, Yaedú RY, da Costa AR. Odontogenic keratocyst and multiple supernumerary teeth in a patient with Ehlers-Danlos syndrome--a case report and review of the literature. Quintessence Int. 2008;39 (3):251-256.
Image and Bar Table 1

Image and Bar Table 2

POS182
A “Neurofascin” Ating Reveal – A Case of Primary Sjogren’s Syndrome with Neurofascin Antibodies
Complaints of numbness over fingers of both hands, both feet and difficulty getting up from sitting position since 2 months. No bladder or bowel disturbances, band like sensation over the abdomen. No preceding fever, constitutional symptoms.
Spo2 – 98% SJC – 0 TJC – 0 Schirmer’s test – both eyes 25mm NS – Conscious, oriented Power – Upper limbs – 5/5 Lower limbs – 4/5 Sensory deficit – None Rhomberg’s negative Areflexia noted in the upper, lower limbs Bilateral plantar flexor
ANA blot – SS-A, Ro52 2+ NF 186 – 495 ng/ml NF 140 – 495 ng/ml NF 155 - Negative NCS Prolonged F wave latency in bilateral upper limbs, right and left tibial nerves Prolonged Latency distal right peroneal nerve Reduced CMAP in right sural and superficial peroneal nerves
Image and Bar Table 1

Image and Bar Table 2
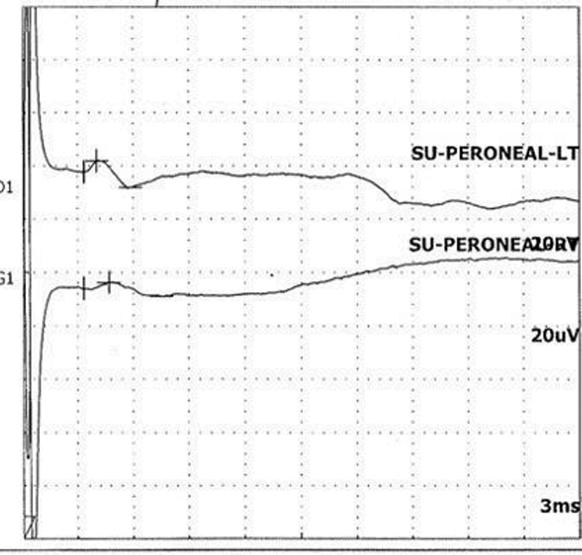
POS183
A Case of Bone and Muscle Woes
Musculoskeletal – hip movements were painful and restricted
CNS - proximal muscle weakness and waddling gait with normal reflexes and sensory examination
Urine showed hyposthenuria with proteinuria; 24 hours urine protein – 976mg Hb – 9gm/dL; ESR – 17mm/1st hour creatinine – 1.1mg/dL, potassium – 3mmol/L, calcium – 7.8mg/dL ALP – 582U/L, 25-OH-Vit D – 30ng/mL ABG – metabolic acidosis ENA – Anti-RO52 3+ X-ray (Figure 1) - insufficiency fractures at the proximal shaft of the femurs.
Image and Bar Table 1

Image and Bar Table 2

POS184
Mesenchymal Stem Cells for Refractory Digital Ulcers in Systemic Sclerosis: A Novel Therapeutic Strategy
Systemic sclerosis (SSc) is a debilitating disease characterized by microvascular dysfunction, immune dysregulation, chronic inflammation and fibrotic damage. Digital ulcers (DUs), particularly over the feet and fingertips, are common disabling manifestation and can be resistant to conventional treatments.
We present a case of 34-year-old female with Diffuse cutaneous SSc, suffering from a severe, non-healing, gangrenous Right great toe ulcer for 2years (Fig 1). She did not respond to maximum doses of vasodilators, wound debridement and infection treatment. Her lower limb angiogram showed complete occlusion of posterior tibial and dorsalis pedis artery suggestive of extensive peripheral vascular disease. Angioplasty was attempted twice for the same, however failed. She was also given anticoagulation and antiplatelet drugs.
Mesenchymal stem cells (MSCs) derived from donor bone marrow of healthy adults has been approved to treat chronic limb ischemia secondary to peripheral arterial and Buerger’s disease. By harnessing the regenerative, angiogenic, and immunomodulatory capacities of MSCs, we may effectively target the dysregulated processes driving SSc.
Our patient underwent MSC transplantation to her Right lower limb. She was given Adult Human BM derived, cultured, and pooled allogenic MSC.
Dose: 2 million cells/kg body wt.
Desired volume of suspension: 0.8 ml/kg body wt.= 2M cells/kg (for 150M cells formulation)
60 injections in a volume of 0.5ml/injection were given intramuscularly in lower half of posterior leg, anterior aspect of foot and around ulcer of great toe.
Image and Bar Table 1

Image and Bar Table 2

POS185
Azathioprine Induced Severe Bone Marrow Suppression with Telogen Effluvium in Undifferentiated Connective Tissue Disorder: A Rare Case
Azathioprine (AZA) is widely used immunosuppressive drug in connective tissue disorders (CTD), rheumatoid arthritis, vasculitis and many more. Toxicity of AZA range from mild to fatal severe myelosuppression as well as severe alopecia. Herein, we report an interesting case of telogen effluvium and severe myelosuppression that occurred following AZA administration. A 36years old female with undifferentiated CTD (UCTD) was treated with oral AZA of 50mg daily dose. A month of starting AZA, she presented to outpatient clinic for her follow-up. Her laboratory reports revealed low white blood cell count with absolute neutrophil count (ANC) of 70/mm3. She was admitted and AZA was withdrawn. After few days of hospital stay, she complained of hair loss which got severe over time. The blood indices returned to normal after AZA withdrawal and initiation of granulocyte colony stimulating factor (G-CSF). Improvement on her hair-fall was seen after 2 weeks. Dermatology consultation was done and a diagnosis of telogen effluvium was made after dermatology consultation.
Image and Bar Table 1

Image and Bar Table 2

POS186
“Hardening the Diagnosis: Unusual Calcification in Morphea Associated with Mixed Connective Tissue Disorder”
Physical exam revealed microstomia, non-scarring alopecia, pitted scars over the right 2nd and 4th finger pulps, hyperpigmented indurated plaques over both thighs, abdomen, trunk, buttocks, chest and left arm with hard well defined mobile subcutaneous nodules.
Immunological investigations revealed ANA (IF) - fine specked pattern, 4+ 1:320, LIA – u1 RNP+++, C3-87, C4-14, DCT +ve, Anti ds DNA negative. 2-Decho an EPAP of 43 mm Hg. CT thorax was normal, and a skin biopsy taken from the medial aspect of the left thigh showed– septal collagenization and dystrophic calcification.
Patient was treated as a case of MCTD with Morphea and was managed with MMF as a common immunosuppressant for both spectrum diseases’. Pulmonary artery hypertension and Raynaud’s withwas managed with sildenafil.
Image and Bar Table 1

Image and Bar Table 2

POS187
Dual Diagnosis Dilemma: A Case Report on the Overlap of Systemic Sclerosis and Rheumatoid Arthritis
Systemic sclerosis is an Autoimmune Connective tissue disease, characterised by immune overactivity and progressive fibrosis that typically involves the skin, with variable organ system involvement. There are two major types of systemic sclerosis: Limited cutaneous systemic sclerosis (lcSSc) and Diffuse cutaneous systemic sclerosis (dcSSc). We report a case of 27yrs old Female patient who presented with tightening of Skin of Face Hands and feet, associated with recurrent painful Bluish discolouration, swelling of hands and feet, multiple joint pain, shortness of breath on exertion and regurgitation of food for the past 3yrs. On examination there was Mauskopf facies, inadequate mouth opening, dry gangrene of fingers, Bilateral Fine crepts on respiratory system ausculatation. In view of suspected Autoimmune disorder, ANA was sent and Nail fold capillaroscopy was done given the history suggesting Raynaud Phenomenon. Anti Scl70 Antibody was strongly positive. Nail fold capillaroscopy examination showed Normal Capillary loops. HRCT was done that revealed ILD with UIP pattern. ECHO revealed normal Study. As patient had history of Joint pain, RA factor and anti CCP antibody were sent that came out to be positive. A diagnosis of Diffuse Cutaneous Systemic Sclerosis- Rheumatoid Arthritis overlap with UIP pattern ILD and Secondary Raynauds was made. Patient was started on Low Dose Steroids, Ramipril, Tadalafil, Mycophenolate Mofetil. Nintedanib and Rituximab were also given in view of ILD associated SSC-RA. Patient responded to above treatment and is on regular OPD follow up.
ILD may occur in any patient with SSc, including those with pulmonary hypertension, but the risk is more with Diffuse (rather than Limited) cutaneous SSc, those with positive anti-Scl-70/anti-topoisomerase I antibody, and negative anti-centromere antibody. Overlap between SSc and RA is quite uncommon and only a few such cases have been reported, mostly associated with Diffuse Systemic sclerosis than Limited type.
POS188
Acquired Bartter’s Syndrome as A cause of Severe and Refractory Hypokalemia in A Patient with Primary Sjogren Syndrome
Rohan Chauhan, Kushal Sood,
Our patient was referred to us for severe and refractory hypokalemia. Her ABG was suggestive of metabolic alkalosis, hence, ruling out dRTA and diabetic ketoacidosis as the causes of hypokalemia. High urinary potassium levels (69 mmol/g Cr) indicated renal potassium loss. A transtubular potassium gradient (TTKG) of 17, metabolic alkalosis, low-normal BP and elevated urinary chloride (149 mmol/L), suggested diuretic use, Gitelman’s Syndrome or Bartter’s Syndrome as one of the causes of hypokalemia in our patient. Further evaluation revealed hypercalciuria with urine calcium/creatinine (Ca/Cr) ratio to be 1.3, hence, ruling out Gitelman syndrome (which is characterised by hypocalciuria with urine Ca/Cr <0.15). Since she was not on loop diuretics, Acquired Bartter’s Syndrome was diagnosed as the cause of her severe and refractory hypokalemia. She was started on Indomethacin at dose of 2 mg/kg/d and Eplerenone 25 mg/d. Her potassium levels gradually improved and we were able to switch her from intravenous to oral potassium replacement at discharge.
POS189
Severe Pulmonary Arterial Hypertension in A Patient of Primary Sjogren Syndrome
POS190
Erasmus Syndrome A Rare Case of Association of Diffuse Systemic Sclerosis with Accelerated Silicosis and Coal Worker’s Pneumoconiosis
The patient developed progressive dyspnea and chronic cough five years ago, which improved during work breaks but worsened with continued exposure. Three years later, he exhibited signs of SSc, including skin thickening, salt-and-pepper rashes over the chest (figure 1) and back, microstomia, Raynaud’s phenomenon, and joint pain. His modified Rodnan score was 25/51. Chest X-rays revealed diffuse nodular opacities, and serological tests confirmed SSc with positive Anti-Scl-70 antibodies. Pulmonary function tests showed a restrictive pattern, while HRCT indicated coalesced small nodules, ground-glass opacities, and egg-shell calcifications, consistent with accelerated silicosis (figure 2).
Image and Bar Table 1

Image and Bar Table 2

POS191
Pancreatitis and Periodic Paralysis in Sjogrens Syndrome-A Rare Case Report
TEST
VALUES
ESR
84mm/hr.
qCRP
24mg/dl
Total WBC count
15000cells/cu.mm
Serum Albumin
3.2g/dl
Serum Globulin
5.5g/dl
Serum Potassium
1.6mmol/L
Serum Bicarbonate
20mmol/L
CSF Glucose
157 mg/dl
CSF Protein
187mg/dl
CSF chloride
138mmol/L
Serum Lipase
1620 U/L
Serum Amylase
1271U/L
D Dimer
5198ng/ml
Urine pH
7.0
Urine Sodium
110mEq/L
Urine Potassium
22.9mEq/L
Urine Chloride
79mEq/L
Nerve conduction study revealed severe axonal sensory motor polyradiculopathy of both upper and lower limbs.
USG abdomen revealed mild peripancreatic collection extending into left anterior pararenal space. Hence CT was done showing features of acute pancreatitis.
Doppler legs- no DVT
So, she had acute pancreatitis and quadriparesis with hypokalemia.
Immunology showed strong positivity for Anti Ro 52 and Anti Ro 60 as well as TPO antibodies.
1. Chandrappa SS, Kumar P, Panda PK, Rao S. Primary Sjogren’s syndrome presenting as hypokalemic periodic paralysis and acute pancreatitis. BMJ Case Rep. 2024 Aug 14;17 (8): e260646. doi: 10.1136/bcr-2024-260646. PMID: 39142847.
2. Kulkarni N, Chopra A. Clinical Profile of Primary Sjogren’s Syndrome with Hypokalemic Periodic Paralysis. J Assoc Physicians India. 2018 May;66 (5):69-70. PMID: 30477063.
POS192
Immune Thrombocytopenia in A Patient with Systemic Sclerosis: A Case Report
Management of ITP in SSc is challenging because the use of high-dose steroids increases the risk of SRC [2]. Generally, SRC occurs early in the course of the disease, almost always within the first five years of disease onset. Because the disease duration was more than five years, he was treated with intravenous methylprednisolone 500mg for three days followed by oral prednisolone after exclusion of SRC.
However, the correct diagnosis is critical because treatment differs substantially for each of these life-threatening conditions.
1. Wielosz E, Majdan M. Haematological abnormalities in systemic sclerosis. Reumatologia [Internet]. 2020 [cited 2024 Sep 15];58 (3):162–6. Available from:
2. Boleto G, Avouac J, Godeau B, Allanore Y. Severe immune thrombocytopenia in two patients with systemic sclerosis. Joint Bone Spine [Internet]. 2023;90 (4):105560. Available from:
Image and Bar Table 1

POS193
Sjogren’s Syndrome Through a Rare Lens: Case Series of Neurological, Vascular, and Hematologic Involvement
A 34-year-old female with a history of SS presented with fatigue, anasarca, and hypertension. Laboratory findings revealed haematuria, proteinuria, hypocomplementenemia, and a positive RF. Kidney biopsy confirmed glomerulonephritis with tubule-Interstial nephritis, EM confirmed subendothelial deposits consistent with cryoglobulinaemic vasculitis. The patient responded well to rituximab and cyclophosphamide along with corticosteroid therapy, but letter succumbed to death at home with unknown reason.
A 54-year-old female diagnosed to have sjogren syndrome in 2019 with sicca, fatigue and serology of Anti Ro and La. In Aug 2023 she started c/o severe headache and after ruling out infections, considering aseptic meningitis which can happen with Sjogren’s syndrome, we gave a trial of MP bolus and oral prednisolone with which she improved but as soon as corticosteroids were tapered, headache again appeared. A neurology consult prompted an MRI which revealed pontine hyperintensity with a diagnosis of CLIPPERS syndrome (Image A) (Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids). She has been on tapering dose of prednisolone and has been started on rituximab to which she has responded. This case highlights the rare neurological manifestation of SS
A 37-year-old female with SS developed progressive pancytopenia and on examination there was moderate splenomegaly. Bone marrow biopsy revealed reticulin fibrosis, and autoimmune myelofibrosis was diagnosed. Treatment with corticosteroids and rituximab resulted in partial recovery of blood counts and reduction in spleen size. This case underscores the potential for severe hematologic involvement in SS.
Image and Bar Table 1

POS194
? Possible Pulmonary Raynaud’s
A 37 years old female presented in the year March2021 on a referral from the neurologist with a clinical diagnoses of Amourosis Fugax to rule out autoimmune etiology. She also had eye sicca and oral sicca symptoms with knee joint pain and right temporomandibular joint pains. She had high inflammatory markers and was found to have Anti SSA Ab and Anti Beta2 glycoprotein IgM positivity. She was initiated on low dose steroids, Methotrexate and Hydoxychloroquin. She was Methotrexate intolerant and was started on Tofacitinib. She responded to the treatment and joint pains reduced. She remained stable till January 2022, when she developed Covid but recovered with symptomatic treatment. Post Covid, she complained of severe fatigue and started developing rashes all over her body which responded to anti-histaminics but recurred on stopping them. In March 2023, she started developing desaturation on minimal exertion, with Oxygen saturation falling upto 75%.6Minute walk test showedsignificant desaturation (77%). CTPA was done to rule out pulmonary embolism, which was normal. She respond to steroids (Methylprednsolone 40mg/day) But we were unable to reduce the steroids below 20mg/day. Subsequently, HRCT chest, V/Q scan were also done, which were normal. MRI chest was done to rule out intercostal muscle myositis. Dynamic USG study was also done to rule out diaphragmatic weakness (r/o shrinking lung syndrome). Cardiac evaluation including Echo was done. All investigations were within normal limits. We tried to reduce the steroids 2-3 times but were not able to reduce below 20mg/day. Subsequently, after discussion with patient about using either Mycophenolate or Rituximab as a steroid sparing agent, it was decided to give Mycophenolate 2 gm/day, which was given for 3 months. Steroids were again tapered, but were unable to doso. Subsequently, Inj Rituximab was given in the dose of 500 mg/week for 4 weeks in October2024i and subsequently steroids were again tapered. We were able to taper the steroids upto 2.5 mg/day on alternate days. After 6 months, a single dose of Inj Rituximab 500 mg was given. At present, patient is off steroids. Plan is to give Inj Rituximab every 6 months.
A possible etiology is inflammatory vasospasm phenomenon occurring in pulmonary vasculature, hence a diagnosis of Possible Pulmonary Raynauds is made. This still remains a diagnostic dilemma.
POS195
From Generalized Pain to Targeted Diagnosis: A Case of Multifocal Skeletal Lesions
A 31 year old female, presented with insidious onset gradually progressive pain in bilateral shoulders and arms, bilateral groin and thighs, bilateral knees for the last 6 months. It was not associated with any history of swelling of joints. She was diagnosed as a case of autoimmune hepatitis 4 months ago and was managed with oral corticosteroids for 3 months (30mg daily, tapered weekly). On examination, she had widespread tenderness across bilateral shoulders, arms, thighs and knees. Musculoskeletal examination revealed painful restriction of bilateral shoulder and hip joints. Rest of the systemic examination was normal. Her haematological, biochemical parameters and acute phase reactants were normal. She was labelled as a case of fibromyalgia and managed with GABA modulators after ruling out secondary causes for fibromyalgia. However she continued to have persistent pain and underwent X-ray bilateral shoulder, hip and knee joints that were non-contributory. MRI right shoulder revealed geographic areas of altered signal intensity involving right humerus head (Hyperintense on T2WI/STIR and hypointense on T1WI) suggesting stage IV osteonecrosis of right humerus head. In view of widespread tenderness, bone scan was done which revealed significantly increased osteoblastic activity at bilateral shoulder, hip and knee joints suggestive of multifocal osteonecrosis. SPECT was done which showed doughnut appearance (increased uptake in the periphery with centrally photopenic region) of the right hip joint and confirmed the diagnosis of multifocal osteonecrosis. Her oral steroids were reduced to minimal dose and was referred to the orthopaedic and joint replacement department. She was advised the initial trial of conservative management with watchful observation.
We highlight this case to sensitise clinicians about this rare entity especially in the setting of autoimmune diseases on long term steroids.
Image and Bar Table 1

Image and Bar Table 2

POS196
Progressive Pseudo Rheumatoid Dysplasia (PPD)
No significant past medical or drug history.
No family history of musculoskeletal disorders.
Multiple skeletal deformities
Bilateral genu valgum and bilateral elbow deformities were present.
Short stature with no significant facial dysmorphism
Mild scoliosis, exaggerated lumbar lordosis and prominent chest was observed.
Positive Valley sign and Gower Sign
Severe wasting of the thenar and hypothenar muscles
Bilateral hip joint tenderness
Mild muscle wasting in the lower limbs
MRI of pelvis: Marrow edema in bilateral femoral heads along the acetabular margins. Cortical irregularity and hip effusion.
X-ray: Cortical irregularity with broadening of metaphyseal areas. Flattened vertebrae with mild abnormalities in vertebral bodies, thin cortices, and mild osteopenia.
Image and Bar Table 1

Image and Bar Table 2

POS197
AVN (Avascular Necrosis) in A Patient with Psoriatic Arthritis (PsA)
In our case the other causes of AVN were evaluated. There was no consumption of alcohol and smoking. Sickling test was negative. APS antibodies negative. Patient was not any drugs causing AVN. After ruling out the possible etiologies, the cause of AVN was considered secondary to psoriasis disease per Se. Previous studies reported that psoriasis by itself can cause AVN. The presence of psoriatic arthritis (PsA) increases the risk of AVN than those without PsA.
In study by Hsien-Yi chiu et al, AVN was more prevalent among psoriasis patients with severe disease compared to mild psoriasis. In a study by Hsien-Yi et al, AVN was positively associated with male sex, younger age, corticosteroid use and concomitant Psoriatic arthritis. In our case patient age was less than 30 years, used topical steroids earlier and he has concurrent Psoriatic arthritis.
POS198
“The Hidden Link: Empyema Revealing An Underlying Rheumatoid Arthritis”
We, here presented the case of a young male with Empyema complicating Rheumatoid arthritis and merely the first presentation of disease.
1. Lillington GA et.al, Rheumatoid Pleurisy With Effusion. Arch Intern Med. 1971.
2. Dieppe PA. Empyema in rheumatoid arthritis. Ann Rheum Dis. 1975 Apr.
3. Yigla M et.al. The problem of empyematous pleural effusion in rheumatoid arthritis: report of two cases and review of the literature. Clin Rheumatol. 2002.
Image and Bar Table 1

Image and Bar Table 2

POS199
Bilateral Sacroiliitis in A Patient with Rheumatoid Arthritis: Unraveling The Rope: A Case Report
The Rheumatoid nodule is the most common cutaneous manifestation of RA and often seen in seropositive RA and more severe disease [3]. There have been case reports of accelerated subcutaneous nodulosis in patient with RA, treated with MTX, leflunomide, azathioprine, TNF alfa inhibitors and tocilizumab [3].
Though Inflammatory back pain, active sacroiliitis, and plantar fasciitis mislead the diagnosis, rheumatoid nodules and positive anti-CCP antibodies aid the classification of RA.
Image and Bar Table 1

Image and Bar Table 2

POS200
A Bumpy Road to Space
Right distal forearm - Ventral aspect - Diffuse swelling 8*5 cm non tender firm and mobile, no change in size of swellings on wrist movements.
Right knee – fullness of suprapatellar fossa+ and patellar tap + Left knee - Cystic swelling in the popliteal fossa, 8*5 cm, non tender, fluctuant- reduced on knee flexion.
Left- moderate effusion, synovial thickening, large bakers cyst with internal echoes showing joint communication.
USG Right Forearm-Diffuse inflammatory thickening of flexor retinaculum of wrist and flexor tendon.
MRI Right thigh
T2/STIR hyperintensities - Posterior compartment, loss of fibrillary pattern thickening of fascia around muscles
Active myositis- Posterior compartment, superficial and deep muscles of mid and lower thigh with intense inflammatory changes
FNAC from swelling of Popliteal fossa of Left knee
Revealed lymphocytes, histiocytes and negative for malignancy
FNAC from swelling over posteromedial aspect of Right thigh
Revealed neutrophils, occasional ?giant cells, elongated spindle cells epithelioid cell aggregates, few lymphocytes.
Biopsy from swelling over posteromedial aspect of Right thigh
Fibromuscular tissue - multiple giant cells surrounded by lymphocytes, histiocytes s/o granuloma
Diagnosed as Sarcoidosis with
Chronic Granulomatous myositis
Synovitis
Tenosynovitis
Treatment and response
Started on 0.5 mg/kg steroids
Swellings gradually reduced in size
While swelling over forearm and bakers cyst disappeared completely, swelling over posteromedial aspect of thigh reduced by 80% in size with treatment
With reduction in dose of steroids- the swelling over thigh has begun to reappear
Steroids hiked and also started on azathioprine 75 mg per day
Evolution of diagnosis from subcutaneous swellings, which have varied etiologies arising from any tissue plane- Skin, SC tissue, muscle, bone -to a disease like sarcoid is interesting.
Having a high index of suspicion considering systemic diseases even with localized signs/ symptoms is the key at clinching the diagnosis.
Image and Bar Table 1

Image and Bar Table 2

POS201
Cardiac Sarcoidosis: A South Indian Collective
The M:F ratio was 8:13, mean age: 45 years (21-62).
The most common presenting feature was palpitations/syncope (n=14, 66%) > dyspnea on exertion (n=10, 47%) > fatigue and chest pain.
The mean delay from first medical visit to DMARD initiation was 21 months (0-144). Delay in workup for cause of cardiac dysfunction and in referral were the main reasons.
Biochemical parameters: Mean Calcium was 9.7 mg/dL and 2 (9.5%) had hypercalcemia. Mean ACE level was 50 U/L (6-118), 8 (38%) had elevated levels.
Mean ESR was 23 mm/hr (3-40) and CRP 9 mg/dL (0.3-40.8), elevated ESR in 10 (47%) and CRP in 8 (38%).
Radiology: All patients underwent Cardiac MR or PET-CT with characteristic findings. (Table 2)
Steroid sparing agents were used in 18 (86%): Methotrexate in 13 (62%), Mycophenolate mofetil in 6 (29%), and Adalimumab in 3 (14%).
One patient developed worsening of LV function on Adalimumab, which was subsequently with held.
Cardiac intervention was done in 12 (57%) in the form of PPI, ICD.
Overall improvement/stabilisation at 6th month and 1 year was seen in 10 (67%) and 5 (33%) respectively.
Mortality: Two (9%) patients succumbed to infection and cardiac failure respectively; both had significant treatment delay and scar burden.
In our series, 66% had elevated ESR/CRP and 38% had elevated ACE during active CS.
Poor outcomes were noted with delay in diagnosis, poor baseline EF, high scar burden.
Three patients had normal 2D-ECHOs, despite significant MR/PET abnormalities, highlighting the need for advanced imaging.
Image and Bar Table 1

Image and Bar Table 2

POS202
A Rare Combo! Heefordt -Waldenstrom Syndrome with Cardiac Sarcoidosis
She had shown improvement at her review visits as there was no fever, weight gain of 3 kg, absence of palpitations (PR – normal), reversal of parotid swelling and diplopia, normal CRP (3.4 mg/L). The slurring of speech however had persisted.
Image and Bar Table 1

Image and Bar Table 2

POS203
Breast Lump in Pregnancy- An Enigma Unveiled
She has no other joint pains/ fever/ known CTD/ any health issue till this presentation. First pregnancy was uneventful.
Her bloods showed normal CBC, LFT, RFT with elevated ESR and CRP. ANA IF was negative. PASP (2D-echo) was high (36 mmHg), USG abdomen was normal. Pregnancy prohibited X ray or CT imaging. A breast biopsy was pursued which showed non caseating granuloma favouring sarcoidosis over TB. ACE level was 34 (normal), serum calcium and Vit D were normal. A provisional diagnosis of sarcoidosis was made and treated with low dose prednisolone (7.5mg slowly tapered over a month), Azathioprine 100mg and cyclosporine 100mg.
Patient has a brisk response with near complete remission by the end of one month. She continued to do well for 2-3 months except for minimal cough and pricking sensation in breast at times. However, by 28 weeks of gestation she developed a purulent discharge from right breast for a week which was non painful. Other symptoms continued to be in remission. At this stage, Inj. Adalimumab was given along with prednisolone 5mg. After 3 doses, patient’s breast lesion is better with complete resolution of discharge and.
Image and Bar Table 1

Image and Bar Table 2
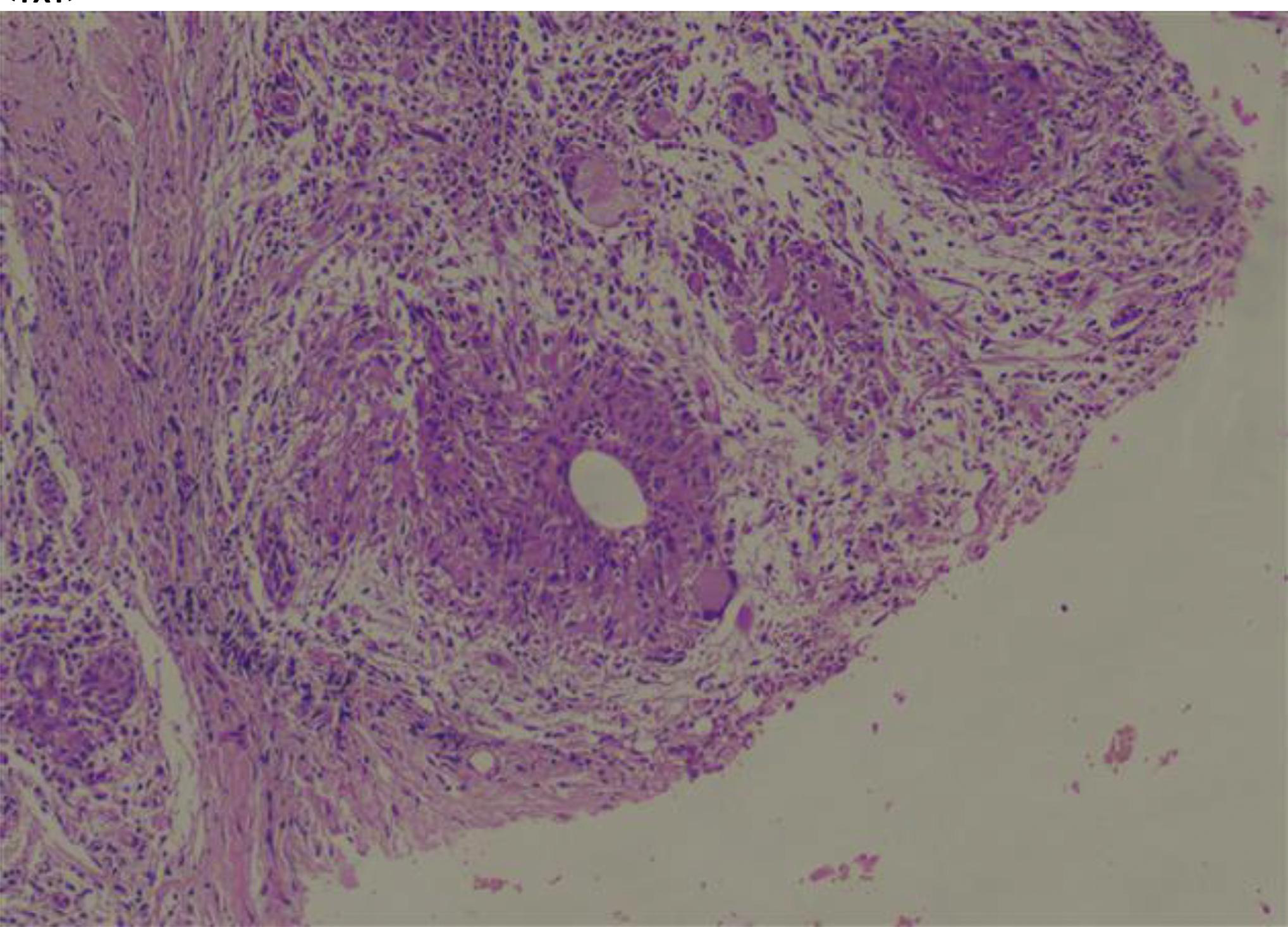
POS204
Leukocytoclastic Vasculitis Resulting from Adalimumab Treatment in A Patient Diagnosed with Ankylosing Spondylitis
Alireza Khabbazi,
Image and Bar Table 1

Image and Bar Table 2

POS205
A Rare Case of Axial Spondyloarthritis with IgA Vasculitis
IgA vasculitis is an immune-complex mediated vasculitis affecting small vessels with characteristic IgA deposition within the vessel walls. It is characterized by a tetrad of purpuric skin rash, arthralgias, abdominal pain and renal involvement. Children are primarily affected and typically have a good prognosis with a self-limiting course seen in about 90%. About 10% of cases occur in adults, in whom renal involvement accounts for 40% and 15% of adults have relapsing disease.
The role of the mucosal immune system of the gastrointestinal tract in the pathogenesis of spondyloarthritis is well established. In the setting of dysregulated mucosal immunity, peripheral B cells induce enhanced production of Galactose-deficient IgA1 (Gd-IgA1). In Gd-IgA, the abnormal glycosylation exposes Galactose and N-acetylgalactosamine (GalNAc) residues, leading to neoepitope formation and autoantibody production against Gd-IgA1 culminating in the formation of circulating immune complexes. These immune complexes get deposited in the small vessels of the skin and mesangium of the kidney further perpetuating the inflammatory process. These immune complex depositions may play a common link in the pathogenesis of the two diseases.
POS206
Axial Spondyloarthritis after Roux-en-Y Gastrojejunostomy: A Case Report
POS207
Breaking Down CRMO: Insights from A 10 Year Follow Up Case!
19-year-old male with onset of symptoms at 10 years of age presented with recurrent episodic pain in right thigh for 2 weeks duration. He had partial relief with NSAIDs. He denied history suggesting inflammatory low back ache, arthritis, extraarticular symptoms, rash, fever or constitutional symptoms. He had a family history of spondylarthritis in his mother and grandmother. On examination he had local tenderness in right mid-thigh. Rest of the systemic examination was unremarkable. Investigation revealed elevated acute phase reactants (ESR-67mm/hr, CRP-87mg/dl). HLA B27 (PCR) was positive. Rest of hematological and biochemical parameters were normal. Whole-body MRI revealed bone marrow edema in bilateral greater trochanter, proximal shaft of femur (right) and roof of acetabulum (left). MRI sacroiliac joints were normal. After ruling out possible infectious and malignant etiologies, he was diagnosed as a case of chronic recurrent multifocal osteomyelitis (CRMO) and started on regular NSAIDs. After an initial response, he had recurrence of symptoms and was started on low dose steroids and sulfasalazine. He remained asymptomatic for 6 months, later he had a flare and was started on weekly Etanercept. Over the last 10 years follow up, he had two episodes of disease flare managed with short course oral steroids and continued on weekly etanercept.
During his last follow up in 2024, he presented with inflammatory low back ache, peripheral arthritis involving bilateral knees and chest wall enthesitis. On repeat MRI he had worsening of BME on imaging and his MRI sacroiliac joints revealed bilateral sacroiliitis. Low dose computed tomography (LDCT) SI joint showed bilateral sacroiliac joint partial ankylosis. He was diagnosed as a case of CRMO with axial spondyloarthritis and was managed with short course of regular NSAIDS, spine physical therapy along with continuation of weekly Etanercept. He has shown good response to the treatment administered.
Image and Bar Table 1

Image and Bar Table 2
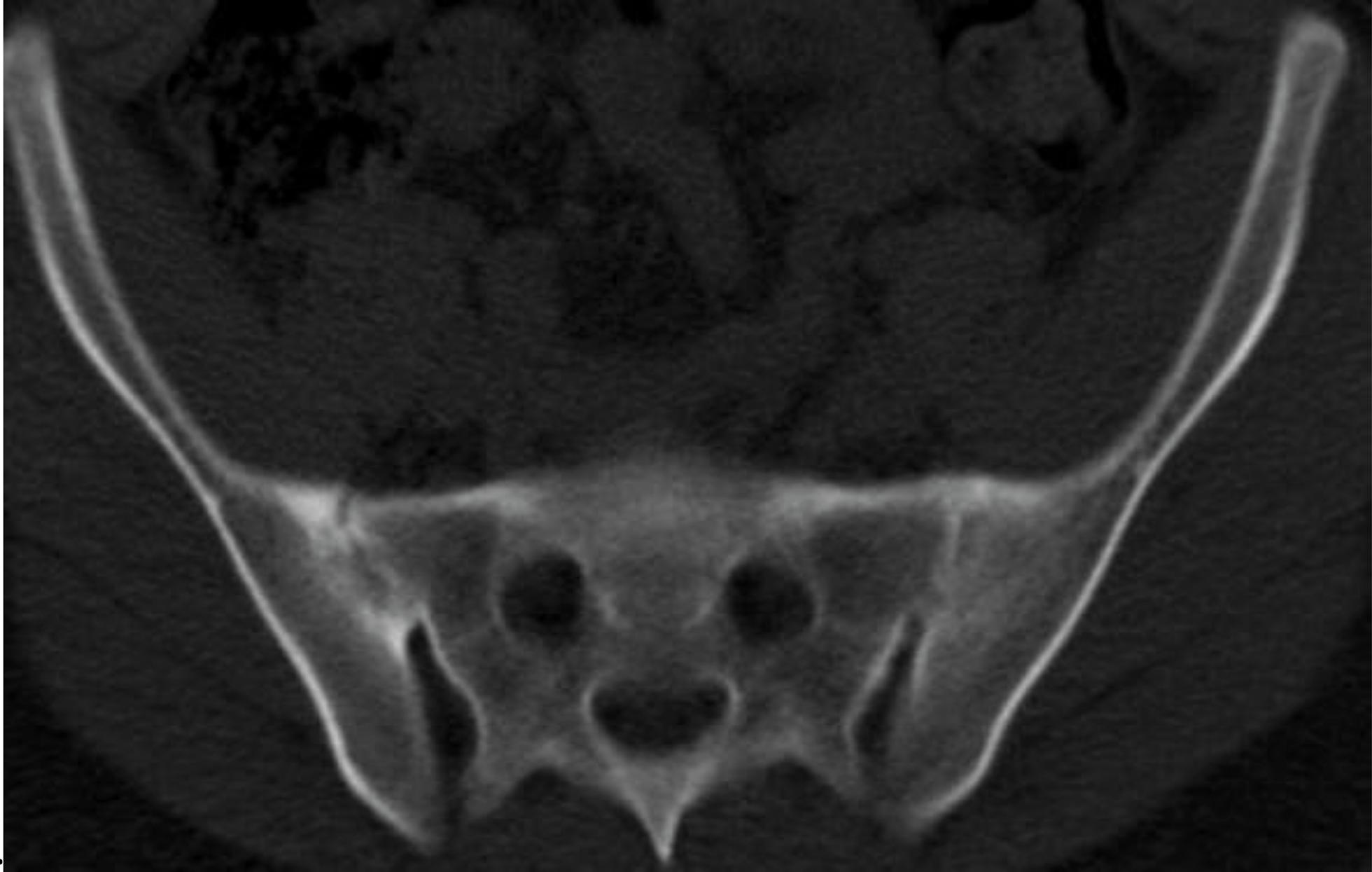
POS208
RS3PE: A Spot Diagnosis with Important Implications
May be the initial manifestation of an idiopathic rheumatic disease in elderly patients or may present as a paraneoplastic condition.
It was formerly considered as a subset of RA, but is now regarded as a distinct disease/syndrome.
While for a rheumatologist it’s a spot diagnosis, making a diagnosis remains uncertain, hindered by the lack of criteria and presence of other much common mimics.
Patient was treated with Deflazcort 12mg OD DPP-IV inhibitors were stopped Followed up after 2weeks and then planned again after 1 month.
1. Varshney AN, Singh NK. Syndrome of remitting seronegative symmetrical synovitis with pitting edema: a case series. J Postgrad Med. 2015 Jan-Mar;61 (1):38-41. doi: 10.4103/0022-3859.147038. PMID: 25511217; PMCID: PMC4944366.
Image and Bar Table 1

Image and Bar Table 2


POS209
Covid 19 Vaccine Booster Dose Hesitancy in Rheumatic Diseases
Yogesh Preet Singh1,
Vaccine hesitancy is prevalent. Appropriate steps are required to reduce the hesitancy and improve the rates of vaccination.
Image and Bar Table 1

Image and Bar Table 2

POS210
Impact of COVID 19 Pandemic on Management of Inflammatory Arthritis Among Adult Out-Patients - A Tertiary Care Centre Experience
POS211
COVID 19 Infection and Avascular Necrosis of the Hip
Image and Bar Table 1

Image and Bar Table 2

POS212
Scopes and Stains, Puzzle for the Brains: Deciphering the Diagnostic Enigma Through Histopathology
Whole-body PET CT revealed diffuse circumferential mural thickening extending from the ascending aorta to the bifurcation of common iliac arteries, including the branches of the aortic arch, indicative of large vessel vasculitis. ANA, anti-PR3/MPO ANCA, and RF, were negative, and serum IgG4 levels were normal. A final diagnosis of IgG4-related disease (possible) was made. He was treated with pulse steroids and cyclophosphamide, resulting in symptomatic improvement. He received three doses of cyclophosphamide and was lost to follow-up thereafter.
3 years later, he presented with complaints of dyspnoea on exertion, nodular swelling near the right shoulder & significant weight loss. Repeat PET CT (Figure 2) showed increased aortic thickening and FDG-avid soft tissue in the pericardium, bone marrow, and subcutaneous tissue. Bone marrow biopsy showed prominent histiocytes (CD68+) suggestive of histiocytosis. Cutaneous nodule biopsy showed diffuse infiltration with foamy histiocytes, scattered touton giant cells & emperipolesis; IgG4+ plasma cells were 7-8/HPF, IgG4:IgG ratio was <10%. BRAF mutation analysis by NGS was negative.
Clinical picture of coated aorta with soft tissue lesions in long bones and pericardium suggested Erdheim-Chester Disease (ECD), while cutaneous nodule and biopsy findings were suggestive of Rosai-Dorfman disease. Hence, a final diagnosis of overlap of Erdheim-Chester Disease with Rosai-Dorfman disease was made. He was started on steroids & azathioprine. He was advised chemotherapy for ECD, but he did not consent for the treatment.
Image and Bar Table 1

Image and Bar Table 2

POS213
“A Case of Masquerading Vasculitis”
After referral to our institution, she underwent emergency popliteal and distal artery embolectomy, but minimal thrombi could be retrieved. A follow-up angiogram showed persistent occlusion of all tibial vessels. The likely etiology was considered thromboembolic, medium vessel vasculitis (primary/ secondary vasculitis), (CTD/APS related). Two days later, progressive oedema of the left lower limb, with gangrenous changes in the toes, necessitated a fasciotomy. Despite aggressive treatment, ischemia persisted, and a below-knee amputation (BK) was performed for pain control. And over the days she had multifocal involvement of opposite leg and she also developed severe pain and progressive bluish discoloration of left 2nd and 5th fingers. CT angiogram of left UL was done which was normal.
Histopathological examination revealed medium and small vessel leucocytoclastic vasculitis with associated thrombus formation. Subsequent workup was negative for autoimmune markers (ANA, dsDNA, APS, RF, ANCA), but HLA-B51 was positive, suggesting Behcet’s disease. The patient was started on intravenous methylprednisolone pulse therapy, followed by monthly cyclophosphamide infusions Initiated on pulse dosing of methylprednisolone. 2 doses of Alprostadil infusion were given and Oral vasodilator were added.
POS214
Stiff and Ulcerated!
A 67 year old lady came with history of 8-10 months’ illness of skin lesions over lower limbs and dorsum of feet with itching. They had now ulcerated at few places and the whole area of lower 1/3rd of legs was hyperpigmented. She also had scattered skin lesions over both hands for last 15 days. Two years back she had h/o spontaneous falls while walking. This was followed by pain over low back with some stiffness which had been gradually increasing. An Anti GAD antibody was negative and she was diagnosed as Stiff Person Syndrome by a neurologist that and was managed accordingly. She had also received the first dose of RTX before 6 months along with IVIG. A biopsy from the skin lesions showed cutaneous vasculopathy with acro angiodermatitis.
While the association of Stiff Person Syndrome is known with autoimmune conditions like IDDM, vitiligo, thyroid disorders etc, there are no reports of its association with vasculitis or cutaneous vasculopathy.
Image and Bar Table 1

Image and Bar Table 2

POS215
The Midnight Intruder: A Case of Recurrent Anemia and Paroxysmal Nocturnal Hemoglobinuria
Image and Bar Table 1
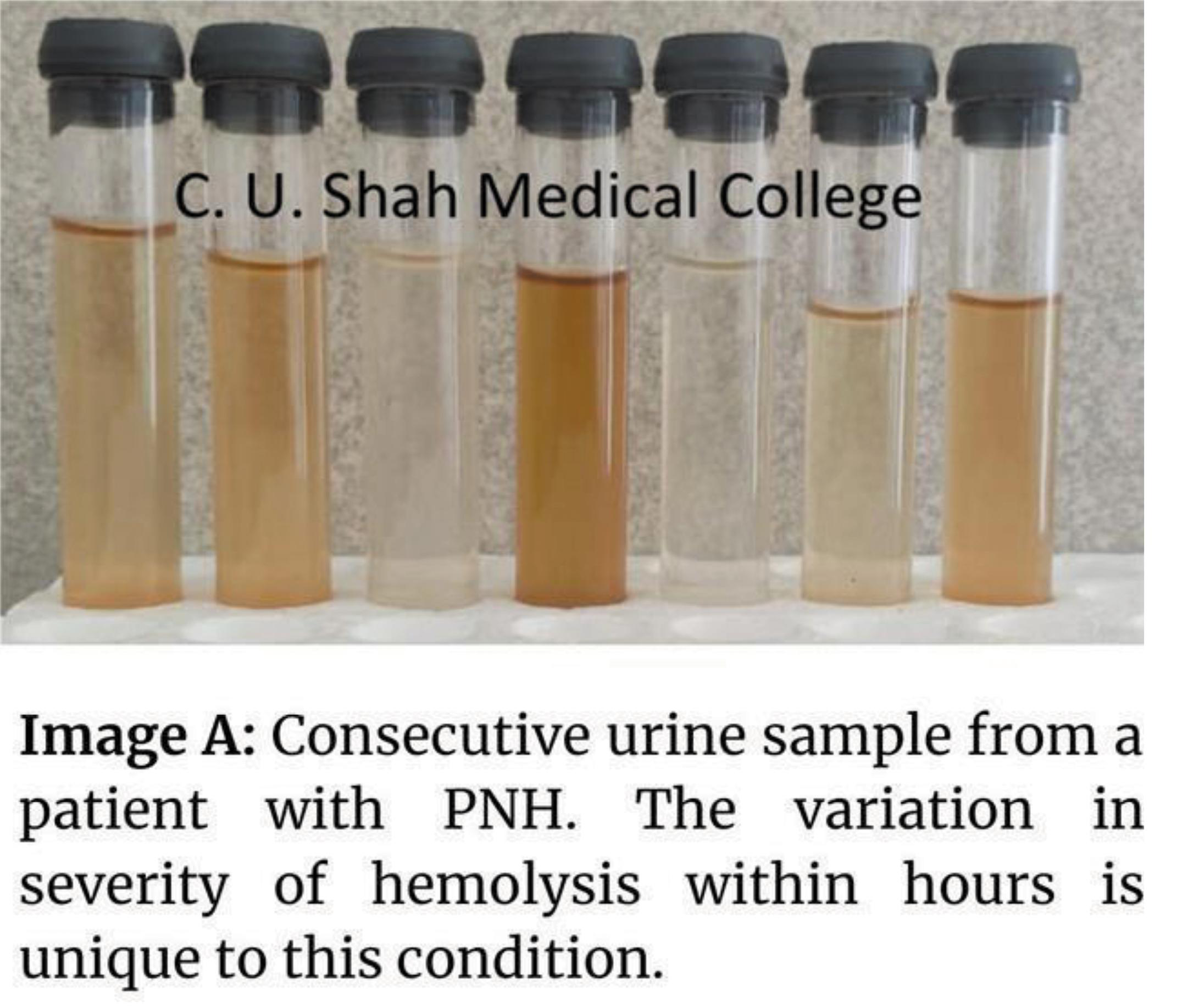
Image and Bar Table 2

POS216
Is it a Double/Triple Trouble!?
Case details
43-year-old female presented with
Skin rash/polyarthralgias for 3 months
Fever- 15 days
Seizure like activity followed by altered sensorium for 1 day
Examination revealed- DLE rash – diffuse- face, Upper limbs, back
Multiple tender joints
Patient was no oriented to time/place/person, Neck Rigidity present
Otherwise, no focal neurological deficet.
Suspected SLE with Acute meningoencephalitis/CNS vasculitis
Started on Dexamethasone, Antibiotics, Antivirals
Intubated in view of worsening sensorium.
Brain Imaging done-
Suggested-Lacunar infarcts in white matter of bilateral fronto-parietal lobes.
Altered signal intensity involving the gyri of left frontal, parietal, temporal, occipital lobes and grey white matter of left temporal
CNS Vasculitis?
Investigations-Mild Anemia, Leukocytosis, ANA +4 (Nucleolar), dsDNA- positive by ELISA,
CSF Examination-
Opening pressure-15 cm H20
Cells-100 (100% Lymphocytes)
Protein-153
Glucose-64
CSF Biofire-Cryptococcus Neoformans
CrAg -Positive
Indian Ink- Budding Yeast cells
Diagnosed as Cryptococcal meningoencephalitis
Also Blood cultures were positive for Cryptococcus neoformans
Started on Flucytosine and Liposomal Amphotericin B
Post 7 days of Antifungals too, no improvement in the Sensorium
Developed Ventilator associated Pneumonia-Hiked antibiotics to Polymyxin B
Patient also developed new onset fever spikes with worsening Anaemia/Thrombocytopenia
Considered HLH/ Drug related- Flucytosine
Stopped Flucytosine and started high dose Fluconazole.
Bone marrow aspiration/Biopsy done-to R/O HLH- Suggested HLH
Repeat CSF Analysis was done as patient had persistent Altered behaviour
Glucose-48
Protein-111
Ultra Gene xpert –ve
CSF cultures- Cryptococcus neoformans
Lymphocyte subset Analysis- NK cell Activity 1.4% (2-4)
Immunoglobulin levels- Normal
Eventually Patient Succumbed and Full Body Autopsy Done after Prior consent
Brain Biopsy Revealed- Meningitis with budding yeast cells
Spleen and Liver- Granulomas
Lymph nodes- Para-aortic
AFB +ve
Also Yeast cells +
Also CSF cultures collected Post mortem – growth of MTB
Growth of Highly resistant isolate of Acinetobacter baumani
Post-Mortem Diagnosis
SLE with DLE, Arthritis- Steroid Naive
Disseminated Tuberculosis (Tb meningitis with endarteritis, Splenic, Liver, Lymphadenitis
Disseminated Cryptococcosis (Meningoencephalitis, Lymphadenitis, Cryptococcemia)
Acinetobacter Septicemia
Presence of such infections in an immunocompetent patient – with co- existent autoimmunity is a rarity.
Immunological basis for this phenomenon – to be studied further
Image and Bar Table 1

Image and Bar Table 2

POS217
Pediatric Cardiac Sarcoidosis: A Case Report
6 months later there was pain abdomen with non productive cough, pain abdomen subsided with conservative management.
Cough persisted which is managed by bronchodilators which gave mild relief.
In April 2024 there was increase in frequency of cough, scanty mucoid expectoration with mild exertional dyspnoea, on examination mild wheeze present and Chest Xray normal but symptoms persisted,
Echo reveals Grade 1 RV diastolic dysfunction, sinus tachycardia, sinus arrhythmia noted,
Cardiac MRI showed on delayed enhancement imaging and diffuse transmural enhancement of lateral wall, patchy nodular enhancement of septum, Enlarged mediastinal lymph nodes are seen in left paraaortic, pre tracheal and sub carinal regions.
PET CT showed Diffuse & patchy hypermetabolic ill-defined asymmetric soft tissue thickenings involving basal septum & lateral wall of left ventricle suggest the possibility of granulomatous disease). Metabolically active multiple subcentimetric & enlarged mediastinal & bilateral hilar lymph nodes likely to be granulomatous in nature.
Later confirmed by subcarinal lymphnode biopsy
Ocular examination, Serum ACE levels were normal.
Treatment initiated with oral steroid, subcutaneous methotrexate, furosemide, enalapril follow up.
POS218
Tale of Jaundice in A Pregnant SLE Patient
POS219
The Gut Feeling: A Case Series on Lupus Enteritis
Image and Bar Table 1

Image and Bar Table 2

POS220
IgG4-Related Disease: Isolated Bone Involvement-A Diagnostic Challenge
Image and Bar Table 1
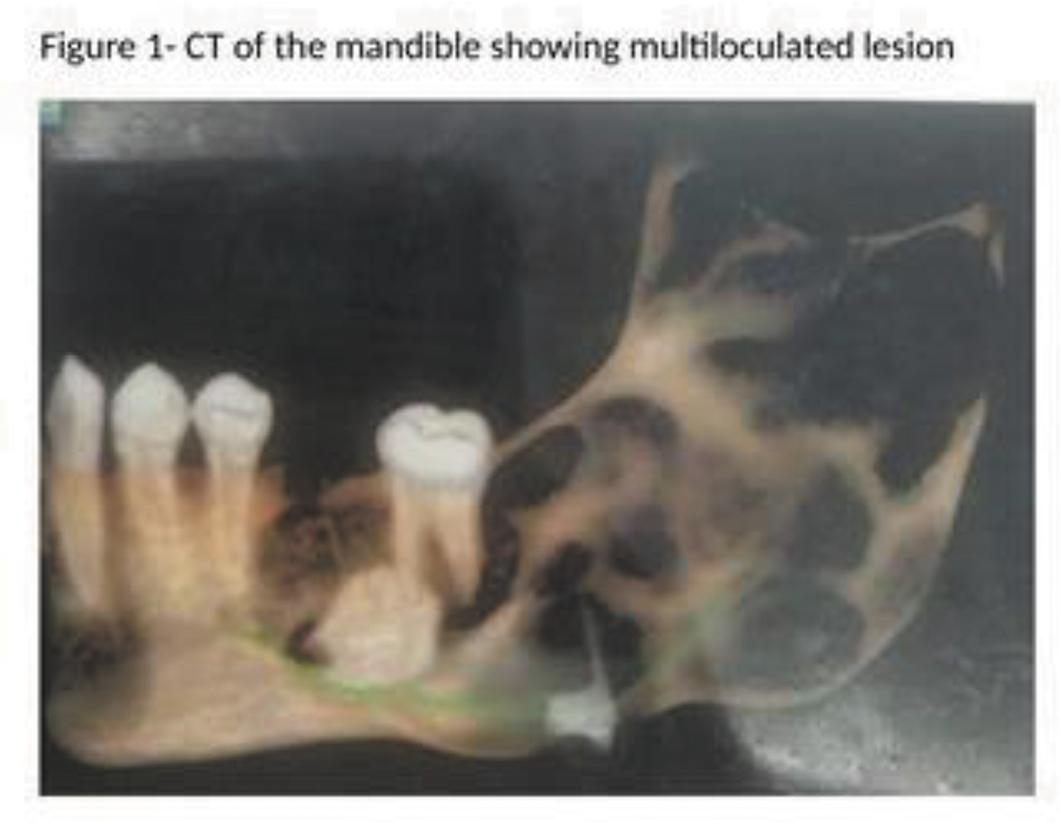
Image and Bar Table 2

POS221
A Rare Case of Altered Sensorium in a Patient With SLE
Pain abdomen was radiating to left shoulder and used to aggravate on taking deep breaths. There was no history of fever, ATT intake and pregnancy loss.
Differentials of SLE with CNS Lupus or SLE with secondary APS was kept.
MRI brain with contrast was done which showed Left sigmoid sinus and transverse sinus thrombosis.
ANA was positive with end titre of 1:1000 and nuclear homogenous pattern. Anti DS DNA was raised. C3, C4 was low.
APLA profile was negative.
Thrombophilia profile showed Protein S deficiency.
2D echo did not show any evidence of clot or vegetation.
The clinical picture was consistent with SLE associated Thrombocytopenia/CNS lupus and Venous Thrombosis secondary to thrombophilia disorder.
Patient was started on pulse steroid, Mycophenolate mofetil and anticoagulation with Warfarin overlapped with Low molecular weight heparin was initiated.
Patient showed gradual improvement in sensorium and her Platelet counts improved to 90, 000 over 2 weeks.
On repeat thrombophilia profile testing after 3 months it showed persistent Protein S deficiency.
POS222
Silent Intruder: Osteomyelitis Due to Non-Tuberculous Mycobacterium in Systemic Lupus Erythematosus
Hematology showed Total count of 13300 cells/cu.mm, Lymphocyte: 5.4%, RBC Count: 3.57ml/cu.mm, Haemoglobin: 9.4g/dl, ESR:99mm/hr, Platelets:31200/cu.mm, INR:1.25, Creatinine:1.5mg/dl, Procalcitonin: 0.234 ng/ml, Urine spot PCR- 2.7mg.
MRI image of the right knee revealed double line sign with central fatty marrow signal, suggestive of medullary bone infarct. Focal thick linear lytic area with internal fluid noted in lateral part of lateral femoral condyle with focal cortical defect, fluid within bone communicating with joint fluid through cortical defect - suggestive of osteomyelitis in the distal femur. CT scan was also suggestive of osteomyelitis of right distal femur.
The culture sensitivity test of the pus from the open biopsy identified atypical mycobacteria- Rapidly growing non tuberculous mycobacterium including Mycobacterium fortuitum, M.chelonae, M.abscesses that are sensitive to Meropenem, Azithromycin, Clofazimine, and Minocycline. These drugs were administered. Currently, the patient remains on steroids, Mycophenolate Mofetil, Hydroxychloroquine, antibiotics, and Warfarin and is recovering well.
Identification of rapidly growing NTM from biopsy culture highlights the importance of tissue diagnosis. Immunocompromised hosts like lupus patients are susceptible to opportunistic infections. Managing complex SLE cases requires a multidisciplinary approach involving rheumatologists, infectious disease specialists.
Acute monoarthritis in knee is considered as septic arthritis unless proved otherwise. The patient required a multifaceted treatment approach, involving continued use of immunosuppressive medications (e.g., steroids, mycophenolate mofetil) for SLE control, alongside antibiotics to treat the NTM infection and anticoagulation for her APLA and DVT. This highlights the complexity of managing overlapping diseases.
Identifying nontuberculous mycobacteria and tailored antibiotics emphasise considering atypical infections in immunocompromised patients.
Image and Bar Table 1

Image and Bar Table 2

POS223
“Crossroads of Complexity: Navigating through A Case of Systemic Lupus Erythematosus and the Rare Challenge of Hydropneumothorax”
She then re-presented to us within 2 weeks with a history of sudden onset breathlessness for 3 days. She denied history of fever, cough, expectoration, chest pain. She was tachypneic with SpO2 94% on room air and reduced air entry in bilateral bases. The chest Xray revealed bilateral CP angle blunting. 2Decho suggestive of mild global LV hypokinesia, LVEF 50%, no Pericardial effusion. An HRCT chest subsequently revealed moderate right pleural effusion with moderate left hydropneumothorax.
A pulmonary medicine review was sought, ICD inserted, and pleural fluid was analyzed. It was turbid, white-yellow, with 1,15, 690 cells, Neutrophils:36%, Lymphocytes:0.3%, Monocytes/macrophages: 63.5%, LDH: 56,387, ADA:275. Pleural fluid gram stain, Gene-Xpert, AFB, culture, malignant cytology were all negative. Pleural fluid Triglycerides were 62, and Cholesterol <50. She was started on empirical ATT suspecting tubercular empyema complicated by Pneumothorax.
Image and Bar Table 1
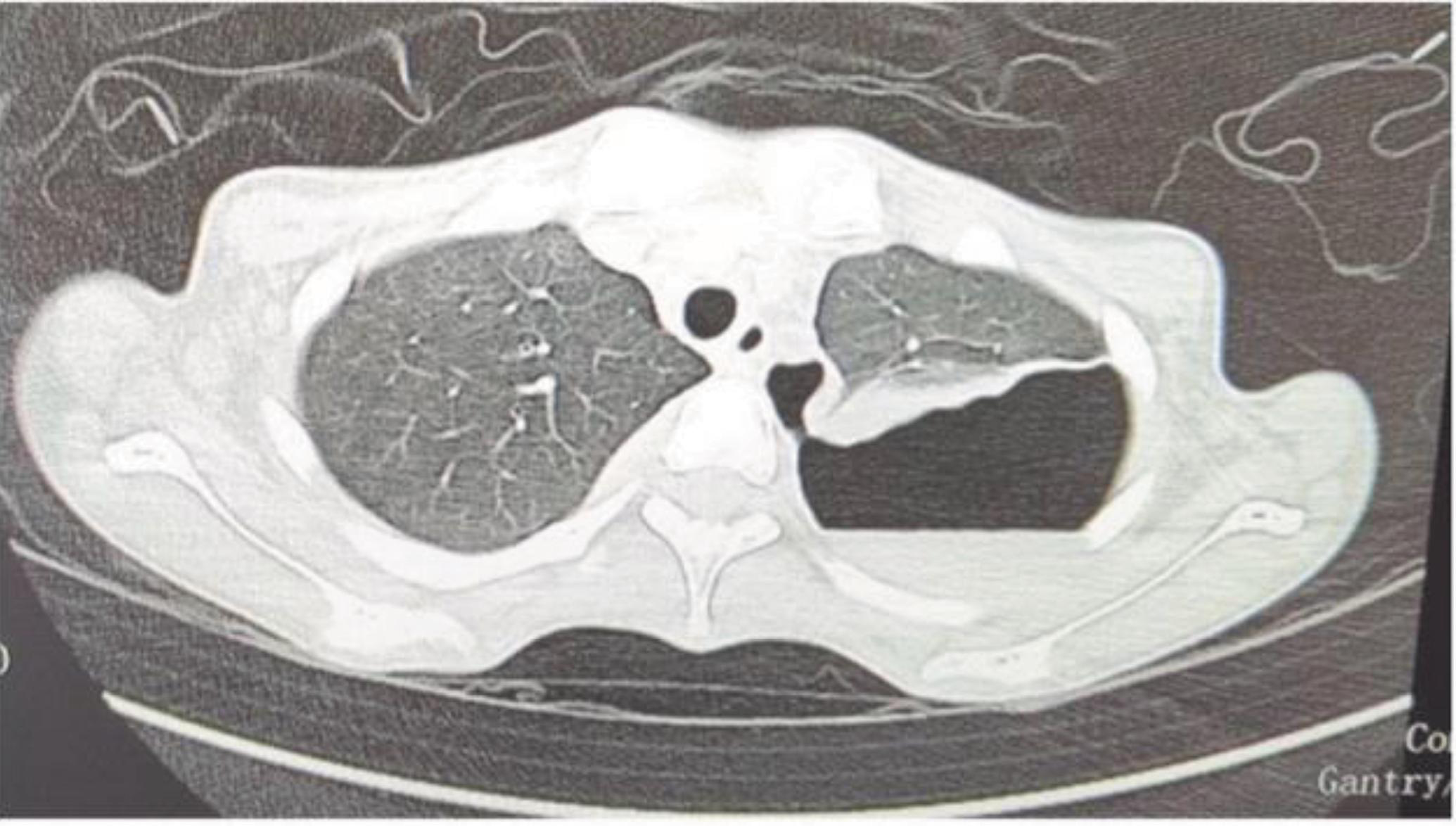
POS224
Verrucous DLE As Rare Presentation Of SLE: Wart I See, What Is It?
Image and Bar Table 1

Image and Bar Table 2

POS225
An Interplay Between Infection and Auto Immunity in A Case of SLE
Dr Nikhil r #, Dr Ramaswamy Subramanian, Dr Shivaprasad, Dr mahabaleshwar mamadapur.
Department of Clinical immunology and Rheumatology, JSS Medical College, Mysuru.
JSS Academy of Higher Education and Research.
Duke criteria 2023 for infective endocarditis can assist to differentiate between infective and Libman–Sacks endocarditis (2).
Decreased white blood cell count, elevated CRP, and the presence of antiphospholipid antibodies all increase the likelihood of Libman–Sacks endocarditis (2).
Infection is the most common cause of SLE flare/ MAS. A vicious cycle between MAS-triggered infection or infection-triggered MAS can co-exist. Early identification will lead to a change in the approach to disease and its outcome.
Image and Bar Table 1

POS226
Fever of Unknown Origin, is It Anca Associated Vasculitis or Yet to Be Known?
POS227
The Blurred Lines between Lupus and Fungus: A Diagnostic Challenge
A 49 year old female patient came to our Out-Patient Department with a history of erythematous, itchy rash over both her forearms for the past 2 months. She was given anti-fungal cream (Clotrimazole) by her previous physician. And it was ineffective though applied daily for the past few months. No history of exposure to a contact or any precipitating agent were mentioned for these rashes. She had no other significant past medical history.
On examination, there were ill-defined annular erythematous patches over both her forearms, warmth and tenderness was elicited on palpation. Rest of the skin examination in other parts was normal, no nail changes, no abnormality on systemic examination.
Given the clinical history and morphology of the rash, a presumptive “Tinea Corporis” diagnosis was made. A skin biopsy was taken from the forearm, and Periodic Acid Schiff (PAS) stain was used which revealed thickened basement membrane and no fungal elements. The biopsy showed hyperkeratosis, and features of interface dermatitis, suggestive of Lupus Erythematosus (LE) rash. Furthermore, Ana by Hep-2 method was 3+ Positive and antibody to Ro-52 was also positive.
Hence, the diagnosis of “Sub-Acute Cutaneous Lupus Erythematosus (SCLE) was made, and she was started on topical steroids and calcineurin inhibitors, and on subsequent follow-up, she had good response with minimal inflammation only.
Sub-acute lupus erythematosus is an entity of cutaneous lupus erythematosus, and it can present as annular, polycyclic, or papulo-squamous eruptions. It can mimic a number of other cutaneous manifestations, tinea corporis, dermatomyositis, erythema annulare centrifugum, drug eruptions, lichen planus, or psoriasis. In our case, as the patient did not mention any history of exacerbation on sun exposure, and the clinical examination was convincing enough to rule in fungal infection in the first place. The absence of systemic features in most cases of SCLE further defer the diagnosis, however, we should consider the possibility of cutaneous lupus in cases which do not improve despite giving antifungals for a given period of time. Since there are striking similarities between these cutaneous manifestations, it is a challenge for the physicians to arrive at the final diagnosis.
Image and Bar Table 1

POS228
Double Trouble: Malignancy and Systemic Rheumatic Diseases. A Single-Center Retrospective Observational Study From South India
Systemic rheumatic diseases preceded the onset of malignancy in 51.3%, after in 31%, and co-occurred in 17.3% of cases. Among patients with malignancy occurring after the onset of rheumatic disease, the most commonly received therapy was combination DMARD therapy (methotrexate and hydroxychloroquine) in 60% followed by mycophenolate mofetil in12.5% of cases. Mortality was observed in 2 patients.
1. Geng Z, Ye C, Zhu X. Malignancies in systemic rheumatic diseases: A mini-review. Front Immunol. 2023 Feb 28;14:1095526.
2. Bojinca V, Janta I. Rheumatic diseases and malignancies. Maedica (Bucur). 2012 Dec;7 (4):364-71.
3. Z. Szekanecz et al. Eight pillars of onco- rheumatology: crossroads between malignancies and musculoskeletal diseases. Autoimmun Rev (2020).
4. Wen, J., Ouyang, H., Yang, R. et al. Malignancy dominated with rheumatic manifestations: A retrospective single- center analysis. Sci Rep 8, 1786 (2018).
Image and Bar Table 1

Image and Bar Table 2
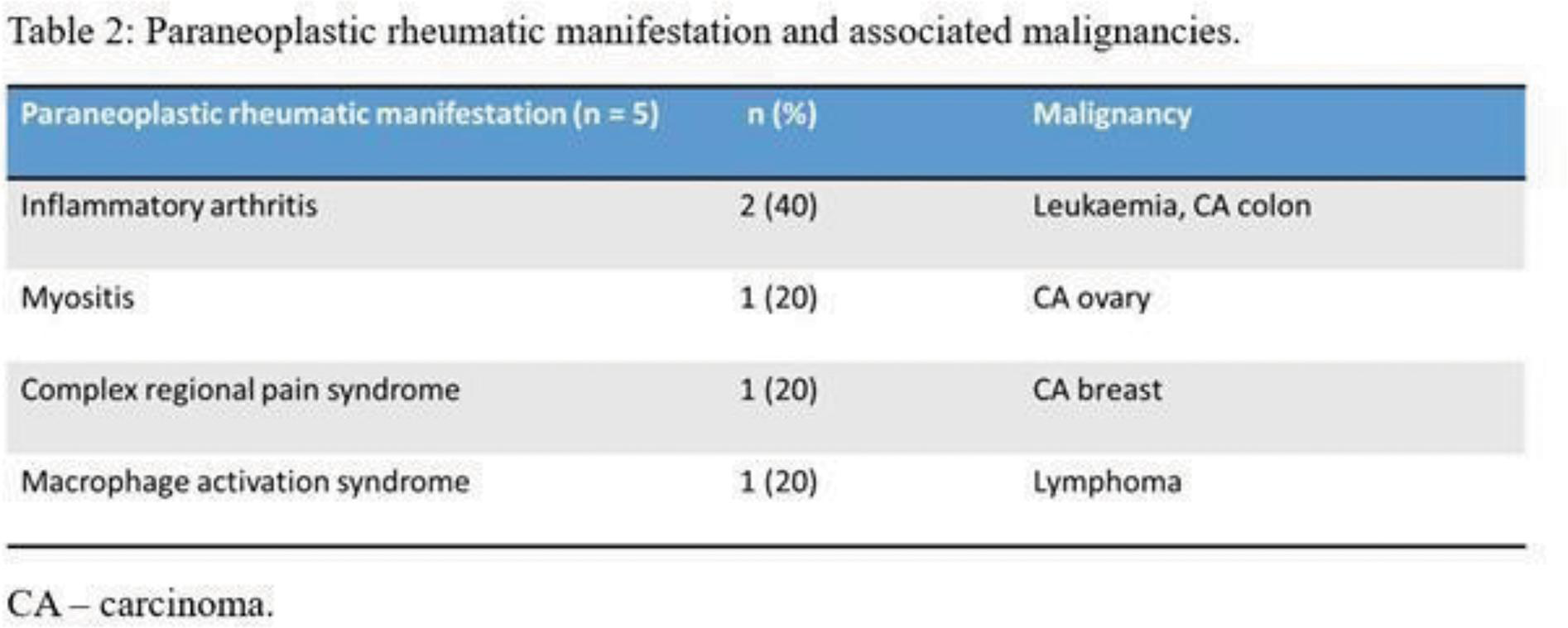
POS229
Xanthoma - A Masquerader of Gouty Tophi
Urate tophi are a common differential for xanthomas.
Xanthomas are treated with lipid lowering therapy – sometimes a combination of statin, ezetimibe, PCSK9-i are tried. Lipoprotein apheresis can also be considered in some resistant cases of familial hypercholesterolemia.
POS230
Immunogenetic Profiling of HLA DR/DQ Alleles in Sjögren’s Syndrome with and without Distal Renal Tubular Acidosis
POS231
Study of Agreement Between Line Immunoassay and Enzyme Linked Immunosorbent Assay for Detection of Anti-dsDNA Antibodies
POS232
MicroRNA-seq Transcriptomic Profiling Highlights Distinct miRNA Expression Dynamics in Juvenile and Adult-Onset Systemic Sclerosis
Heatmap for significantly expressed miRNAs (jSSc)

miRNA clustergram (adult onset SSc)

POS233
FcγRIIB Polymorphism In SLE: Association with Clinical Phenotypes, Disease Activity and Levels of Cytokines (IL6, IL17 and TNFα).
Image and Bar Table 1

Image and Bar Table 2

POS234
Serum Based Clinical NMR Metabolomics Reveals Altered Sugar Metabolism in Systemic Sclerosis and Mannose-To-Myoinositol Ratio (MMR) as Potential Diagnostic Biomarker
Gurvinder Singh1, Sakir Ahmed2, Durgesh Dubey3, Mohit Kumar Rai4, Atul Rawat5, Dinesh Kumar6,
Image and Bar Table 1

POS235
Could Isolated Anti-Ro 52 be a Harbinger of Occult Inflammatory Myositis? A Single Centre Experience
1. Clinical Significance of Different Profiles of anti-Ro Antibodies in Connective Tissue Diseases Journal of Immunology Research Volume 2023, Article ID 9195157
2. Myositis specific antibodies are associated with isolated anti-Ro-52 associated interstitial lung disease. Rheumatology 2022;61:1083–1091. Advance Access publication 15 June 2021.
Image and Bar Table 1

Image and Bar Table 2
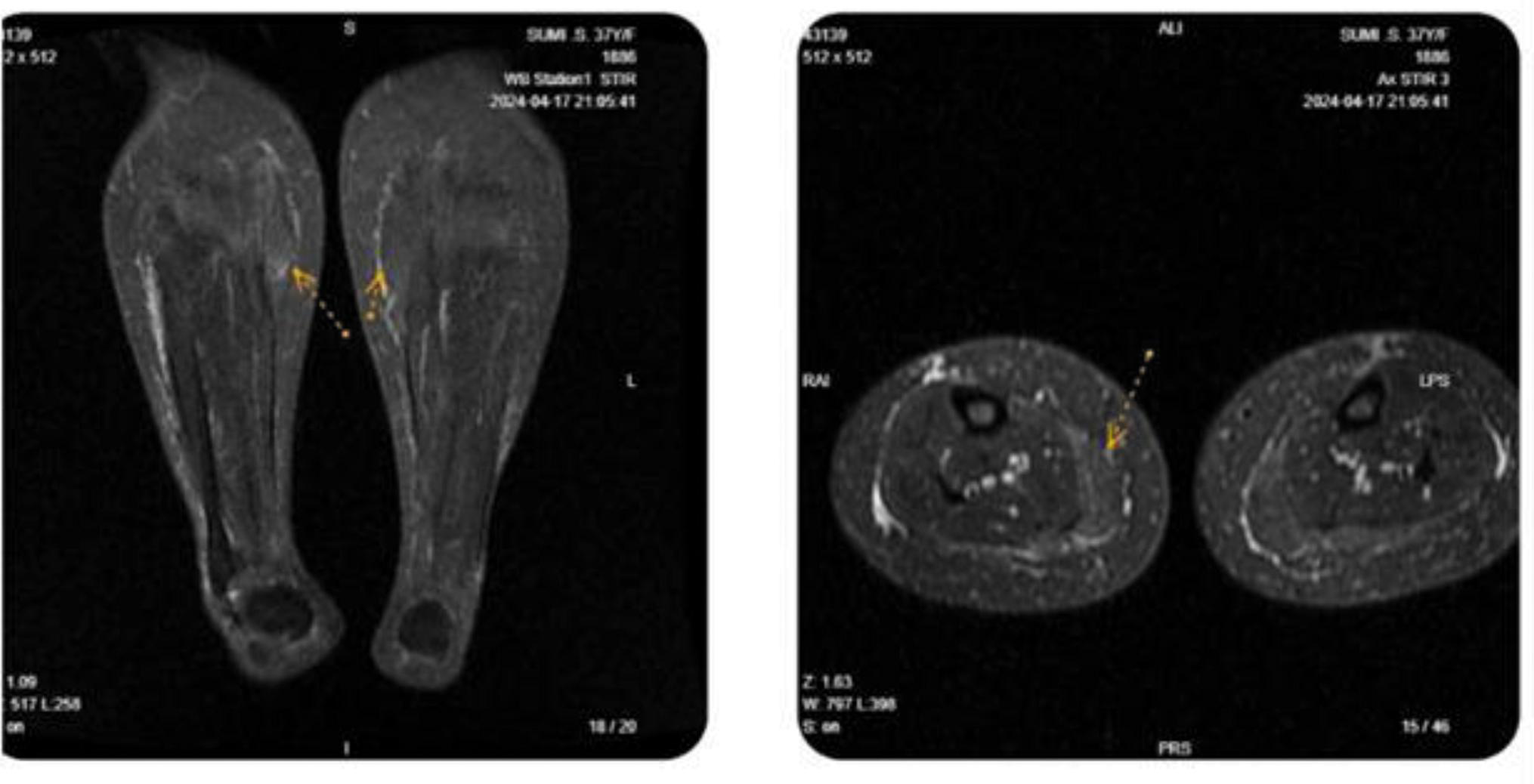
POS236
Macrophage Subsets in Patients with Active Takayasu Arteritis Compared with Healthy Controls, and Longitudinal Changes Following Immunosuppressive Therapy - A Cohort Study
Image and Bar Table 1

POS237
The Matricellular Protein Mindin Induces a Pro-Inflammatory Response in Fibroblasts to Manifest Dermal Fibrosis in Scleroderma
POS238
Role of Urinary Exosomal Micro-RNA in Lupus Nephritis
POS239
Soluble TNFRII in Lupus Nephritis as a Biomarker of Disease Activity and Treatment Response
Similarly, baseline sTNFRII (pg/ml) was significantly higher in AN group as compared to ANR, HC and DC (p-value <0.05). At baseline, sTNFRII also showed good correlation with urinary protein:creatinine ratio (r=0.5; p-value<0.001), rSLEDAI (r=0.4, p-value <0.05) and SLEDAI (r=0.4, p-value <0.05).
Both sTNFRII and uTNFRII could differentiate between AN and ANR groups (ROC analysis – sTNFRII (AUC=0.8), uTNFRII (AUC=0.6), C3 (AUC=0.6), C4 (AUC=0.37) and anti-ds DNA antibodies (AUC=0.64) - Figure1).
On follow-up, both uTNFRII and sTNFRII showed significant decrease in AN group at 3, 6, 9 and 12 months as compared to baseline (Table1).
Image and Bar Table 1
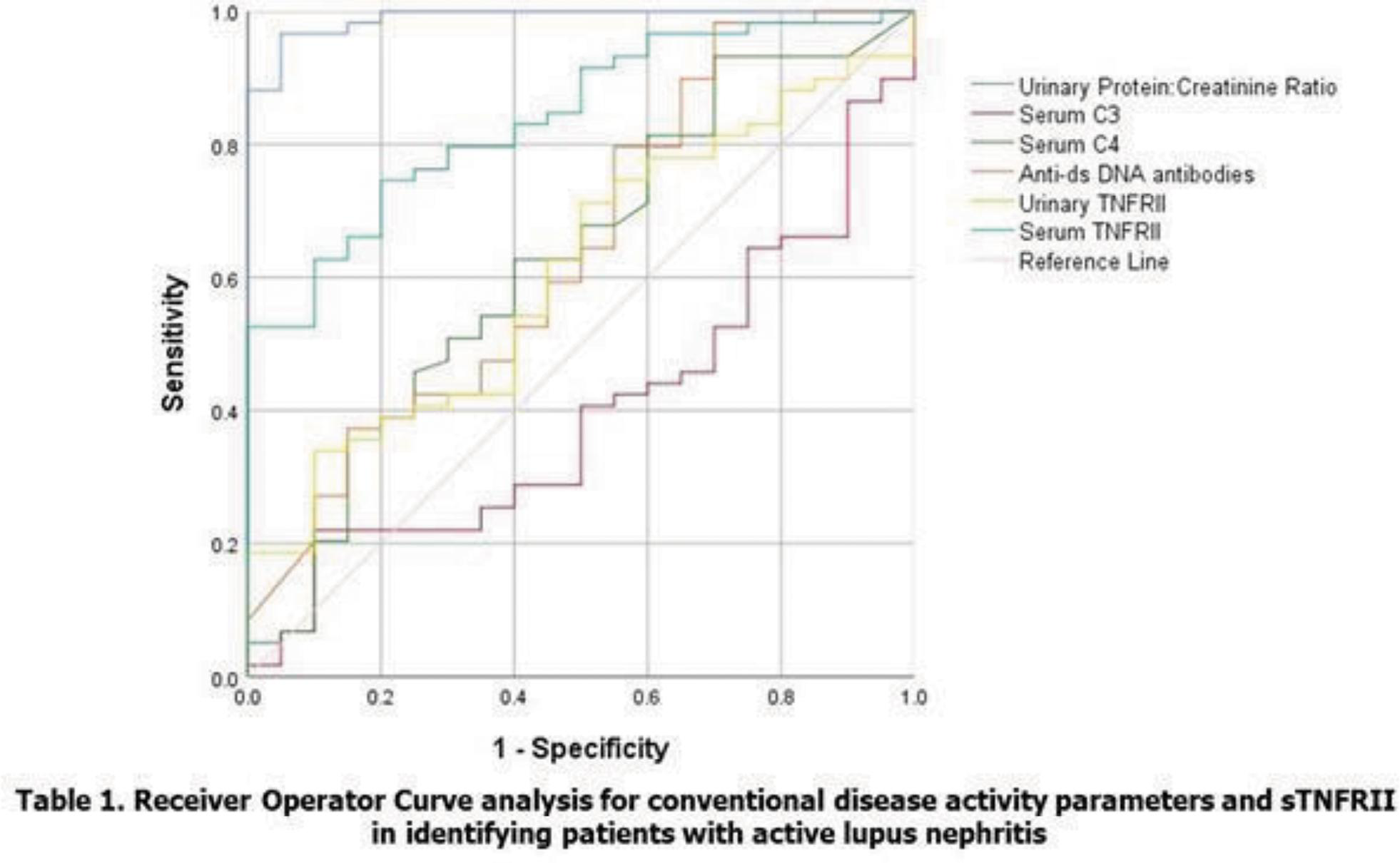
Image and Bar Table 2

POS240
Role of Peptide Disitertide and Curcumin-Loaded Double Nanoemulsion in Epithelial-to-Mesenchymal Transition to Ameliorate Peritoneal Fibrosis in In-vitro and Peritoneal Dialysis Rat Model
1. Zhao, Jun-Li, et al. “Curcumin suppresses epithelial-to-mesenchymal transition of peritoneal mesothelial cells (HMrSV5) through regulation of transforming growth factor-activated kinase 1 (TAK1).” Cellular & molecular biology letters 24 (2019): 1-13.
Image and Bar Table 1

Image and Bar Table 2

POS241
Serial Changes in P-Glycoprotein Expression on Peripheral Blood Lymphocytes from Patients with Active Systemic Lupus Erythematosus Following Immunosuppressive Therapy – A Longitudinal Study
To compare the change in expression and function of p-gp and MRP1 before and 3 months after treatment.
Image and Bar Table 1
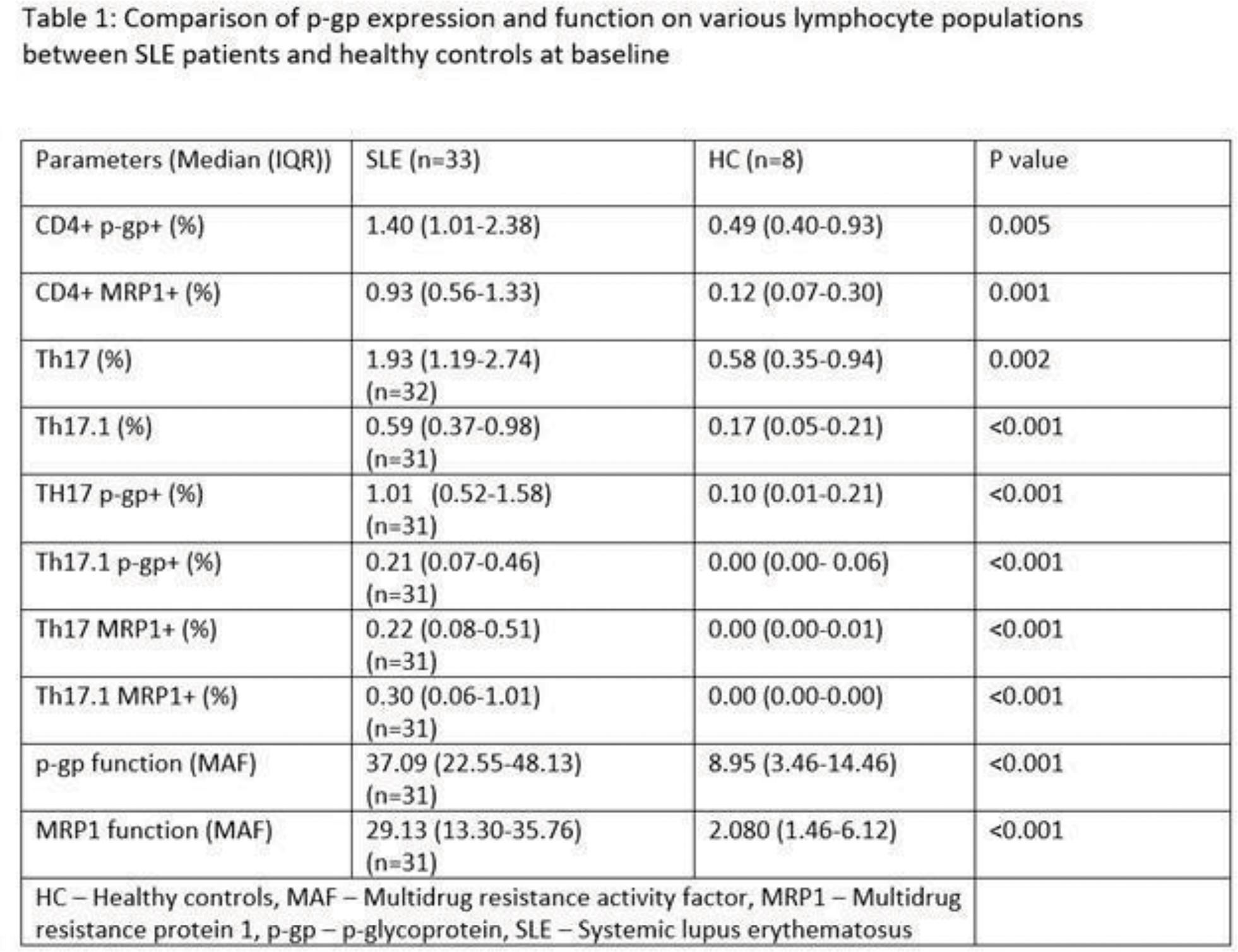
Image and Bar Table 2

POS242
IL18, Marker of Inflammasome Activation, As A Predictor of Nephritis in Systemic Lupus Erythematosus
IL18 levels were determined in serum and urine using total IL18 ELISA (R&D Systems, MN, USA) and is expressed as pg/ml. Statistical analysis was performed using Graph Pad Prism 9. Data is presented as mean ± SD or as median (range). Correlation analysis was done using Spearman correlation.
The median serum IL18 levels in patients with SLE were higher than HC (1545 Vs 379; p<0.001) and urinary IL18 levels were also higher in patients (209 vs 173; p<0.001). Serum IL18 levels were higher in patients with nephritis than without nephritis (1586 Vs 1465, p<0.05).
Serum IL18 correlated positively, with SLEDAI (r= 0.28, p <0.01) and negatively with C3 (r=-0.301, p<0.01). Urinary IL18 levels had positive correlation with serum IL18 levels (r=0.11, p<0.01) and with proteinuria (r= 0.23, p<0.05). On multivariable logistic regression, younger age (0.963, 0.9265 to 0.9991) and serum IL18 levels (1.412, 1.085 to 1.910) were predictors of nephritis at baseline.
Image and Bar Table 1

Image and Bar Table 2
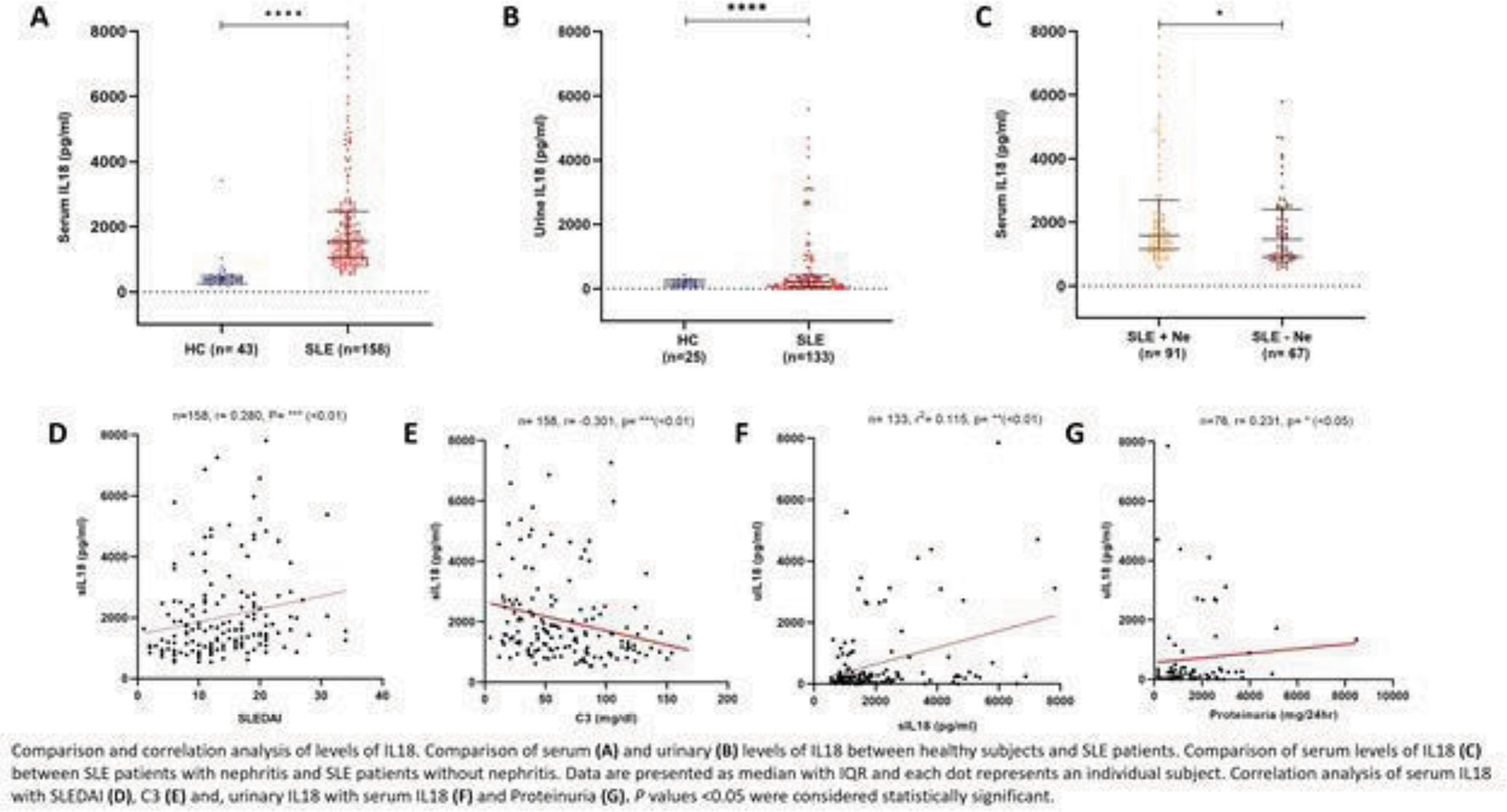
POS243
Analysis of the Performances of ACR, SLICC and EULAR/ACR 2019 Classification Criteria in Childhood Onset Systemic Lupus Erythematosus in A Tertiary Care Centre in South India
Image and Bar Table 1

Image and Bar Table 2

POS244
A Retrospective Study of Clinical Characteristics, Serological and Treatment of Male SLE Patients in India
Ethical consent was taken wide letter no IEC Reg no 54/2024 AH RR
POS245
Phase 2 Safety and Efficacy of Subcutaneous (S.C.) Dose Ianalumab (VAY736; Anti-BAFFR mAb MAb) Administered Every 4 Weeks up to 48 Weeks in Patients with Systemic Lupus Erythematosus (SLE)
Image and Bar Table 1

Image and Bar Table 2

POS246
Ocular Manifestations of Systemic Lupus Erythematosus (SLE): Results from An Institutional SLE Registry
Image and Bar Table 1
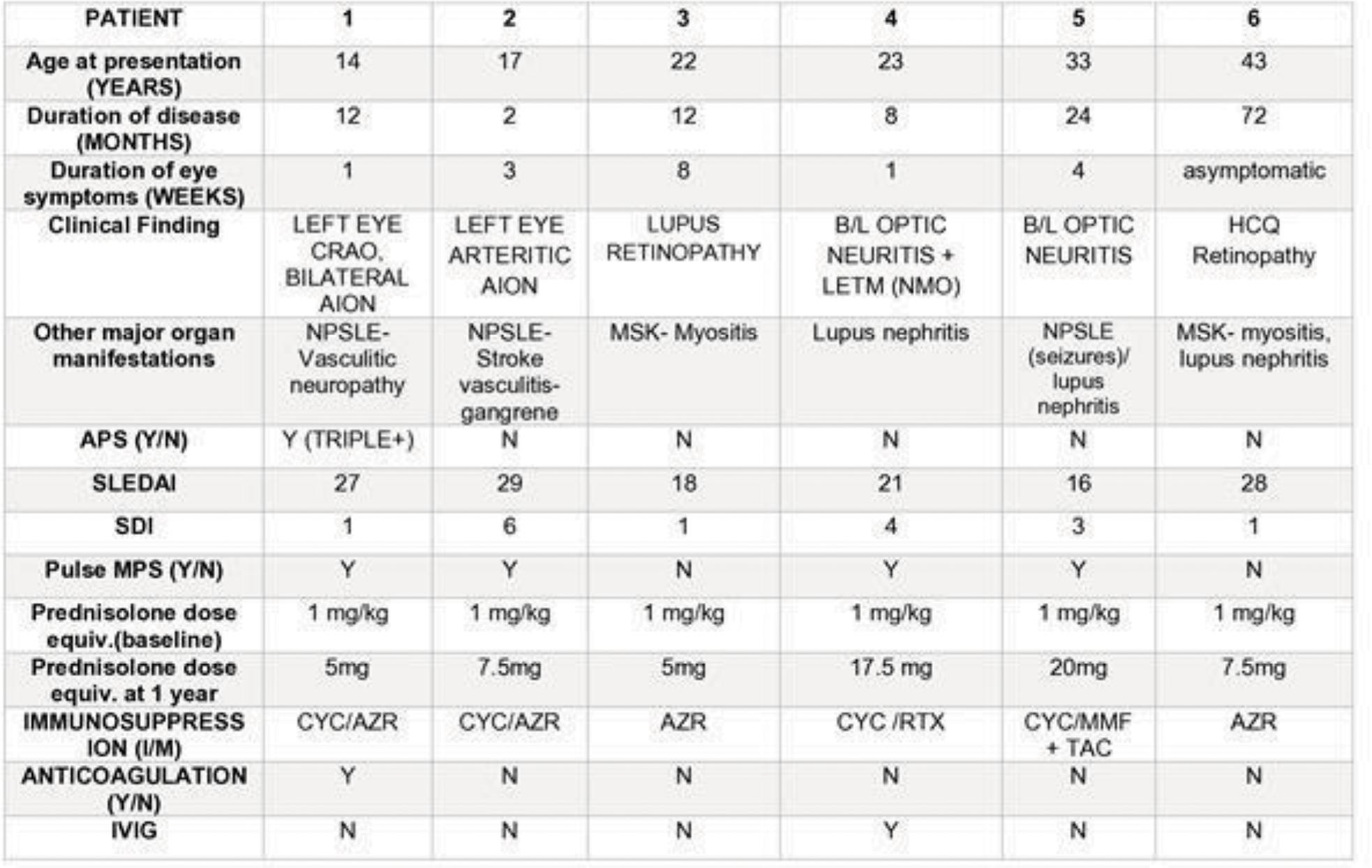
Image and Bar Table 2
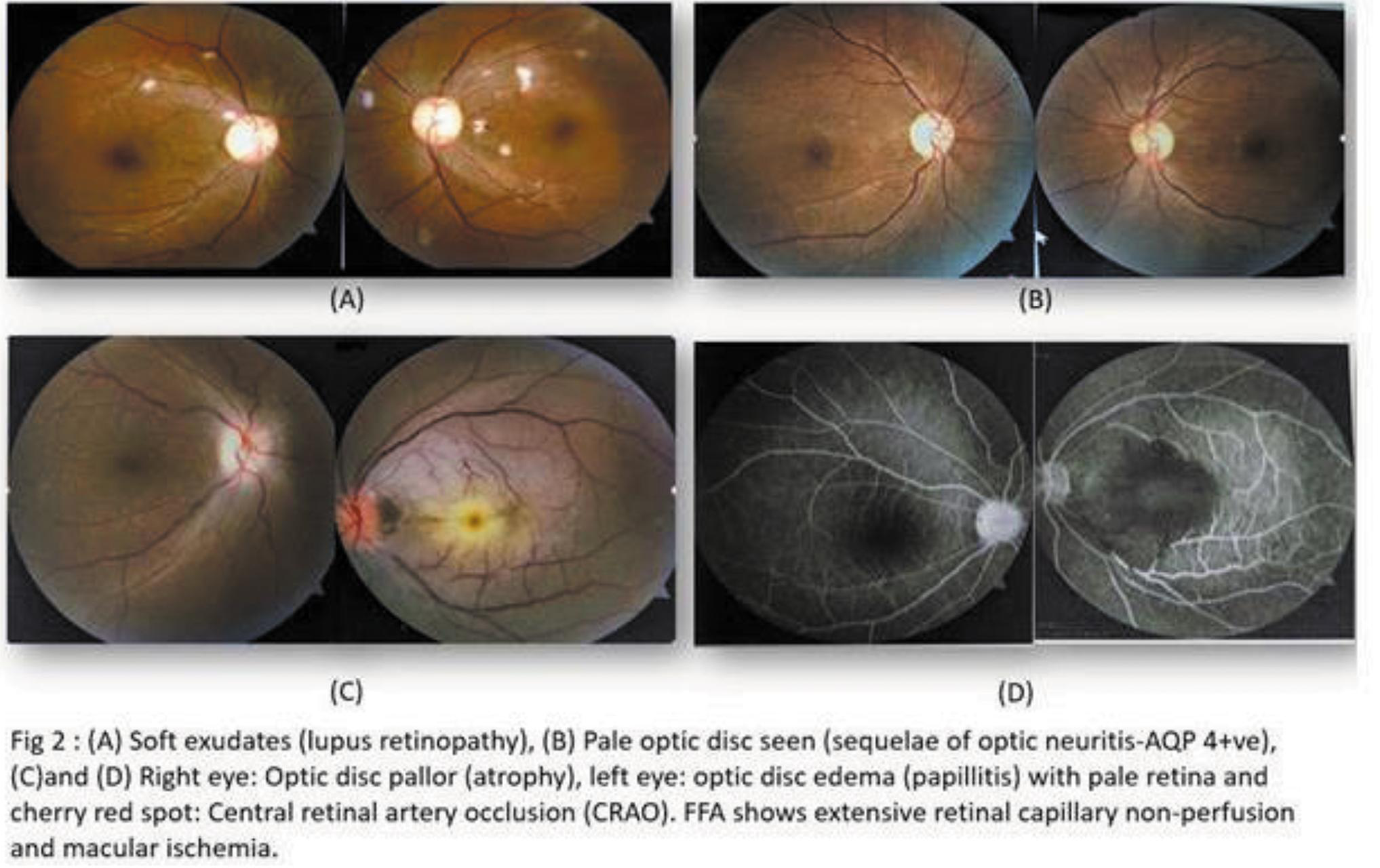
POS247
Sleep Quality in Systemic Lupus Erythematosus
Image and Bar Table 1

Image and Bar Table 2
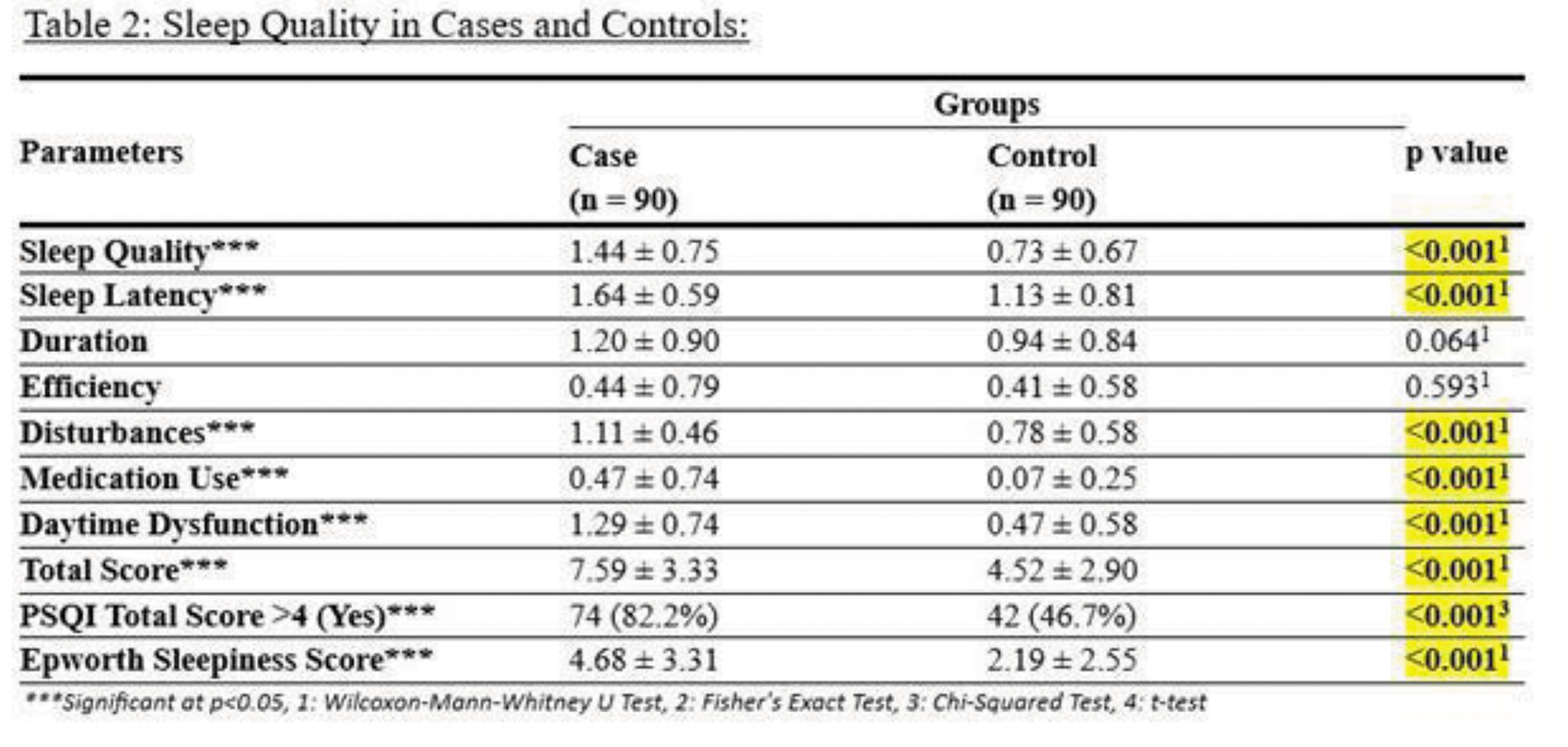
POS248
Profile of Indoor Patients of Lupus Presenting to A Municipal Hospital
Septicemia: 4
Pneumonia and URTI: 9 AGE/Gastritis: 4 UTI: 3 TB: 2 Oral candidiasis: 2
Infectious agents isolated were:
Acinetobacter baumannii: 2 Salmonella typhi: 1 Mycobacterium tuberculosis: 2 Pseudomonas aeruginosa: 2 Candida albicans: 1 Escherichi coli: 2 MRSA: 1 Enterococcus faecalis: 2 Aspergillosis fumigatum: 1 CMV: 1
Causes of death, Total 9:
Infection: Sepsis/Septicemia/Pneumonia/Pneumothorax: 6
Lupus related: Renal: 5, 1 DAH, 1 lupus pneumonitis
Our data of indoor patients matched that reported elsewhere from our country and the West (although cardiovascular disease and infections were more common in one). Our patients had more co-morbidities and less of major organ involvement.
Image and Bar Table 1
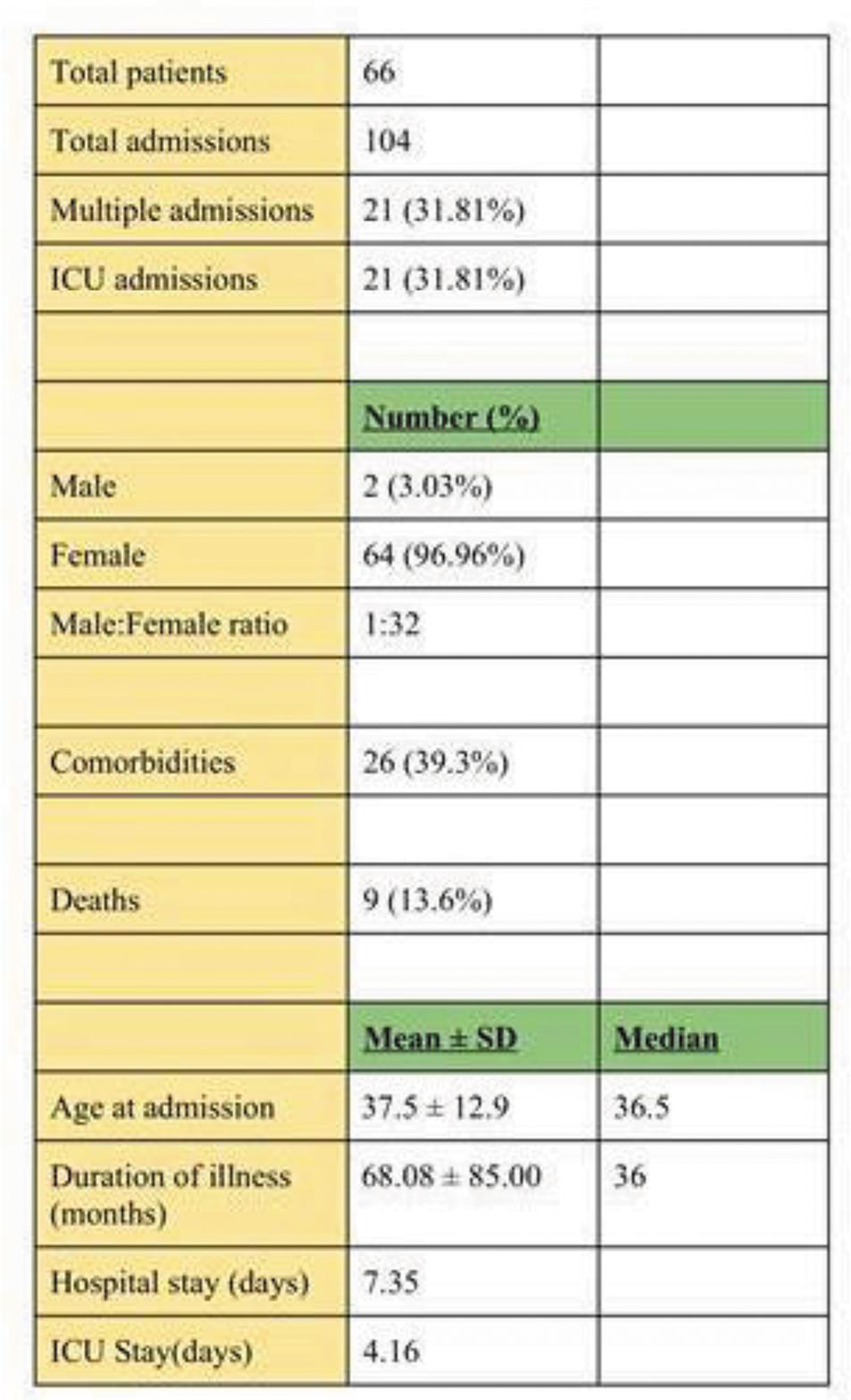
Image and Bar Table 2

POS249
Incidence and Type of Hearing Loss in the Primary Sjogren Syndrome in Birjand Province of South Khorasan Between 2021-2022
Primary Sjögren’s syndrome (pSS) is a chronic autoimmune disorder that mostly affects middle-aged women. The disease mainly involves the lacrimal and salivary glands. Primary Sjögren’s syndrome causes SNHL as an extraglandular manifestation of the disease. This affects the patient’s quality of life in many ways. In the years 2021-2022, we investigated the prevalence and audiometric pattern of patients with primary Sjögren’s syndrome in the city of Birjand.
This study was conducted on patients diagnosed with early Sjögren’s, referred to the rheumatology clinic. A comprehensive examination for the symptoms of Sjögren’s disease and the severity statement was done. The audiometry assessment for hearing evaluation was then performed using PTA and tympanometry. The audiometry results of all patients were interpreted by an otolaryngologist. At the level of significance of 0.05, independent t-tests and chi-square statistical tests were used. SSB, RF, ESR, and FANA tests and disease duration were compared using the Mann-Whitney U test, and an ANOVA was used to compare age and SSA.
A total of 44 people, including42 women (95.5%) and 2 men (4.5%), participated in this study. In the hearing tests, 21 people (47.7%) had hearing loss in left ear audiometry and 17 people (38.6%) in right audiometry. Six people (13.6%) had hearing loss in the left tympanometry and five people (11.4%) in the right tympanometry. Age and serum levels of ANA and ESR have a significant relationship with the severity of hearing loss. The average age was higher in those with mild hearing loss, and serum ANA and ESR levels were higher in those with mild sensorineural hearing loss (P = 0.006, P = 0.02, and P = 0.03).
In Sjögren’s patients, older age and higher serum levels of ANA and ESR, as well as corticosteroid use and severe and resistant disease, are related to a higher prevalence of hearing deterioration.
Image and Bar Table 1

Image and Bar Table 2
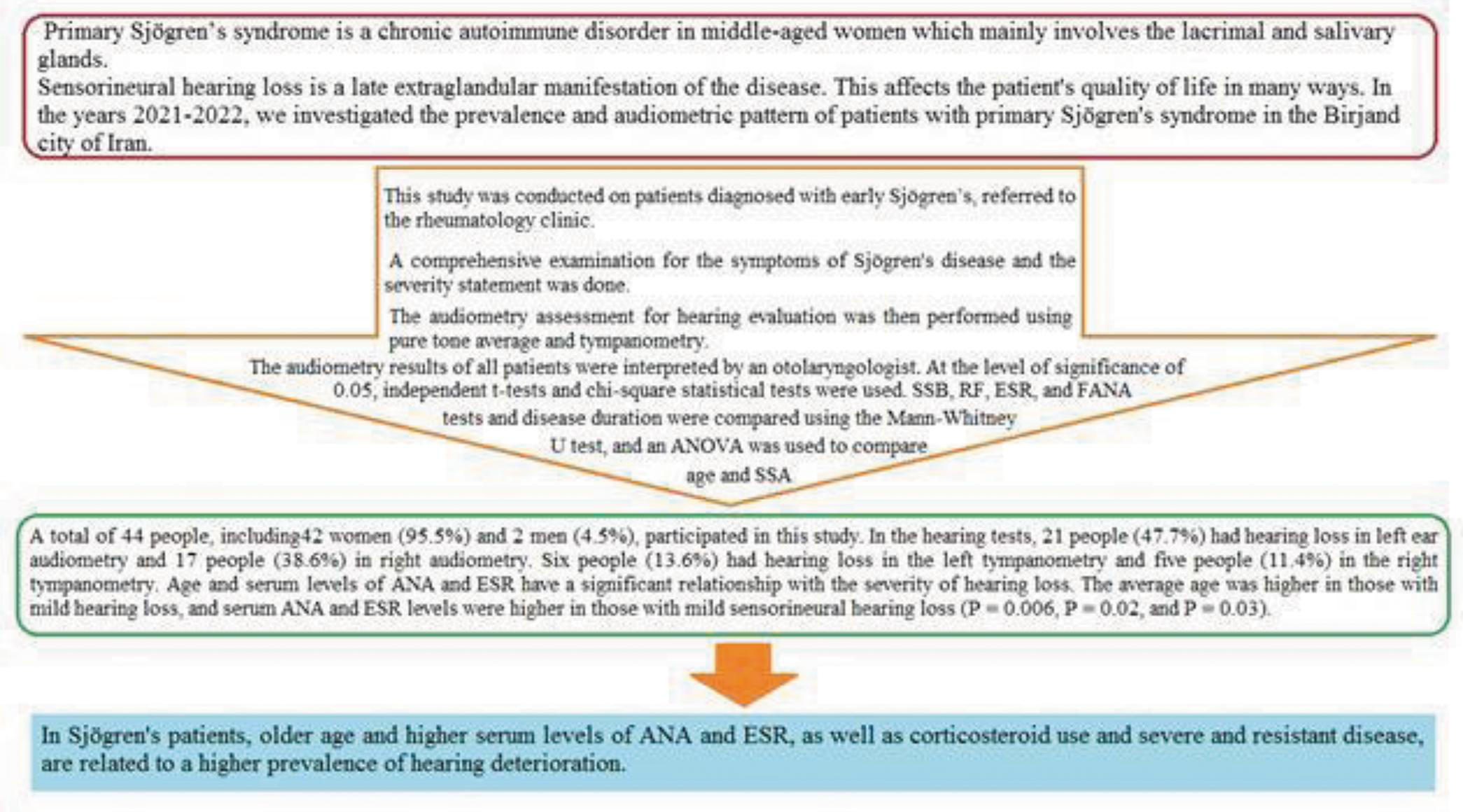
POS250
Predictors of Vasculitis in Systemic Lupus Erythematosus Patients
Image and Bar Table 1

Image and Bar Table 2

POS251
A Comparative Study of Clinical Features and Antibody Profile of Young and Late Onset Lupus Patients from a Tertiary Care Center
Image and Bar Table 1

Image and Bar Table 2

POS252
Unweaving the Complexities of SLE the Role of Autoantibodies, Covid-19 Vaccines, Drugs, Disease Manifestation and Overlap Syndrome: A New Paradigm to Personalized Medicine in SLE
Stratification of SLE patients based on autoantibodies, drugs and disease manifestations Exploring prevalence and potential risk associated with COVID-19 vaccine additionally investigating the outcomes of overlap syndrome in patients with SLE.
We have 42.8 % having overlap syndrome with a maximum of 17 patients with autoimmune haemolytic anaemia, followed by rheumatoid arthritis (20%) and APLA (17.7%). HCQ in combination of Prednisolone seems to be useful in overlap syndrome (77.4%).78% of our SLE patients took the Covid-19 vaccine predominantly Covishield. 6 newly diagnosed SLE patients, with thrombotic manifestations, obstruction of IVC, pelvic veins and dermatomyositis overlap.
Image and Bar Table 1

Image and Bar Table 2

POS253
Acute Pancreatitis in Systemic Lupus Erythematosus: Associated factors and Outcome
Comparison with cohorts showed that Mortality (p=0.01), Infection (p=0.02), Positivity for Lupus anticoagulant (p=0.028), Macrophage activation syndrome (p=0.002), and serum LDH (p=0.003) are more common in SLE with pancreatitis patients when compared to SLE patients with high disease activity and without pancreatitis.
In spite of advances in therapy Acute pancreatitis in SLE has high mortality. Higher incidence of coexisting infection and MAS along with high disease activity in SLE pancreatitis patient may explain higher mortality. Extensive search for underlying infection should be considered in SLE patients presenting with acute pancreatitis.
Image and Bar Table 1

POS254
Clinical, Radiological, and Treatment Outcomes in Lupus Enteritis
CT severity scores were classified as low (≤ 3) or high (> 3). The anatomical involvement was scored based on bowel wall thickness and extra-GI organ involvement. Time to tolerable oral intake (PO 50%) was calculated from symptom onset until patients could tolerate >50% of their regular diet.
POS255
A Study to Estimate Prevalence of Depression and Anxiety in Patients with Systemic Lupus Erythematosus and to Evaluate Association with Disease Activity, Damage Index and Social Factors
1. Bachen EA, Chesney MA, Criswell LA. Prevalence of mood and anxiety disorders in women with systemic lupus erythematosus. Arthritis Rheum.2009;61 (6): 822–9.
2. Du X, Chen H, Zhuang Y, Zhao Q, Shen B. Medication adherence in chinese patients with systemic lupus erythematosus. J Clin Rheumatol. 2020;26 (3): 94–8.
3. Jordan J, Thompson NJ, Dunlop-Thomas C, Lim SS, Drenkard C. Relationships among organ damage, social support, and depression in African American women with systemic lupus erythematosus. Lupus. 2019;28 (2):253–60.
Image and Bar Table 1
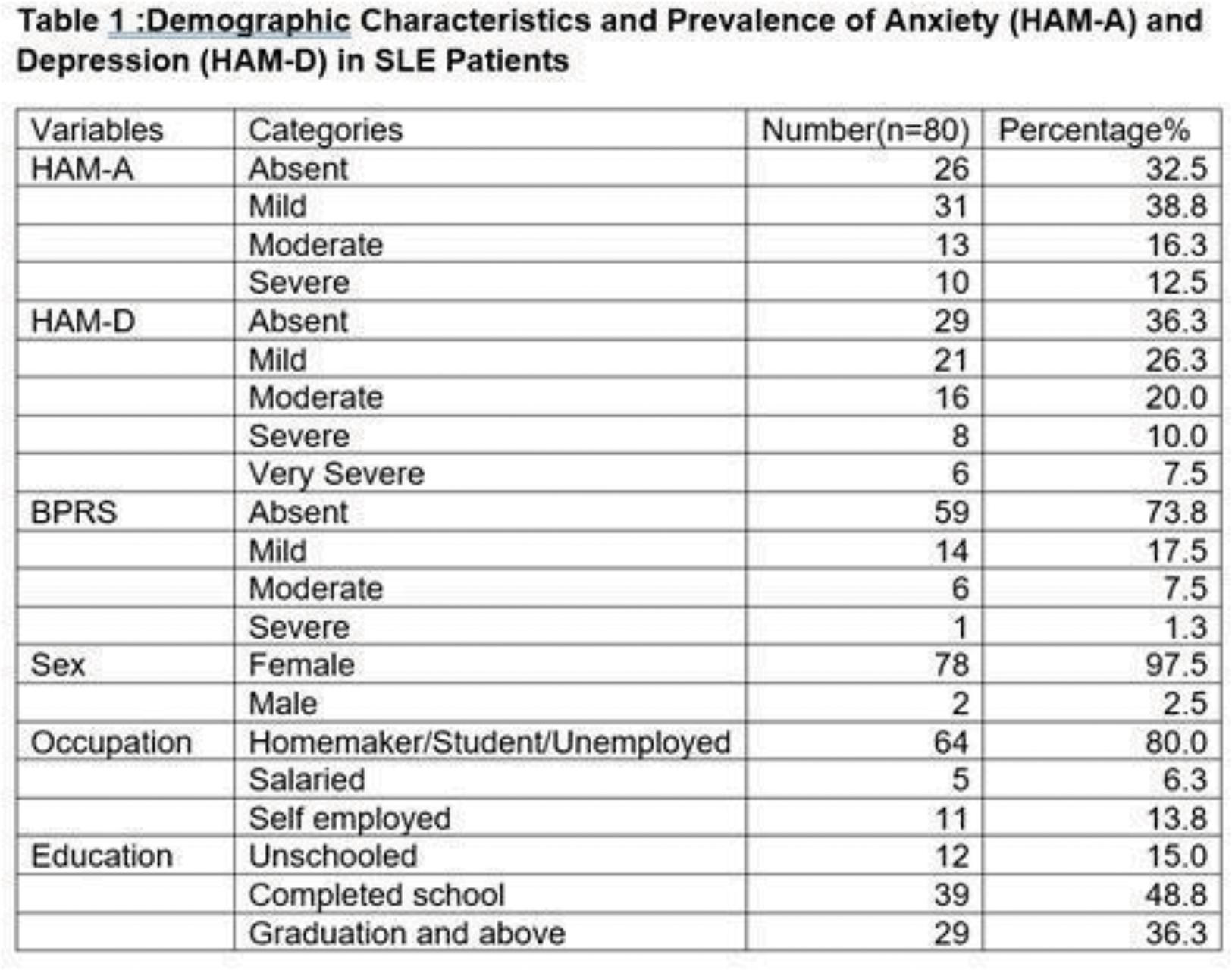
POS256
Clinical Utility of Repeat Renal Biopsies in Lupus Nephritis: Long Term Experience from North India
Rudrarpan Chatterjee1,
The NIH activity scores did not significantly differ between first (median 3, IQR 1-5), second (median 3, IQR 1-5) and third (median 3, IQR 2-5) biopsies. The NIH chronicity score rose from first (median 1, IQR 0-2) to second biopsy (median 2.5, IQR 1-3.75) (P<0.001) to third biopsy (median 5, IQR 3-8) (P<0.05). The eGFR rose from first (median 33.5, IQR 22.5-53.8) to second biopsy (median 43.7, IQR 24.7-64) but then reduced markedly at the time of third biopsy (median 20.7, IQR7.7-30.1) (p<0.05 for both).
Thirty-two (33.68%) of those with repeat biopsies developed ESRD. On multivariable logistic regression, a higher chronicity score at first biopsy (OR 1.99, 95% CI 1.05-3.77) predicted ESRD on follow up.
Image and Bar Table 1

POS257
Clinical Profile of SLE Patients with Tuberculosis
Major organ involvement (hematological/renal/myositis/cardiac/neurological/vasculitis) was present in 82.9% of the patients; majority had nephritis (74.3%). Median prednisolone dose at TB diagnosis was 10mg, median duration of prednisolone being 24 months. 17.1% (6) patients had received methylprednisolone pulse (125-1000mg) at some point during their disease course; As 2nd immunosuppression, patients had received Cyclophosphamide (40%), MMF (37%), Azathioprine (17.14%) and Tacrolimus. The median SELENA SLEDAI was 7.
All patients were on Antitubercular therapy; 1 patient died due acute liver failure which was attributed to possible drug induced liver injury. Following TB diagnosis, steroid dose was reduced and all 2nd immunosuppressive agents were withheld for a minimum period of 2weeks; for 4 weeks if disease activity necessitated. Cyclophosphamide was not rechallenged; rituximab was planned instead.
1. Smiyan, S., Koshak, B., Komorovsky, R. et al. Diagnostic challenge of tuberculosis in systemic lupus erythematosus: a case report and literature review. Rheumatol Int 43, 2131–2139 (2023).
POS258
Assessment of Clinical Practice Variations in Diagnosis, Monitoring and Treatment of SLE in India
POS259
Observational Study of Clinical and Laboratory Profile of Myositis in Systemic Lupus Erythematosus Patients in A Tertiary Care Hospital
POS260
Performance and Concordance of Two Different Methods of Detecting the Eight Common Autoantibodies in Systemic Lupus Erythematosus
The Cohen’s kappa for the two methods was 0.14, 0.38, 0.45, 0.54, 0.51, 0.35, 0.49 and 0.48 (p<0.001 for all; for dsDNA p<0.05) respectively showing poor to modest concordance. Since low-intensity positivity on immunoblot assay could adversely impact the concordance between the two methods, we re-analyzed the results after omitting 1+ intensities from the positive results and considering only 2+ and 3+ as positive. For all 8 antibodies, this did not improve the concordance between the two methods and led to a significant loss of positivity rate on the immunoblot assay (11.11%, 22.22%, 23.33%, 38.89, 11.67, 41.67, 28.89% and 22.78% respectively) (Table 2).
Image and Bar Table 1

Image and Bar Table 2
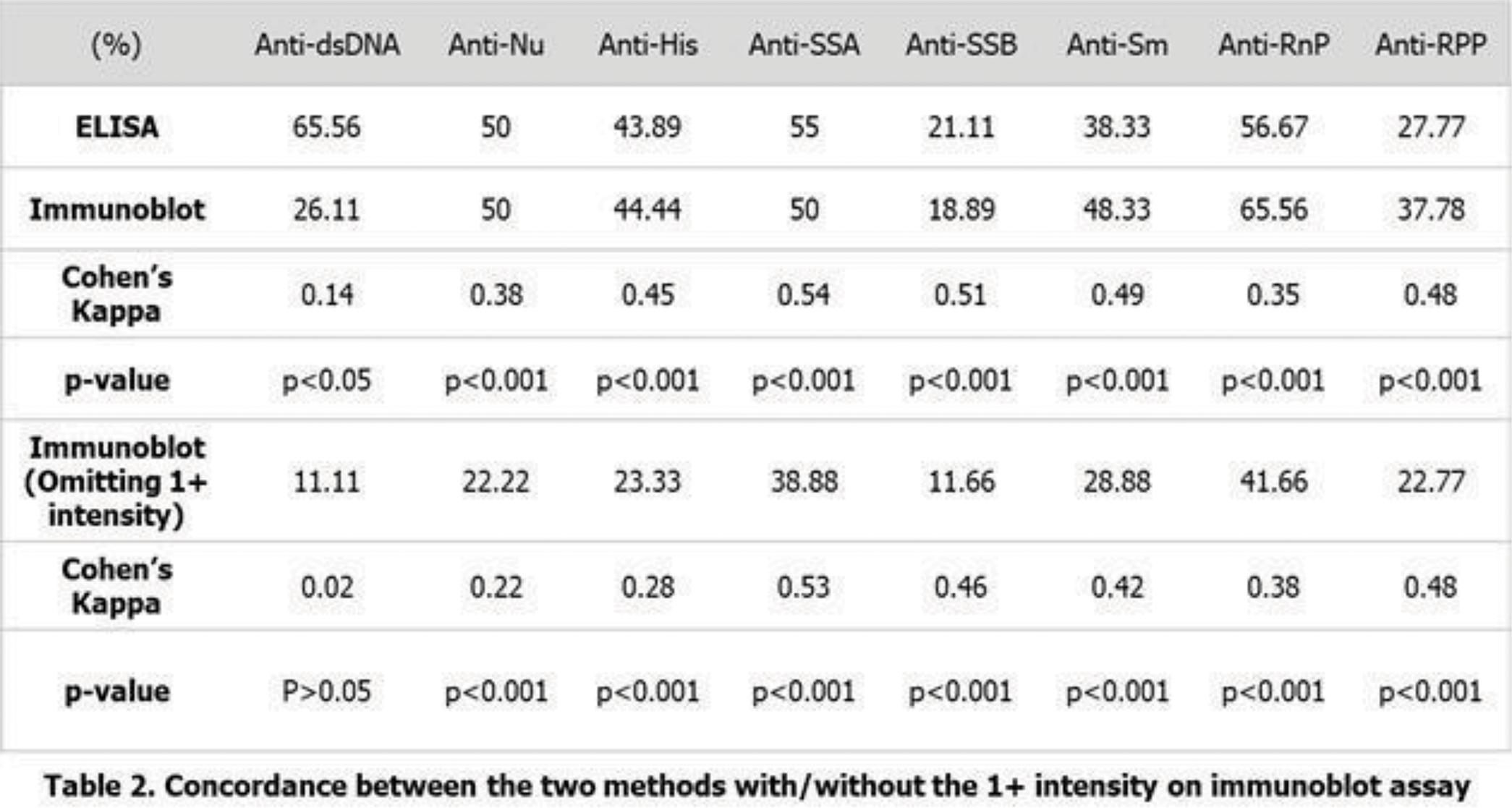
POS261
Clinical Profile and Outcomes of Myocarditis in Patients with Systemic Lupus Erythematosus: Single Centre Observational Study
Intravenous methylprednisolone was given in 85.7% of patients and all patients received oral glucocorticoids. Intravenous cyclophosphamide was used in 25 (89.3%) patients while rituximab and azathioprine were used in one patient each. Four patients received IVIg and one patient received plasma exchange. Eighteen (64.3%) patients clinically improved and were under active follow up. Among the eight patients with follow up echocardiography report, seven (87.5%) had normalisation of ejection fraction while in one patient hypokinesia persisted. Seven (25%) patients died with majority (71.4%) happening during admission. Three (10.7%) patients were lost to follow up.
Image and Bar Table 1

Image and Bar Table 2

POS262
Prevalence and Outcome of Renal Lupus at One Year in A Tertiary Care Center in Central India
POS263
Outcome of Pregnancy in Patients with Systemic Lupus Erythematosus (SLE): A Case-Controlled Study from the Indian SLE Inception Cohort for Research (INSPIRE) Cohort
Compare pregnancy outcomes in SLE patients before and after onset of SLE manifestations.
Pregnancies in the POST time period were significantly more likely to result in abortion (p=0.001), MTP (p=0.027) and preeclampsia/ eclampsia (p<0.001) as compared to the PRE time period as depicted in Table-1. Logistic regression showed odds of abortion as [1.97, (95%C.I.-1.34-2.91)], preeclampsia/eclampsia [18.7, (95%C.I.-2.4, 142.2)], MTP [2.4, (95% C.I-1.04-5.7)] and LBW [1.59, (95% C.I.-1.00-2.55)] in the POST time period.
The maternal outcomes were satisfactory, lupus flares occurred in only 6.2% (15/241) patients intra or postpartum period. Majority [205 (85.1%)] were on HCQ treatment at conception, and 55 (22.8%) had received prior cyclophosphamide treatment (Table 2).
Image and Bar Table 1
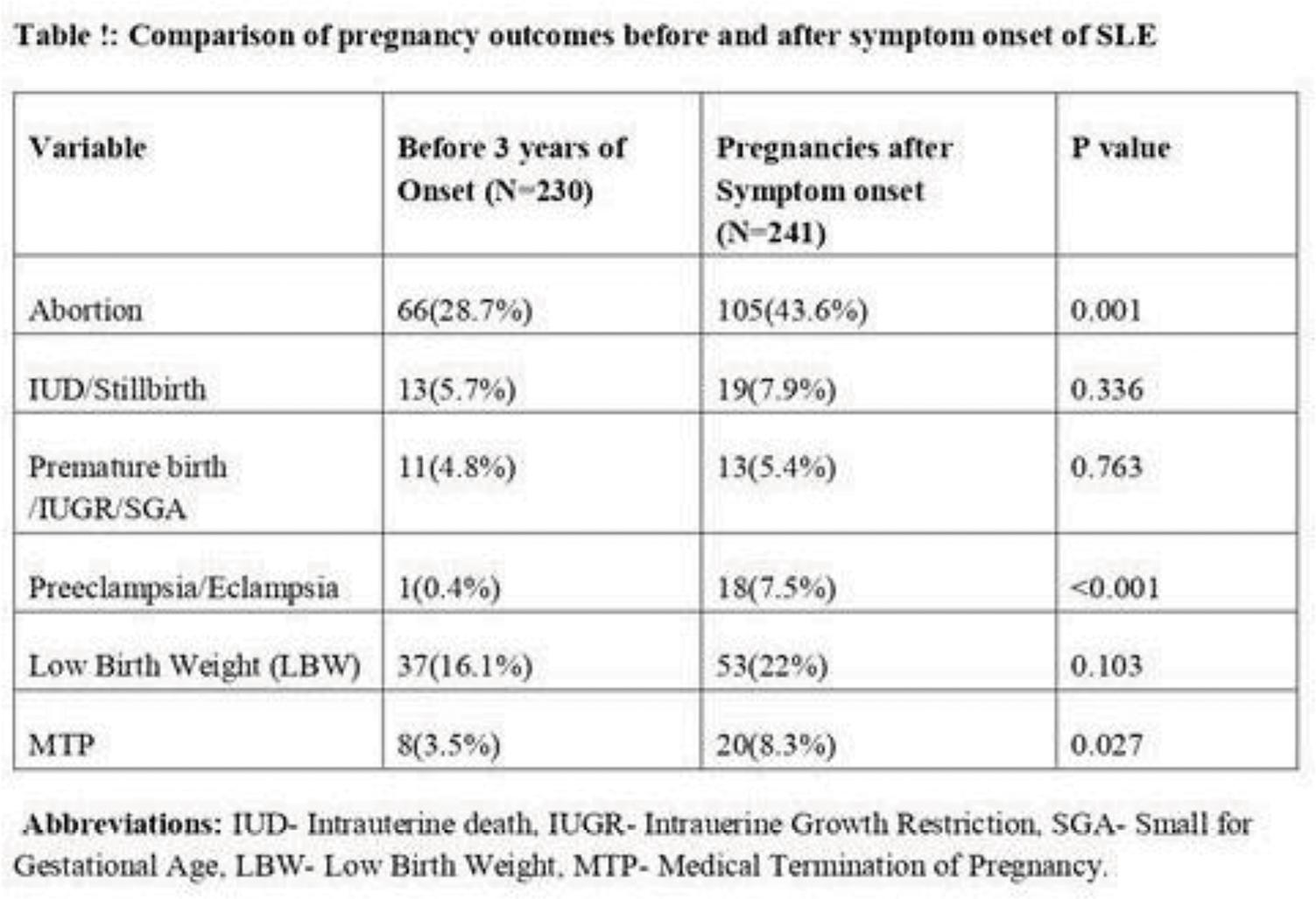
Image and Bar Table 2

POS264
An Early Renal Biopsy Strategy Uncovers Interstitial Inflammation and Leads to Improved GFR in the Initial 6 Months of Therapy in Lupus Nephritis
Of note, 3/13 patients in the group 1 had proliferative nephritis. In group 1, biopsy was done earlier in the disease course and these patients had lower NIH activity scores at the time of biopsy (Table 1). However, NIH chronicity scores and interstitial involvement, including interstitial inflammation, tubular atrophy and interstitial fibrosis were similar between groups (Table 1). In group 1, 24-hour Creatinine Clearance rose from 38.2±16.4 ml/min to 82.6±32.9 (p=0.004) at 6 months while in group 2, it rose from 46.6±24.8 ml/min to 77.01±39.4 ml/min (p<0.001).
At 6 months follow up, on multivariate analysis increase in GFR was predicted by lower C3 levels (Coefficient -0.57), higher C4 levels (Coefficient: 1.33) and the absence of tubular atrophy (Coefficient:-20.6) on biopsy.
POS265
Outcome of Systemic Lupus Erythematosus Patients with Active Tuberculosis
Following TB diagnosis, 40 (77%) were continued on low to moderate dose of steroids. Twenty-four (43%) patients received steroid-sparing immunosuppression simultaneously and 26 (46%) after the completion of antituberculosis therapy (ATT). Overall, during a follow up of 2 years, 20 patients attained clinical remission at a median time of 9 months (95%CI6.3-11.6). Adverse outcomes were noted in 30 (54%). 8 (14%) died during 2 years of follow up. In the remaining, 14 (31%) suffered TB related complications, 14 (31%) had SLE flare, 10 (22%) did not attain LLDAS remission over 2 years of follow up and 5 (11%) developed organ damage due to SLE.
ETB/DTB with CNS involvement was the predictor of adverse outcome in regression whereas timing of immunosuppression or dose of steroids did not predict the same.
1. Yang, Y., Thumboo, J., Tan, B.H. et al. The risk of tuberculosis in SLE patients from an Asian tertiary hospital. Rheumatol Int 37, 1027–1033 (2017).
2. Muhammed, H., Jain, A., Pattanaik, S.S. et al. Clinical spectrum of active tuberculosis in patients with systemic lupus erythematosus. Rheumatol Int 41, 2185–2193 (2021).
POS266
Clinical Characteristics and Predictors of Lupus Enteritis: A Single Centre, Retrospective Study
To characterize the clinical, laboratory and radiological parameters of patients with LE and compare with non-LE controls. To explore the predictors of LE.
Screening of LE cases and non-LE controls: Among 5280 SLE cases, LE was diagnosed in 19 cases (0.36%). 18 cases (94.7%) were female. They were compared with an age and gender matched cohort of 38 subjects with SLE without LE (non-LE). The baseline characteristics of the study population is depicted in Table 1. Comparison of clinical data between cohorts: The most common symptom of LE was abdominal pain (94.7%) and vomiting (94.7%). C3, LDH, CRP, IgG, IgM, and IgA were found to be elevated more in LE cohort with statistically significant difference (p<0.05). Hydronephrosis, ascites, and pleural effusion was seen more in LE cohort with statistically significant difference (p-value<0.05). Abnormal bowel wall enhancement (bowel wall edema/thickening) was seen in 84.2% cases with target seen and comb sign present in 47.4% and 26.3% cases, respectively. Methylprednisolone (MPS) pulse was given in 52.6% cases. Cyclophosphamide was the most common second immunosuppression (68.4% cases). All cases improved with treatment. Analysis to define parameters associated with (predictors of) LE Clinically significant variables with statistical significance on univariate analysis were subjected to bivariate logistic regression with selection of most accurate model of prediction. High CRP (>0.6 mg/dL), HDUN and ascites were independently associated with LE (Table 1).
Image and Bar Table 1

Image and Bar Table 2

POS267
High Prevalence of Neuropsychiatric Lupus in North India and the Utility of Standardized Tools to Assess Delirium in Lupus
On comparing NPSLE vs Non NPSLE group (Table 2), malar rash (n=41, 85.4% vs 100, 98%, p=0.003) and fever (38, 79.2% vs 98, 96%, p= 0.004) were less frequent in NPSLE group. NPSLE group had higher SLEDAI 2K score (18.8 ± 11 vs 7.1 ± 6.4, p <0.001), higher proportion of active disease (n= 42, 87.5 % vs n=44, 43%, p<0.001), antibodies to histone (n=16, 33.3% vs n =22, 21.5%, p = 0.032), U1RNP (n=8, 16.7% vs n=6, 5.8%, p=0.024) and low C4 levels (n=33, 69% vs n=51, 50%, p=0.018).
With respect to delirium assessment tools, NPSLE group had lower mean MMSE score (25.25 ± 3.4 vs 29.9 ± 4.1, <0.001) and high ICDSC score (2.5 ± 2.2 vs 0, <0.001) and higher proportion of CAM-ICU positivity as compared to non NPSLE group (n= 12, 25% vs 0, <0.001). The prevalence of delirium as per CAM-ICU and ICDSC was 6 % and asper MMSE was 5 %. Those with delirium had higher systemic disease activity as compared to NPSLE patients without delirium (Mean SLEDAI 2K score (27.3 ± 8.4 vs 16.3 ± 10.62, p = 0.004) as compared to other NPSLE patients The three scores had good concordance with each other with Cohen’s Kappa of 0.799 between CM-ICU and ICDSC, 0.827 between CAM-ICU and MMSE and 0.729 between ICDSC and MMSE.
Image and Bar Table 1

Image and Bar Table 2

POS268
Treatment Response and Long-Term Outcomes of Pure Membranous Lupus Nephritis: A Ten-Year Data
Image and Bar Table 1

Image and Bar Table 2

POS269
Comparison of Clinical Characteristics and Outcomes of Systemic Lupus Erythematosus Related Thrombotic Thrombocytopenic Purpura and Non-Autoimmune Thrombotic Thrombocytopenic Purpura: A Single Centre Study
Image and Bar Table 1

Image and Bar Table 2

POS270
Lupus Cohort with Antinucleosome Based Clinical Characteristics
1. Suleiman S, Kamaliah D, Nadeem A, Naing NN, Che Maraina CH. Anti-nucleosome antibodies as a disease activity marker in patients with systemic lupus erythematosus. Int J Rheum Dis. 2009 Jul;12 (2):100-6. doi: 10.1111/j.1756-185X.2009.01391.x.
2. Elsayed, S.AR., Kamaly, H.M. & Esmail, M.A. Co-positivity of anti-dsDNA, anti-nucleosome, and anti-smith autoantibodies as serological biomarkers for disease activity in systemic lupus erythematosus. Egypt Rheumatol Rehabil 49, 8 (2022).
POS271
Prevalence of Iron Deficiency Anemia in Systemic Lupus Erythematosus and Its Relationship with Disease Activity: A Cross Sectional Study
In addition, baseline data of SLE patients with iron deficiency anemia recruited for a prospective longitudinal study was used to study the relationship between serum ferritin levels and disease activity using SLEDAI along with patients enrolled in INSPIRE cohort.
An additional 48 SLE patients (47 females) with iron deficiency anemia [from longitudinal study] were included. Their median age and duration of disease was 33.0 (25.2-42.5) years and 72.0 (31.5-121.5) months, respectively. Most patients had inactive disease with median SLEDAI of 2 (0-4).
A strong correlation was found between serum ferritin and disease activity in the combined cohort (Spearman’s Rho R = 0.65, p < 0.001) (Fig. 1). Non-iron deficient SLE patients had high prevalence of serositis, neurological involvement, lower hemoglobin, and high disease activity (Table 1).
ACR – American College of Rheumatology
EULAR – European League against Rheumatism
INSPIRE – Indian SLE Inception cohort for Research
SLEDAI – Systemic lupus erythematosus disease activity Index
Image and Bar Table 1

Image and Bar Table 2

POS272
P-Gp and MRP-1 Positive Plasma Cells and Th17 Lymphocytes are Increased in Peripheral Blood of Active and Refractory Lupus Nephritis
The frequency of PB CD138+CD38+ PCs were significantly increased in refractory and active LN as compared to inactive LN and HCs at baseline (Figure 2) which was significantly reduced after 3 months following treatment with tacrolimus, MMF or Cyclophosphamide. Expression of P-gp and MRP-1 on PCs was significantly increased in refractory and active LN, as compared to inactive LN and HCs, which decreased significantly following treatment (figure 2).
The level of NGAL, IL-17, IL-6, TNF-ɑ and CXCL12 in plasma of refractory and active LN were significantly raised at baseline, as compared to inactive LN and HCs, which decreased significantly after 3 months of treatment.
Image and Bar Table 1

Image and Bar Table 2

POS273
Unraveling Thyroid Dysfunctions in Patients of Systemic Lupus Erythematosus
The objectives of the study were multifold. Firstly, it seeks to assess thyroid dysfunctions among patients of SLE. Secondly, it aims to assess autoimmunity using antibodies like anti TPO antibody in patients of SLE. Also, it aims to correlate thyroid autoimmunity with thyroid dysfunction. It aims to correlate thyroid dysfunctions in various domains in patients of SLE. And lastly it aims to correlate thyroid dysfunctions with disease activity of SLE using SLEDAI score.
POS274
Effect of Cyclophosphamide on Ovarian Function in Systemic Lupus Erythematosus and Comparison with Other Immunosuppresant-Mycophenolate Mofetil and Azathioprine
Patient with history of hysterectomy or cervical malignancy Patients with ESRD or chronic liver disease Those who had undergone hysterectomy, oophorectomy, or pelvic irradiation Those who were on oral contraceptive pills or hormone replacement therapy
Mean age of CYC, MMF & AZA are 25.7, 27.35 and 28.1 yrs respectively. The mean BSA of recruited subjects was 1.6, of CYC group was 1.6, of MMF group was 1.63 and of AZA group was 1.58 with p=0.0492*. Mean SLEDAI was 16.2 (±4.5), in CYC group was 15.56 (±4.84), in MMF group was 16.6 (±4.4), and in AZA group was 17 (±4), with P=0.6490.
At 6 months follow up oligomenorrhea raised from 27 to 36 subjects with CYC group rose to 21from 10 at baseline, MMF group became 5 from 10, AZA group became 10 from 6.
AMH levels in CYC group showed at follow up from baseline value of 3.7±3.4 pg/ml (P <0.0001). In MMF group 6 month follow up AMH 3.7±1.9 increased from baseline AMH 3.9±1.9 pg/ml (P=0.044*). In AZA group baseline AMH 5.2±3.36 vs. follow up 4.9±3.4 (P=0.2278).
Analysing 3 treatment groups (CYC, MMF, AZA) in SLE patients who had comparable demographic and clinical details mean AMH levels at baseline and at 6 month follow up, were significantly lower in patient treated with CYC and MMF No correlation is observed between total duration of disease and AMH levels No correlation observed between SLEDAI and serum AMH levels Adverse effects of induction with IVCYC monthly (moderate dose) on the ovarian function is predominantly subclinical not progressing to POF.
Image and Bar Table 1
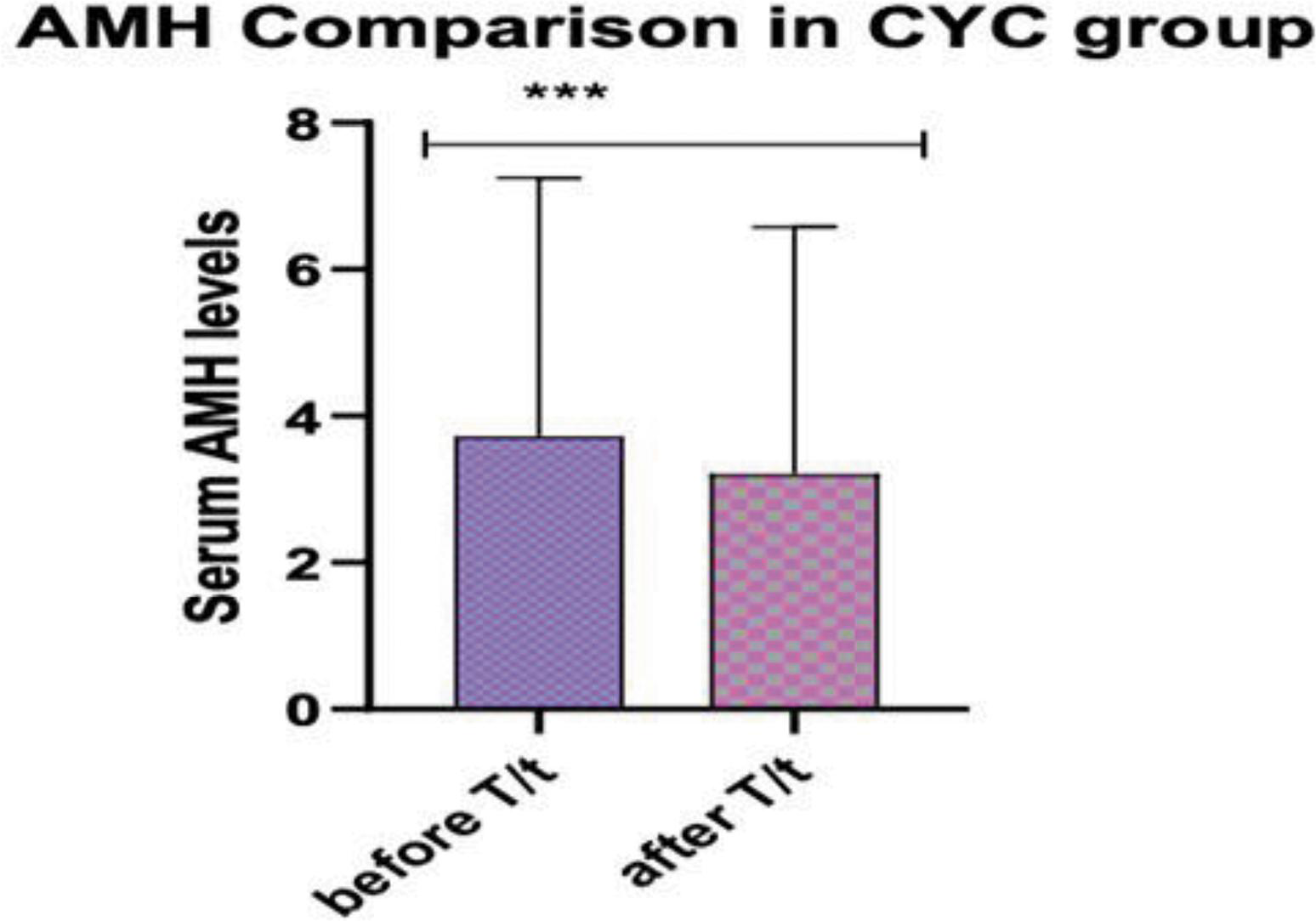
Image and Bar Table 2

POS275
Clinical Features of Lupus Enteritis and The Diagnostic Role of Bowel Ultrasound in Lupus Enteritis
Image and Bar Table 1
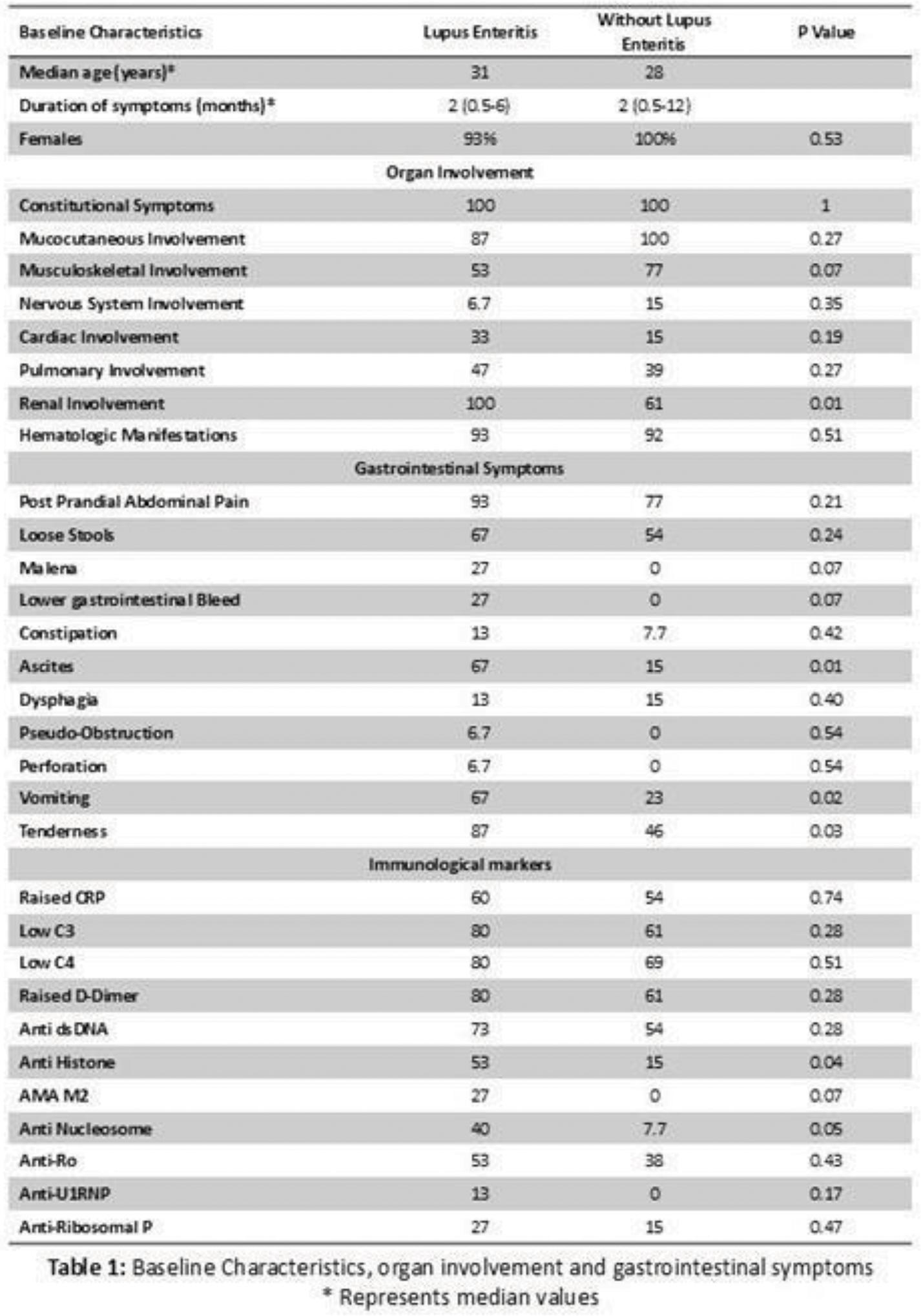
Image and Bar Table 2

POS276
Unmasking Dyspnea in Systemic Lupus Erythematosus
Image and Bar Table 1
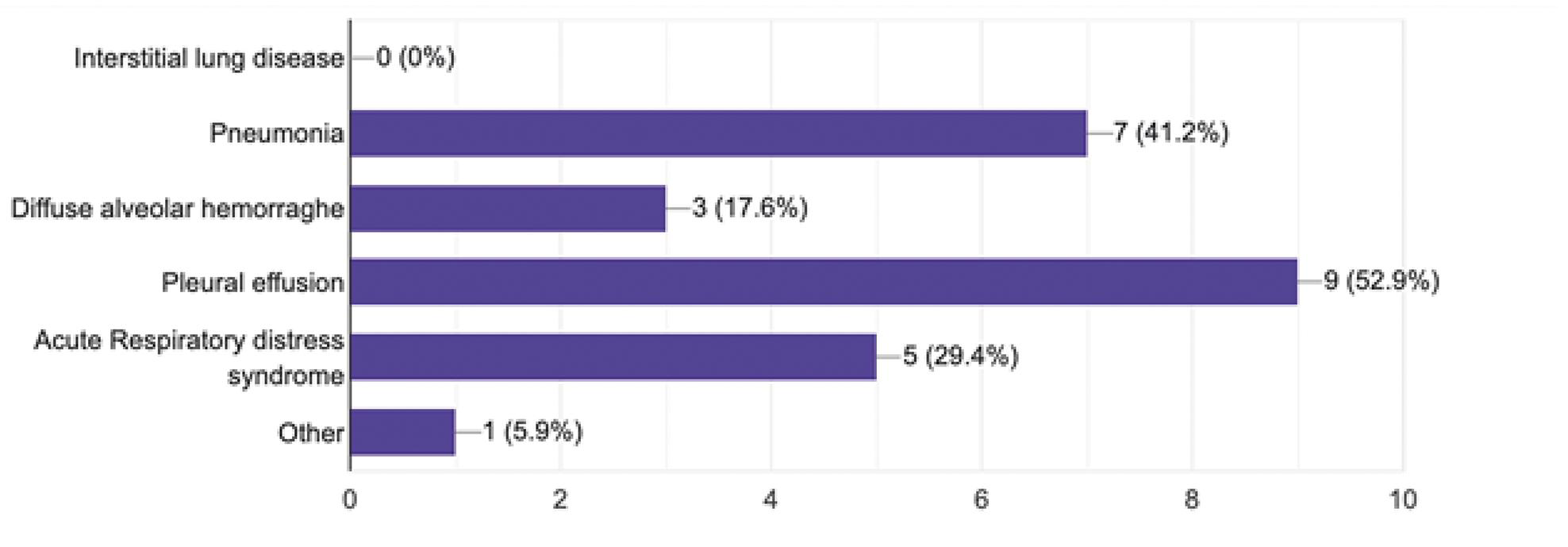
Image and Bar Table 2

POS277
Contraceptive usage in Females of Reproductive age with Systemic Lupus Erythematosus
Characterize the types of contraception used by this population Determine factors affecting the contraception use
Factors affecting Contraception use include Higher age group (35-45yrs) (p <0.001), Higher Socioeconomic status (p = 0.035), two or more pregancies (p = 0.006), two or more children (p < 0.001) had higher usage of contraception Compared to remaining Study population. Disease activity, Use of teratogenic drugs, Knowledge of contraceptive methods, reproductive counselling, and contraceptive counselling did not show statistically significant associations with contraceptive use.
Small sample size, Single center study
1. Yazdany J, Trupuin L, Kaiser R, et al. Contraceptive counseling and use among women with systemic lupus erythematosus: a gap in health care quality. Arthritis Care Res (Hoboken). 2011;63 (3):358-365.
2. Kittisiam T, Werawatakul Y, Nanagara R, Wantha O. Low prevalence of contraceptive counseling at Srinagarind hospital, Thailand among women of reproductive age with systemic lupus erythematosus. Reprod Health. 2013 Apr 11;10:21. doi: 10.1186/1742-4755-10-21. PMID: 23577791; PMCID: PMC3640918.
3. P. Buasawat, J. Manonai, P. Ngamjanyaporn, Perception of Contraceptive Counselingand Contraceptive Use among Systemic Lupus Erythematosus Patients, Contraception (2020), doi:
Image and Bar Table 1

Image and Bar Table 2

POS278
Systemic Lupus Erythematosus and Its Impact on Reproductive Health: A Comprehensive Review of Pregnancy Outcomes
1. Dao KH, Bermas BL. Int J Women Health. 2022;14:199-211.
2. Patel BS. Systemic lupus erythematosus and pregnancy – A brief review.
Image and Bar Table 1
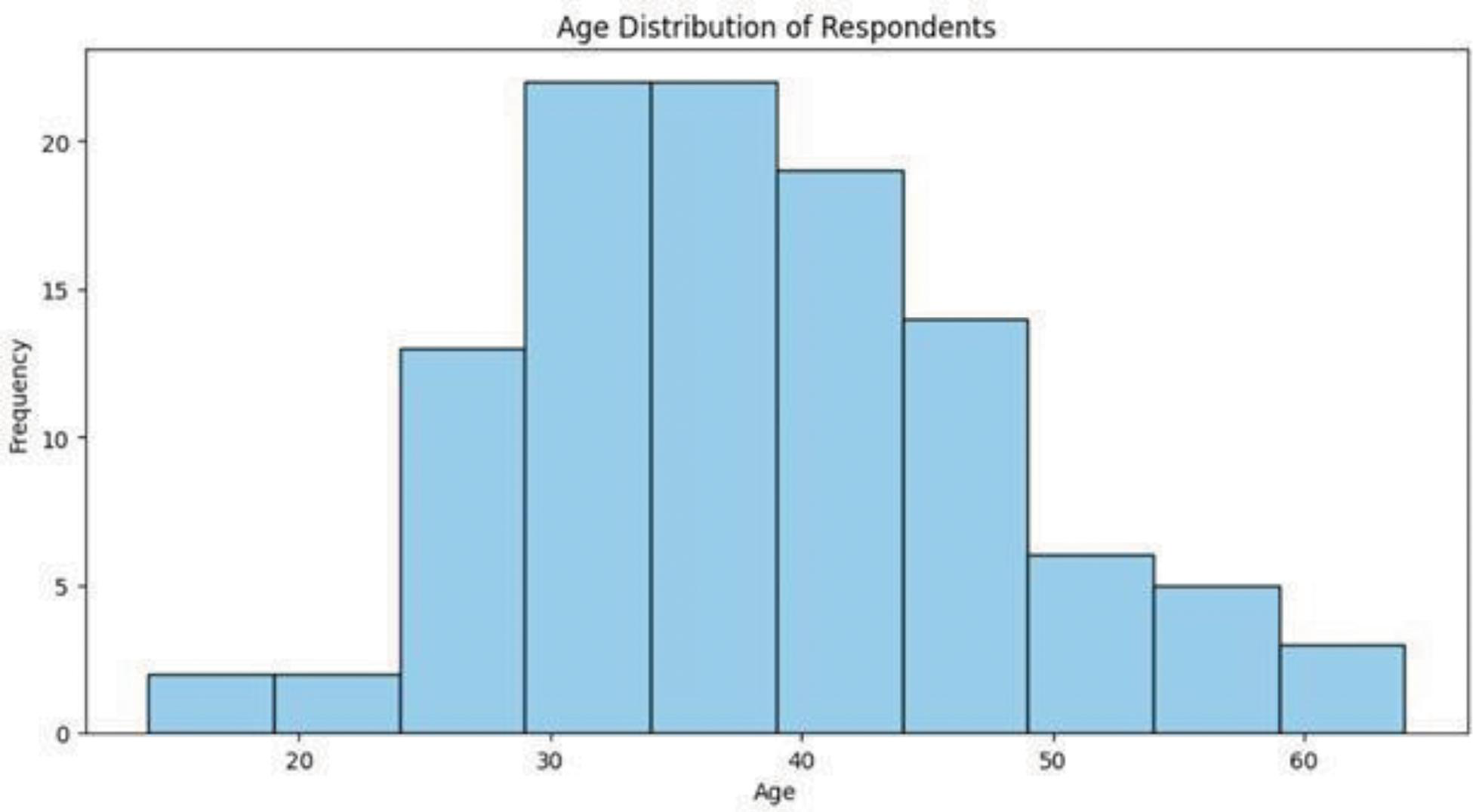
Image and Bar Table 2

POS279
SGLT2 Inhibitor as Add-On Therapy in Lupus Nephritis with Persistent Proteinuria – Interim Results of An Ongoing Pilot Study
To assess the reduction in 24-hour proteinuria and urine protein/creatinine ratio after the addition of dapagliflozin in patients with lupus nephritis having persistent proteinuria. To assess SLE disease activity by SELENA SLEDAI score at 3 and 6 months after the addition of dapagliflozin. Adverse effects attributable to dapagliflozin and reasons for discontinuation.
POS280
A Randomized, Controlled, Open-Label Phase III Trial Comparing Efficacy and Safety of Intravenous Cyclophosphamide, Mycophenolate Mofetil, or Tacrolimus as Induction Therapy in Lupus Nephritis
Image and Bar Table 1

Image and Bar Table 2

POS281
Discriminant Factors in Lupus Flare and Its Determinants: Study from A Tertiary Care Hospital
POS282
Association of Duration in Modified DORIS Clinical Remission/LLDAS with SDI: A Single-Center Cross-Sectional Study in SLE Patients
To analyse the association between the duration spent in modified DORIS clinical remission/LLDAS and the SDI in SLE patients. To compare SDI scores between patients in modified DORIS clinical remission plus LLDAS and those in modified LLDAS only.
The cumulative time spent in either DORIS clinical remission or LLDAS was calculated from previous clinical visits and recorded as follows:
Sum of all time intervals in modified LLDAS or modified DORIS remission / Total length of follow up 2* 100
No significant difference in damage index was observed between those who were in modified DORIS plus LLDAS and LLDAS remission only.
No significant difference in damage index was observed between those with major organ involvement (NPSLE/ Lupus nephritis) during the course and SDI score of 1 or above
1. Prolonged clinical remission and low disease activity statuses are associated with better quality of life in systemic lupus erythematosus. N Poomsalood et al Lupus. 2019 Sep;28 (10):1189-1196.
2. Lupus low disease activity state and remission and risk of mortality in patients with systemic lupus erythematosus: a prospective, multinational, longitudinal cohort study), Rangi Kandane-Rathnayake et al, Lancet Rheumatol. 2022 Dec;4 (12).
Image and Bar Table 1

Image and Bar Table 2

POS283
Clinical and Serological Profile of Patients with Lupus Associated Myocarditis- A Single Center Study
Image and Bar Table 1

Image and Bar Table 2

POS284
Myocardial Involvement in Systemic Lupus Erythematosus - A 5 Year Retrospective Observational Study from A Tertiary Care Center in South India
Image and Bar Table 1

POS285
Posterior Reversible Encephalopathy Syndrome in Young Lupus Patient: A Case Series
14 year old young boy, a diagnosed case of Systemic Lupus Erythematosus presented with complain of multiple joint pain, malar rash, oral ulcer and headache admitted for cyclophosphamide pulse.
We retrospectively evaluated the clinical records of pediatric patients (age 10-14 years) who were diagnosed as having posterior reversible encephalopathy syndrome and followed up National Center for Rheumatic Disease, over a period of 3 years. We reviewed the demographic and clinical data, underlying medical condition, blood pressure reading, neuroimaging findings, treatments received and recovery status.
A total of two pediatric patients were identified, the common clinical manifestation included hypertension (2/2), generalized tonic clonic seizure (2/2), altered consciousness (2/2), recent immunosuppressive use (2/2), visual disturbance (1/2). Early diagnosis and differentiation from other causes along with imaging studies is important to initiate treatment and prevent further complication hence high index of suspicion and prompt treatment can minimize morbidity and mortality, and pave the path for early recovery.
POS286
Verbal Autopsy Identifies Disease Activity as A Cause of Death in SLE Home Deaths
POS287
Cutaneous Lupus Erythematosus and COVID-19: The Neglected Kid on The Rheumatologist’s Block An Observational Study
Abhibroto Karmakar,
The spectrum lies from localized cutaneous LE to severe systemic LE (SLE). The interplay between autoantibodies, cutaneous findings, physical photoprotection along with topical ointments in addition immunosuppressants is an area of current interest. Our studyhig highlights the different aspect of CLE including COVID-19 vaccination and treatment regimen.
To evaluate the prevalence, pattern of skin lesions and correlation between cutaneous, systemic manifestations, serological profile and treatment a dermatologist perception.
Image and Bar Table 1

Image and Bar Table 2

POS288
Lupus Profundus: A Non-Life-Threatening Disease with Significant Morbidity – A Case Series
Here we present five cases of Lupus profundus, all five cases were biopsy proven and four of the five cases were associated with systemic lupus and one case in isolation, three of the five cases were females and two male and one pediatric case.
1. Lauren K Rangel BA, Camilla Villa-Ruiz MPH, Kelly Lo BS et al. Clinical Characteristics of Lupus Erythematosus Panniculitis/Profundus: A Retrospective Review of 61 Patients. JAMA Dermatol. 2020;156 (11):1264-1266.
A middle-aged male with Discoid lupus and profundus lesions and lipoatrophy

A 14-year-old girl with an active panniculitis lesion and lipoatrophy

POS289
Clinical Profile and Treatment Outcomes of Diffuse Alveolar Hemorrhage in SLE: A Report of 5 Cases
Image and Bar Table 1

POS290
Rare Associations with SLE-3 Cases
Sapan Pandya1,
A 30 years old lady, presented with a complaint of yellow discoloration of skin associated with nausea and vomiting for 2 months. She had a history suggestive of fever associated with weight loss of 14 kg, inflammatory polyarthritis, photosensitive erythematous skin rash, sicca features and raynauds for 1 year. On examination she had icterus and serpiginous palatal ulcers. Her AST/ALT were 83/139 U/L, ALP was 1565 IU/L, Bilirubin- total/direct/indirect were 27.1/20.5/6.6 mg/dL. Her ANA by immunofluorescence was 3+ with fine speckled pattern and ANA blot strongly positive for AntiSSA/Ro-60, AntiSSA/Ro-52, AntiSSB, RNP-A/C antibodies. Her ASMA and Anti-LKM antibodies were negative. Magnetic resonance cholangiopancreatography showed multifocal intrahepatic and extrahepatic dilatation of biliary radicles suggestive of primary sclerosing cholangitis. Her liver biopsy showed mild inflammatory infiltrate and cholestasis and portal tracts showing fibrosis on trichrome stain.
A diagnosis of SLE associated with PSC (based on serological, MRCP and histological investigations) was made which is a rare association.
Image and Bar Table 1

Image and Bar Table 2
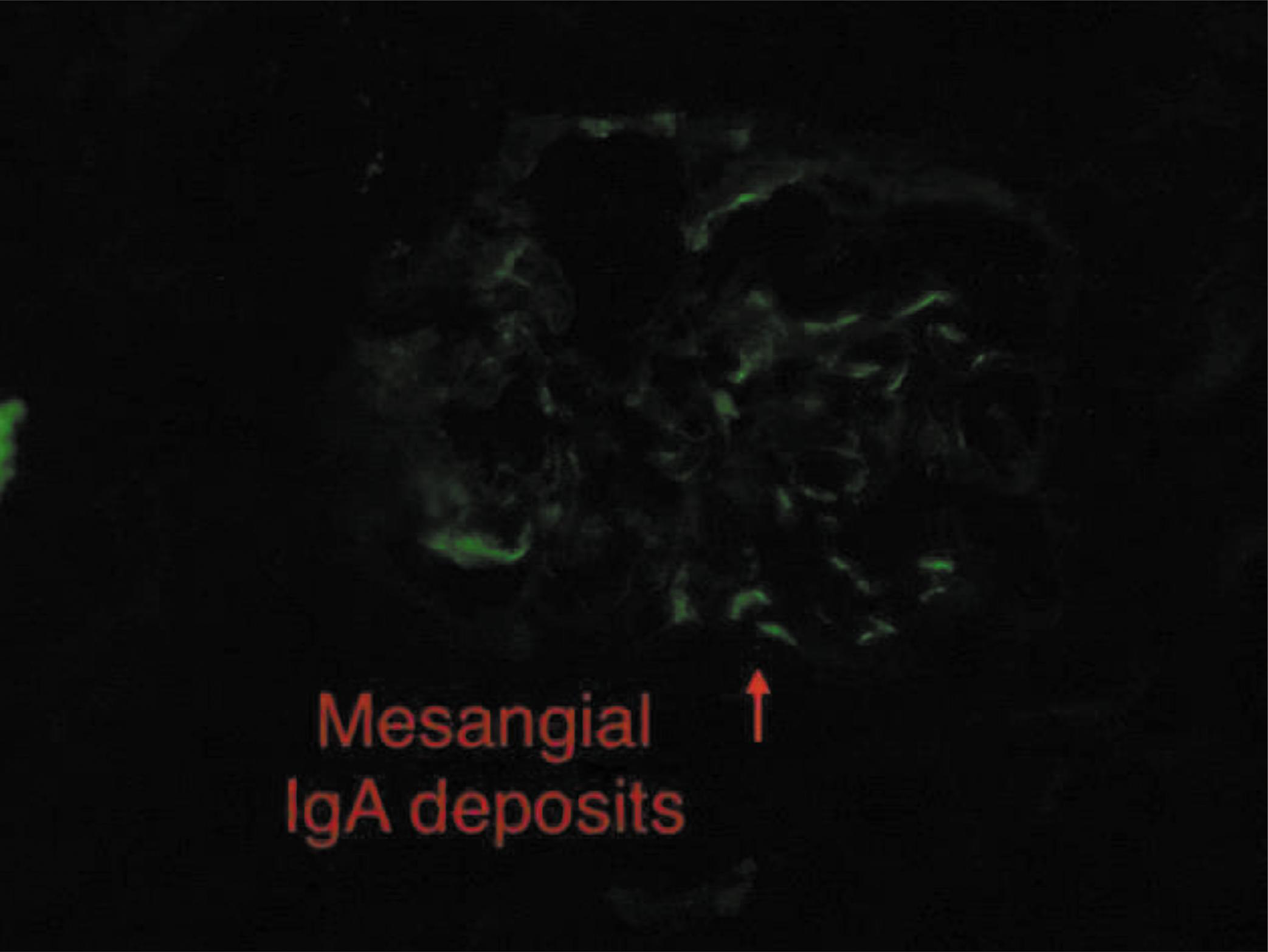
POS291
Unveilling Mysteries of the Inflamed Heart: A Case Series of Lupus Myocarditis
1. Harrison’s Principle of Internal Medicine 21st edition.
2. Tanwani et al Lupus myocarditis: A single center experience and a comparative analysis of observational cohort studies. Lupus. 2018;27:1296–302.
POS292
A Case Series on SLE Pancreatitis: From Presentation to Flare
The second case pertains to a 35-year-old female with a known history of SLE, primarily manifesting with cutaneous involvement. She presented with acute pancreatitis as a flare of her underlying disease. Comprehensive evaluation excluded other etiologies, including infectious, metabolic, drug-related, or vascular causes. Immunological markers confirmed the exacerbation of SLE. Aggressive management with corticosteroids and immunosuppressive therapy led to clinical improvement.
1. Sagawa A, Murakami M, Saito I, et al. Acute pancreatitis as a complication of systemic lupus erythematosus. Lupus. 2002;11 (10):678-683.
2. Tsai HL, Wu TH, Huang CC, et al. Acute pancreatitis in systemic lupus erythematosus: A cohort study. Lupus. 2011;20 (11):1198-1204.
Image and Bar Table 1

POS293
Prevalence and Clinical Significance of Antiphospholipid Antibodies in Systemic Lupus Erythematosus
Anny Kharel,
Image and Bar Table 1

Image and Bar Table 2

POS294
Outcome of Patients with Non-Criteria Manifestations of Primary Antiphospholipid Syndrome Treated with Immunosuppressants -A Single Centre Study
During a median follow up of 32 months (IQR: 20-63), 80% patients responded to treatment. The response was sustained in 59% at the last follow up. The best response was noted among patients with thrombocytopenia. n=20 (83%) of thrombocytopenia responded to immunosuppressive treatment including rituximab (n=9, 81%), mycophenolate (n=5, 85%) and Azathioprine (n=6, 66%). Response rates of all manifestations is depicted in Table 2.
Major adverse events included death in 2 patients due to sepsis and pneumocystis carinii pneumonia in patients receiving rituximab and 1 death due to sepsis, disseminated TB, Ca breast in patients receiving MMF
Image and Bar Table 1

Image and Bar Table 2

POS295
Non Criteria Manifestations of Primary Antiphospholipid Antibody Syndrome-Single Centered Retrospective Descriptive Study
Image and Bar Table 1
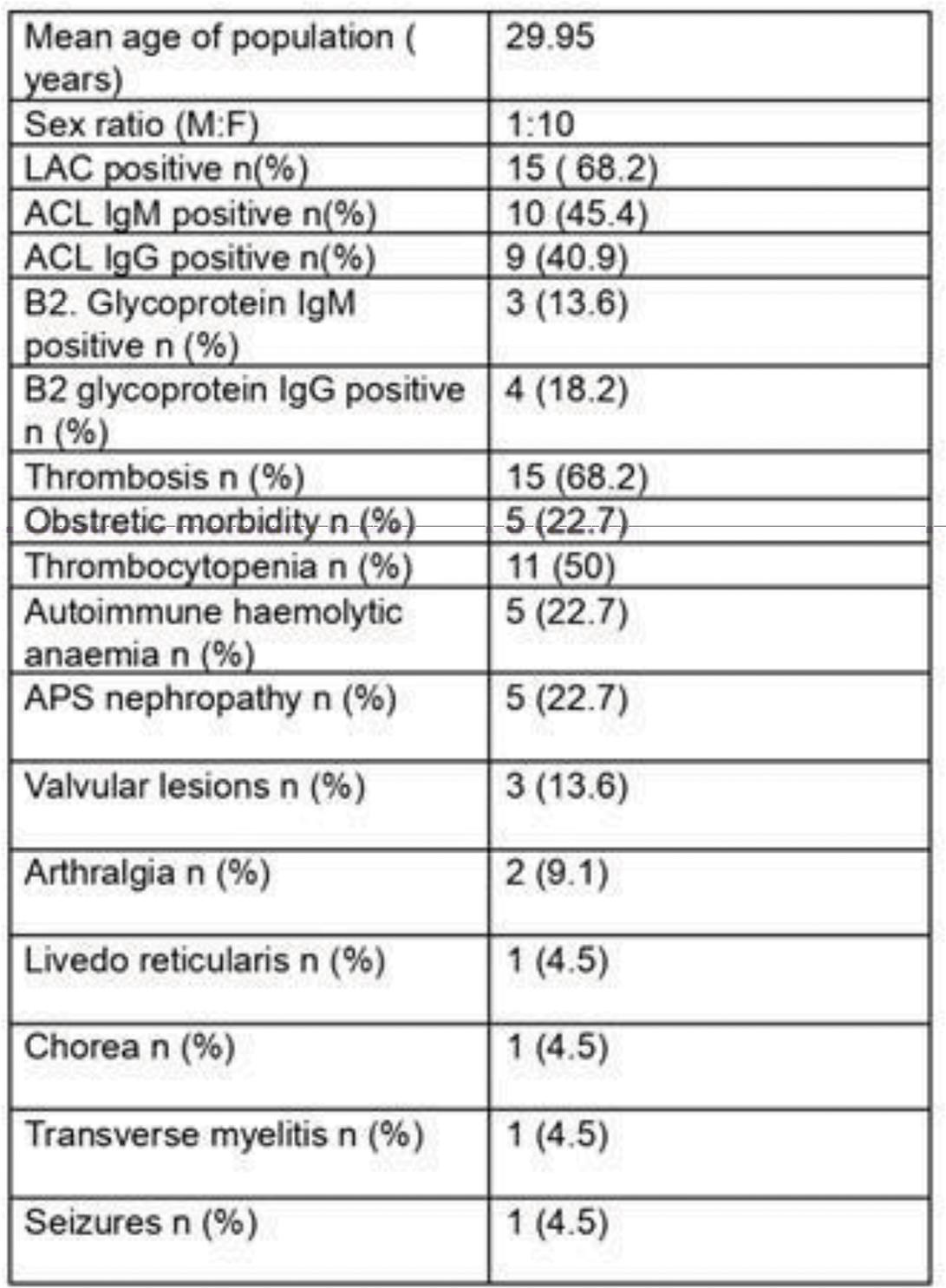
POS296
Phenotype of Antiphospholipid Syndrome in SLE vs Non SLE Cases – Spectrum of Clinical and Laboratory Findings-A Single Centre Retrospective Study
To examine the clinical manifestations of APS in patients with and without SLE. To determine the spectrum of positivity for LA. ACL and β2GPI in SLE vs non SLE group
The titres of ACLA and (IgG and IgM) and β2GPI differed between 2 groups as represented in figure 1a, 1b.
Image and Bar Table 1
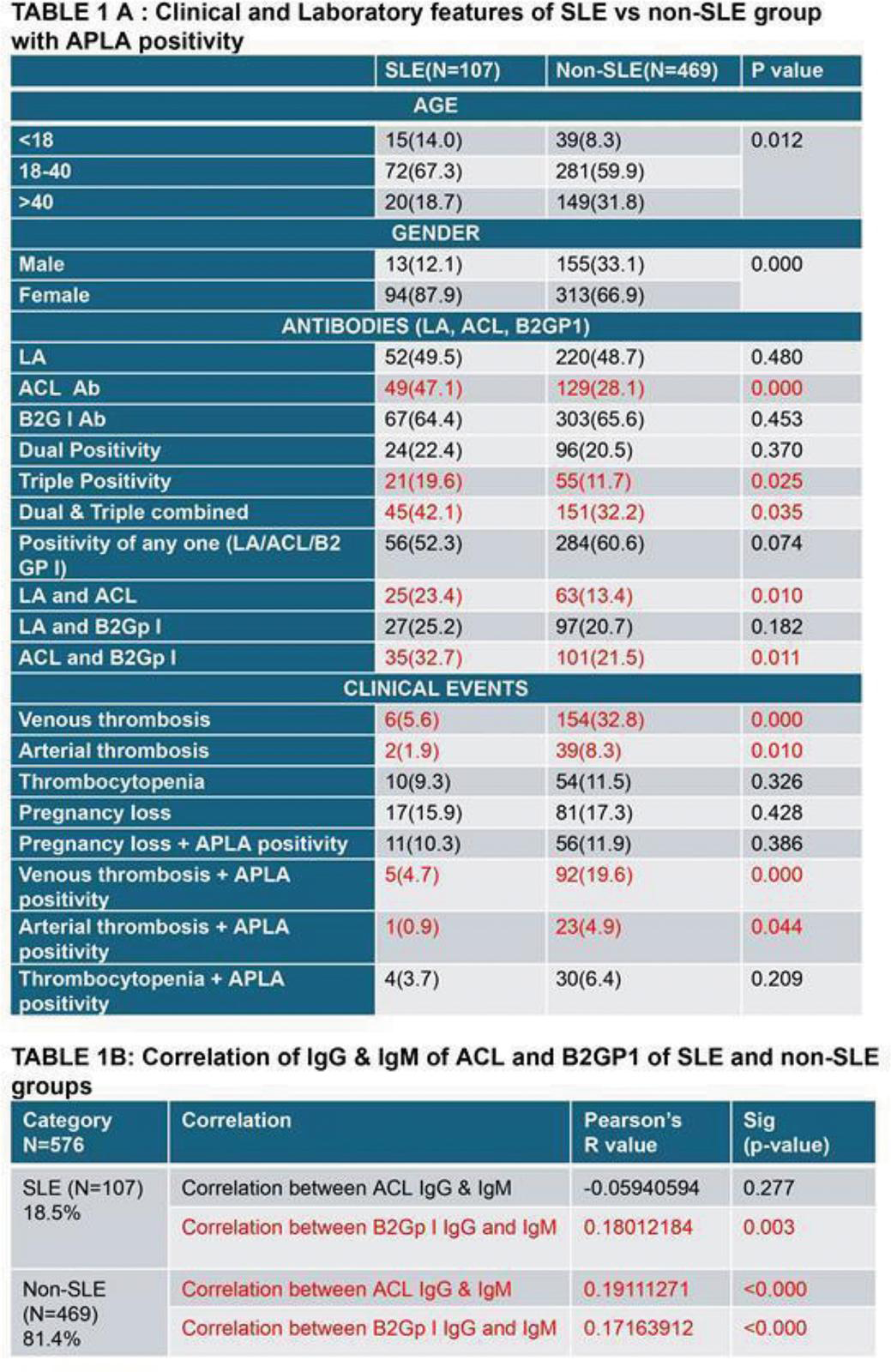
Image and Bar Table 2


POS297
A Study of Association of Pulmonary Hypertension in Connective Tissue Disorders
Estimate the frequency of PH in patients with CTD.
Study the potential clinical and laboratory risk factors for PH in patients with CTD. Compare the severity of PH with the duration of the CTD.
(Complete study is expected to finish by November 2024 for the complete data and analysis.)
1. Cansu DÜ, Korkmaz C. Pulmonary hypertension in connective tissue diseases: epidemiology, pathogenesis, and treatment. Clin Rheumatol. 2023;42 (10):2601-2610.
POS298
Interstitial Pneumonia with Autoimmune Features (IPAF): Clinical; Radiological and Serological Profile of Patients – A Single Centre Experience
A) Clinical Domain:
IPA – 11
Puffy hands – 2
Skin fissuring – 2
Raynaud’s phenomenon – 3
Sine pattern – 9
B) Serological Domain:
Anti SSA/SSB – 14
Anti SnRNP – 3
RF – 2
ACA – 2
Others – 6
C) Radiologic Domain:
NSIP – 21
OP – 1
UIP – 5.
Other common variables observation were as follows:
Average age of presentation: 40- 60 years (15n). out of 27, six were male Average duration of symptoms at referral: 2 years (6months - 4 years) Restrictive pattern in PFT:Mild (5) moderate (18) severe (4n) PHTN: 8n - Mild (5) severe (2) moderate (1) GERD: 4n Prior ATT intake: 6 Non smokers: 24 Covid shots - 22 patients had recieved 2 covid shots already. Patients with history of significant o2 dependent covid infection were excluded. NFC: done in 14 numbers (6 had SSc pattern) (8 non specific)
Ten patients had other non criteria symptoms like numbness of distal extremities, sicca symptoms, skin tightening, subcutaneous nodules etc. Other non criteria antibodies like anti pm scl 70, anti ku, anti CenP were seen in 4 patients. Though UIP not included in morphological domain of HRCT IT was present in 5 patients, but fulfilling other two domains.
Therefore, revision of current IPAF criteria stays as the need of the hour.
POS299
Clinical Profile and Treatment Outcomes of Systemic Polyarteritis Nodosa- Largest Series from Asia
1. Lightfoot RW, Michel BA, Bloch DA, Hunder GG, Zvaifler NJ, McShane DJ, et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum. 1990 Aug;33 (8):1088–93.
Image and Bar Table 1

Image and Bar Table 2

POS300
Multi-Vessel Intimal Medial Thickness as A Biomarker for Disease Modification in Takayasu Arteritis: A Prospective Observational Study
Image and Bar Table 1

Image and Bar Table 2
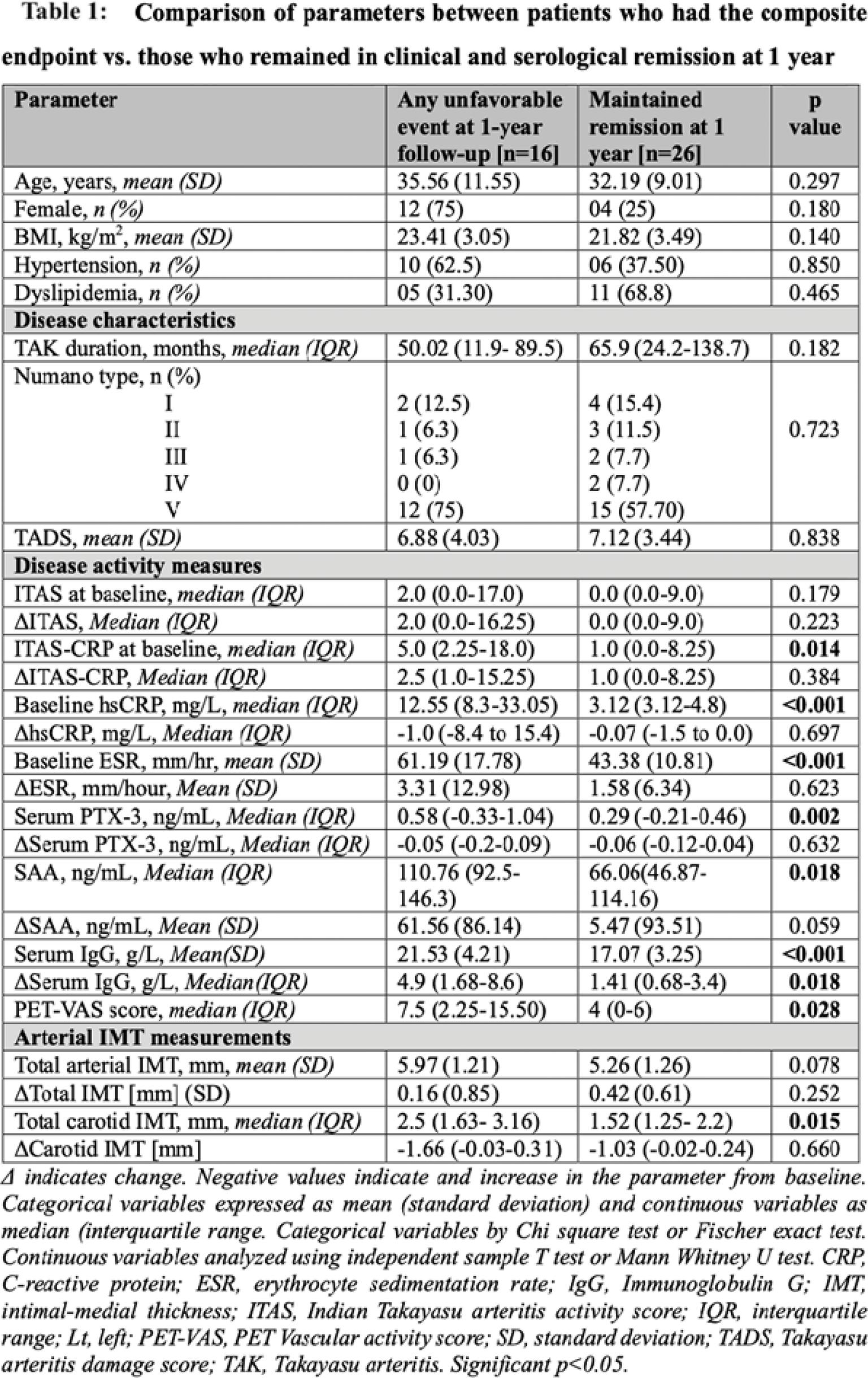
POS301
Interventions in Patients with Takayasu Arteritis, their Clinical and Angiographic Associations, and Prognostic Relevance - A Cohort Study
Image and Bar Table 1

POS302
Efficacy of Tocilizumab in Remission Induction in Patients with Takayasu Arteritis: A Multicentric Retrospective Study from Western India
Aditi Patankar1, Nilesh Nolkha2, Sunil Singh3, PV Mamtha4, Shalini Suralkar5, Kavita Krishna6, Aditi Erande7,
The mean dosing interval of TCZ was once in 8 weeks in the intravenous group. TCZ was administered for an average of 14.75±11.04 months. A significant 90% (18/20) achieved CR, and 50% (9/18) maintained SR with an average time to remission 3.5±2.7months and a steroid dose of 5.4±2.3mg/day. The dosage of concurrent DMARDs could be tapered in 6 patients.
Two patients had refractory disease, with one cardiovascular-related mortality. 8 relapsed, with an average time to relapse of 6.3±4.6months. 7/8 relapses were minor, while 1 was major. Relapses were attributed to reduced TCZ frequency in 6 patients, discontinuation due to pregnancy in 1, and a lower dose in another due to financial constraints. After adjusting dosage or frequency, 7 of the 8 relapsed achieved remission. Overall, 17 patients had relapse-free survival on TCZ for an average of 11.2±6.06months. 4 patients successfully discontinued TCZ, remaining in remission for an average of 17 months.
Image and Bar Table 1
Image and Bar Table 2

POS303
Biologicals in Management of Takayasu Arteritis – A Single Center Retrospective Study
To study the baseline characteristics, type of vessel involvement in imaging and inflammatory markers in Takayasu arteritis patient requiring Biologicals. To study the indication of Biologicals in these patients. To Compare the imaging of these patients - pre and post Biologicals. To study the efficacy of Biologicals in these patients.
14 of these patients had Type V vessel involvement in imaging.5 of them had cardiomyopathy and 4 had Intra-cranial involvement. Post Biologicals, 10 patients had resolution of symptoms over 3-6months.5 of these patients did not develop any new symptoms.5 of them developed new clinical symptoms out of which 4 required switching of these biologicals but still did not have clinical improvement.
7 of these patients had a follow up imaging over a period of 6-12 months out of which 3 had no progression, 3 had increased metabolic activity in the involved vessels in PET-CT and 1 had regression of metabolic uptake in PET-CT.
Image and Bar Table 1

Image and Bar Table 2

POS304
A Single Centre Follow Up Study of Takayasu Arteritis Patients and Comparison of Patients with and without Cerebrovascular Complications
To study the clinical presentation, angiographic features and the treatments initiated with follow up in Takayasu Arteritis patients attending a tertiary care center. To compare the presenting factors, angiographic features between patients with and without stroke and identify any prediction models for identifying patients at risk of Stroke.
Patients with and without stroke when compared revealed significant difference in visual disturbances (p<0.05), arterial segments involved which include left common carotid artery (LCCA) and left vertebral artery (LVA) (p<0.05).
Image and Bar Table 1

Image and Bar Table 2
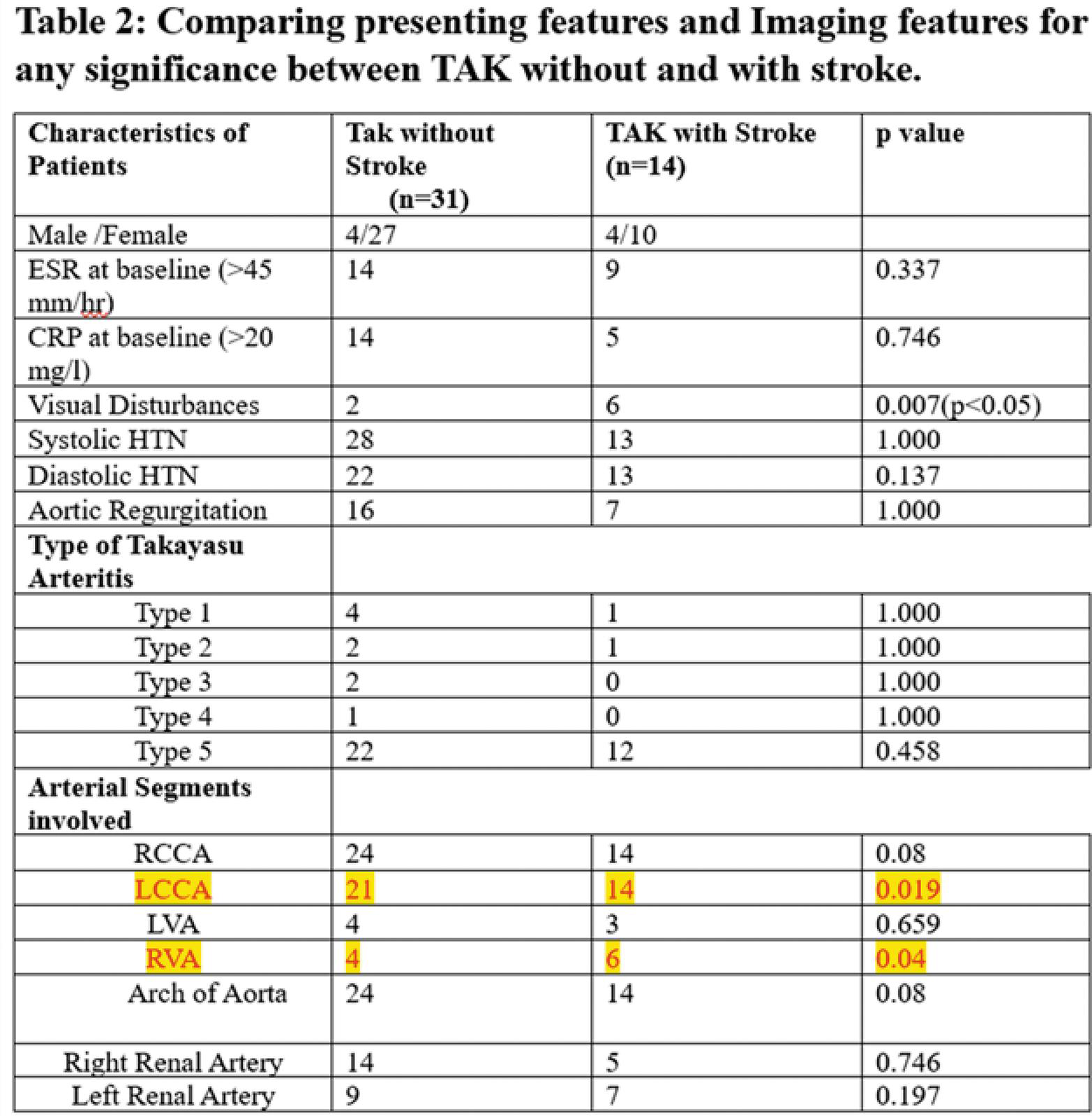
POS305
Small Vessel Involvement and Its Dysfunction in Takayasu Arteritis: A Single Centre Cross Sectional Study
Takayasu Arteritis (TA) is a rare, chronic, inflammatory large-vessel vasculitis with potential small vessel involvement. Emerging evidence suggests TA may involve medium and small vessels, affecting the eyes, heart, and skin. Retinal changes, myocarditis, and skin lesions indicate small vessel involvement.
Our study aimed to elucidate small vessel dysfunction in TA by examining Nailfold capillaries, assessing flow-mediated dilatation (FMD), and investigating retinal vessels. We correlated the observed small vessel dysfunction in these parameters with the corresponding large vessel involvement.
Our methodology involved comprehensive clinical evaluations, including Nailfold capillaroscopy (NFC), FMD measurement, and retinal assessments using fluorescein angiography (FFA) and optical coherence tomography (OCT) and OCT Angiography. Arterial involvement was determined by CT and PET angiography.
The study included 35 TA patients, predominantly females (85.7%) with a mean age of 29.9 years. Results revealed Subclavian artery involvement was observed in 41% unilaterally and 31% bilaterally, while common carotid artery involvement was seen in 51% unilaterally and 31% bilaterally. Abnormal nailfold videocapillaroscopy (NVC) findings were present in 40% of patients, with reduced density as the most common abnormality, but these did not correlate with large arterial involvement, suggesting direct microcirculatory involvement in TA. FMD was abnormal in 31.4% of patients, with no correlation to subclavian artery involvement, indicating endothelial dysfunction due to microcirculation effects. Fundus fluorescein angiography (FFA) revealed abnormalities in 74.3% of patients, with Grade 3 Takayasu Retinopathy and dilated vessels being most common. OCT showed abnormal central macular thickness (CMT) in 28.6% of patients, predominantly with thinned macular thickness, which did not correlate with common carotid artery involvement. The foveal avascular zone (FAZ) area was larger at the deep capillary plexus level in OCT angiography (OCTA), indicating significant impact on these vessels.
Overall, by visualizing the structural changes in the small vessels of nailfold and retina and the functional changes in the small vessels by FMD, we postulate that small vessel involvement and dysfunction occurs in TA and is independent of the large vessel involvement. This is further corroborated by the fact that the changes in NVC, FMD and CMT had significant correlation on either side signifying a systemic process. We detected the changes without any disease manifestation of small vessel vasculitis and thus these changes may represent sub clinical findings. Further studies are required to determine the probable clinical effects and the effects of these changes on the disease manifestations of TA.
Image and Bar Table 1

POS306
Clinical and Epidemiological Profile of Takayasu Arteritis Patients From A Tertiary Care Centre in North Karnataka: One Year Data 2023-2024
Image and Bar Table 1

POS307
Clinical Profile and Treatment Outcomes in Patients with Early Takayasu Arteritis
All patients received corticosteroids at dose of 37.0±11.6 mg/day along with non-biologic DMARDS in 19 (86.4%) and biologics in 3 (13.5%).
During a median follow up period of 32 (18-56) months, 18 (81.8%) had complete/partial remission. Fourteen (63.6%) patients relapsed at median duration of 12 (6.5-17.5) months which required immunosuppressant switch in 13 (59.1%) patients (>1 switch in 9patients). Among 14 patients who underwent repeat imaging, 8 (57.1%) had progression at a median of 42 (95%CI 8.0-76.0) months while 6 (42.9%) had stable disease.
At the last follow up, 18 (81.8%), 10 (45.5%) and 8 out of 14 (57.1%) were in clinical, laboratory and angiographic stable disease respectively with steroid dose of 5 (2.5-7.5) mg/day. Sixteen (72.7%) patients had symptoms/signs of vascular ischemia while only 6 (27.3%) developed new pulse loss. TADS score remained ≤1 in 6 (30%) patients at last visit with a median TADS 3 (1-5). None of baseline parameters predicted relapses or angiographic progression.
Image and Bar Table 1

Image and Bar Table 2
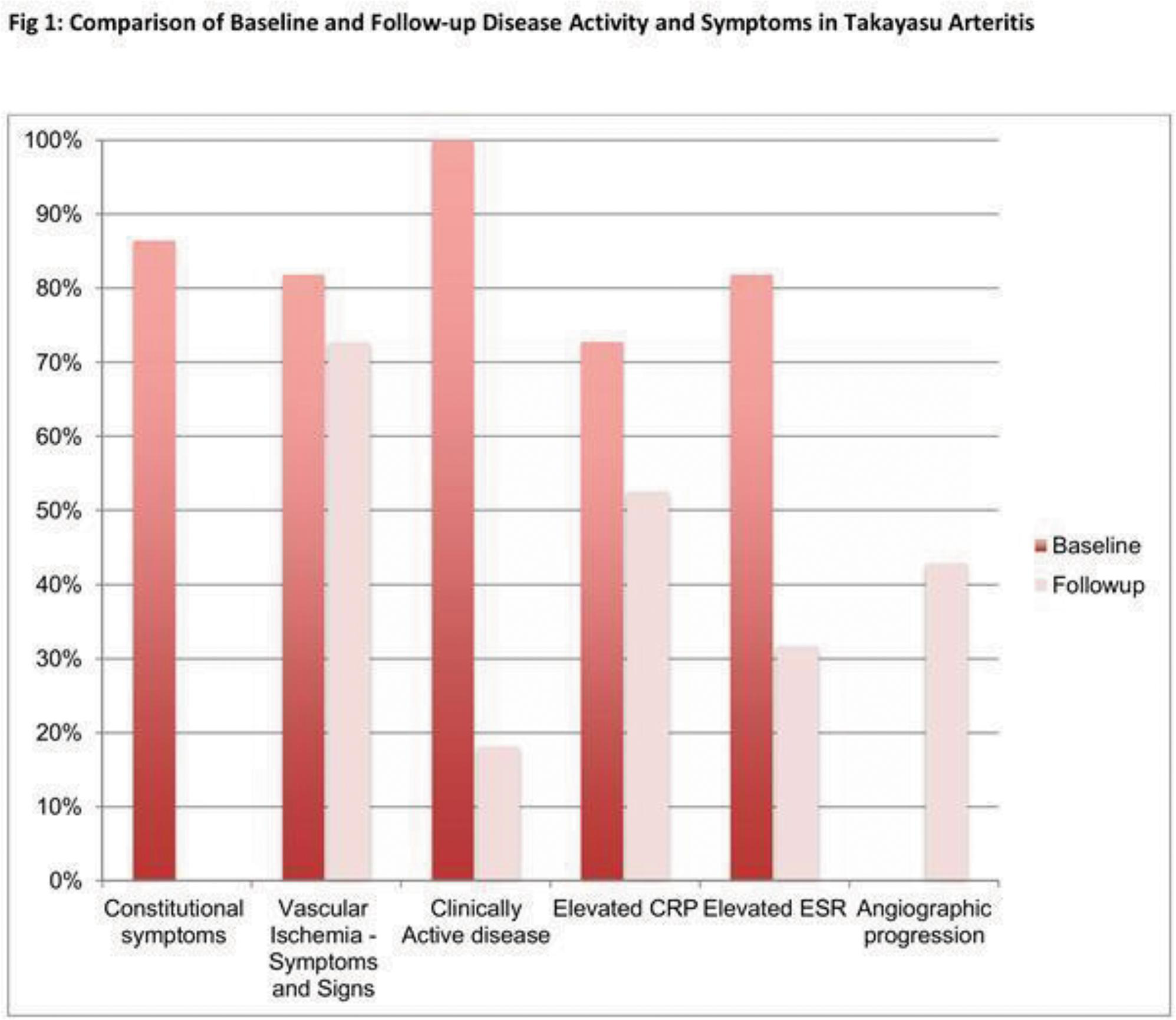
POS308
Efficacy of Biological Agents in Indian Patients with Refractory Takayasu Arteritis- A Retrospective Study from A Tertiary Care Center in South India
Image and Bar Table 1
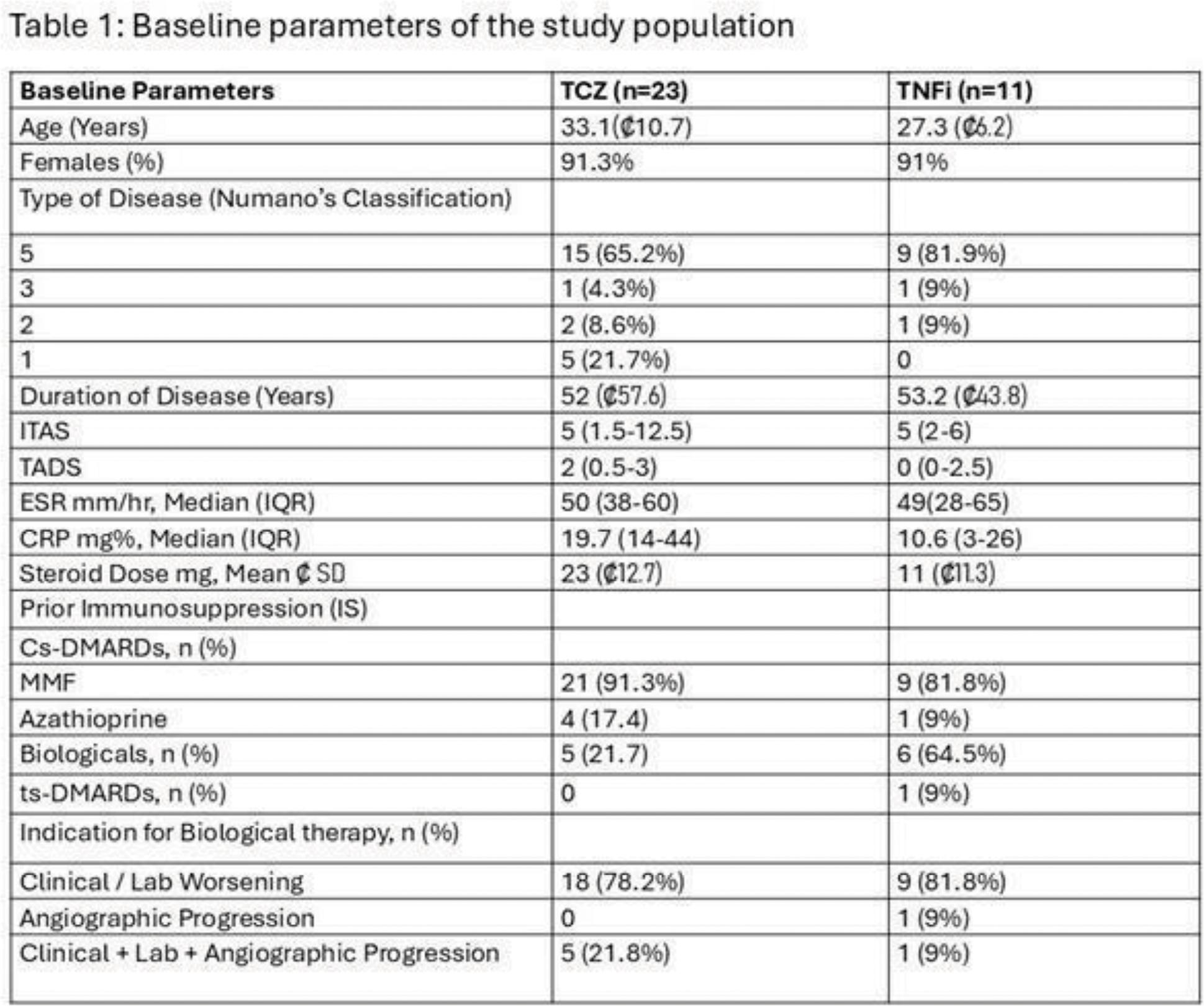
Image and Bar Table 2

POS309
Efficacy and Safety of Tocilizumab in Patients with Refractory Takayasu Arteritis
Image and Bar Table 1

POS310
Late-Onset Takayasu Arteritis: Preliminary Observations of Clinical Manifestations and Vascular Involvement
Image and Bar Table 1

Image and Bar Table 2

POS311
A Case Series (06) of Takayasu Arteritis – Serendipity Versus Structured Approach
Image and Bar Table 1

POS312
Triple Vessel Coronary Artery Disease in A 30 Year Old Female - A Rare Presenting Symptom of Takayasu Aortoarteritis
POS313
“Unmasking Takayasu Arteritis: A Rare Cause of Refractory Hypertension in the Elderly”
Image and Bar Table 1

Image and Bar Table 2
POS314
Comparison of the Clinical Profiles of MPO V/S PR3 Positive AAV Patients, A Cross-Sectional Study
Defining clinical characteristics of the two main antibodies to PR3 and MPO gives deeper insight into the evolvement of the disease and its organ involvement along with disease severity, thus guiding the clinician into making more confident and robust therapeutic and prognostic decisions.
1. Rhee, R. L., Hogan, S. L., Poulton, C. J., et al. (2016). Clinical features and outcome of anti-PR3 vs. anti-MPO ANCA-associated vasculitis. Journal of the American Society of Nephrology, 27 (6), 1883-1890.
2. Cornec, D., & Specks, U. (2020). ANCA-associated vasculitis: Clinical characteristics and outcomes. Nature Reviews Rheumatology, 16 (2), 103-114.
3. Jennette, J. C., Falk, R. J., & Bacon, P. A. (2013). 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitis. Arthritis & Rheumatism, 65 (1), 1–11.
Image and Bar Table 1
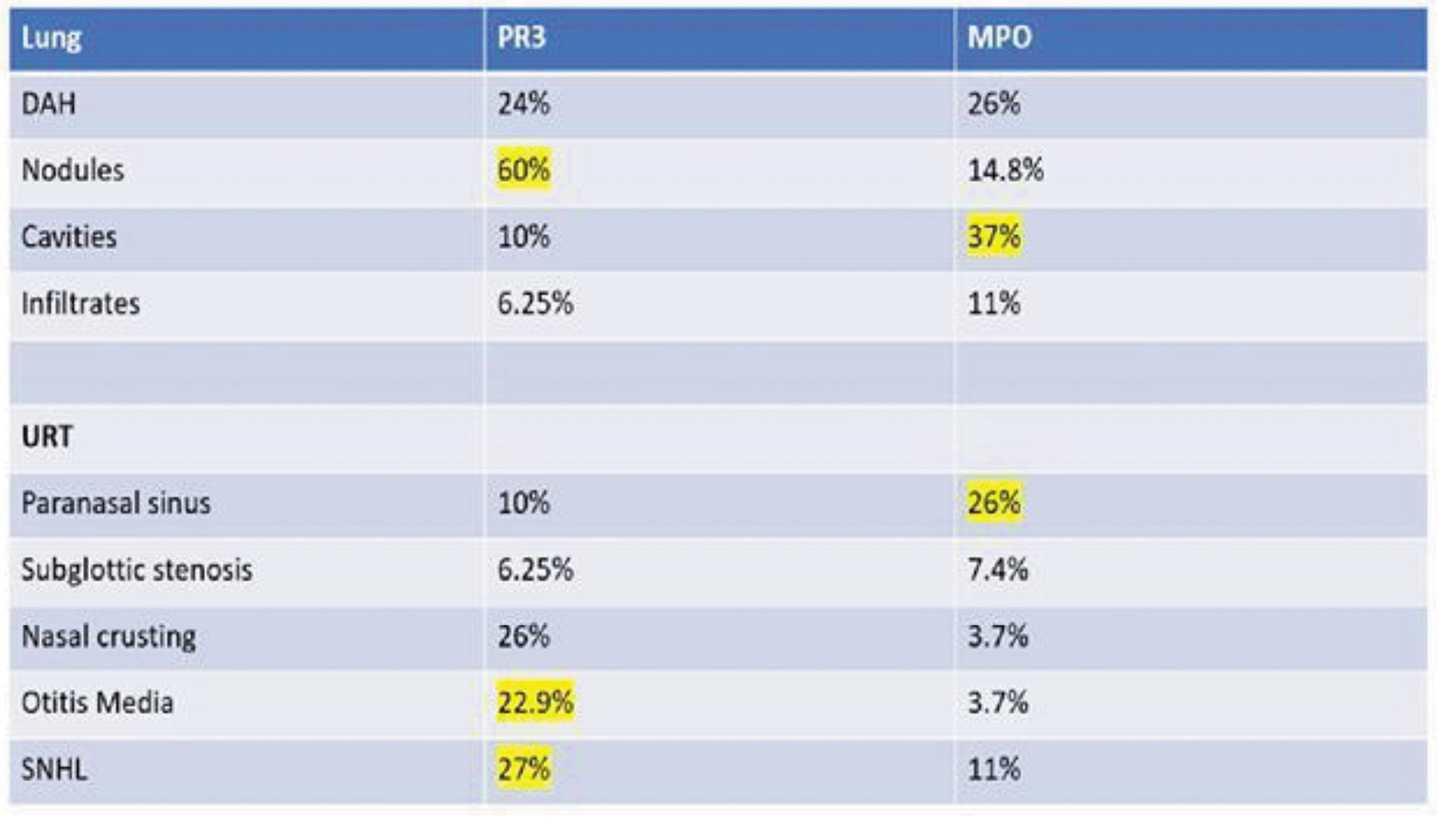
Image and Bar Table 2
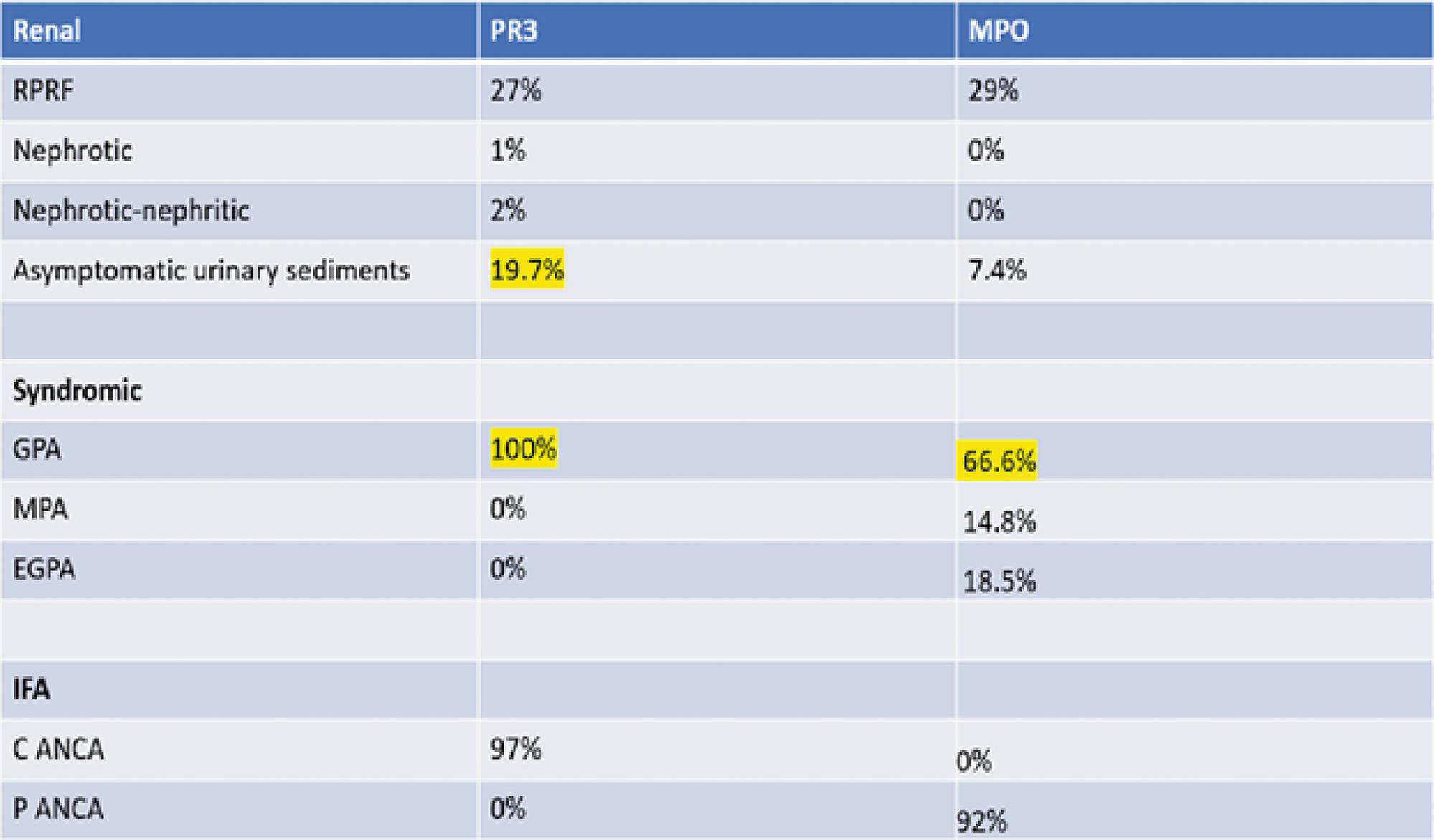
POS315
Spectrum of Vasculitic Neuropathy Among Patients of Systemic Autoimmune Rheumatic Diseases
Image and Bar Table 1

Image and Bar Table 2
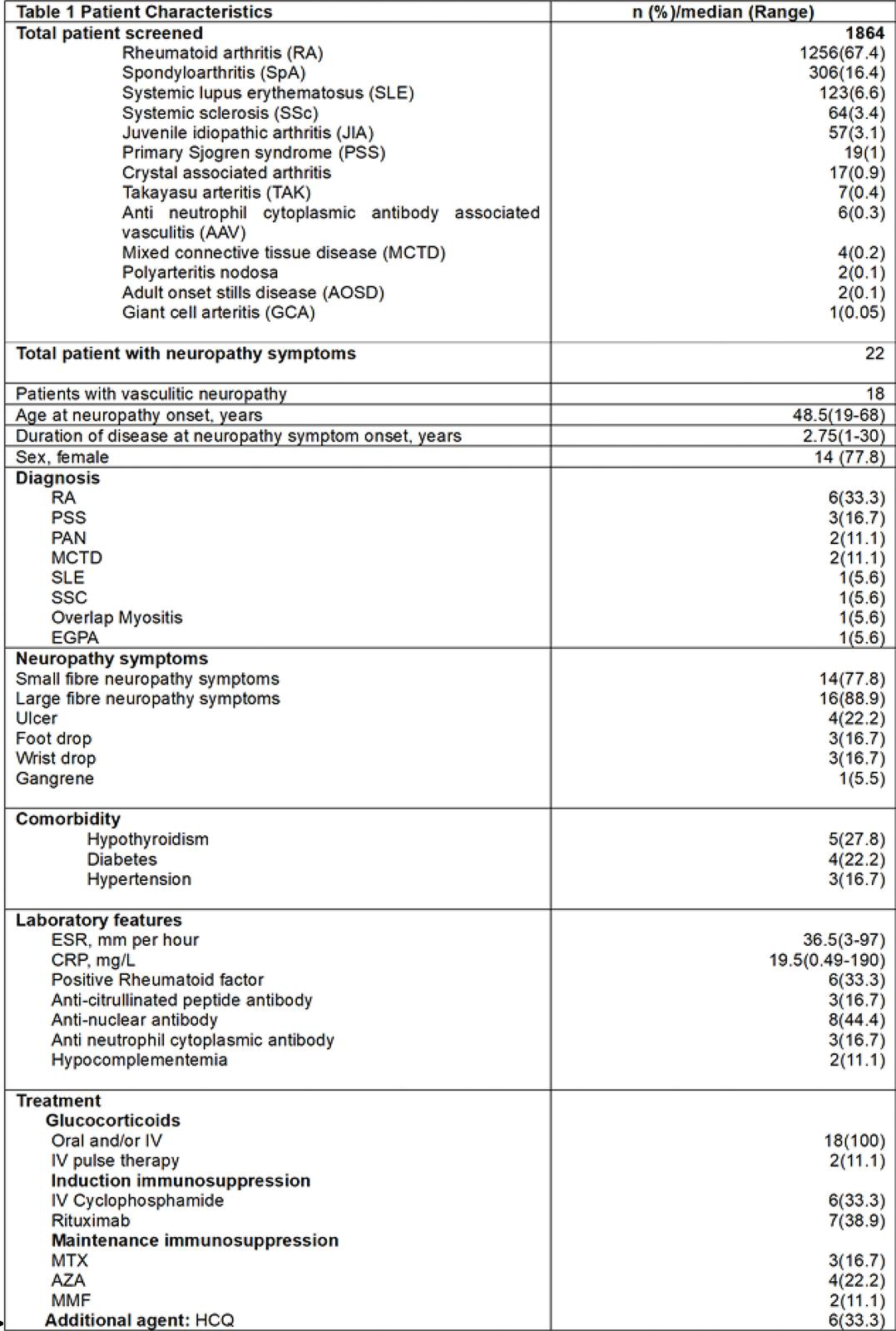
POS316
A Cross Sectional Study Classifying AAV Patients Based on Renal Involvement to Predict Prognosis and Disease Characteristics of AAV.
In clinical practice, the differences between PR3-AAV and MPO-AAV could possibly be used for therapeutic diversity in future treatment, such as intensity of treatment or duration of maintenance therapy. Questions also remain about differences in prognosis between AAV without and with renal involvement, especially in those patients who need renal replacement therapy (RRT).
Chi square test was used for analysis of results with a p value of 0.05 being significant at a confidence interval of 95%.
1. de Joode AA, Sanders JS, Stegeman CA. Renal survival in proteinase 3 and myeloperoxidase ANCA-associated systemic vasculitis. Clin J Am Soc Nephrol. 2013;8 (10):1709-1717. doi:10.2215/CJN.01020113
2. Renal and Systemic Vasculitis, Meghan Free et al. Comprehensive Clinical Nephrology, 26, 294-308.e3
3. Sethi S, Fervenza FC. Standardized classification and reporting of glomerulonephritis. Nephrol Dial Transplant. 2019;34 (2):193-199. doi:10.1093/ndt/gfy220
Image and Bar Table 1

Image and Bar Table 2
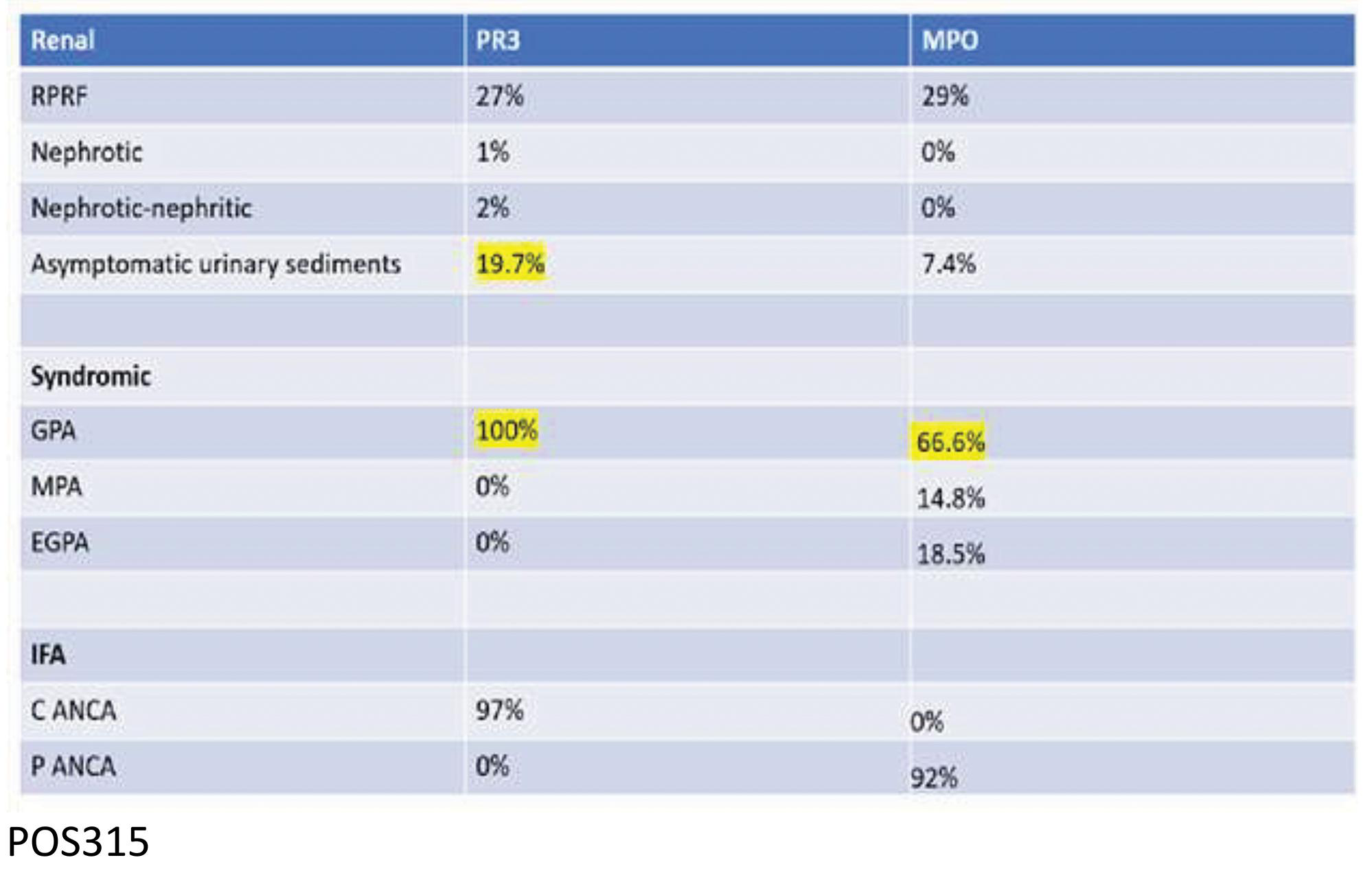
POS317
Faces of ANCA Associated Vasculitis: Clinical Presentation and Insight
Image and Bar Table 1

Image and Bar Table 2

POS318
Tofacitinib as An Effective Treatment for Refractory Cutaneous Polyarteritis Nodosa: A Case Series
Diagnostic delays varied, with 4 patients experiencing 1-year delays, 10 patients 2-5 years, and 2 patients delays of 17 and 23 years.
Diagnosis and treatment initiation occurred at our center for 3 patients; others were referred from external facilities.
Seven patients had high cumulative steroid doses, with one receiving approximately 19, 370 mg over six years.
All patients presented with ulcers (3-4 per patient) on both lower limbs; one patient had an upper limb ulcer, and none had trunk ulcers. Axonal sensory neuropathy was confirmed in 8 patients. Skin biopsies indicated medium vessel vasculitis, and viral markers for hepatitis B and C were negative.
The median duration of disease before initiating Tofacitinib was 2-6 years in 9 patients, 7-13 years in 5, and 24-26 years in 2. Tofacitinib was initiated at 5 mg twice daily. All patients showed significant reductions in ulcer size and number, with complete healing in 7 patients within one month, 5 patients within 2-4 months, and 4 patients within 6-8 months. Improvements in pain and quality of life were noted. No major adverse events like dyslipidaemia or infections were reported, and Tofacitinib was well tolerated.
POS319
Moyamoya Disease – Primary CNS Vasculitis?
RNF213 gene has been established as MMD susceptibility gene with autoimmune background and second hit hypothesis. Its commonly seen in Asian children between 10 to 14 years of age.
Our case report is of a 11year old girl who has history of recurrent seizures for the past one year with poor treatment compliance.
The patient had no unilateral weakness, speech difficulties, blurring of vision, involuntary movements or difficulty thinking.
During evaluation fundus examination revealed Papilloedema, normal BP, heart was normal and no other neurological manifestations were found.
CRP: 20 mg/l ESR: 38mm/hr CBC: 8800cells/cu.mm RBC count: 4.75 mls/cu.mm Peripheral smear: RBC normocytic normochromic Platelet count: 524000 cells/cu.mm Liver profile: normal Serum sodium: 14mEq/L Serum pottsium: 3.9 mEq/L Serum chlorine: 106 mEq/L
MRI Brain with contrast study revealed diffuse intimal thickening of left CCA bifurcation, cervical and intracranial course of left ICA. Diffuse disease of both cavernous and supraclenoid ICA seen. Priming of M1 to M4 segments of left MCA, A2 to A5 segments of right ACA seen. Chronic lacunar infarcts noticed in left ganglio capsular region, corona radiata and central semiovale.
EEG was abnormal, showed bilateral paromysmal bursts of epileptiform discharge.
ECG and ECHO were normal and USG abdomen was normal.
But is this a primary cerebral vasculitis or vasculopathy?
(Scan images shall be displayed during conference)
POS320
A Comparative Study to Assess the Efficacy & Safety of Tailored Vs. Fixed Dose Regimen of Rituximab During Maintenance Treatment in ANCA Associated Vasculitis
Image and Bar Table 1

Image and Bar Table 2
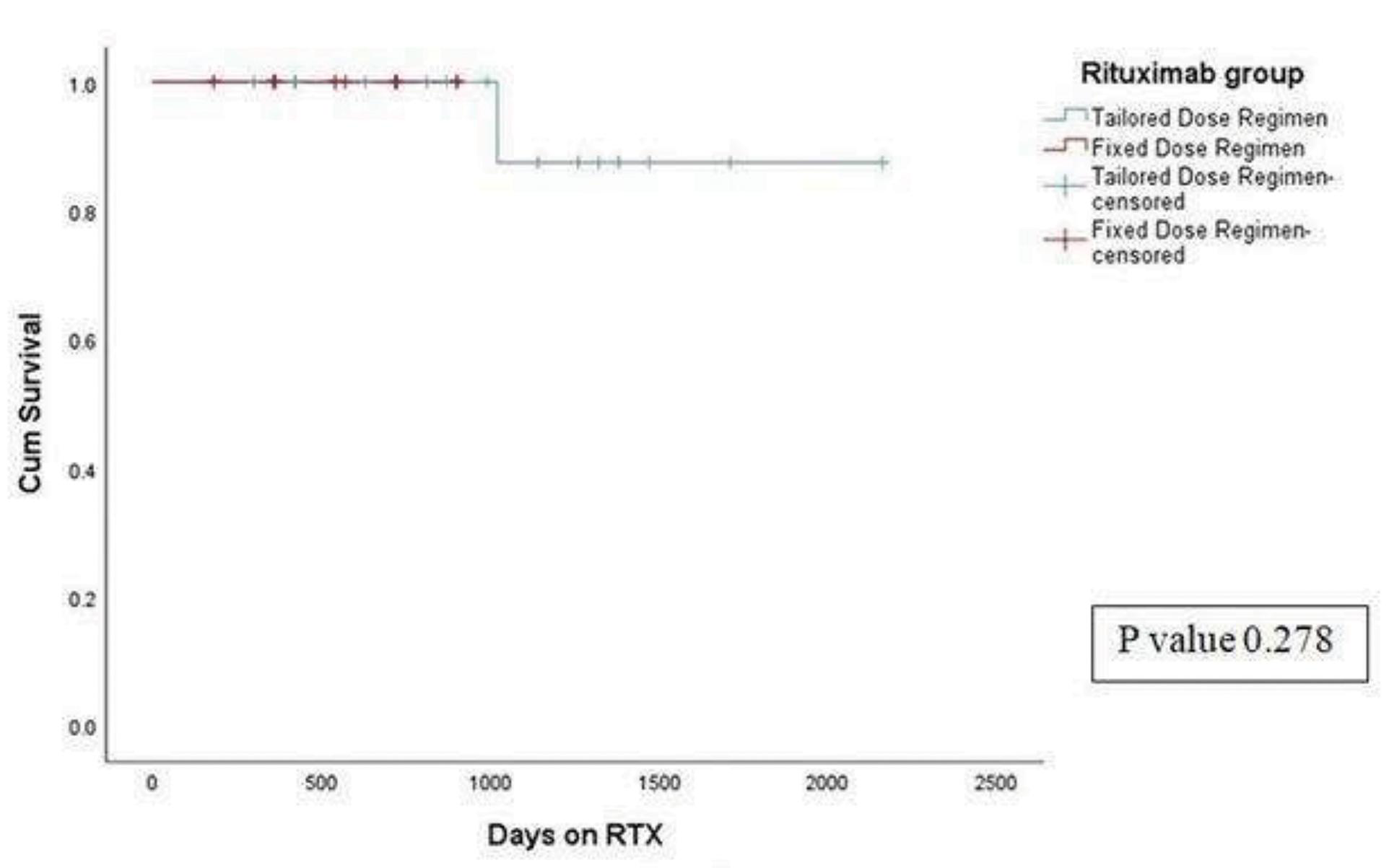
POS321
Outcome of Adult IgA Vasculitis in A Teritiary Care Centre from 2005 to 2023
Out of 72 patients with IgAV, 36 patients received systemic corticosteroids and 35 required additional immunomodulators. During a median follow up period of 3 years, 41.67% (30) patients relapsed. Most commom relapse seen with skin manifestations (53.3%). In our cohort, treatment with systemic corticosteroids alone had a complete remission (CR) of 77.8% and corticosteroid with additional immunomodulators had CR of 85.7% at 6 months (p=0.499). The relapse on median follow up of 3 years was 58.3% in the corticosteroid alone group and 25.7% in the corticosteroid with additional immunomodulator group (p=0.005).
Renal involvement and treatment response is given in table 1&2 respectively.
On follow up, 5 patients (7%) had developed CKD (stage3) out of which hypertension was seen in 4 patients. On initial biopsy 4 of them had fibrocellular crescents and 3 had fibrinoid necrosis.
Image and Bar Table 1
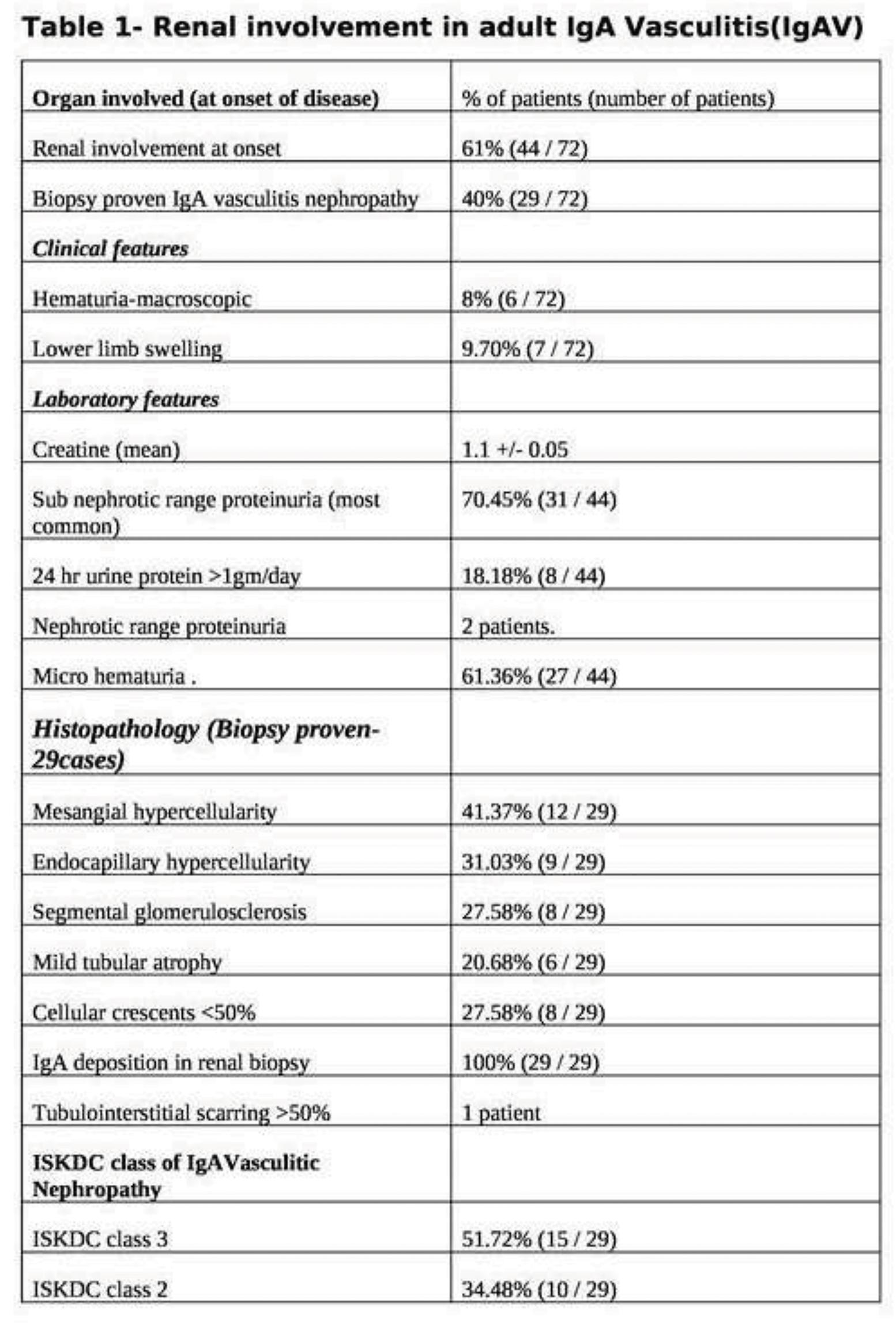
Image and Bar Table 2
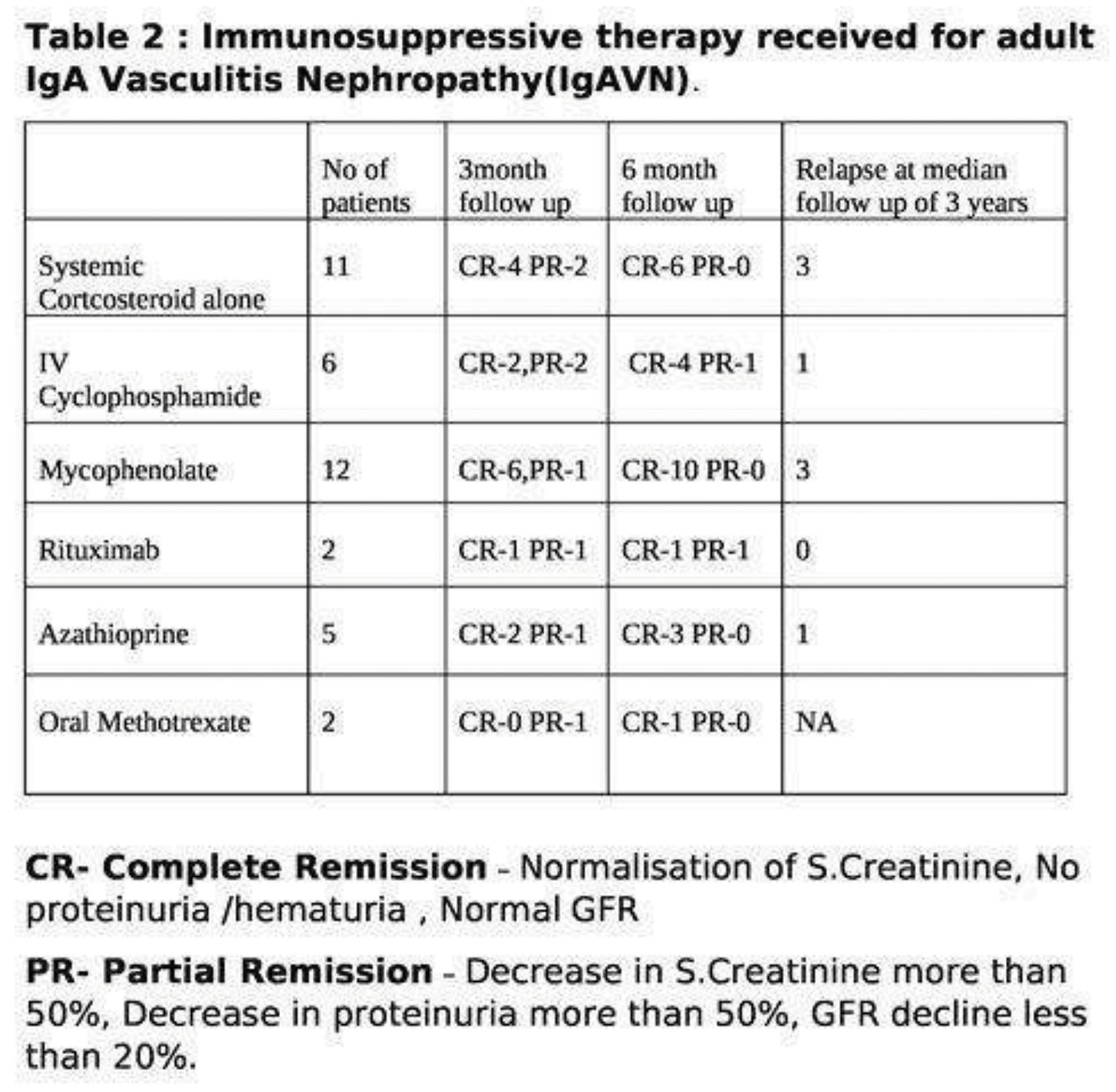
POS322
Does Persistent Laboratory Quiescence Signify A Monophasic Disease in Takayasu Arteritis?
During a follow-up period of 44 (24-71) months, 37 (42%) had relapse of clinical activity as per ITAS>0. Overall, 13 (14.7%) patients had angiographic progression while 75 (85.3%) had stable disease. Nine of 13 (69.2%) progressors had one visit with clinical relapse which is significantly higher than in non-progressors (28, 37.3%), p=0.038. Higher ESR, and TADS, bruit and involvement of left subclavian artery at baseline were associated with angiographic progression. However, bruit at presentation was the only parameter associated with progression in multivariate analysis. The increment in clinical damage (TADS) was significantly higher in progressors (1 (0.5-3)) than non-progressors 0 (0-1).
Image and Bar Table 1

Image and Bar Table 2

POS323
Clinical Spectrum and Management Strategies of IgA Vasculitis: Insights from Two Tertiary Care Centers in South India
1. Audemard-Verger A, Terrier B, Dechartres A, Chanal J, Amoura Z, Le Gouellec N, et al. Characteristics and management of IgA vasculitis (Henoch-Schönlein) in adults: data from 260 patients included in a French multicenter retrospective survey. *Arthritis Rheumatol.* 2017;69 (9):1862-70. DOI: 10.1002/art.40178.
2. Villatoro-Villar M, Crowson CS, Warrington KJ, Makol A, Ytterberg SR, Koster MJ. Clinical characteristics of biopsy-proven IgA vasculitis in children and adults: A retrospective cohort study. Mayo Clin Proc. 2019;94 (9):1769-1780. DOI: 10.1016/j.mayocp.2019.04.034
Image and Bar Table 1

POS324
A Case of Selective Serotonin Reuptake Inhibitor (SSRI) Induced Small Vessel Vasculitis Presented with Facial Palsy
POS325
ANCA Vasculitis with Ear, Nose and Throat Involvement: Long-Term Outcomes from a Single-Center Cohort
POS326
Renal Blitzkrieg: Anti-GBM Disease and Aggressive Glomerulonephritis in a Young Male
Image and Bar Table 1

Image and Bar Table 2

POS327
Behçet’s Disease and Crohn’s Disease: A Tale of Two Gastrointestinal Pathologies
Bechet’s disease (BD) is an idiopathic, chronic, relapsing-remitting mixed vessel vasculitis, characterized by recurrent oral and genital aphthous ulcers, ocular disease, skin lesions, and systemic organ involvement, primarily targeting young adults. GI manifestations are seen in approximately 10%-15% of patients typically appear 4.5–6 years after oral ulcers onset, and the involved sites and endoscopic views often resemble those of Crohn’s disease.
We present the case of a middle-aged male who presented with a 7-day history of fever, abdominal pain, and haematochezia with loose stools. On general examination, the patient exhibited oral aphthous ulcers and pustular lesions on the back and lower limbs, with the systemic examination otherwise normal. Laboratory investigations revealed elevated erythrocyte sedimentation rate and white blood cell count, with normal liver function tests, amylase, and lipase levels. With an initial diagnosis of acute dysentery, the patient was started on ceftriaxone. Despite the resolution of loose stools, the patient continued to experience persistent abdominal pain. Ultrasound imaging showed mild hepatomegaly, while computed tomography of the abdomen revealed ileocecal wall thickening and multiple enlarged lymph nodes in the right iliac fossa. Differential diagnosis included Bechet’s disease and Crohn’s colitis. A Pathergy test was conducted and yielded a positive result. Subsequently, a colonoscopy was performed with a biopsy of the ascending colon and cecum. Histopathological examination revealed necro-inflammatory debris surrounded by dense mixed inflammatory cells and perivascular inflammatory cell infiltrate, and, most importantly, no granulomas - findings suggestive of Bechet’s disease. The patient was treated with intravenous methylprednisolone and responded well to the therapy.
This case highlights the importance of differentiating between Crohn’s disease (CD) and Bechet’s disease (BD) colitis which is critical due to their distinct treatment regimens and potential for different complications. Only a limited number of case reports document Bechet’s disease presenting with gastrointestinal manifestations. Notably, one case by Eun-Sun Kim et al. highlights Bechet’s disease masquerading as Crohn’s disease. While both can present with similar gastrointestinal symptoms such as abdominal pain and ulcers, the nature, location, and progression of these symptoms vary between the two conditions, affecting prognosis and management. Accurate diagnosis is essential to avoid misdiagnosis and ensure effective, targeted treatment, which can significantly improve patient outcomes and reduce the risk of adverse effects from inappropriate therapy.
Image and Bar Table 1

POS328
Clinical Profile and Treatment Outcomes of Macrophage Activation Syndrome in Autoimmune and Rheumatic Diseases: A Retrospective Study
The most common clinical manifestations of MAS were fever (100%), lymphadenopathy (43.75%), and neuropsychiatric symptoms (43.75%). Splenomegaly and hepatomegaly were observed in 18.75% of patients. Cytopenia was present in all cases (100%), with median total leukocyte counts of 6514 cells/µL at MAS diagnosis. Hypofibrinogenemia occurred in 62.5% of cases, while hypertriglyceridemia, hyperferritinemia, elevated AST and LDH were observed in all patients (100%). Hemophagocytosis on bone marrow biopsy was seen in 28.5% of cases (Table 1).
In terms of diagnostic criteria, 87.5% of patients met the HLH-2004 criteria, and 100% fulfilled the Ravelli and 2016 consensus criteria for MAS. However, only 28.5% met the more stringent Parodi criteria for definite MAS.
High dose steroids were the first-line treatment, with either pulse methylprednisolone (MPS) or 1mg/kg prednisolone equivalent doses of dexamethasone being administered. Cyclophosphamide and cyclosporine were the most frequently used immunosuppressants. The median hospital stay was 20.5 days, and 31.25% of patients requiring ICU care. Despite treatment, two patients died, while the remaining 14 showed clinical improvement.
Image and Bar Table 1

Image and Bar Table 2

POS329
A Prospective Study to Look for Diagnosis of All Patients Presenting with Erythema Nodosum Like Rash in A Rheumatology Centre
TB screening with montoux test (5TU) and TB Quantiferon Igra was done in all patients. In abnormal chest x ray finding Contrast Enhanced CT Chest was also done. Six patients lost to follow up and were not being further diagnosed.
POS330
Safety of Rituximab in Autoimmune Diseases-An Audit from A Single Centre Biologic Registry
To identify risk factors for infection following first dose of rituximab in autoimmune disease. To ascertain infection free survival over 5 years in Rituximab treated autoimmune diseases.
Image and Bar Table 1

Image and Bar Table 2

POS331
Rituximab Use in Autoimmune Rheumatic Diseases. Experience from A Rheumatology Clinic in Dehradun, North India
1. Chandramohan P, Jain A, Antony G, Krishnan N, Shenoy P. Low-dose rituximab protocol in rheumatoid arthritis—outcome and economic impact. Rheumatology advances in practice. 2021;5 (1):rkaa077.
POS332
Rheumatological Conditions and Complementary and Alternative Medicines (CAM) Usage: A Cross-Sectional Study
Image and Bar Table 1

Image and Bar Table 2

POS333
A Study on Pulmonary Manifestations of Patients with Rheumatic Diseases in a Tertiary Center in Central India
The most typical manifestation of Rheumatoid disease associated pulmonary involvement is ILD.
Out of 19 Rheumatoid arthritis patients, 11 had ILD, 5 had bronchiectasis and 3 had Pleural effusion. Out of 15 SLE patients, 11 had pleural effusion and 4 had ILD. Out of 8 SSc patients, all (100%) had ILD. Out of 3 AIM, all had ILD.
As compared to Rheumatoid arthritis, Systemic sclerosis and AIM, SLE patient have a lower risk of ILD and common pathology in SLE is Pleural effusion.
High Anti-CCP titres were significantly associated with ILD development (p < 0.0001).
POS334
A Cross-Sectional Retrospective Multicenter Study to Evaluate the Phenotypic Spectrum of IGG4-Related Disease in India
Lalit Duggal1,
Almost every organ system can be involved in this disease.
Diagnosing IgG4-RD requires consideration of the clinical, serological, radiologic, and pathologic data and exclusion of potential mimickers (eg, malignancy).
The goals of therapy are to reduce inflammation and induce disease remission, with the aim of preserving organ function with glucocorticoids and other agents.
POS335
Clinical Profile of Cardiac Sarcoidosis in South India
POS336
Clinical Profile of Sarcoidosis and Response to Therapy- Retrospective study from a Tertiary Care Center in Southern India
To describe the clinical, radiological and laboratory profile of Sarcoidosis patients. To determine the clinical response to therapy.

50% of cases had Scadding stage 2 at presentation. The median ACE level at presentation was 62.0 (range 7.4-290.0). 7% (n=2) patients were misdiagnosed and initially treated as Tuberculosis, 3.7% (n=1) treated as Mumps Parotitis and 3.7% (n=1) treated as non-Hodgkin lymphoma. All except two patients received steroids with 12 patients receiving 1mg/kg and 11 patients 0.5mg per kg steroids. Steroid monotherapy was given in 13/27 patients.) 44.4% (n=6) were on Methotrexate, 29.6% (n=4) each on Mycophenolate Mofetil or Azathioprine as the steroid sparing agent. At the end of one-year, clinical response was seen in 15 (55.5%) patients, with relapses in 2 (7.4%) patients. 4 (14.8%) patients expired at the end of 1 year and 2 (7.45%) patients were lost to follow-up.
POS337
Single Organ Sarcoidosis: A Rheumatologists Perspective of 42 Cases
POS338
Clinical Profile and Outcome of Cardiac Sarcoidosis: A Retrospective Study from North India
Symptomatic CS had higher proportion of prediabetes (n=20, 89% vs n= 17, 56.7%, p=0.033) whereas mean HbA1c (6.2 vs 5.8, p 0.27) and Hypertension (n=10, 43.8 % vs n=8, 26.6% p=0.605 were not different.
During mean follow-up period of 26.7 months (SD), 45 patients (85%) showed improvement, 4 patients (7.5%) experienced worsening cardiac functions. There was four mortality, all were symptomatic CS, VT (n=2), RCMP with AF (n=1), sepsis (n=1). Three out of four mortality had ICS (Isolated CS).
Image and Bar Table 1
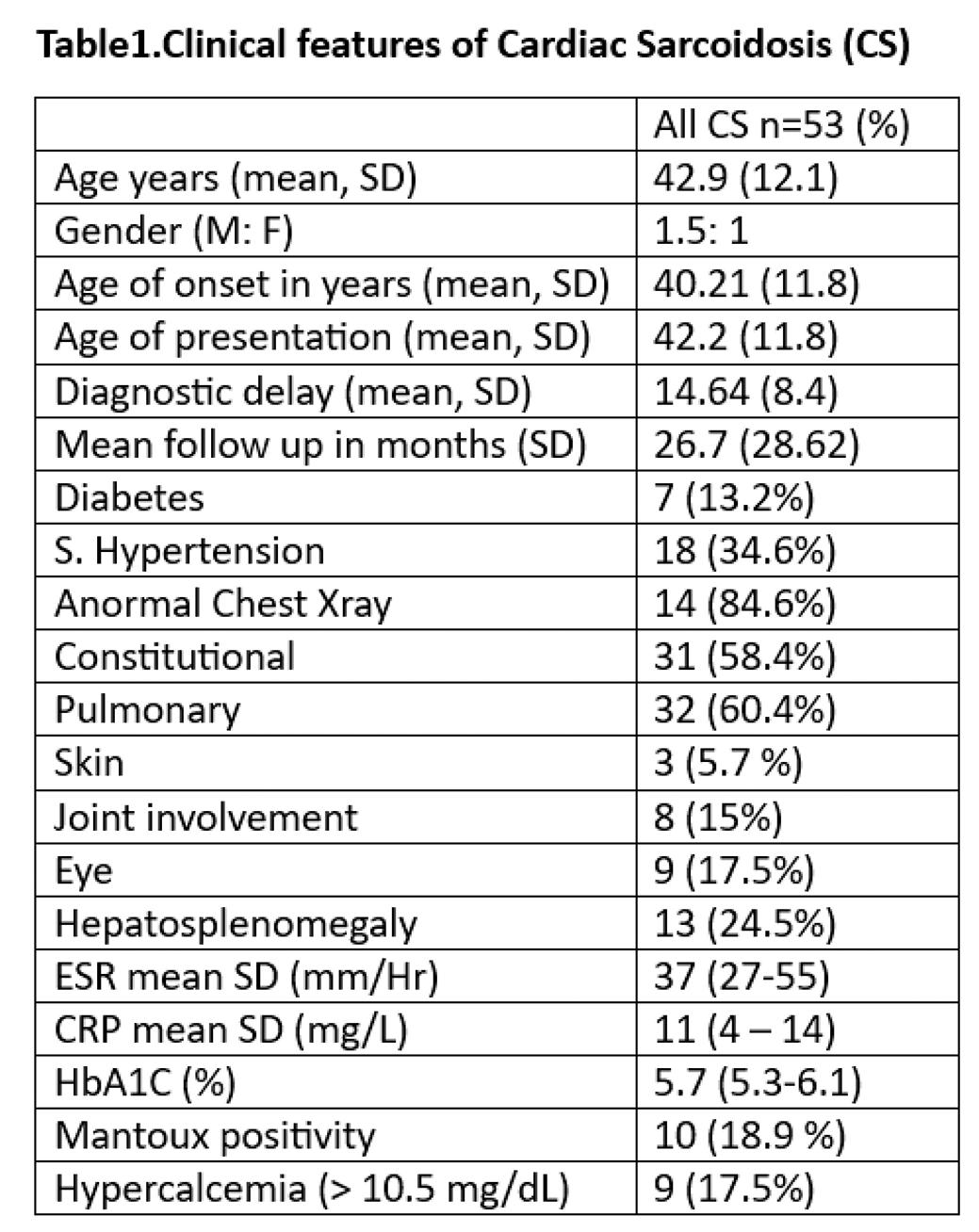
Image and Bar Table 2

POS339
Cyclophosphamide is Associated with Reduced Infections Compared to Other Immunosuppressants in Connective Tissue Disease Related-Interstitial Lung Disease
Mean follow-up under our care was 308.5 ± 235.1 days with 57 instances of serious infection occurring in 36 individuals. There were three infection-related mortalities. Overall, 43 had received mycophenolate, 22 had received monthly pulse cyclophosphamide, 20 rituximab, 9 azathioprine, three tocilizumab, three tofacitinib and two intravenous immunoglobulins. Besides, 32 had received the anti-fibrotic nintedanib. Excluding steroids, 36 patients had received only one, 22 had received two, and 16 patients had received more than two immunosuppressants during the total duration of follow-up. Vaccination for influenza and pneumococcus was up-to-date for 41 (47.7%).
In the survival analysis, cyclophosphamide was associated with infection-free survival [p=0.019, Log-rank test, Figure 1] while mycophenolate [p=0.054] and rituximab [p=0.6] were not. Even in the Cox regression [Figure 2], the Hazard ratio for cyclophosphamide was 0.34 (95%CI:013-0.84, p=0.048) even after controlling for the dosage of steroids at the time of infection [HR 1.11 (95% CI:1.04-1.18)] and other immunosuppressants [HR: not statistically significant].
In the subgroup analysis, infection-free survival for SSc-ILD was also associated with cyclophosphamide use (p=0.012; log-rank). The hazard ratio was 0.2 (95% CI:0.046-0.86) for cyclophosphamide and not significant for other variables in the model (age, mycophenolate, rituximab, vaccination status, pulmonary hypertension or steroid dose at the time of infection).
In the MCTD-ILD subgroup, cyclophosphamide use was not significantly associated with infection-free survival. No other subgroup analyses were done since other subgroups had lower numbers.
Image and Bar Table 1
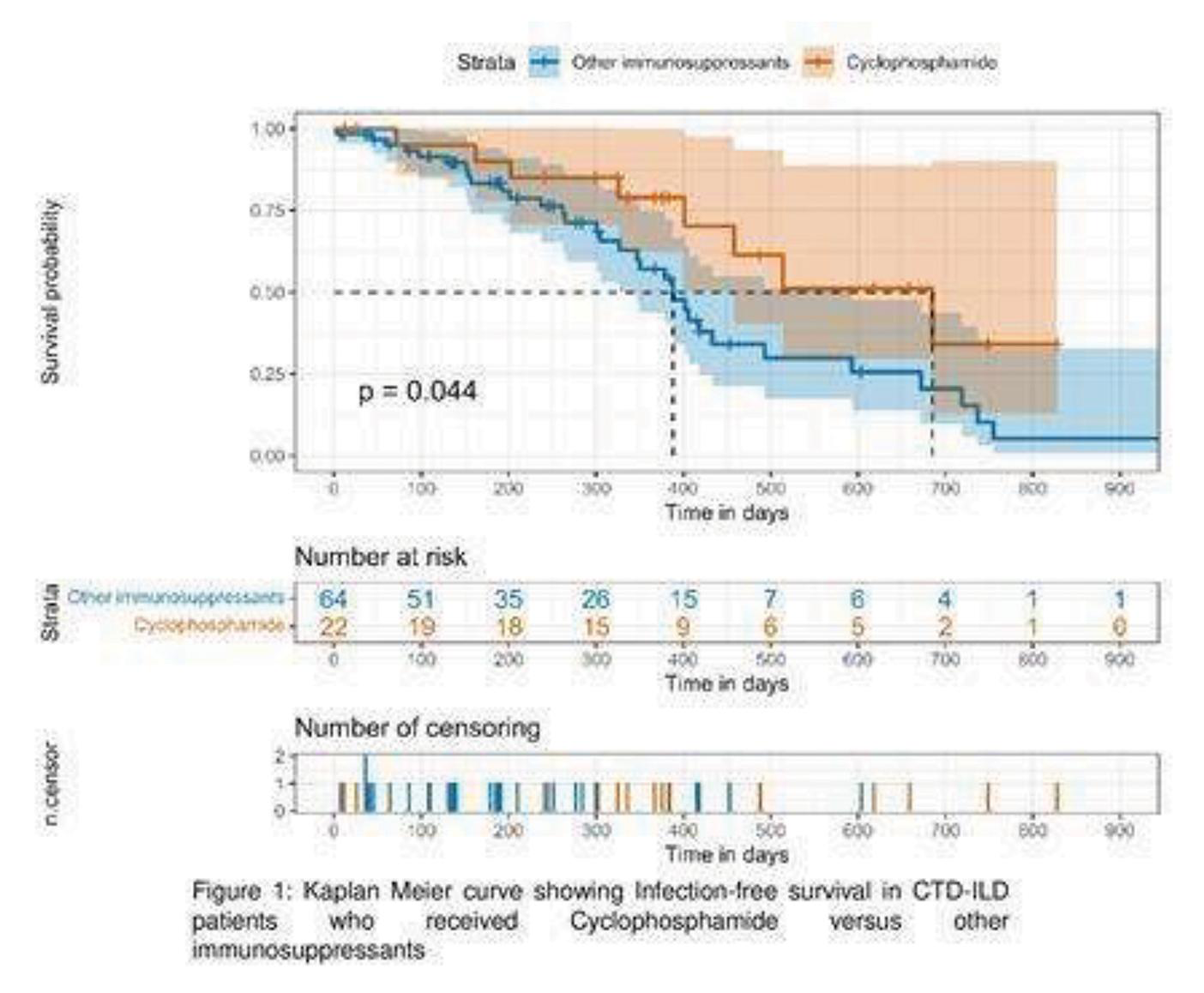
Image and Bar Table 2

POS340
Articular and Periarticular Structure Involvement in Systemic Sclerosis: A Cross Sectional Study
Image and Bar Table 1

Image and Bar Table 2

POS341
Study of Cardiac Autonomic Dysfunction in Systemic Sclerosis: An Observational Study from Northern India
To evaluate the prevalence and severity of cardiac autonomic dysfunction in SSc. To study the correlation of autonomic dysfunction with GI manifestations in SSc.
1. Adler BL, Russell JW, Hummers LK, McMahan ZH. Symptoms of Autonomic Dysfunction in Scleroderma Assessed by the COMPASS-31 Questionnaire. J Rheumatol. 2018 Aug;45 (8):1145–52.
Image and Bar Table 1

Image and Bar Table 2

POS342
Prevalence and Treatment of Palindromic Attacks in Scleroderma Patients: First Report in Literature
1. Schmeiser T et. al. Arthritis in patients with systemic sclerosis. Eur J Intern Med. 2012 Jan;23 (1):e25-9. doi: 10.1016/j.ejim.2011.09.010. Epub 2011 Oct 20
2. Avouac J et al. Articular involvement in systemic sclerosis. Rheumatology (Oxford). 2012;51 (8):1347-1356. doi:10.1093/rheumatology/kes041
POS343
Profile of Anti Nuclear Antibodies and Their Association with Clinical Diagnoses & Manifestations
Female to male ratio was 225:13= 17.30:1
Mean age= 39.53 ± 13.15 years
Median age= 38.5 years
When we looked at the dominant clinical manifestations associated with these antibody groups, top 3 were musculoskeletal, mucocutaneous and hematologic in all groups:
Spliceosome antibodies: Musculoskeletal 66%, Mucocutaneous 69% and Hematologic 44%
Antibodies to nuclear antigens: Musculoskeletal 77-78%, Mucocutaneous 66-86% and Hematologic 73%.
Image and Bar Table 1
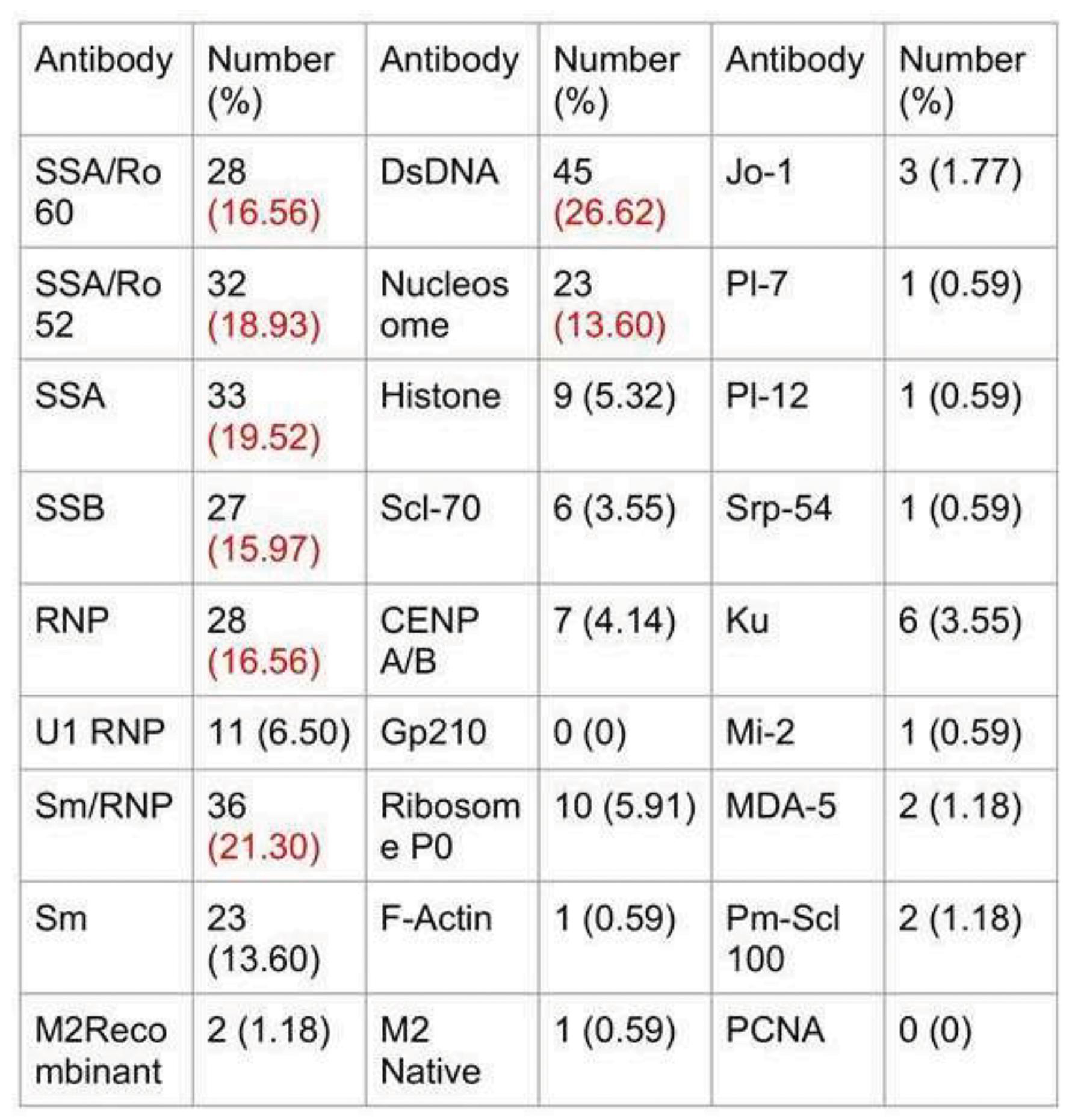
Image and Bar Table 2
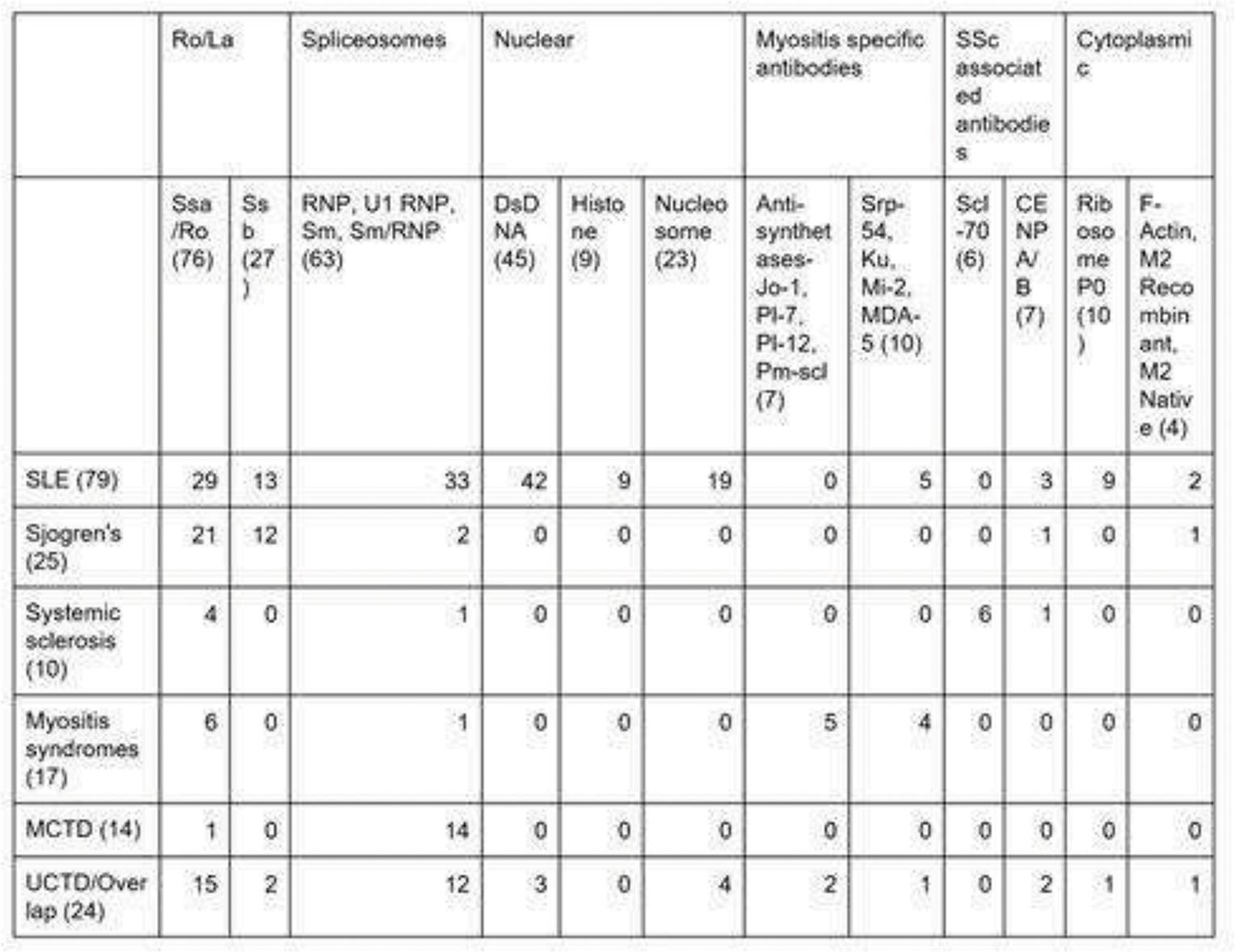
POS344
“Nerve Encounters - Trigeminal Neuralgia in Landscape of Mixed Connective Tissue Disorders”
To determine incidence rate of trigeminal neuralgia among patients with mixed connective tissue disorders. To evaluate clinical characteristics and severity of trigeminal neuralgia symptoms in patients with mixed connective tissue disorders. To explore the relationship between duration and severity of mixed connective tissue disorders and onset of trigeminal neuralgia. To identify potential biomarkers that could predict the development of trigeminal neuralgia in MCTD patients.
From literature, 15 studies (Table 1) were selected from 2013- 2024 based on their relevance and adherence to our inclusion criteria. Statistical analysis was performed using Review Manager (RevMan) software and Stata.
Image and Bar Table 1

Image and Bar Table 2


POS345
Ultrasonographic Study of Salivary Glands in Primary Sjogren’s Syndrome and Correlation with Histopathology and Disease Activity
Its diagnosis is challenging due to its complicated clinical manifestations and non-specific signs. Salivary gland biopsy plays an important role in the diagnosis of SS, especially with anti- SSA and anti-SSB negativity. Salivary gland USG is emerging as a promising non invasive modality in the diagnosis and assessing severity of Sjogrens syndrome.
A few studies have measured SGUS as a diagnostic modality for PSS and correlation with histopathology. There is a lack of data on the use of salivary USG for diagnosis of Primary Sjogrens Syndrome and correlation of disease activity with SGUS and histopathology.
POS346
“Nerve Implications: Peripheral Neuropathy in Autoimmune Connective Tissue Disorders”
The objectives of this study are:
Estimate the Incidence of Peripheral Neuropathy
Characterize Patterns of Peripheral Neuropathy
Assess the Impact of Specific ACTDs
Evaluate Nerve Conduction Studies:
Inform Diagnostic and Management Strategies:
Image and Bar Table 1

POS347
Clinical Phenotype of Isolated Anti-U1 SnRNP Positive Patients in Tertiary Care Center-A Cross-Sectional Observational Study
Image and Bar Table 1

Image and Bar Table 2

POS348
Self-Efficacy Contributes to Better Health Outcomes in Patients of Idiopathic Inflammatory Myopathies: Insights from the COVAD 3 Dataset
Ioannis Parodis has received research funding and/or honoraria from Amgen, AstraZeneca, Aurinia Pharmaceuticals, Elli Lilly and Company, Gilead Sciences, GlaxoSmithKline, Janssen Pharmaceuticals, Novartis and F. Hoffmann-La Roche AG.
The rest of the authors have no conflict of interest relevant to this abstract.
Image and Bar Table 1

Image and Bar Table 2
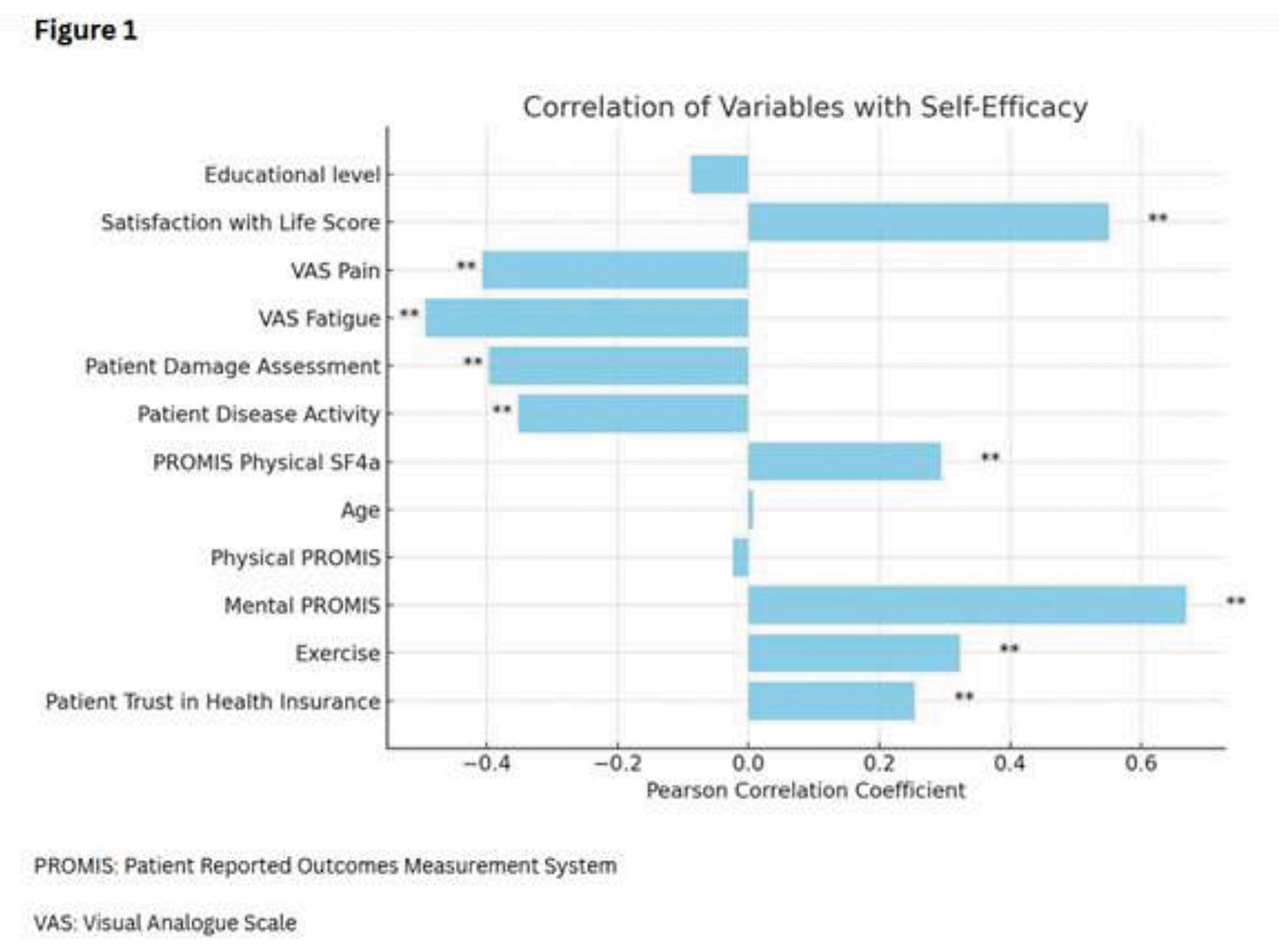
POS349
A Cross-Sectional Comparative Study on “Evolving Role of Lung Ultrasound in Comparisson to HRCT Chest in the Detection of Interstitial Lung Disease (ILD) in Autoimmune Connective Tissue Disorders (AICTDS)”
The artifacts caused by air in the lung can be interpreted meaningfully. More importantly, subpleural pathologies and interstitial pathologies give rise to imaging patterns that give useful insight into the pulmonary pathology. (9, 10) Ultrasound is a cheap, real-time, non-invasive and portable imaging tool without the risk of ionizing radiation and thus becomes an attractive tool for assessment of pulmonary diseases. (9–12) For assessment of ILDs, LUS has largely been studied in connective tissue diseases where it has been proposed that LUS can be used for screening, assessment and monitoring of progression of ILD, especially as a screening tool for the subset of patients suspected to have IPAF (Interstitial pneumonia with autoimmune features). (13–17)
In our study AICTDs included were-
Rheumatoid arthritis Systemic sclerosis Systemic lupus erythematosus Sjogren’s disease Mixed Connective Tissue Diseases Undifferentiated Connective Tissue Diseases Idiopathic inflammatory myositis.
To compare lung ultrasound findings and HRCT chest findings in conjunction with spirometry (FVC).
Image and Bar Table 1

Image and Bar Table 2

POS350
A Comparative Study of Interstitial Pneumonia with Autoimmune Features (IPAF) and Connective Tissue Disease Associated Interstitial Lung Disease (CTD-ILD)
POS351
Clinical Profile of Patients with Systemic Sclerosis Presenting to A Tertiary Care Centre
Image and Bar Table 1

POS352
Real-World Outcomes of Anti-Fibrotics in Scleroderma-Related Interstitial Lung Disease: A Retrospective Study
Gastrointestinal (GI) adverse events were common, with diarrhea reported in 9 patients (64.3%), nausea in 7 patients (50%), and vomiting in 2 patients (14.3%). GI side effects required dose adjustments in 7 patients (50%) and led to drug switches in 6 patients (42.9%).
Image and Bar Table 1

Image and Bar Table 2

POS353
Autoantibody Profiles and Organ Involvement in Scleroderma Patients: A Tertiary Care Center-Based Study
Image and Bar Table 1

POS354
A Prospective Cohort Study of MCTD – A Systemic Autoimmune Disease with Perplexed Individual Identity Amidst Many Faces
Study the clinical and diagnostic profile of MCTD patients. Follow-up for monitoring the disease course and prognosis.
Image and Bar Table 1

POS355
Anti Ro Antibodies and Clinical Associations: An Observational Study
To investigate the spectrum of clinical diagnoses and associations of Anti Ro antibodies in our patients presenting to the OPD. To compare our data with the existing data.
Positive for Anti-Ro52 antibodies only - 13, Positive for Anti-Ro60 antibodies only - 7,
Positive for both Anti-Ro52 and Anti-Ro60 antibodies-22 Not differentiated (Anti-Ro positive) - 10
In 36 patients, other autoantibodies were identified, Anti-SSB/La - 18 patients (22.22%).
Anti-dsDNA - 11 patients (13.58%),
Anti-Histone - 3 patients (3.70%),
Anti-U1RNP - 9 patients (11.11%)
Anti-Sm - 8 patients (9.88%)
Anti-Scl70 - 3 patients (3.70%)
Anti-PmScl - 2 patients (2.47%)
Rheumatoid Factor - 3 patients (3.70%)
Anti-CCP - 2 patients (2.47%)
In 16 patients (19.75%), no other antibodies were identified.
Image and Bar Table 1

Image and Bar Table 2

POS356
Safety of Cyclophosphamide in Autoimmune Disease with Respect to Infections: A Single-Centre Retrospective Observational Study
Baseline demographics, laboratory data, treatment details, vaccination status, and antibiotic prophylaxis were documented. Cumulative doses of prednisolone were calculated to assess glucocorticoid exposure.
Five infections were serious, requiring intravenous antibiotics and hospitalization. The median time to infection was 3.5 months.
No significant increase in infection risk was noted across age groups, gender, disease activity scores, vaccination status, various hematological parameters.
Patients on cotrimoxazole prophylaxis had a significantly lower infection risk compared to those not on prophylaxis (p=0.005).
Lower doses of corticosteroids were linked to reduced infection risk (p=0.025).
A cutoff cumulative steroid dose of <6.76g predicted lower infection risk with a sensitivity of 72.7% and specificity of 61.5%.
Infection-free survival was similar across SLE, vasculitis, and myositis patients.
Image and Bar Table 1

Image and Bar Table 2

POS357
Prevalence of Hand Dysfunction in Patients with Systemic Sclerosis: A Questionnaire Based Cross Sectional Study
Primary Objective: To document the burden of hand dysfunction in SSc patients using Cochin Hand Function Scale. Secondary Objective: To correlate the degree of hand dysfunction with clinical domains and overall functionality of individuals using the Indian Health Assessment Questionnaire (HAQ).
Table 1
Demographic data showed majority of individuals being female and from middle economic status. The duration of illness had a bimodal pattern with individuals having illness for either less than 5 yrs or more than 10 yrs. Most individuals had a diffuse pattern of illness. Correlation of hand function with clinical domains and overall functionality.
Table 2
Mean CHFS in the study is 21.29 which represents the burden of hand dysfunction in patients with SSc. MRSS score was correlating with CHFS score with a p value of 0.019 CHFS was correlating with HAQ-DI with a p value of 0.000
The degree of hand dysfunction represented by CHFS was positively correlating with HAQ.
Hence this study is aimed at identifying the prevalence of hand manifestations and its impact on quality of life in patients living in India.
1. Bairwa D, Kavadichanda CG, Adarsh MB, Gopal A, Negi VS. Cultural adaptation, translation and validation of Cochin Hand Function Scale and evaluation of hand dysfunction in systemic sclerosis. Clinical Rheumatology. 2021 May;40:1913-22
2. Ouimet jm, pope je, gutmanis i, koval j: work disability in scleroderma is greater than in rheumatoid arthritis and is predicted by high haq scores. Open rheumatol j 2008; 2: 44-52.
Image and Bar Table 1
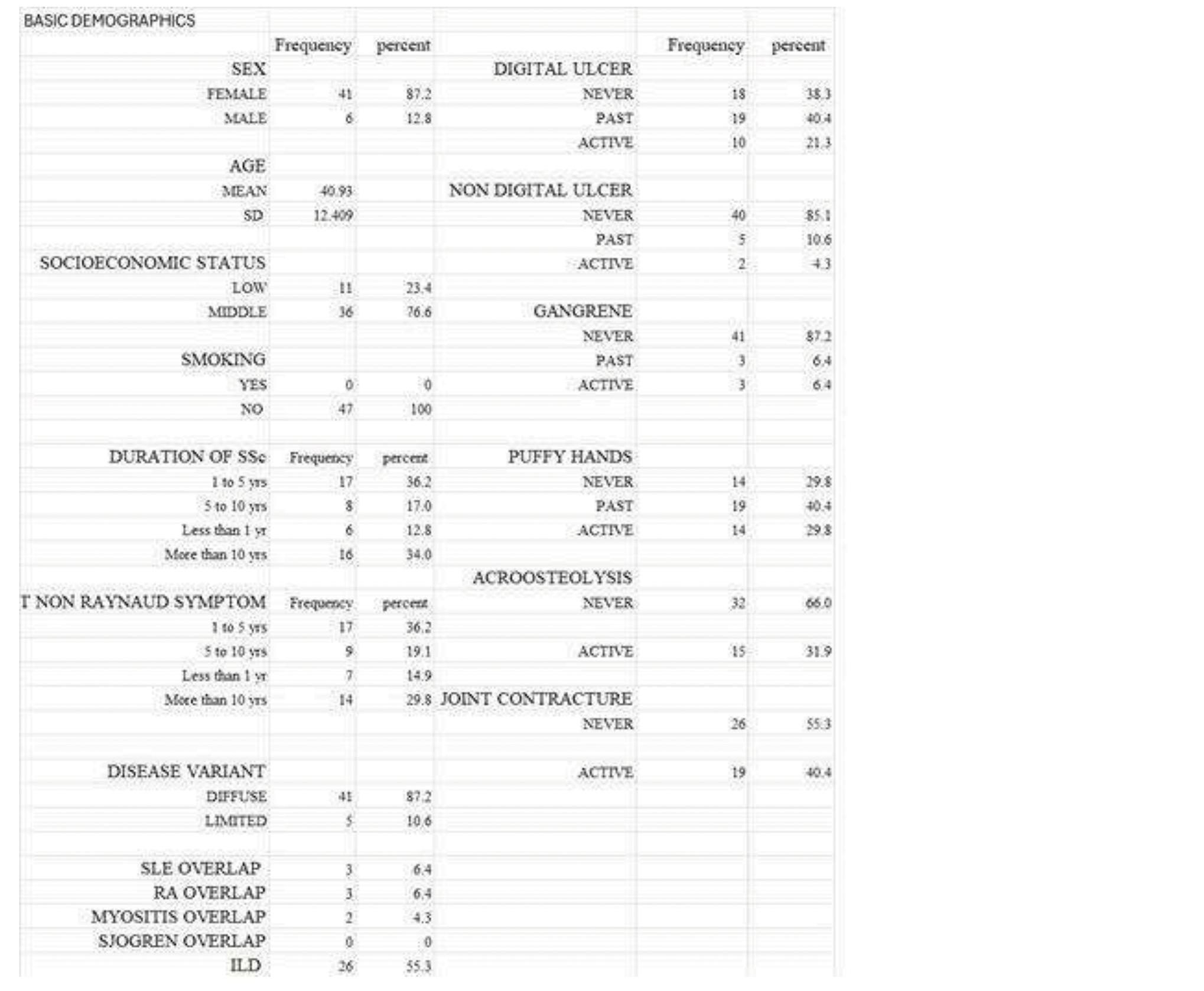
Image and Bar Table 2
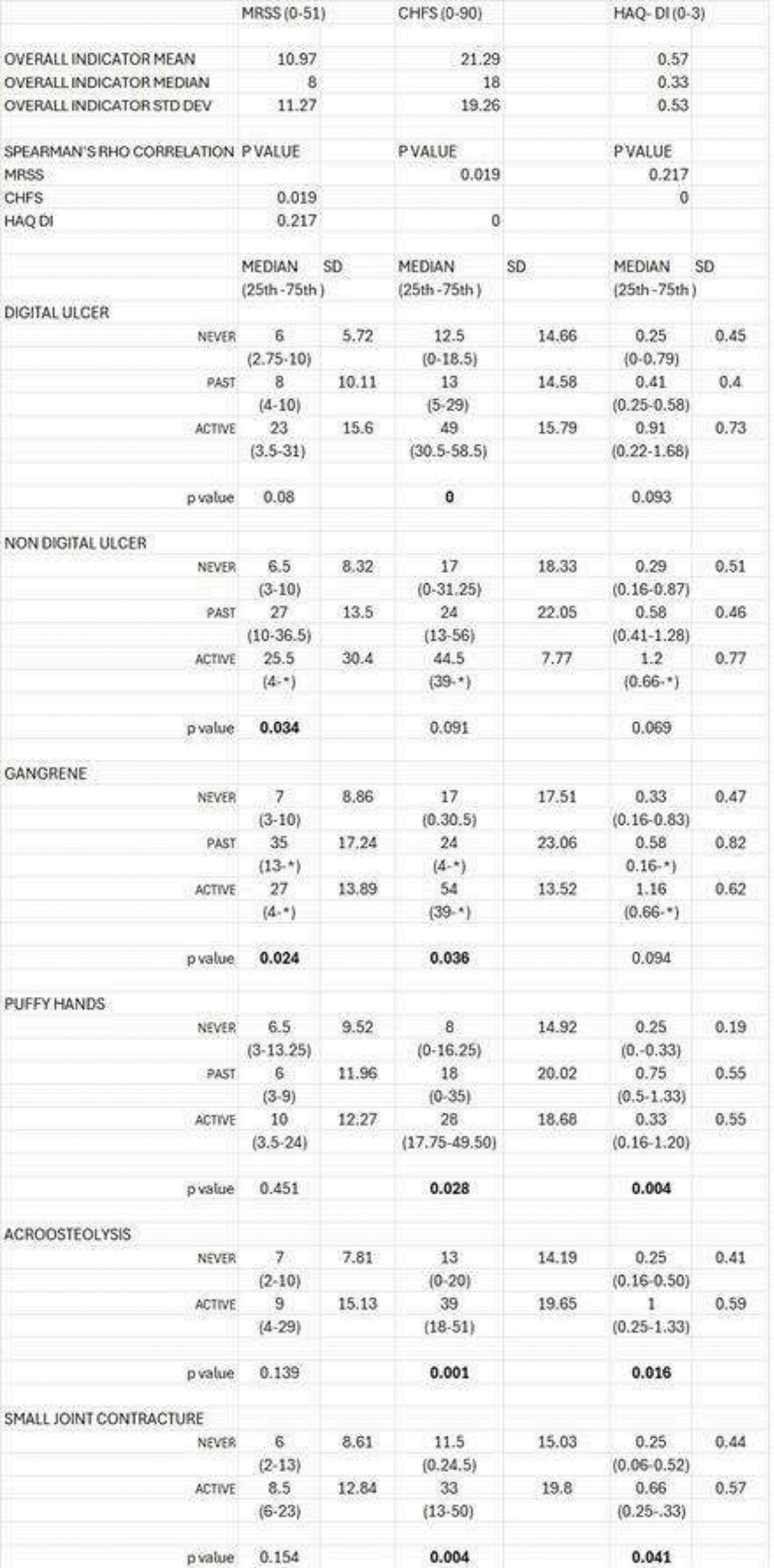
POS358
Determinants of Persistent Disease in Systemic Sclerosis: Report of Ten Year Follow-Up from A Single Centre Cohort
Define disease & treatment-related risk factors for activity on long-term follow-up.
We found a significant correlation between the time to start immunosuppression from RP and non-RP symptoms and active status after a decade (Table 2).
Image and Bar Table 1
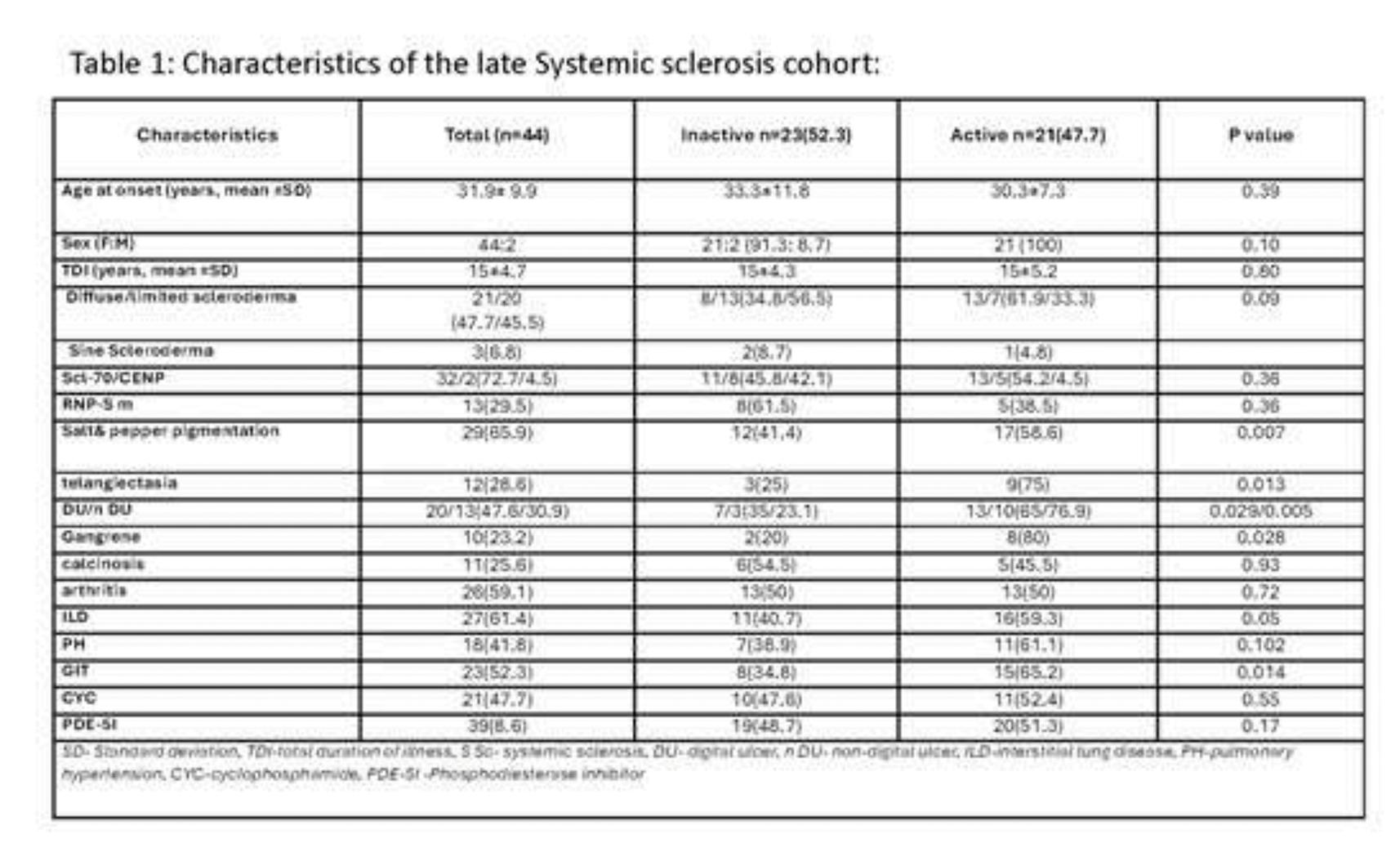
Image and Bar Table 2

POS359
Assessment and Treatment Patterns in Systemic Sclerosis: Insights from a Survey of Indian Rheumatologist
To identify differences in management trends between practice settings.
In assessment patterns, performance of mRSS was significantly more among trainees and teaching hospitals (Table 2). Chest imaging for ILD detection was significantly higher among practitioners; with higher documentation of 6MWT at baseline among teaching centers. Evaluation of PH did not significantly differ; NFC was performed significantly more in teaching centres and by trainees.
Use of prednisolone did not significantly differ across settings. Maximum use was for myositis (n=206, 68%) and arthritis (n=199, 65.7%) at a dose of <10 mg (n=192, 63.4%) for < 3 months (n=155, 51.2%). Use of Immunosuppression for early skin disease was significantly more among practitioners. Preferred immunosuppression for SSc-ILD was Mycophenolate (n=212, 97%).
Image and Bar Table 1
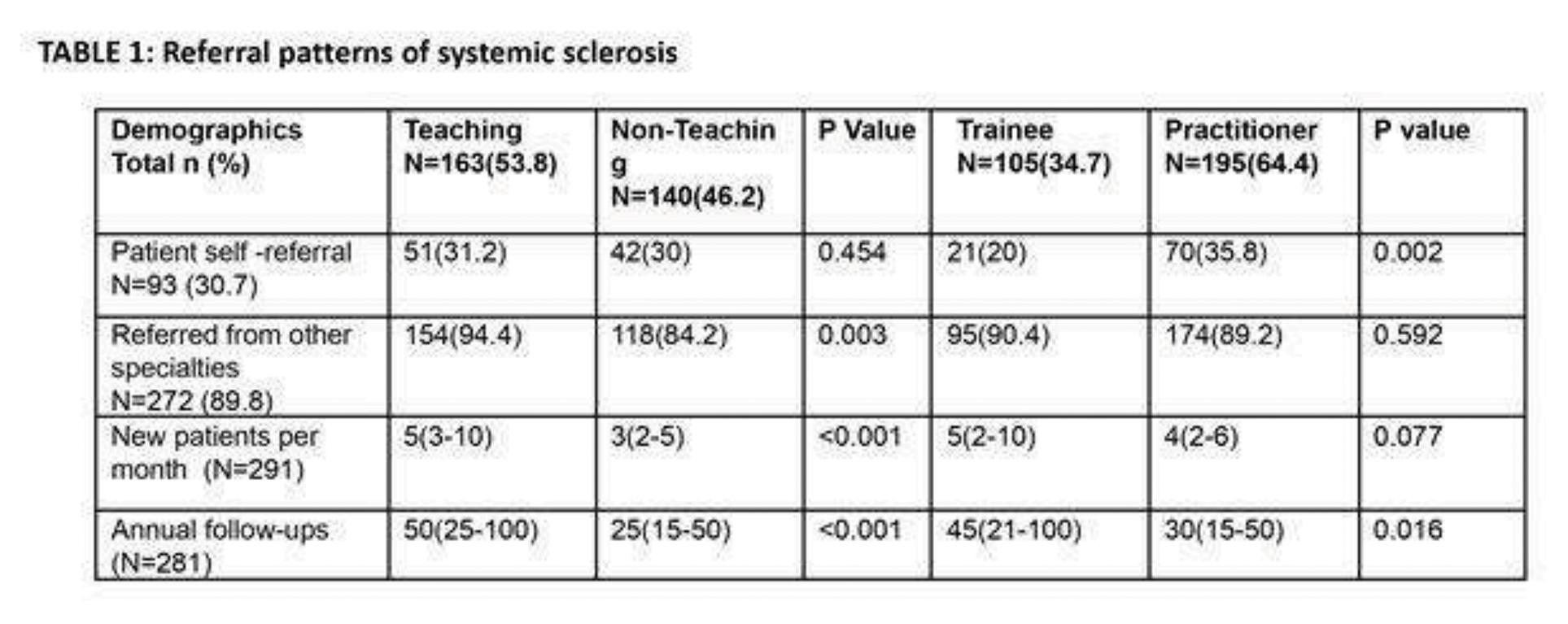
Image and Bar Table 2

POS360
Ultrasonography of the Salivary Glands as An Investigation Tool in the Diagnosis of Sjögren’s Syndrome
Image and Bar Table 1

Image and Bar Table 2

POS361
Nailfold Capillaroscopic Findings Using USB Digital Microscope - An Inexpensive Way to See the Capillaries
1. Etehad Tavakol M, Fatemi A, Karbalaie A, Emrani Z, Erlandsson BE. Nailfold Capillaroscopy in Rheumatic Diseases: Which Parameters Should Be Evaluated? Biomed Res Int. 2015;2015:974530. doi: 10.1155/2015/974530
Image and Bar Table 1

POS362
Predictors of Mortality in Systemic Sclerosis: A Single Centre Study from India
Sundaram T.G.1, Sakir Ahmed2, Vishwesh Agarwal3,
Image and Bar Table 1

Image and Bar Table 2

POS363
Prevalence of Oral Manifestations in Systemic Sclerosis Patients and Their Association with Clinical and Serological Profile - A Case Control Study
Image and Bar Table 1

Image and Bar Table 2

POS364
PRES Revealing Takayasu Arteritis- A Case Series
1. Camara-Lemarroy CR, Lara-Campos JG, Perez-Contreras E, Rodríguez-Gutiérrez R, Galarza-Delgado DÁ. Takayasu’s arteritis and posterior reversible encephalopathy syndrome: a case-based review. Clinical rheumatology. 2013 Mar;32:409-15.
2. Ni J, Zhou LX, Hao HL, Liu Q, Yao M, Li ML, Peng B, Cui LY. The clinical and radiological spectrum of posterior reversible encephalopathy syndrome: a retrospective series of 24 patients. Journal of Neuroimaging. 2011 Jul;21 (3):219-24.
Image and Bar Table 1

POS365
Small Airway Dysfunction in Patients with Scleroderma Spectrum Disorder
To assess the utility of respiratory oscillometry in scleroderma spectrum disorder when compared to spirometry.
Respiratory oscillometry might be useful in scleroderma spectrum disorders especially when conventional means like spirometry is difficult to perform.
POS366
Autonomic Dysfunction in Fibromyalagia Patients
Fibromyalgia (FM) is a chronic widespread pain syndrome characterized by persistent pain, fatigue, sleep disturbances. FM disrupts the major stress response system, which includes the HPA-axis and the autonomic nervous system (ANS). ANS dysfunction may play a role in the pathogenesis of fibromyalgia but it is not clear if this is a cause or effect.
Patients with a H/o of CAD, Malignancy, h/o of smoking, alcoholism and drug which interfere with results were excluded. A healthy Age and sex matched controls were selected based on same exclusion criteria
Non-invasive autonomic function tests were performed by CAN Win Analysis System. Heart Rate variability (HRV) by AD instruments. The HRV Time domain parameters, SDRR (standard deviation of RR intervals), SDSD (SDSD standard deviation of successive RR intervals), RMSDD (Root mean of squared successive RR Intervals), SDRR/RMSD Ratio. HRV frequency domain parameters LF/HF were measured. Hand grip strength (by Hand Held Dynamometer) and FIQ-R scores were recorded.
Baseline demographics and clinical characteristics.

Autonomic function parameters.

All Data are presented as median with interquartile range
POS367
Nightmare Coming True- Triple Whammy in A Case of Primary Sjogren Syndrome
We present the case of 26-years lady, usually fit and healthy, who presented with drowsiness, disorientation and severe bicytopaenia (anaemia, thrombocytopaenia). Previously she had 3days of low-grade fever with dry cough that had resolved with medications around 7 days before, following which she was well. This was followed by multiple episodes of convulsions and unresponsiveness for which she had been admitted at another centre and managed as meningoencephalitis with antibiotics and antiepileptics. There her CSF study had 14 cells (70% lymphocytes), raised protein and normal sugar. She was subsequently shifted to our centre.
No history found of rash/joint pain/trauma/bleed.
Here, her vitals were stable, with low-grade fever (990F), persisting disorientation and irritability without frank seizures, severe pallor and mild splenomegaly. Baseline investigations- severe normocytic-normochromic anaemia with polychromasia, severe thrombocytopaenia, raised CRP/ESR (negative PCT) and transaminases. Common tropical infections came negative. Further workup showed ANA 4+, Anti Ro-52, Anti-Ro, Anti-La positive, DAT positive with IgG+, normal C3 and C4; ferritin, D-Dimer, LDH- elevated; and negative for hepatitis C, cryoglobulin, dsDNA, ANCA, ACPA and Rheumatoid factor. Repeat peripheral smear had schistocytes, ADAMTS13 levels very low. Bone marrow suggested peripheral platelet destruction, PET-CT and MRI brain non-contributory. With findings indicating Thrombotic Thrombocytopaenic Purpura (TTP) /warm Autoimmune Haemolytic
Anaemia (AIHA) coexistence and likely primary Sjogren syndrome (SS) in first presentation, pulse-dose methylprednisolone for 3 days followed by maintenance steroids, intravenous immunoglobulin 2mg/kg body weight over 5 days, and plasmapheresis were done. Other symptomatic treatment including anticonvulsants and broad-spectrum antibiotics were given.
The patient responded well with reversal of cytopaenia, improved sensorium and was discharged in a stable condition with plans for further evaluation and follow-up.
SS is a chronic autoimmune disorder with primarily mononuclear cell infiltration of exocrine glands. The extraglandular spectrum rarely includes haematological alterations especially coexisting severe anaemia and thrombocytopaenia. SS with coexisting TTP and AIHA is extremely rare with only handful reports in literature. Neurological symptoms are variable and may precede the onset of sicca symptoms. Aggressive therapy, long term follow-up and low threshold for diagnosis is imperative.
Image and Bar Table 1

POS368
Diagnostic Value of Salivary Gland Ultrasound in Seronegative Primary Sjögren’s Syndrome
Image and Bar Table 1

Image and Bar Table 2

POS369
Clinical Characteristics of Localized Morphia: A Retrospective Study
Assess demographic distribution, including gender and age. Analyze clinical presentations and laboratory parameters. To enumerate treatment modality and evaluate long term outcome.
Skin changes were a presenting feature in all cases. Comorbidities were identified in 21.7% of cases. 47.8% of patients tested positive for ANA, 8.7% for Centromere, and 17.4 % for SCL70 antibodies. The mean ESR of the patients was 17.4 ±11.3 mm/hr. Elevated ESR (>20 mm/hr) was observed in 39.1% of patients. Treatment with DMRD like Methotrexate (57.9%) and Tacrolimus (42.1%), MMF (30.43%) and steroids (43.5%).
POS370
Biosimilar Denosumab in Osteoporotic Patients Attending A Tertiary Care Hospital of Eastern India – A Real-World Comparative Retrospective Observational Study
The mean LS-TS values for innovator and biosimilar groups at baseline were -3.85±0.20 and -3.82±0.21 respectively while the mean HIP-TS values for innovator and biosimilar group at baseline were -3.60±0.22 and -3.57±0.21 respectively. Both the groups were comparable at baseline and there was no significant difference between the two groups in terms of T score at both sites. After 2 years of denosumab treatment, mean LS-TS values for innovator and biosimilar groups reached to -2.82±0.26 and -2.74±0.25 respectively while the mean HIP-TS values for innovator and biosimilar group were recorded to be -2.41±0.27 and -2.40±0.24 respectively. When post treatment T scores were compared, there was no significant difference between the two groups at any of the sites [Table-1].
When intra-group change in T scores from baseline over 2 years were evaluated, both innovator and biosimilar denosumab groups were observed to have significant improvement (p<0.0001) in mean LS-TS as well as HIP-TS values. [Figure-1] No severe adverse effects were noted in any group and the safety profile of both the groups was comparable.
Image and Bar Table 1

Image and Bar Table 2

POS371
Clinical Profile and Outcomes of Antisynthetase Syndrome Patients: A Tertiary Centre Experience
1. Witt LJ, Curran JJ, Strek ME. The Diagnosis and Treatment of Antisynthetase Syndrome. Clin Pulm Med. 2016 Sep;23 (5):218-226.
2. Sreevilasan SK, Devarasetti P, Narahari NK, Desai A, Rajasekhar L. Clinical profile and treatment outcomes in antisynthetase syndrome: a tertiary centre experience. Rheumatol Adv Pract. 2021 Nov 5;5 (Suppl 2):ii10-ii18.
POS372
Clinico-Immunological Profile and Treatment Outcomes of Clinically Significant Diaphragmatic Weakness in Patients with Idiopathic Inflammatory Myopathies: Results from The Largest Single-Center Cohort of 16 Cases
Image and Bar Table 1

Image and Bar Table 2
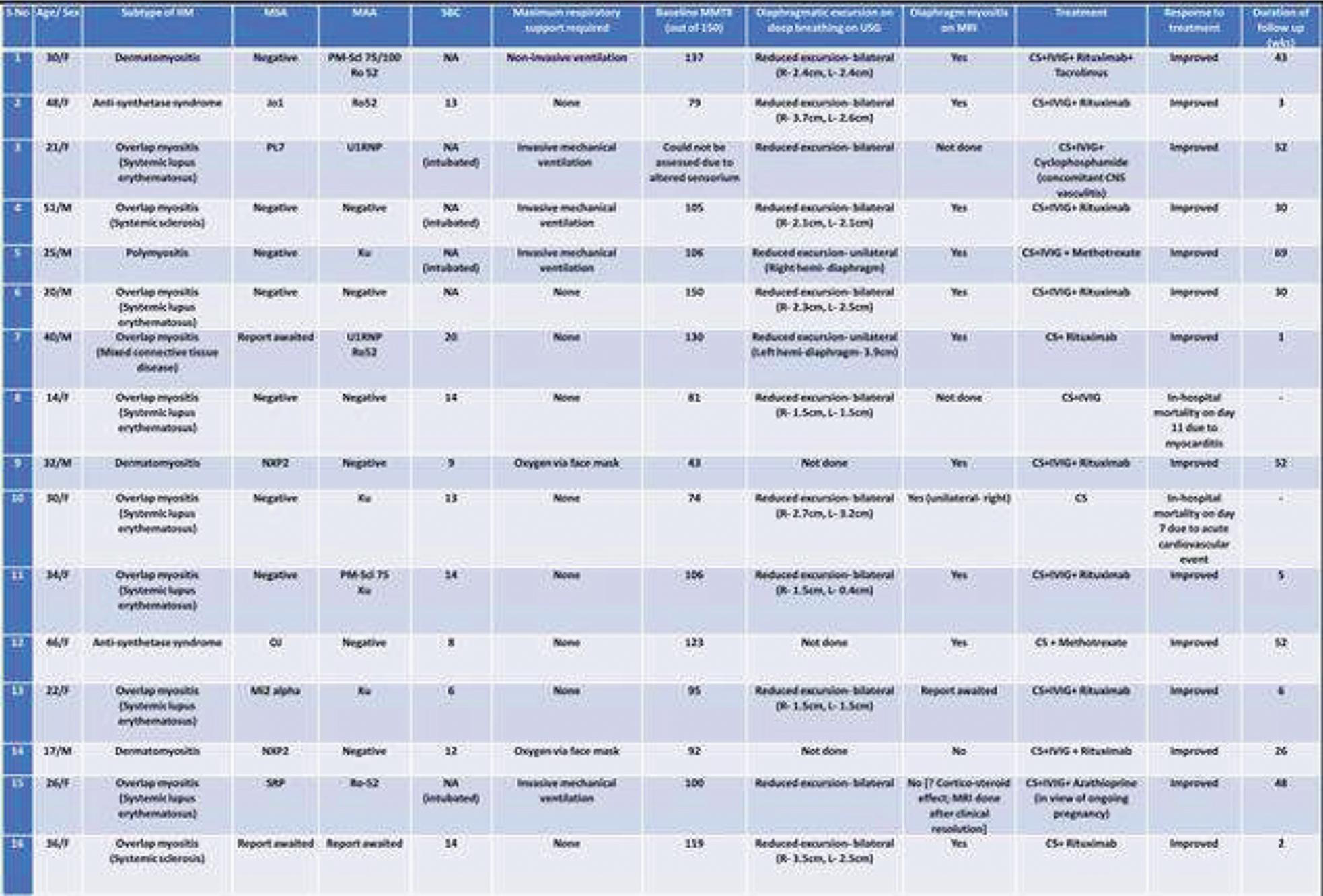
POS373
Myositis-Specific Antibodies (MSAs): Characteristics and Six-Month Follow-Up Outcomes of a Single-Centre Cohort of MSA-Positive Connective Tissue Disease
The most common MSAs in our population was anti-Mi-2 (n=6), at 33.3%. The commonest diagnosis was Dermatomyositis (27.8%), and 50% had the presence of ILD (NSIP being the most common radiologic pattern). Table 1 describes the disease characteristics. Two of the MSA-positive patients passed away: one due to aspiration pneumonia after 3 months of rituximab (RTX) induction (Mi-2 +), and another lady (PL 12, Ro52+) with Anti-synthetase Syndrome, due to renal failure and cardiac arrest. Both the patients had ILD.
Figure 1 depicts the changes in median serum CPK levels, MMT8 scores, physician global, patient global and extramuscular global VAS scores at baseline and 6 months. While 80% of the Jo-1+ patients had ILD, one patient also had Anti-TIF 1γ, Anti-CCP and Anti-PmScl 100 antibodies, and was diagnosed with colon carcinoma. Mi-2+ patients had the highest baseline CPK levels, and rash was the most common extramuscular symptom. Cyclophosphamide and RTX had been used for induction therapy in 6 (33.3%) and 4 (22.2%) patients, respectively. Jo-1 positivity had a significant correlation with the presence of ILD.
Image and Bar Table 1

Image and Bar Table 2

POS374
Efficacy of IVIG in Idiopathic Inflammatory Myopathy: A Comparative Analysis with Non-IVIG Therapy
Evaluate the efficacy of IVIG in IIM patients - Total Improvement Score (TIS) at 3 months. Analyze the clinical course of patients receiving continued monthly IVIG. Compare the outcomes- TIS and Manual Muscle Testing-8 (MMT-8) - single IVIG dose versus continued monthly IVIG. Compare outcomes in patients treated with IVIG versus a control group - 3 month follow up. Study the safety profile of IVIG.
Single-center, ambispective study - Nizam’s Institute of Medical Sciences, Hyderabad. Patients with new or refractory IIM s-Bohan and Peter criteria
IVIG Group: Single cycle or continued monthly IVIG. Control Group: Patients with similar baseline MMT-8 scores, bulbar weakness, and CPK levels but who did not receive IVIG. Primary Outcome: TIS at 3 months, categorized as minimal, moderate, or major clinical responses - ACR/EULAR 2016 criteria. Secondary Outcomes: MMT-8 scores, CPK levels, and adverse events.
After homogenization - 14 patients in the IVIg group and 12 patients in the control group were compared for the outcomes.10 of the 12 patients in control group had received Rituximab at baseline. Significant improvement in MMT-8 and CPK at 3 months in both IVIG and control groups, no difference amongst groups. Minor infusion reactions (fever) in 3 patients; 1 patient -thrombocytopenia in IVIg group.
Image and Bar Table 1

Image and Bar Table 2

POS375
Clinical Profile and Outcomes in Antisynthetase Syndrome- A Single Centre Eperience
To study the pattern of clinical presentation of patients with Asys. To assess the survival and response outcomes of ASyS patients; identify any potential determinants of response.
Jo-1 vs. non-Jo-1
Jo1 with Ro52 vs Jo1 without Ro52
Outcomes were categorized as follows:
Complete Response (CR): Absence of clinical symptoms/signs or an increase in forced vital capacity (FVC) by ≥10% in the ILD domain; functional class 1, improvement in MMT8, and normal muscle enzyme levels in the myositis domain. Partial Response (PR): Improvement in any domain that did not meet the criteria for CR. Disease Worsening: Worsening clinical parameters or a decline in FVC by >10%.
Complete Response: 30 patients, Partial Response: 13 patients, Disease Worsening: 4 patients, Long-Term Oxygen Use: 2 patients
Logistic regression revealed no significant impact of clinical presentation or antibodies on response. The p-value for PL-7/12 positivity was 0.05, suggesting a potential association with response but not statistically significant.
Survival: Out of 75 patients, 65 were survivors and 10 Non survivors. Kaplan-Meier survival analysis did not reveal any significant impact of clinical domains (arthritis, myositis, ILD, mechanic’s hand, constitutional) on survival. However, the PL-7/12 subgroup had numerically higher mortality.
Image and Bar Table 1

Image and Bar Table 2

POS376
“A Clinico- Serological Correlation of Idiopathic Inflammatory Myopathies with Interstitial Lung Disease: Insights from A Single Center Cross-Sectional Study”
The clinical findings of statistical significance present in the IIM-ILD group were Mechanic’s Hands (p=0.0002), Raynaud phenomena (p=0.0004) and arthritis (p=0.0113). The mean CPK levels in IIM-ILD group were 3400, and 8187 in the latter.
Image and Bar Table 1

POS377
Clinical Characteristics and Outcome of Anti Sae Myositis – Data From A Tertiary Centre in South India
Skin manifestations were the most prevalent clinical feature at disease onset, found in 13 (68%) patients. Neck muscle weakness was found in in 3 (15%) patients.
Most common ILD pattern was non-specific interstitial pattern in 3 (30%) patients.
9 patients were treated with mycophenolate mofetil and 6 patients with methotrexate as second line agents. 15 patients had clinical response.
There was one patient with hypomyopathic dermatomyositis. Amyopathic dermatomyositis was seen in 5 (26%) patients and tend to present late.
Cutaneous ulcers were significantly associated with anti SAE myositis as compared to other myositis subtypes (p=0.000).
Out of the 19 patients, 2 (10%) patients had expired in out cohort. One patient had presented with severe muscle weakness with dysphagia, aspiration pneumonia and global left ventricular dysfunction and had expired within 3 days of hospital stay. Another patient with severe muscle weakness (MMT80 SCORE 22/80) and organising pneumonia had been discharged with methotrexate and 1mg/kg steroid, but 2 weeks post discharge he succumbed to sudden cardiac arrest.
Image and Bar Table 1
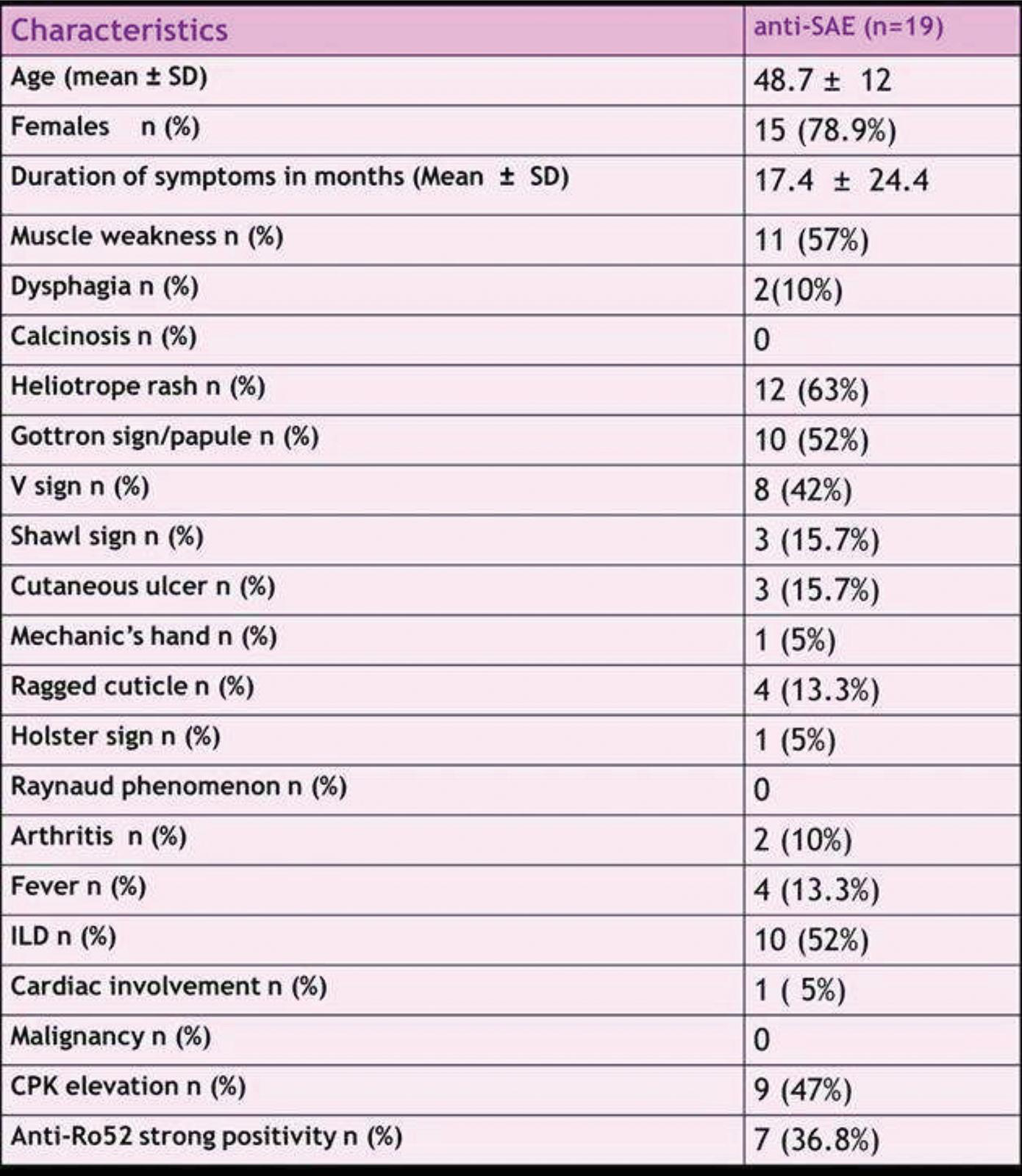
POS378
Implications of Anti-Ro52 Antibodies on Clinical Phenotype of Adult Idiopathic Inflammatory Myositis (IIM): A Cross-Sectional Study
To assess the influence of anti-Ro52 antibody on the clinical phenotype in a cohort of adult IIM patients. To assess association of Anti-Ro52 antibodies with (i) ILD, (ii) MMT-8 and muscle enzyme elevation (CPK and LDH) in the presence of other myositis-specific-autoantibodies (MSA) - Mi-2, PL-7, MDA-5, and Jo-1.
In the subgroup analysis, Mi-2+Ro52+ patients had a significantly higher ILD prevalence (50% vs 6.8%, p < 0.001). Similar increased prevalence of ILD was noted in the Jo1+Ro52+ group (72.5% vs 47.8%, p=0.050). However, Ro52 negative patients displayed higher CPK and LDH levels, indicating more severe muscle involvement, particularly in the Mi-2 and PL-7 subgroups (Table 5).
Anti-Ro52 antibodies are associated with an increased risk of ILD, especially in Mi2 positive and Jo-1 positive patients. Serological stratification based on anti-Ro52 status could be useful in personalizing treatment strategies and predicting disease prognosis in IIM patients.
Image and Bar Table 1
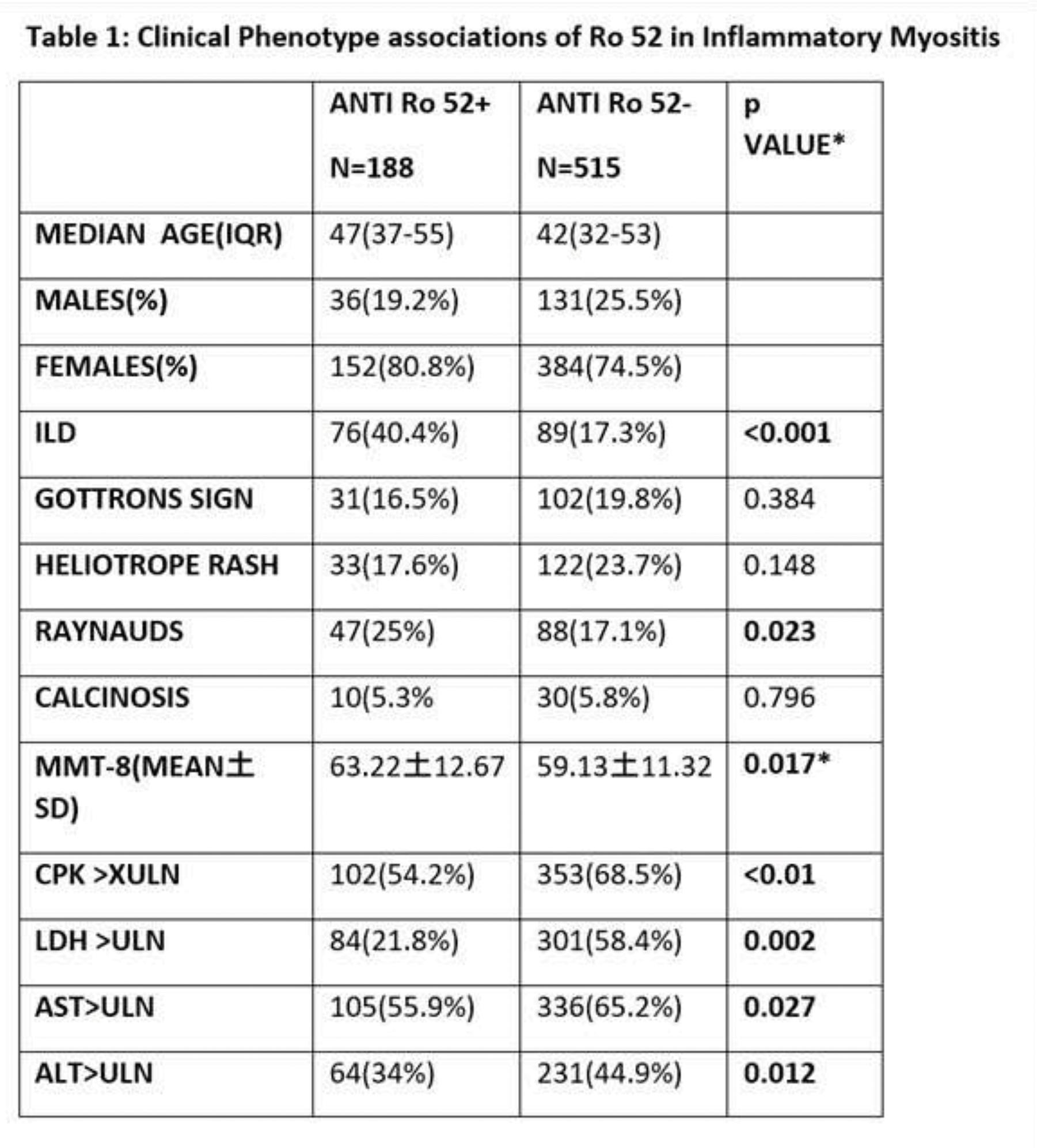
Image and Bar Table 2

POS379
Clinical, Serological, and Histological Profiles, Along with Outcomes, of Patients Attending the Myositis Clinic in a Tertiary Center in South India: An Ambispective Study
Muscle biopsy performed on 36 patients revealed distinct features, including perifascicular atrophy, fiber necrosis, size variation, and regeneration in both ASS and DM patients. Vacuolization was observed in 1 ASS patient (2.8%), perivascular inflammation in 2 DM patients (5.6%), while phagocytosis and perifascicular necrosis were exclusive to DM, highlighting key histopathological differences.
Among patients presenting with muscle weakness, 20% showed moderate improvement, 20% major improvement, and 30% minor improvement after 6 months of treatment. Proximal muscle weakness (48.82%) was the most common symptom, and Mi-2a was the most frequently detected antibody. IMACS core set measures, including MMT8 and CPK, demonstrated significant improvement over 6 months.
Image and Bar Table 1

Image and Bar Table 2

POS380
Idiopathic Inflammatory Myopathy: A Clinic-Serological Correlation
POS381
Study of Prevalence, Progression and Response to Therapy in Connective Tissue Diseases Related Pulmonary Artery Hypertension
To study the prevalence of PAH in SLE and CTDs. To study the relationship between the disease activity of CTD with the severity of PAH. Response to various immunosuppressive therapies in CTD associated PAH.
There was no correlation between disease activity and occurrence of PAH in the present study. There was statistically significant difference on improvement in PAH variables by immunosuppression with Cyclophosphamide. 6 patients with asymptomatic PAH were identified.
Image and Bar Table 1
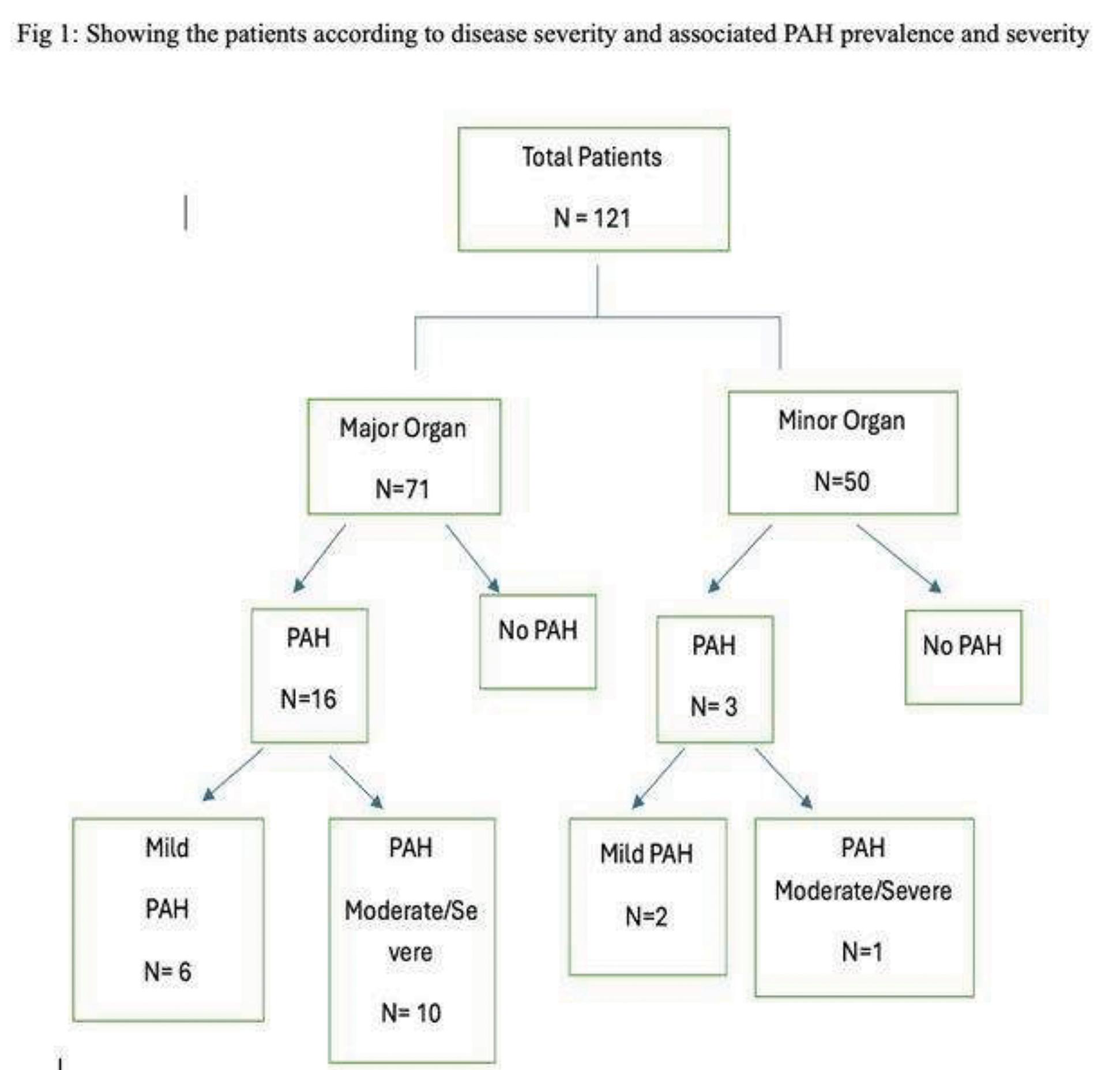
Image and Bar Table 2
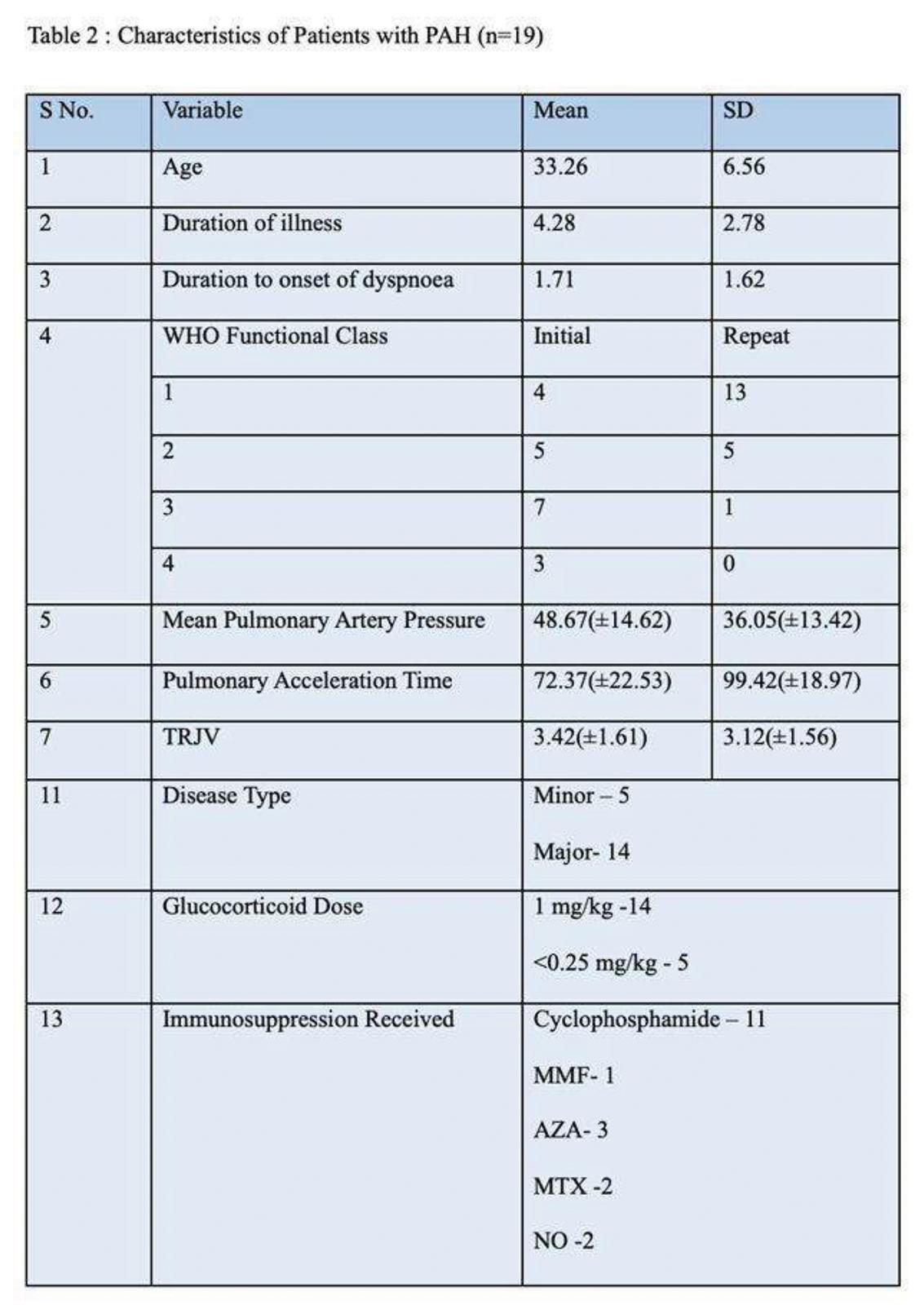
POS382
Peripheral Ulcerative Keratitis in Rheumatology Clinic
POS383
Evaluating Infection Incidence in Tofacitinib Therapy: A Cross-Sectional Study
POS384
Effectiveness, Tolerability, and Safety of Tofacitinib in Autoimmune Rheumatic diseases: A Cross Sectional Study from A Tertiary Care Centre
Image and Bar Table 1

POS385
Correlation of Serum KL6 with Pulmonary Function Tests in the Monitoring of Connective Tissue Disease Associated Interstitial Lung Disease: A Prospective Cohort Study
Image and Bar Table 1

Image and Bar Table 2

POS386
Methotrexate Induced Pancytopenia: Single Center Case Series of 33 Cases
POS387
Predictors of Mortality in A Prospective Cohort of Adult Patients with Idiopathic Inflammatory Myopathy (IIM)
During a median follow up of 9.5 months (4-22), there were 11 deaths (16.2%). The causes of death were: cardiovascular complications-5 (4 sudden cardiac deaths, 1 refractory ventricular tachycardia), pneumonia-3 (2 COVID, 1 MDR Pseudomonas), RP-ILD-2 and respiratory muscle weakness- 1 patient. The 1-year survival rate of the cohort was 80.9 %. Among the 11 deaths, 7 died within 1 year of disease onset (63.6%). On univariate analysis, older age, infections and RP-ILD were associated with mortality (Table 1). On multivariate analysis, only RP-ILD [Odds Ratio- 7.5 (95% CI, 1.04-54.4), p=0.04] was identified as the significant predictor of mortality.
Cardiovascular risk assessment and management is of paramount importance in IIM. Mortality rate in IIM is high, especially the early mortality (ie within 1 year of disease onset). Hence, close monitoring of patients is required, especially in the first year of disease.
Image and Bar Table 1

Image and Bar Table 2
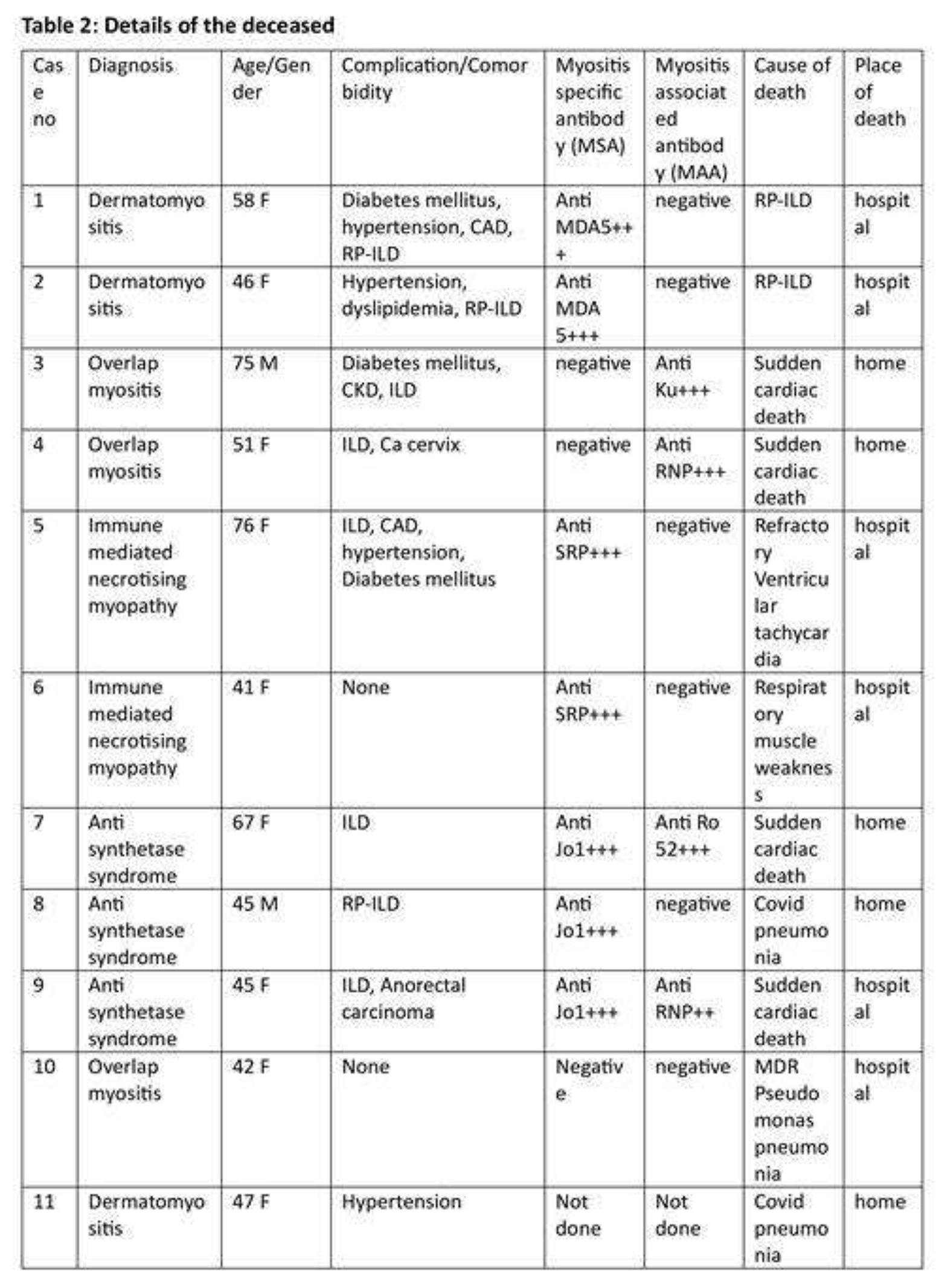
POS388
Correlation of Serum KL6 with Pulmonary Function Tests in The Monitoring of Connective Tissue Disease Related Interstitial Lung Disease: A Prospective Cohort Study (Edited Version Of Paper No 375)
Image and Bar Table 1

Image and Bar Table 2

POS389
A Study to Evaluate The Efficacy of Tofacitinib in Refractory Palindromic Rheumatism: A Retrospective Study
Image and Bar Table 1

Image and Bar Table 2
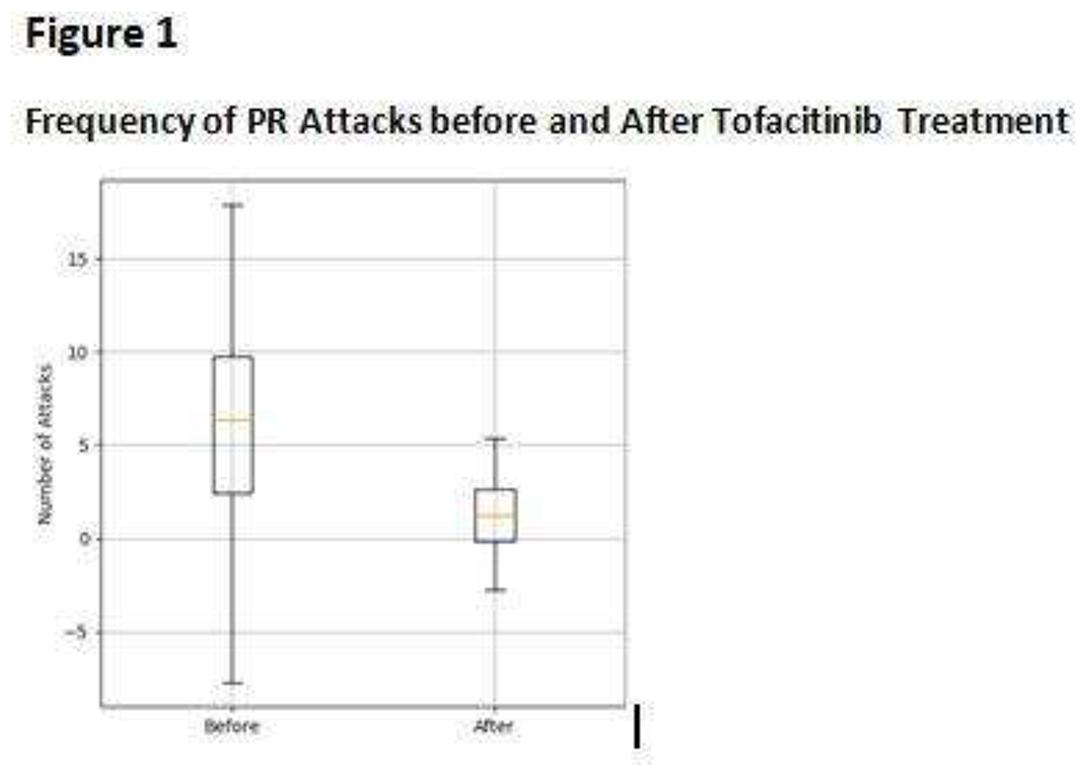

POS390
Incidence of ANA Positivity in Autoimmune Rheumatic Diseases after The Administartion of Biologicals and Its Clinical Co-Relation
1. Sharma, A., & Gupta, S. (2023). Effects of biological agents on antinuclear antibody levels in axial spondyloarthritis: A study from India. *Rheumatology International*, 43 (5), 765-772.
2. Desai, R., & Patel, V. (2022). Biological therapies and ANA dynamics in axial spondyloarthritis: Insights from an Indian cohort. *Journal of Clinical Rheumatology*, 28 (3), 205-212.
POS391
Clinical Characteristics and Outcome of Posterior Reversible Encephalopathy Syndrome in Patients with Autoimmune Rheumatic Diseases: A Retrospective Observational Study
Image and Bar Table 1

Image and Bar Table 2

POS392
Comparison of Erythrocyte Sedimentation Rate (ESR) Measurements Between Westergren’s Method and An Automated Analyser: A Bland-Altman Analysis
Image and Bar Table 1

Image and Bar Table 2

POS393
Vascular Riddles: Myeloproliferative Neoplasms as Vasculitic Mimics
Case 1:
A 69 year old lady, diagnosed as PAN, presented with persistent symptoms of paraesthesias, and ulcers over her toes. She did not respond well to immunosuppression with Inj Cyclophosphamide or steroids. Examination revealed bruit over bilateral femoral artery, and absent DPA, PTA pulsations. No organomegaly present. Doppler of bilateral lower limbs revealed stenosis of both femoral arteries more than 90 %. In view of persistent thrombocytosis and leucocytosis, with normal inflammatory markers – Myeloproliferative neoplasm screening was done - JAKV2617F mutation was positive.
Case 2:
70 year old lady, diagnosed as Hepatitis B associated PAN, with background of hypertension, with complaints of ulcers over her feet, paraesthesias and was on treatment with antivirals, steroids, and Cyclophosphamide. She continued to have persistent symptoms, despite optimal doses of immunosuppression. Examination revealed no organomegaly and dorsalis pedis and PTA were not palpable. Doppler of lower limbs revealed diffuse atherosclerosis with vascular calcification involving deep arteries of lower limbs. Inflammatory markers were normal, however leucocyotosis and thrombocytosis persistent. MPN screening panel done revealed JAK2V617F to be positive.
Case 1
ESR/CRP - 6/1.06mg/dl Creatinine - 2.04mg/dl ANA/ANCA - Negative APLA - Negative
Case 2
ESR/CRP - 3/0.04mg/dl Creat - 2.59mg/dl HbSAg - Positive ANA/ANCA - Negative APLA - Negative
Essential thrombocytosis is a slowly progressive, indolent disorder. High index of suspicion is required Elderly patients who present with MVV/LVV Cell line abnormalities are noted No response to immunosuppression Median age of onset of MPN associated vasculitis is 71 years, most common phenotype described is GPA, followed by PAN. Discordance between inflammatory markers and leucocytosis and thrombocytosis is an indicator of possible MPN Around 13% of Essential thrombocytosis patients may have no splenomegaly noted.
This case highlights the need to evaluate for malignancy as an etiology in elderly patients presenting with vasculitis features.
Image and Bar Table 1

Image and Bar Table 2

POS394
Oncologic Imposters: Malignancies Masquerading as Rheumatologic Diseases
Image and Bar Table 1

Image and Bar Table 2

POS395
Evaluating Infection Incidence in Tofacitinib Therapy: A Cross-Sectional Study
POS396
Herpes Zoster in Rheumatology Practice - Post Generic Tofacitinib Use
1. Domínguez-Casas LC, Lasa-Teja C, Ferraz-Amaro I, Castañeda S, Blanco R. Increased Risk of Herpes Zoster in Rheumatoid Arthritis Not Only Due to JAK Inhibitors-Study of 392 Patients from Single University Center. J Clin Med. 2024 May 26;13 (11):3121. doi: 10.3390/jcm13113121.
POS397
IgG4-Related Disease: From Diagnostic Dilemma to Therapeutic Success
Image and Bar Table 1

POS398
Overlap of Spondyloarthritis and Aortoarteritis: Insights from Two Cases from A Tertiary-Care Centre
1. Esen SG, Armagan B, Atas N, Ucar M, Varan Ö, Erden A, et al. Joint Bone Spine. 2019;86 (4):497–501.
2. Patelis N, Nana P, Spanos K, Tasoudis P, Brotis A, Bisdas T, et al. Ann Vasc Surg. 2021;76:555–64.
Image and Bar Table 1
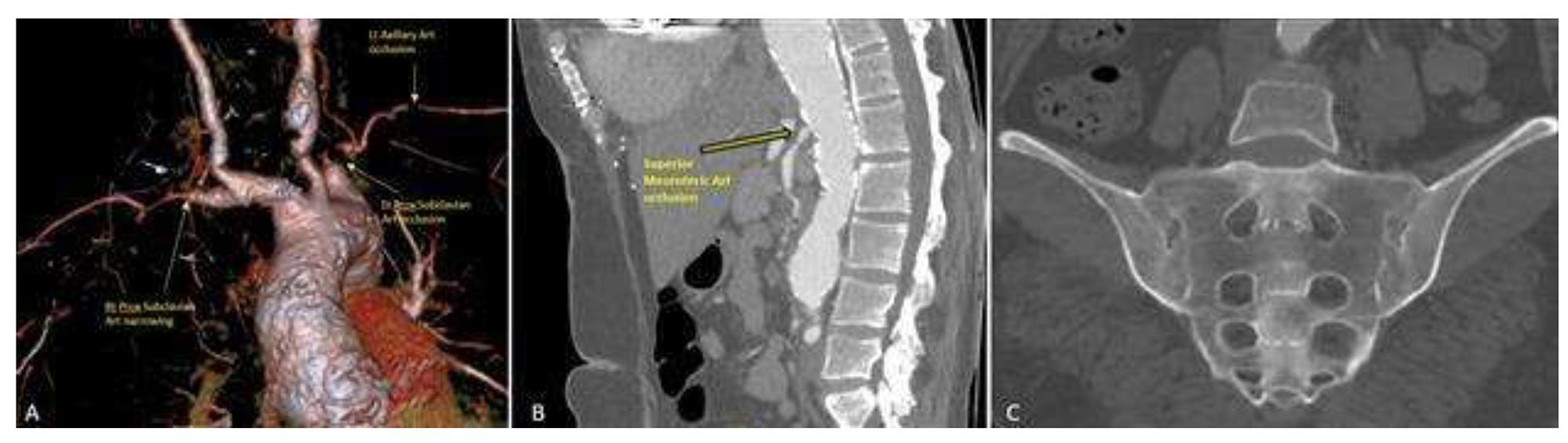
Image and Bar Table 2
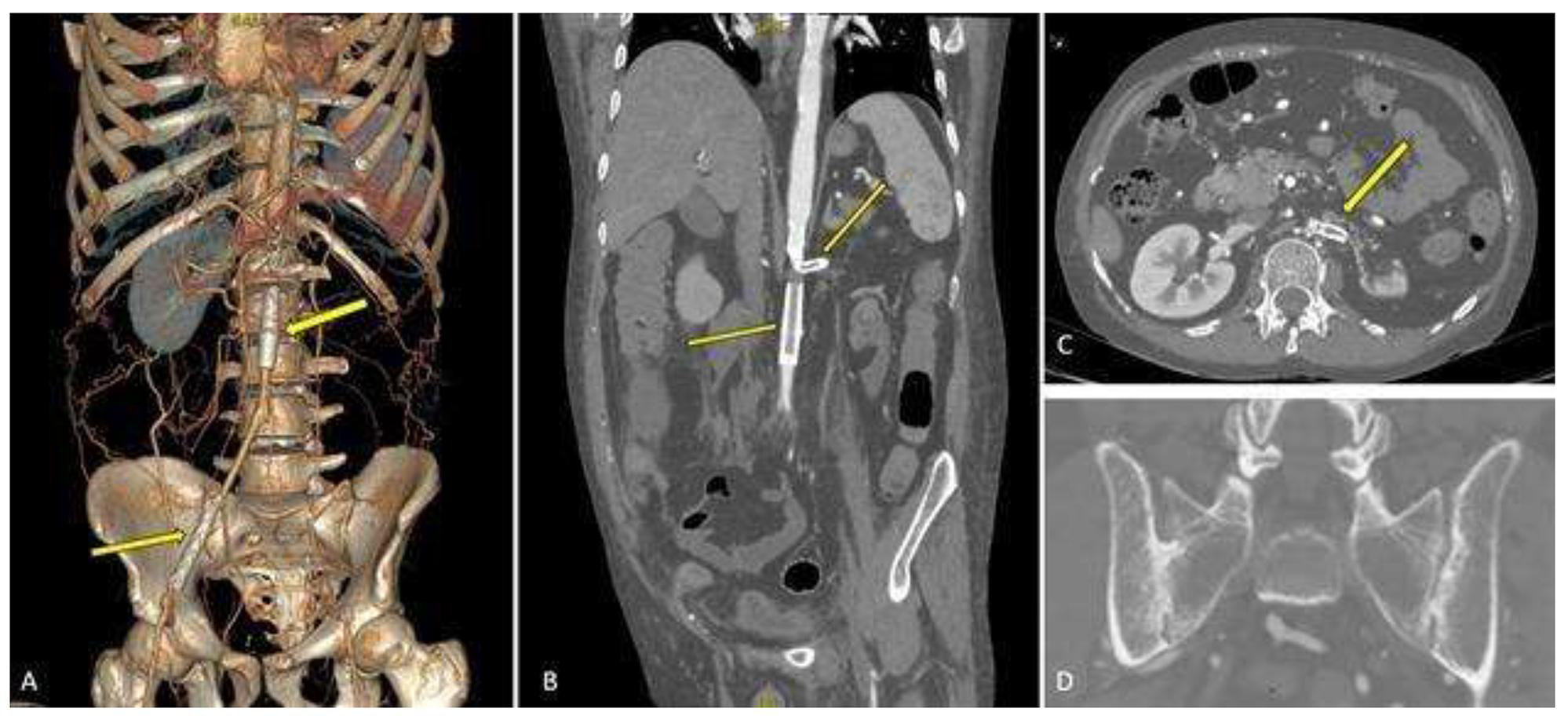
POS399
Oncologic Imposters – Malignancies Masquerading as Rheumatologic Diseases
Subsequent investigations, including advanced imaging (PET scans, MRIs), bone marrow biopsies, and cytogenetic analyses, revealed malignancies such as multiple myeloma, acute myeloid leukemia, Hodgkin’s lymphoma, prostate carcinoma, ovarian carcinoma, and Ewing’s sarcoma. Lymphoid and hematological malignancies accounted for the majority, comprising 57% of the total. The presence of unusual clinical features—such as refractory symptoms, atypical progression, or unexplained systemic signs—played a crucial role in prompting further investigation.
Image and Bar Table 1

Image and Bar Table 2

POS400
Medication Related Osteonecrosis of Jaw; Experience in a Tertiary Care Centre in UK
Chamith Rosa, Devika Dua, Banerjee Siwalik, Ganesh Kasavkar,
There are additional risk factors such as IV/parenteral drug use, cancer and chemotherapy, long duration, higher dose, dental extractions, concomitant steroid use, poorly fitting dentures, smoking, diabetes and pre-existing dental issues.
Cohort of patients under the care of rheumatology and documented evidence of osteonecrosis of the jaw by an Orofacial maxillary surgeon were selected. Demographic characteristics, anti-resorptives used, additional risk factors and subsequent management of osteoporosis were described.
Of the 5 cases, all the patients were female. All of them were on anti-resorptive therapy when they developed ONJ. Four patients were on treatment for osteoporosis while 1 developed ONJ while on treatment for multiple myeloma.
Generally, the literature does suggest an increased risk of ONJ associated with denosumab which is the case in our case series. Similarly, another well-known risk factor is the use of concomitant steroids which is also seen in a majority the cases which we have described.
Image and Bar Table 1

POS401
Masquerades and Mimics
POS402
Prenatal Binders Phenotype in Mothers Affected with Rheumatic Disorders - Case Series
Patients 1, 3 and 5 have delivered healthy babies uneventfully. Two newborns had slightly depressed nasal bridges, there were no feeding difficulties or bony abnormalities.
Image and Bar Table 1

Image and Bar Table 2


POS403
Tenofovir and the Subtle Onset of Osteomalacia: Cracks Beneath the Surface
On examination, she had tenderness over her ribs, shins, and bilateral hip joint line. Faber’s test was positive on both sides. There were no signs of other systemic disease.
In the setting of elevated creatinine with metabolic acidosis, low serum phosphate, high ALP, and radiographic findings of pseudo-fractures, the diagnosis of tenofovir-induced Fanconi syndrome, with osteomalacia was considered. The absence of other risk factors for bone disease further supported tenofovir as the primary cause. Tenofovir was changed to an alternative antiviral agent, abacavir. Additionally, phosphate, vitamin D, and calcium were supplemented to address the underlying mineral deficiencies and promote bone mineralization. At 3-month follow-up, the patient reported significant relief from symptoms with phosphate and ALP returning to normal levels. No new fracture was reported in the meantime.
1. Joseph A, Cherian KE, Diabetes Metab Case Rep. 2023 Mar 1;2023 (1):22-0259.
Image and Bar Table 1

POS404
Infection Burden is Highest in the First Year of Rituximab Use in Autoimmune Rheumatic Diseases:a Single Center Study from North India
Among the microbiologically proven infections (45.6%), bacterial infections (80.9%) were predominant. Enterococcus (4), Klebsiella (4), E.coli (4) and Pseudomonas (3) were the most common. Of the opportunistic infections, 2 had Cytomegalovirus and 3 had Herpes zoster, 1 had Candida and 2 had M. tuberculosis. On univariate and multivariate analysis, no significant association was found with serious infections, although IgM and IgG levels were closely approaching significance cut-off.
Mortality occurred in 2 patients with suspected CMV pneumonitis. On Kaplan-Meier analysis, 1-year and 5-year infection free survival was found to be 82.2% (76%-89%) and 59.1% (48.1-72.7%) respectively.
Image and Bar Table 1

Image and Bar Table 2

POS405
Development of A Mobile App for Imaging of Leg Ulcers
1. Md. Talat Mahmud, Faria Soroni, Mohammad Monirujjaman Khan. Development of a Mobile Application for Patient’s Medical Record and History. [https://www.researchgate.net/publication/352642992]
2. C. Lee Ventola, MS - Mobile Devices and Apps for Health Care Professionals: Uses and Benefits. [
POS406
Outcomes of Thrombocytopenia in Various Connective Tissue Diseases in a Tertiary Care Hospital
Image and Bar Table 1

Image and Bar Table 2
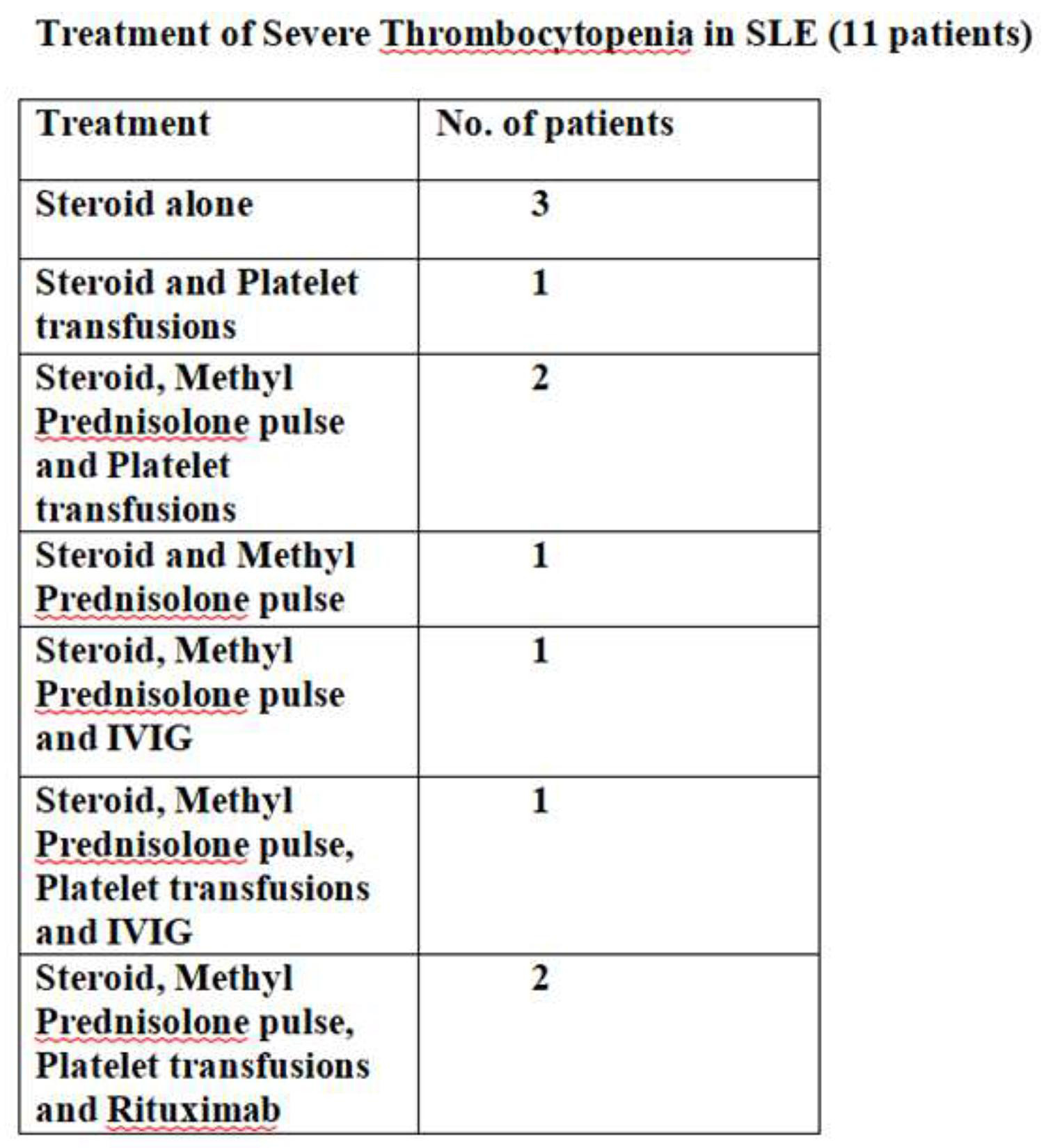
POS407
Observational Study of Fatigue in Rheumatic Diseases
This study on patients with rheumatological diseases tried to identify the fatigue and its impact on quality of life.
Study design: Prospective Oral questionnaire method.
Questionnaires:
MHAQ for RA, SLE and PS
BASFI for AS
FIQ for FMS
DAS28 for RA.
SLEDAI for SLE.
BASDAI for AS
SS for FMS
PSARC for PS
Sample size: 50 consecutive patients under rheumatological care
Inclusion criteria:
All patients with diagnosed autoimmune conditions
Exclusion criteria:
Children < 18 years
Pregnant females
Patients under psychiatric medications
In the patient group, there was 32 females and 12 males with mean age 40.7 ± 19.3 years. The patient group included 4 subgroups: RA, SLE, AS, and FM. 50% (10 of 20) of RA patients had active disease (DAS28 mean=3.55). 45.4% (5 of 11) of SLE patients had moderate disease activity (SLEDAI mean=15.18). 44.4% (4 of 9) of AS patients had high disease activity (BASDAI mean=4.55).
Confounding factors- Depression, Vitamin D deficiency, FMS coexistent.
Further data will be submitted during the conference.
Discussion: Maha K. Khallaf et al described fatigue in rheumatological diseases in 2019. Their results showed that most (35%) of RA patients had moderate disease activity, 60% of SLE patients had high disease activity, and 46.4% of AS patients had severe disease activity. In the current study, results are found to be similar to the previous one. Further clarity will be obtained with a higher sample size.
Image and Bar Table 1
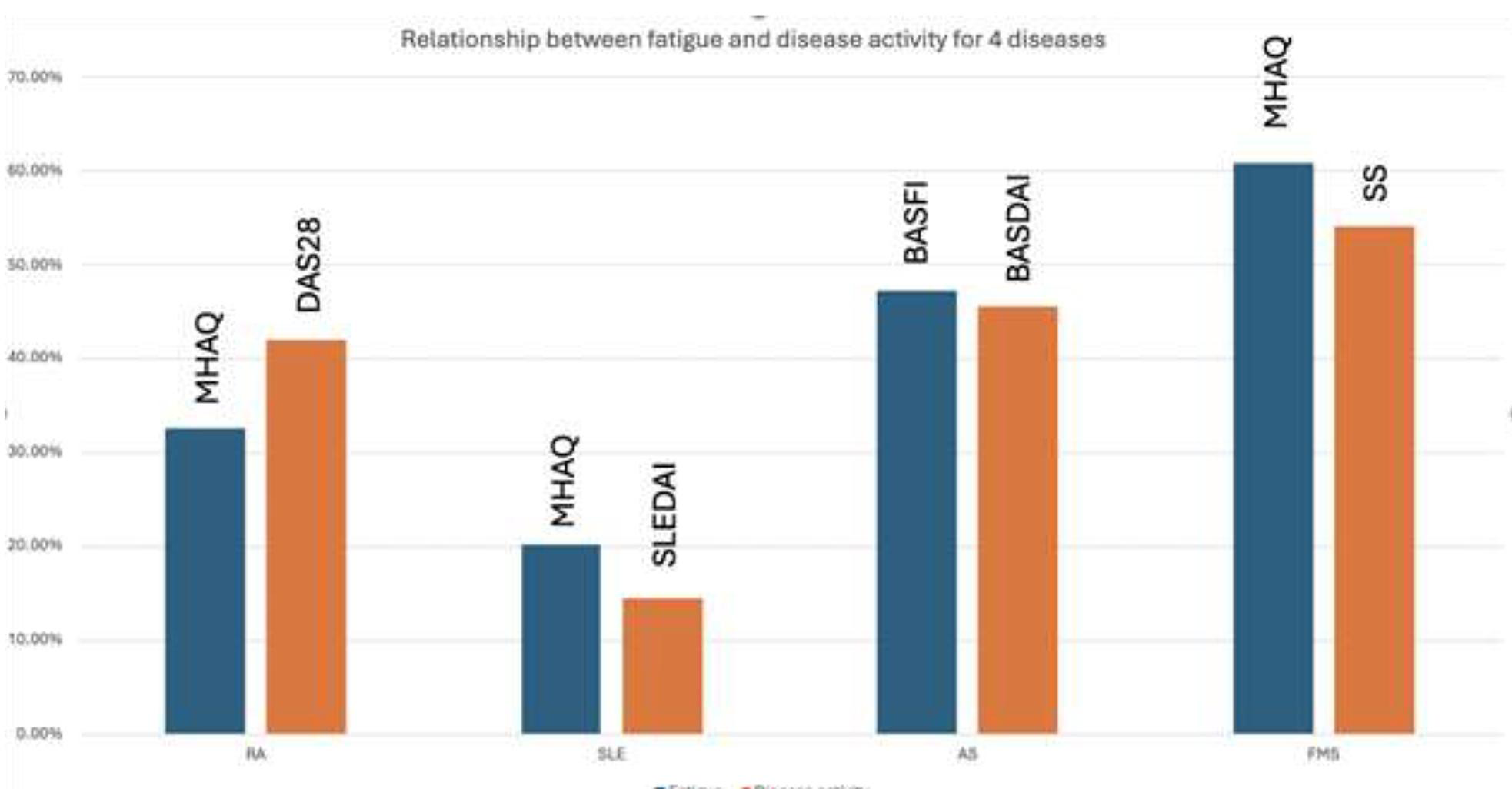
Image and Bar Table 2

POS408
Descriptive Analysis of Patients of Inflammatory Myositis: A Tale of Two Centers
Constitutional - fever (35.62%; N=27), fatigue (26.92%; N=21) Mucocutaneous - oral ulcers (16.67%; N=13) Other CTD related features - alopecia (17.95%; N=14)
Out of 78 patients, 25 were anemic, 4 had leukocytopenia (TLC < 4kU/L) and 4 had thrombocytopenia (PC <1 lakh/μL). A total of 38 patients had enzyme elevation 3x above upper-normal-limit (LDH/CPK/AST/ALT).
While the subsets of myositis in our data matched those reported elsewhere from India and the West, we had a greater proportion presenting with arthritis/arthralgias and lesser with muscle weakness/myalgias and dysphagia. As compared to the West, we had lesser proportion with ILD and Raynaud’s phenomenon. The MSA/MAA profile also matched that reported from other Indian series.
Image and Bar Table 1

Image and Bar Table 2
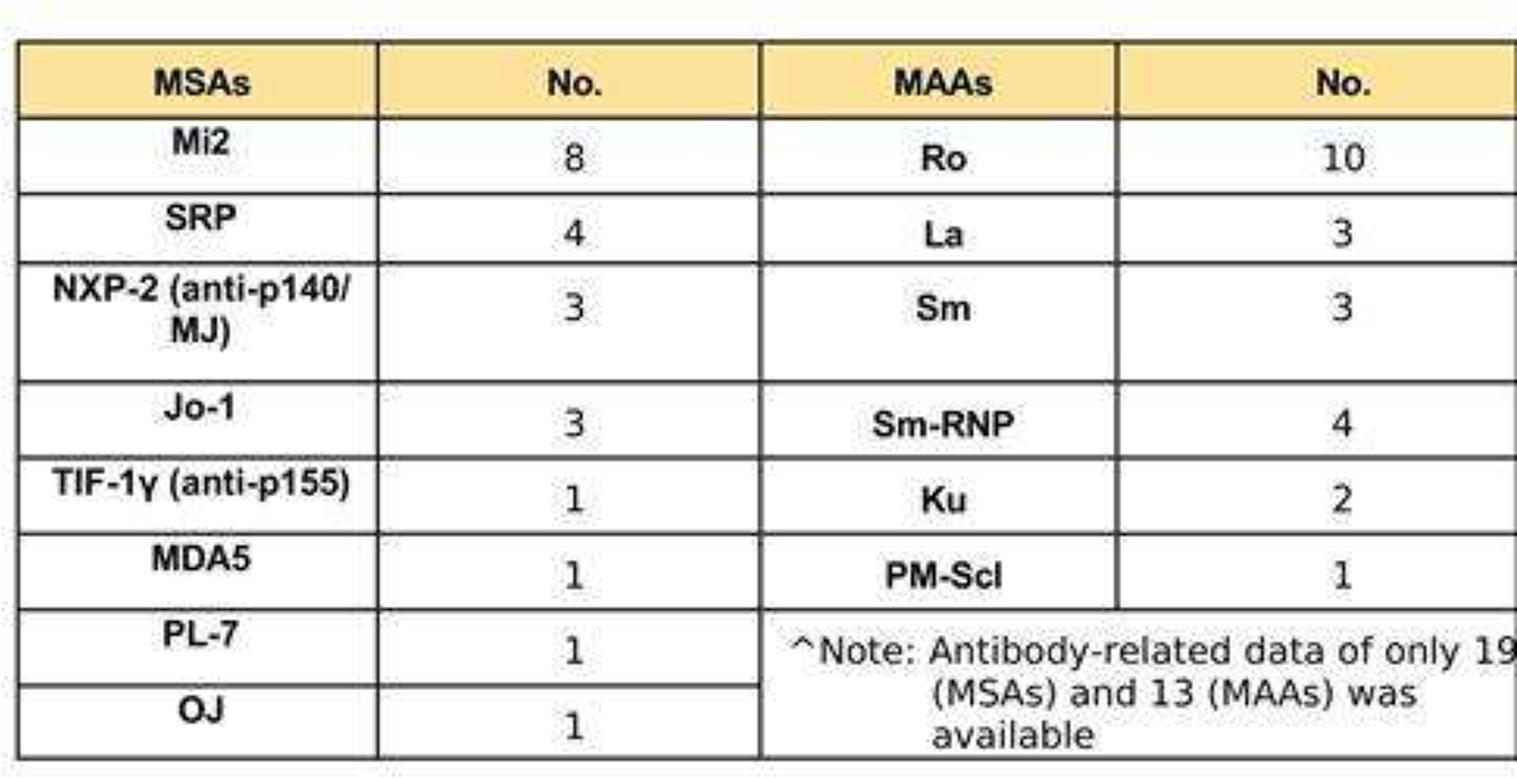
POS409
“Medical Gangrene”: Don’t Wait, Call a Rheumatologist
Image and Bar Table 1

POS410
Hansen’s as A Rheumatological Mimic: Observations from A Tertiary Care Centre in North India
On microbiological evaluation, Slit Skin Smear was positive in 21 (75%) patients. Biopsy was available in 15 patients, of which 10 patients had evidence of Hansen’s on skin biopsy, 10 on nerve biopsy. On immunological evaluation, 8 patients had antibody positivity in the form of Rheumatoid Factor (n=1), Anti CCP (n=2), ANA (n=2), ENA (n=3). Abnormality in radiography was observed in 5 patients, Metacarpophalangeal erosions (n=1), Carpal crowding, joint space narrowing (n=1), acro-osteolysis (n=1), bilateral sacroiliitis (n=1), Charcot (n=1). Follow up data was available for 19 patients, most of the patients responded to multidrug anti-leprosy therapy and glucocorticoids. On follow up, One patient had developed Dapsone induced haemolytic anaemia, 1 had Dapsone induced liver injury, 2 patients had presented with Lepra reaction, 1 patient developed neuropathic ulcers.
Image and Bar Table 1

POS411
Myelitis in Different Rheumatological Disorders: Hide and Seek
Image and Bar Table 1

POS412
Rheumatic Burden of Tuberculosis: A Single Center Experience
Image and Bar Table 1

Image and Bar Table 2

POS413
Clinical Medicine will Never Die- A Review of Six Patients with Rheumatoid Arthritis and Clinically Detected Papillary Carcinoma Thyroid
Shehanaaz Begum, Anjana Varier,
POS414
Chronic Arthritis and Dactylitis Following Foreign Body Prick: Two Cases from Eastern India
The case reports:
In both the above cases, only the site of prick was involved. There were no systemic features. ESR and CRP were raised in both.
1. Mangat P, Jawad ASM. A case of rose thorn tenosynovitis. Grand Rounds. 2007;7:16-17. DOI: 10.1102/1470-5206.2007.0001
Image and Bar Table 1
Image and Bar Table 2

POS415
A Rare Manifestation of Neuro-Behçet’s Disease- Paroxysmal Dysarthria Caused by A Single Demyelinating Midbrain Lesion
Image and Bar Table 1

Image and Bar Table 2

POS416
Polyarteritis Nodosa: A Rare Disease Which Remain Undiagnosed
In our patient, although there was no risk factor for PAD, the initial complaint of pain and gangrene led to misdiagnosis of peripheral arterial disease. However, as the disease process progressed bowel and renal involvement became obvious which led to suspicion of systemic vasculitis. Arteriogram and biopsy revealed features suggesting PAN.
In a case of limb ischemia when there is lack of risk factors and other features of PAD, there should be high degree of suspicion for PAN as reaching the correct diagnoses and starting early treatment are crucial for its prognosis.
POS417
Pachydermoperiostosis (Touraine–Solente–Gole syndrome): Familial Clubbing - A Case Series
Pachydermoperiostosis (PDP) is a rare disorder characterized by clubbing (acropachy) of the fingers and toes; thickening of the skin (pachyderma), usually of the face; excessive sweating (hyperhidrosis); and new bone formation associated with joint pain. The three dermatologists Touraine, Solente, and Gole recognized this condition as a familial disorder presenting in three forms, namely complete (periostosis and pachyderma), incomplete (without pachyderma), and the forme fruste (pachydermia with minimal skeletal changes). PDP is therefore also known as the Touraine–Solente–Gole syndrome. The estimated prevalence is of approximately 0.16%. It usually manifests in adolescence, occurring almost exclusively in males, with a male to female ratio of 7:1.
POS418
Upper Extremity Deep Vein thrombosis (UEDVT) in SLE and APS
1. Nikolova-Vlahova MK, Nikolov KV, Baleva MP, Savov AS. Antiphospholipid antibodies in patients with upper-extremity deep vein thrombosis. Cent Eur J Immunol. 2015;40 (3):307–10.
Contrast-enhanced CT - coronal (left) and axial (right) images showing hypodense filling defects in the left brachiocephalic vein
Image and Bar Table 1
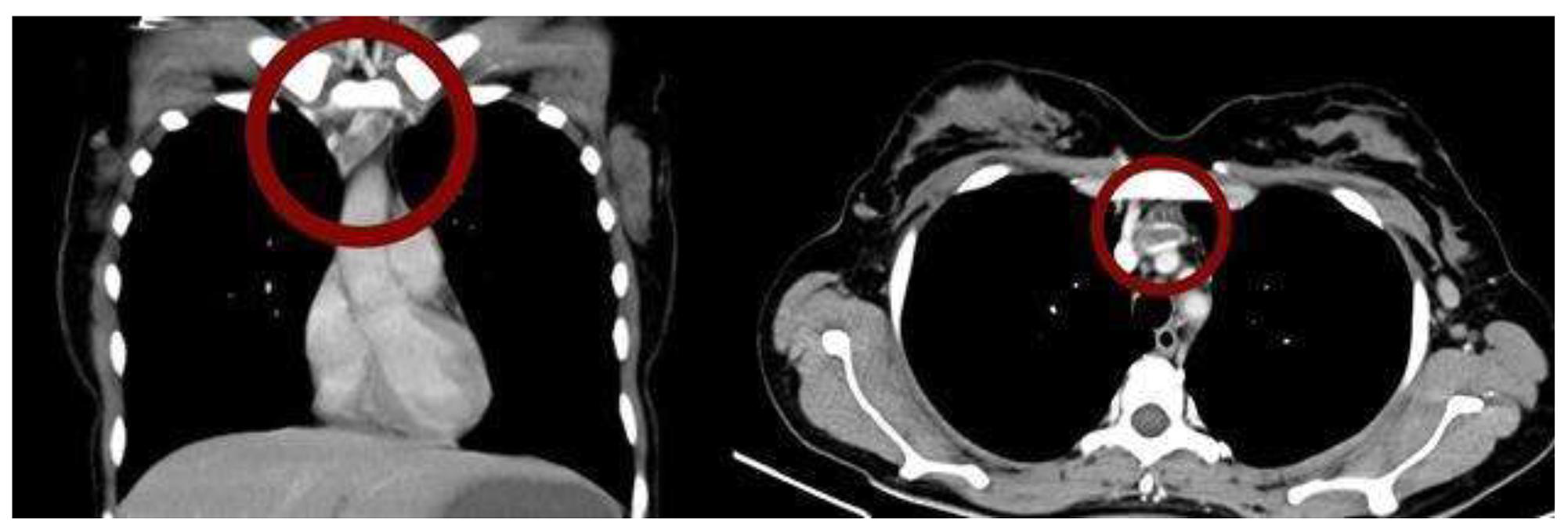
Image and Bar Table 2
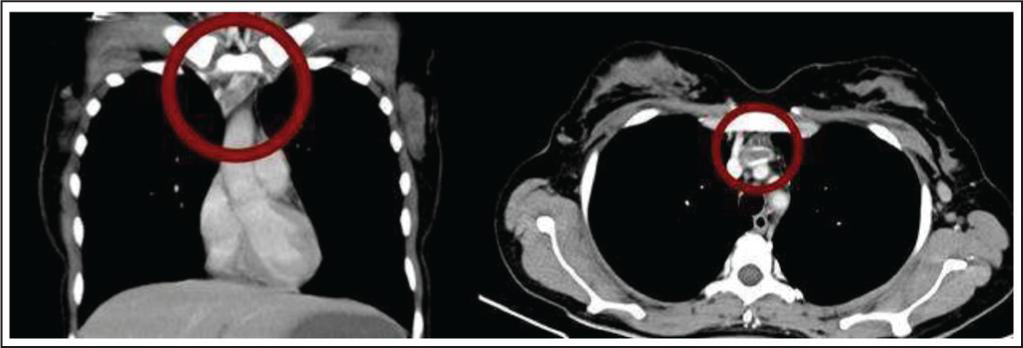
POS419
An Uncommon Presentation of Takayasu Arteritis - Masquerading Ear Pain
On further examination blood pressure (BP) and pulse of both arms were normal and equal. Examination of the neck revealed bilateral carotid bruits. Her ESR and CRP were high. Ultrasound scan neck and doppler of neck vessels showed significant luminal narrowing of bilateral common carotid arteries with right more than left. CT angiogram of the neck vessels detected narrowing of the common carotid arteries by 80% more in the right together with bilateral subclavian stenosis. Angiography of the abdominal vessels were normal. Based on the above findings she was diagnosed as TA and successfully managed with steroids and Methotrexate. Her ear pain was resolved following commencement of the steroids.
POS420
Glancing the Out of Ordinaries in A Critical Juncture: Pulmonary Arterial Hypertension in Systemic Lupus Erythematosus
POS421
Nail Fold Capillaroscopy in Healthy Individuals: A Single Centre Cross-sectional Observational Study from Southern India
As compared to an Italian cohort, our population had lower capillary density, greater capillary width and intercapillary distance. Comparison with another Indian cohort revealed greater percentage of enlarged capillaries and avascular areas in our population. Difficulties in visualizing capillaries due to pigments in dark-skinned individuals can affect accurate reporting of pathologic patterns.
Image and Bar Table 1

Image and Bar Table 2
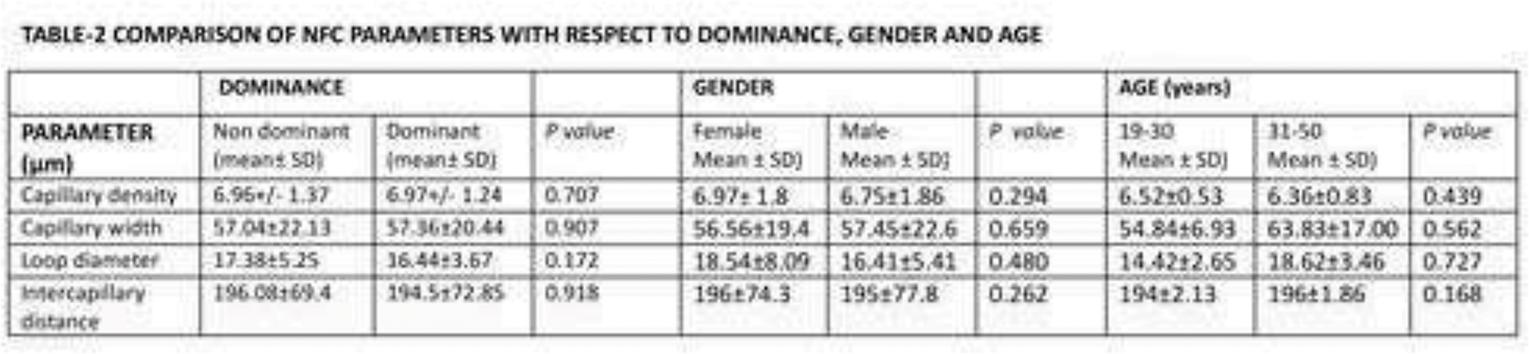
POS422
Sulfasalazine Versus Tofacitinib in Refractory Reactive Arthritis
Image and Bar Table 1

Image and Bar Table 2

POS423
Acute Transverse Myelitis and Spinal Subarachnoid Haemorrhage - A Rare Presentation of IgA Vasculitis
Image and Bar Table 1

Image and Bar Table 2

POS424
A Case of Recurrent Anaemia in Sickle Cell Disease- A Serendipitous Solution
A 29-year-old female, diagnosed with sickle cell anaemia six years back, presented with complaints of fatigue, bilateral lower limb swelling and fever for 3 months. The fever was intermittent, documented at 100 F with no localising symptoms. Over the course of 3 months, she was treated in multiple hospitals for recurrent severe anaemia and received 18 PRBC transfusions, steroids and hydroxyurea.
At presentation, she had a normocytic normochromic anaemia of 7.6, creatinine of 1.51, indirect hyperbilirubinemia, normal LDH and corrected reticulocyte counts. Previous reports showed deranged renal function with creatinine values ranging from 0.8 to 1.47 mg/dl and a normal urinalysis. DCT and ICT were negative. Bone marrow biopsy showed trilineage haematopoiesis.
Initially, anaemia due to hydroxyurea usage was suspected but there was no improvement in Hb after stopping the drug. Based on renal dysfunction, sickle cell nephropathy with anaemia of chronic disease was thought of and erythropoietin injections were started. However, as ultrasound showed normal kidney size with maintained CMD, a diagnosis of sickle cell nephropathy was unlikely. ANA was negative, complement levels were normal and 24-hour urinary protein showed proteinuria of 1.32 gm /day, hence, a renal biopsy was planned. Vasculitis workup revealed positive anti-PR3 antibodies (>200 IU/ml) and negative anti-MPO antibodies for which steroids were started. PRBC transfusions were given and a renal biopsy was done but a further drop in haemoglobin, precipitating heart failure, was seen despite no biopsy-related complications. The biopsy report revealed crescentic and necrotising glomerulonephritis with insignificant glomerular immune complex deposits, suggesting renal limited PR3 ANCA-associated vasculitis. The patient received 1 dose of Rituximab and was discharged on oral steroids and EPO injections with an Hb of 6.8 gm/dl. On follow-up, Hb had increased to 8.57 g/dl with normal creatinine. Retrospectively, a diagnosis of recurrent anaemia due to delayed haemolytic transfusion reaction that responded to Rituximab given for ANCA-associated vasculitis was made.
ANCA-related vasculitis is a rare rheumatological disease with an incidence of 24.7 to 33 per million globally, with renal-limited vasculitis being even rarer and presenting with multiple non-specific features such as anaemia, fever, weight loss and rashes. This case highlights the need for extensive evaluation of recurrent anaemia and renal dysfunction and the importance of keeping a low threshold for evaluation of vasculitis, despite its low incidence, as early diagnosis is crucial for the initiation of treatment and prevention of progression to CKD.
Image and Bar Table 1

Image and Bar Table 2

POS425
A Case of Subcutaneous Panniculitis Like T Cell Lymphoma with Macrophage Activation Syndrome
Incisional skin biopsy was done from the right upper quadrant of abdomen. During her hospital stay, she started having increase in frequency of fever spikes, pancytopenia (Hemoglobin 7.8g/dl, total leucocyte count 3150/cu.mm, platelet count 45000/cu.mm), ESR of 2, high ferritin (>10800mcg/ml), high triglycerides (638mg/dl) and low fibrinogen (103). She was diagnosed to have macrophage activation syndrome and there was no evidence of active infection. She was treated on methylprednisolone pulse, IVIG and later started on tacrolimus. She became afebrile with this therapy and her cytopenias didn’t worsen further.
Histopathology of skin biopsy revealed lobular infiltration of scattered atypical lymphoid cells within the subcutaneous adipose tissue along with necrosis (Fig 2). Immunohistochemistry showed atypical cells are CD3 positive, CD4 & CD20 negative and Ki67 index of 70-80%. The diagnosis of subcutaneous panniculitis like T cell lymphoma (SPTCL) was made and she was transferred to Hematology. She developed sepsis, septic shock, and acute respiratory distress during her stay in Hematology and succumbed to her illness a month later.
Image and Bar Table 1

Image and Bar Table 2

POS426
“Unraveling the Complexity – A Case Series on IgG4-Related Disease”
Patients were divided into 4 major clusters based on phenotypic presentation. 7 (15.2%) each in Cluster 1 (Pancreatic and hepatobiliary) and Cluster 2 (Retroperitoneal fibrosis, aortitis); 19 (41.3%) in Cluster 3 (head and neck); 14 (30.4%) in Cluster 4 (Classic Mikulicz) and 22 (47%) had other system involvement.
Most common presentation was head and neck involvement in 19 patients (41.3%). Rare presentations were hypertrophic pachymeningitis (3) superior mediastinal mass, subglottic stenosis, hilar and renal mass (1 each).
Site-specific imaging was done in 44 patients (95.6%). Elevated serum IgG4 levels were seen in 42 patients (91.3%). Serum eosinophilia was seen in 6 (13%)
36 (78%) underwent biopsy of the involved organ and had histopathological findings consistent with a diagnosis of IgG4-RD. Among 46 patients, 18 (39.1%) were definite; 6 (13%) were probable and 22 (47.8%) were possible IgG4RD as per revised comprehensive diagnostic (RCD) criteria. Biopsy was not done in 10 (21.7%) patients due to inaccessibility of involved tissue or refusal to provide consent.
45 (97.8%) patients received glucocorticoids and steroid sparing drugs. Patient with hilar mass underwent lobectomy which was curative. Across various treatment regimes, 10 (21.7%) received Methotrexate, 21 (45.6%) MMF, 4 (8.6%) Azathioprine and 1 Tofacitinib and 4 (8.6%) received combination DMARDs.20 (43%) patients received Rituximab. 8 (17.4%) failed conventional DMARDs before RTX.
Organ-specific clinical improvement was seen in 35 (76%) patients; relapse/poor response in 9 (19.5%). 2 patients succumbed to infection.
Image and Bar Table 1

Image and Bar Table 2
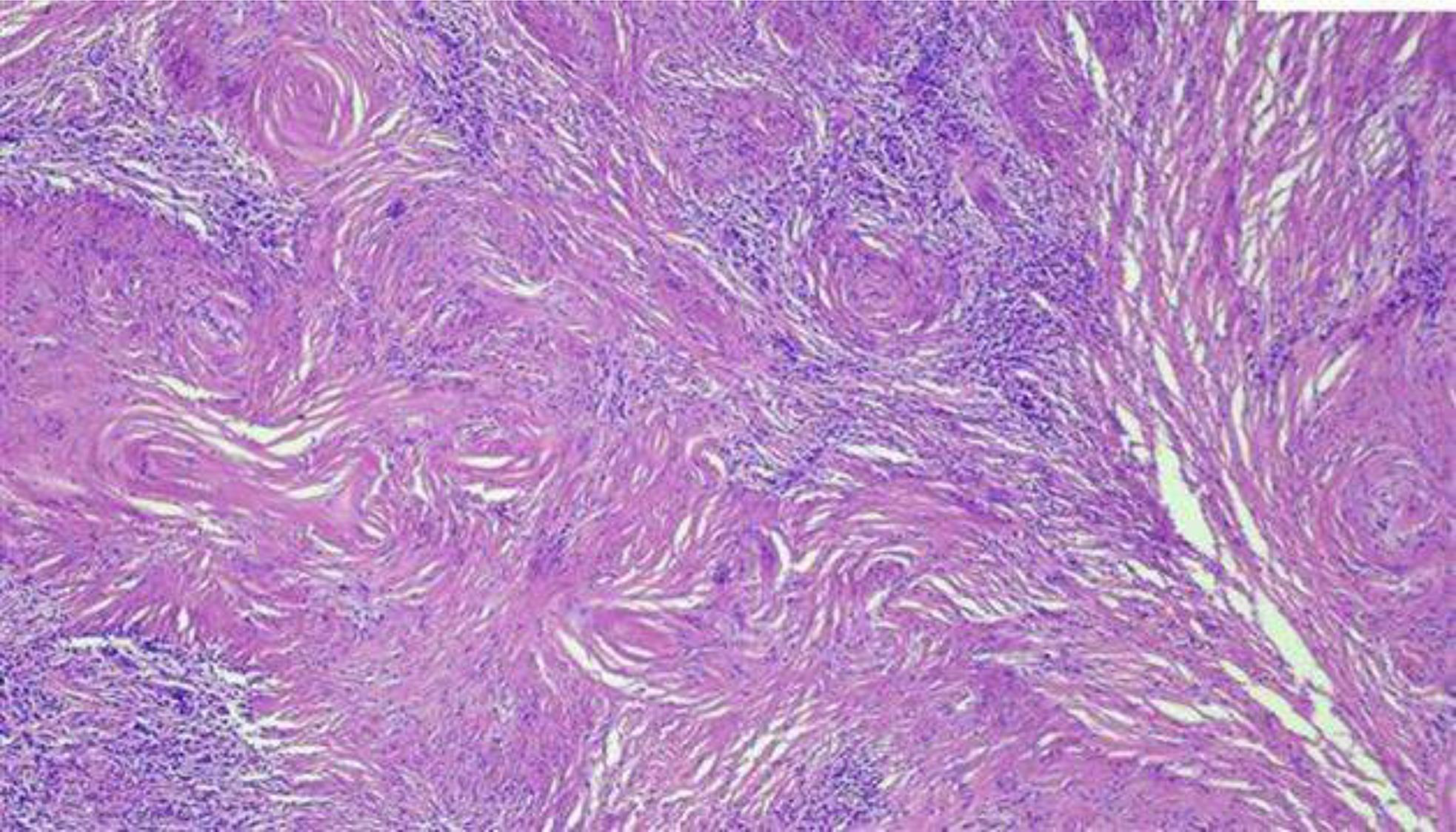
POS427
A Rare Presentation of Behcet’s Disease
Image and Bar Table 1

Image and Bar Table 2

POS428
Uncommon Presentation of Type 4 Renal Tubular Acidosis in Systemic Lupus Erythematosus: A Case Report and Review
Image and Bar Table 1

POS429
Idiopathic Granulomatous Mastitis: A Respondent and A Non-Respondent
A 25 years old lady presented with complaints of right sided breast lump associated with pus discharge for 3 months. She didn’t complain of fever or weight loss. She has 2 children, one 10 years old (breast fed for 5 years) and another 4 years old (breast fed for 3 months). Ultrasonography of breast suggested mastitis and ductal ectasia. Patient was initially prescribed oral antibiotics followed by which she had undergone incision and drainage considering infectious etiology. Her pus sample cultures were negative and acid-fast bacilli were absent. Her swelling re-appeared, subsequently she had undergone left breast quadrantectomy. The histopathology was suggestive of cystic granulomatous mastitis. She was started on oral steroids and methotrexate, and later on oral steroids were tapered off as she responded well to methotrexate.
Our second patient was a 25 years old lady who had history of multiple and recurrent bilateral breast lumps for 6 months. She has 2 children, one 5 years old and another 4 years old (breast feeding stopped 2 years back). She was treated as breast abscess and was given antibiotics. She had undergone 3 surgeries for removal of breast lumps followed by which she repeatedly developed painful swelling with pus discharge at the operated sites. Ultrasonography of her breasts showed diffuse mastitis with abscess formation. Her histopathology report showed cystic neutrophilic granulomatous mastitis.
She was started on steroids in form of prednisolone 0.5mg/kg 10 months back which was tapered every week. 9 months back she was started on injection methotrexate 0.3mg/kg/week due to continued formation of new lesions and steroids continued in tapering dose. Eight months back she was started on mycophenolate mofetil sodium 360mg BD and then thrice daily and dose of injection methotrexate increased to 0.4mg/kg/week. Five months back she still continued to develop new lesions with pus discharging sinuses despite 3 months of treatment with mycophenolate mofetil and methotrexate. Injection adalimumab 40mg subcutaneous once every 2 weeks was started and methotrexate was continued. Subsequently new lesions stopped appearing and pus discharge was absent. Injection adalimumab frequency was reduced to once every 4 weeks over next 3 months and steroids tapered off.
Idiopathic granulomatous mastitis (IGM), a diagnosis of exclusion, is often initially misdiagnosed as furunculosis or cellulitis. After ruling out infectious causes in a case of repeated breast abscess, diagnosis of IGM should be considered.
Image and Bar Table 1

Image and Bar Table 2

POS430
A Mysterious Case of Neck Swelling
A 41-year-old female, presented with complaints of right-sided neck swelling and pain for 1 year. She had no complaints of dizziness, fatigue, syncope, upper limb claudication or limb weakness. History of 2 episodes of nodular episcleritis in the right eye was present 2 years back. Initially, a right-sided nerve sheath or carotid body tumour was suspected, and an MRI revealed an ill-defined hyper-intense soft tissue mass in the carotid sheath at the carotid artery bifurcation. A carotid doppler showed circumferential moderate wall thickening in the right carotid bulb causing 30% luminal stenosis. A carotid artery biopsy showed adventitia with patchy dense lymphoplasmacytic infiltrate around vasa vasorum with focal neutrophilic infiltrate and necrosis and IgG4 staining was negative. Serum IgG4 was normal, and autoimmune markers (ANA, ANCA) were negative. CECT abdomen was done, which was normal.
The patient was managed outside with 5 doses of monthly Cyclophosphamide and prednisolone following which symptoms resolved. A month later, a recurrence of right-sided neck swelling and carotidynia prompted the patient to present at our centre. On reviewing the history, the possibility of TIPIC syndrome versus isolated carotid vasculitis was considered.
A CT angiography of neck vessels done, revealed stenosis of the right common carotid artery throughout its length, with 60-80% stenosis at the carotid bulb and complete occlusion of the right ICA with collateral formation supplying the right MCA and ACA. The rest of the branches of the aortic arch were normal.
Inflammatory markers, such as ESR (51mm/hr) and CRP (14mg/dl) were elevated.
Such recurrent course of the disease and rapid progression with severity (complete occlusion of right ICA) ruled out the TIPIC syndrome. Considering the isolated involvement of the right carotid artery, a diagnosis of isolated carotid vasculitis was made. She was restarted on high-dose prednisolone and weekly methotrexate (15 mg).
Very few reports are present in the literature of patients with isolated carotid vasculitis without fulfilling the criteria for systemic vasculitis such as Takayasu arteritis or GCA. Data regarding the natural history and outcome of patients with isolated carotid vasculitis are lacking. Only more extensive studies would identify whether isolated carotid vasculitis should be considered a separate disease or merely, an initial presentation of a systemic large vessel vasculitis.
POS431
A Case Series of 3 Atypical Cases of Behcet’s Disease Away From the Silk Route
Image and Bar Table 1

Image and Bar Table 2

POS432
An Interesting Case of Metoprolol Induced Periungual Pyogenic Granuloma
POS433
A Case Report of SLE with Multiorgan Involvement, Infection and Treatment Complications: The Warrior Who Survived all Odds
Now, she presented with complaints of fever and cough for 1 month, abdominal pain for 6 days, acute onset shortness of breath for 5 days. She was taken to private hospital where she was intubated and suffered cardiac arrest twice, requiring CPR with successful ROSC. Thereafter, she was extubated after 3 days, but took LAMA and came to our center. On examination, she had pallor, tachycardia, tachypnea, BP 140/90 mmHg, bronchial breath sound in left mammary area with decreased breath sounds, epigastric tenderness with normal bowel sounds. Evaluation revealed Hb 7 g/dl, schistocytes 3%, LDH 1106 U/L, DCT positivity, TLC 15900/mm3, platelets 90000/mm3, albumin 2.3 g/dl, creatinine 1.5 mg/dl, amylase 272, lipase 225 U/L, ProBNP >35000 pg/ml, C3/C4 22.3 and <7.4 mg/dl, dsDNA 170.98 IU/ml, CRP 15.3 mg/dl, procal 6.06 ng/ml, urine r/m showing albumin, 5-6 RBCs and 24 hour urine protein of 700 mg/day. 2D-Echo revealed EF of 40% with global left ventricle hypokinesia. Ultrasound abdomen revealed pancreatitis (Figure 1). CTPA+HRCT Chest revealed pneumonia with synpneumonic effusion without embolism (Figure 2). Sputum workup revealed gram positive cocci. Left side pleural fluid tapping revealed TC/DC 4800/80% neutrophils and was transudative. Diagnosis of pneumonia along with lupus nephritis, pancreatitis, myocarditis, myositis, AIHA, thrombocytopenia, mucocutaneous with SLEDAI of 26 was made. She was started on antibiotics (teicoplanin and meropenem) along with 0.5 mg/kg prednisolone equivalent (dexamethasone 4 mg). Furthermore, she developed iatrogenic left pneumothorax, which was managed with pigtail insertion. Patient improved with treatment and completed NIH protocol on follow-up and was put on MMF 2g maintenance, and is currently doing well.
Image and Bar Table 1

Image and Bar Table 2

POS434
From Weakness to Sepsis- A Complicated Case of Rheumatoid Vasculitis (RV)
A 35 year old female k/c/o RA for 10 years, on DMARDS which she defaulted for last 2 months presented with acute onset tingling, numbness and weakness of all 4 limbs in an asymmeytric fashion, a ulcer over left foot for 20 days and fever for last 5 days.There was no history of rash, sinusitis, asthma, hematuria or abdominal pain. She was not a known diabetic or a smoker. On examination Temperature was 100.8 F, HR 120/minute, BP 128/84 mmHg, and RR 20/min. There were two circular ulcerating lesions: 8 x 8 cm on the left lateral malleolus and 4 x 4 cm on the dorsum of the left foot. Both had mild mucopurulent discharge.Distal pulses were palpable.Neurologic examination revealed reduced power in distal muscle groups than proximal with graded impaired proprioception, pin prick and fine touch in the distal extremities.Generalized hyporeflexia was present.Labs showed Hb 10.4g/dl, TLC 17400/μl and negative for ANA, anti PR3, anti MPO and HIV, HBsAG, HCV.Urine routine microscopy was normal. CT angiogram was within normal limits.EMG and NCS showed asymmetric axonal sensory-motor neuropathy.Punch biopsy was suggestive of necrotizing arteritis.Tissue culture from ulcer were sterile. The clinical picture was consistent with the diagnosis of Rheumatoid vasculitis with cutaneous (ulcer) and neurologic (mononeuritis multiplex) involvement. The patient was started on pulse steroids, methotrexate along with antibiotics. Higher immunosuppression was deferred in view of sepsis secondary to infected ulcer. On six weeks follow up, there was marked improvement with power returning to near normal and continued healing of the wound.
RA patient presenting with a ulcer and neurological weakness may not always be vasculitis. Ulcer may be related to venous or arterial insufficiency, trauma, Felty’s, prothrombotic states including APS, infectious or hematologic diseases, and pyoderma gangrenosum. Neuropathy can be due to drugs, CIDP among various other causes.
Vasculitis in a RA patient can be due to DMARDs, Infections, malignancy or co-exisiting autoimmune disorders like ANCA vasculitis, PAN, Cryoglobulinemia, SLE, APS, Sjogren’s. RV should be considering only after ruling out these causes. Vascuitic ulcers when get infected should be managed promptly with antibiotics but immunosuppression remains the mainstay of treatment.
Image and Bar Table 1

Image and Bar Table 2

POS435
Spontaneous Perinephric Hematoma in A Patient with Granulomatosis with Polyangiitis
A 60 year old man, known case of hypertension and hypothyroidism presented with fever, fatigue and dull aching periumblical pain with no radiation of one week duration. Clinically he had pallor, bilateral pedal edema, high BP and bibasilar crackles on chest examination. His lab investigations were suggestive of anemia, PMN leucocytosis, positive CRP, active urine sediments (2+ proteins, RBC casts) and proteinuria (4.44 g/day). His immunological investigations revealed positive Anti MPO ab (ELISA) with negative ANA/Anti PR3/Anti ds DNA/PLA2R Ab/Anti GBM.
USG abdomen was suggestive of bilateral enlarged kidneys (RK/LK – 13.1/13.7 cm) with 9.5X8.7X13.5 cm (~550ml) hypoechoic collection (hematoma) in Lt renal subcapsular space which was confirmed on CT abdomen and renal angiography (Fig 1). Renal angiogram and DSA was suggestive of large pseudo-aneurysm (20.6 X 14.6 cm) in interpolar region of Lt kidney with active oozing (Fig 2). He underwent coil embolization of pseudoaneurysm and hemostasis was achieved.
Subsequently he was managed with pulse methylprednisolone followed by Rituximab doses, to which he responded favorably. He also underwent renal biopsy later which showed pauci-immune GN.
Presently the hematoma has reduced in size and he is normotensive. His Anti MPO titres have dropped and he is on regular follow up in OPD.
We describe a rare case of GPA with SPH at presentation. Our patient had high titer anti-MPO and renal biopsy findings of crescentic glomerulonephritis. But presence of vascular aneurysm is a rare manifestation of GPA.
1. McKinnom k, Barker K, Ravi R. Case of Spontaneous Bilateral Perinephric Hematomas; 2015
2. Zhang JQ, Fielding JR, Zou KH. Etiology of spontaneous perirenal hemorrhage: a meta-analysis. J Urol. 2002;167
Image and Bar Table 1

Image and Bar Table 2

POS436
Double Trouble: A Rare Case Report of Hemophagocytic Lymphohistiocytosis Secondary to Leptospira
First defined in the year 1939, Hemophagocytic Lymphohistiocytosis (HLH) still evades the diagnosis of physicians thus carrying a high mortality rate. Classified as Primary and Secondary, the latter usually presents in adulthood and is often associated with an underlying condition like infection, malignancy or autoimmune disease driving this hyperactive immune response. Spirochete bacteria Leptospira interrogans, causing Weils disease in humans has been implicated as a rare cause of HLH with only a few cases reported.
We present a case of a 41year old Female who presented with Acute onset Shortness of Breath, Fever and Dry Cough for 4 days. There was associated abdominal distension, pedal Edema, facial puffiness and decreased urine output.
On examination, patient was Febrile with Temperature if 101F. Her Blood investigations revealed Bicytopenia with Leukocytosis, Deranged liver and Kidney functions. Serum Ferritin and Triglycerides levels were markedly raised. Serum Fibrinogen was low. Leptospira Antigen and Igm Antibody was positive. Bone Marrow biopsy revealed Histiocytosis with Evidence of Hemophagocytosis. Her H score was 278. She was diagnosed as iHLH secondary to Leptospira. She responded to High IV MPS with oral maintenance dose along with Broad Spectrum Antibiotics for Leptospira infection.
Image and Bar Table 1

POS437
Multifaceted Crisis in Lupus: Managing Diffuse Alveolar Haemorrhage, Varicella Infection, Refractory Thrombocytopenia, and Subarachnoid Haemorrhage in a Complex Case
Chest X-ray on day-2 showed consolidation of the entire right lung. HRCT chest --consolidation with GGO in multiple lung segments. She was diagnosed with DAH. Treated with pulse doses of methylprednisolone (500 mg daily for 5 days), f/by dexamethasone (1 mg/kg), IVIG and packed RBC and NIV support.
Day 10-she had headache and seizures (GTCS). NCCT brain- subarachnoid haemorrhage. Treated with Nimopdipine and antiepileptic drugs (AED). Persistent thrombocytopenia was managed with platelet transfusions, IVIG. Cyclophosphamide was administered due to Flare up of SLE. The patient improved with resolution of hypoxia, stabilization of Hb and was transitioned to oral prednisolone and supportive care. she was discharged and doing well
Image and Bar Table 1

Image and Bar Table 2

POS438
A Case of Libman-Sacks Endocarditis in a Young Lady with Systemic Lupus Erythematosus and Antiphospholipid Syndrome Presenting as Acute Ischemic Stroke
Further work-up revealed significantly elevated inflammatory markers. Blood cultures were negative, ruling out infective endocarditis. Given the cardiac findings and stroke, an autoimmune etiology was suspected. Serological tests were positive for antinuclear antibodies (ANA) at a titer of 1:1260 with a nuclear pattern, double-stranded DNA, and Anti-Smith antibodies. Additionally, antiphospholipid antibodies, including lupus anticoagulant, anti-beta 2 glycoprotein, and anticardiolipin antibodies (IgG, IgM), were positive, confirming the diagnosis of Libman-Sacks endocarditis (LSE) associated with systemic lupus erythematosus (SLE) and antiphospholipid syndrome (APS).
The patient was initiated on oral prednisolone (20 mg daily), anticoagulation with enoxaparin and warfarin, and disease-modifying therapy with hydroxychloroquine and azathioprine. A follow-up echocardiogram showed resolution of the mitral vegetations and improvement in mitral regurgitation, accompanied by normalization of inflammatory markers.
The pathogenesis of LSE involves immune complex deposition and hypercoagulability, particularly in patients with APS. The vegetations are typically identified via echocardiography, although they can be challenging to detect in some cases. In this patient, the combination of stroke, mitral vegetations, and positive autoimmune serology (particularly antiphospholipid antibodies) was crucial in making the diagnosis.
Management of LSE involves addressing the underlying autoimmune disorder and preventing further thromboembolic events. Immunosuppressive therapy, such as corticosteroids and disease-modifying antirheumatic drugs (DMARDs), is essential for controlling the autoimmune activity, while anticoagulation helps mitigate the risk of further embolization.
Image and Bar Table 1

POS439
Squats! The Ups and Downs of Being A Muscle Man - A Case Report
POS440
Post Intravesical BCG Reactive Arthritis: Clinical Features and Outcomes
Image and Bar Table 1

Image and Bar Table 2

POS441
What Lies Beneath The Eyes.. A Case of Takayasu Ophthalmopathy at Onset
Kunal Kishore,
Fundus examination revealed multiple microaneurysms in the mid-peripheral retina across all quadrants, along with a wreath-like arteriovenous anastomosis near the left optic disc and FFA revealed multiple 360-degree peripheral capillary nonperfusion areas in both eyes, microaneurysms in the mid-periphery, and leakage from type 3 anastomosis in the left eye (Figure 1).
CT angiography (Fig 2) revealed diffuse mural thickening of the aorta and its branches, with near total occlusion of CCA, ICA, ECA, subclavian artery, and left vertebral artery. His lab evaluation revealed high CRP (26 mg/l) and negative ANA/Anti -PR3/ Anti -MPO. His WB PET scan didn’t reveal any active FDG uptake in aorta and its branches
He was diagnosed with Takayasu’s arteritis (TAK) with stage 4 Takayasu’s retinopathy (TR). He was managed with pulse methylprednisolone, followed by oral steroids and azathioprine. He also underwent pan-retinal photocoagulation in both eyes, along with an intravitreal injection of ranibizumab in the left eye.
Image and Bar Table 1

Image and Bar Table 2

POS442
Acute Necrotizing Pancreatitis and the Unmasking of ANCA Vasculitis: A Case of Coexistent Relapsing Polychondritis
Image and Bar Table 1

Image and Bar Table 2

POS443
Systemic Lupus Erythematosus with Acquired Hemophilia A in A Young Female: A Case Report from Nepal
Image and Bar Table 1

POS444
Tofacitinib and Tuberculosis Reactivation: A Retrospective Study on Safety and Adverse Effects
Image and Bar Table 1
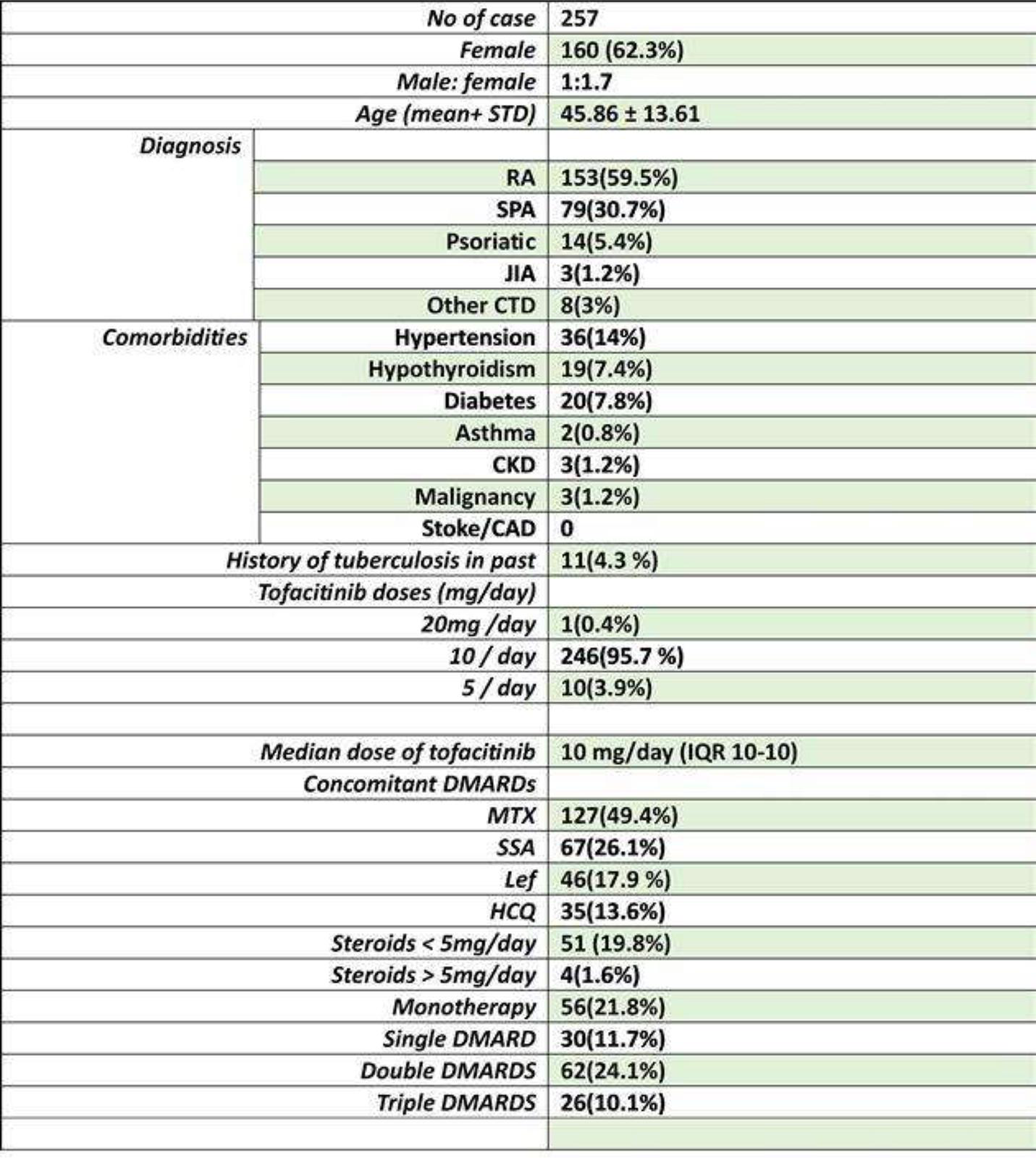
Image and Bar Table 2

POS445
Stabilisation of Myelodysplastic Syndrome in Vexas Syndrome With Tofacitinib: A Case Report
Image and Bar Table 1

Image and Bar Table 2
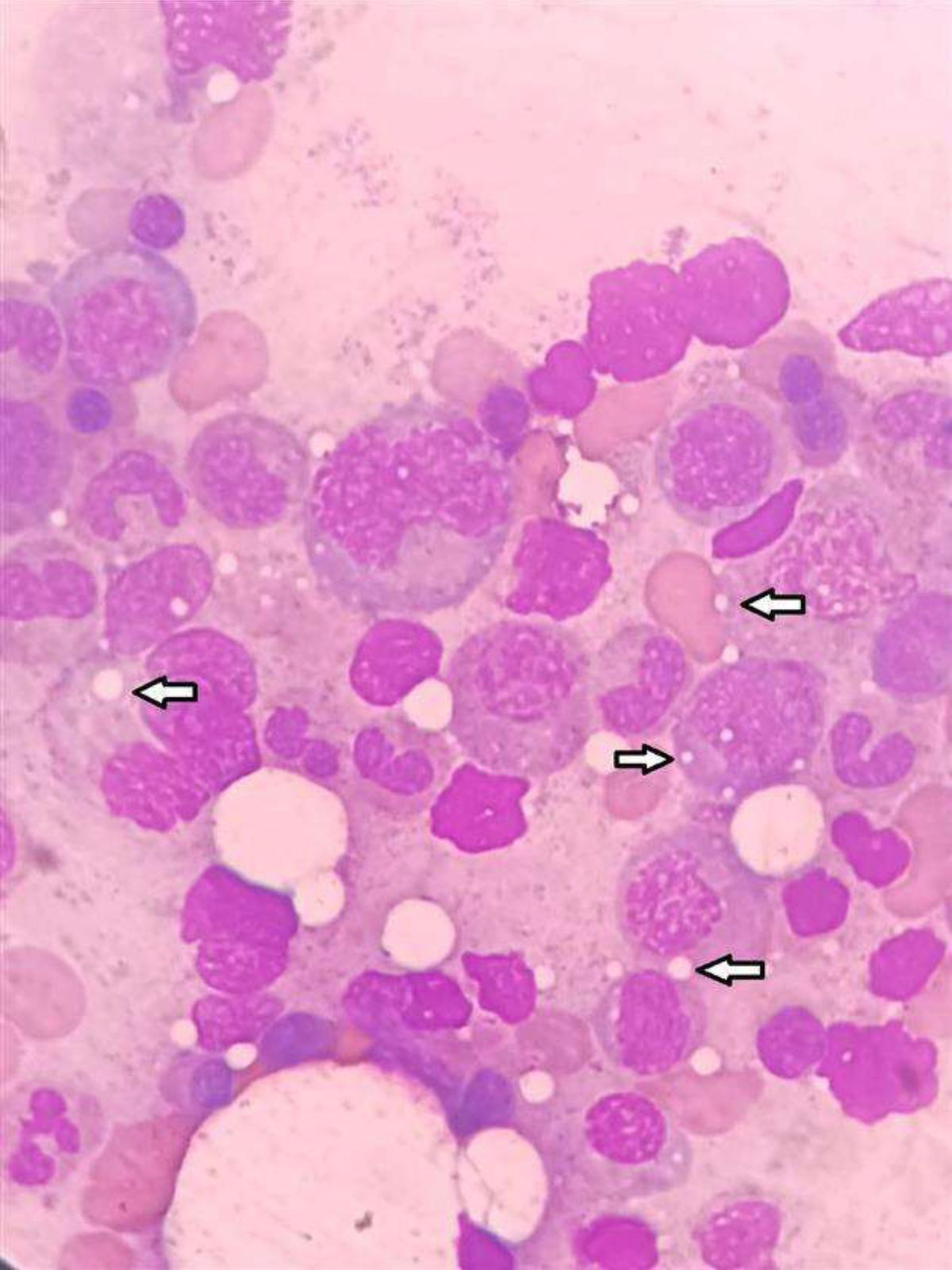
POS446
“Orbital Inflammation Under the Lens: Key Findings From A Case Series”
Compared to other series where dacryoadenitis/ myositis were the most prominent locations (1), non specific soft tissue involvement was the most common in our series
Among these individuals, 3 had IgG4-related disease (image 1), 3 had sarcoidosis, 1 with giant cell arteritis, and 6 with idiopathic orbital inflammation. Notably, one patient with IgG4 disease also presented with concurrent mucormycosis, while two patients were diagnosed with tuberculosis. 3 patients (18%) had bilateral disease.
The mean age of the study cohort was 33 years, with a female-to-male ratio of 4:1. All patients underwent imaging studies (CT and/or MRI of the orbit) and biopsy of the lesions for definitive diagnosis.
Notably, 11/13 patients (84%) with inflammatory etiology achieved complete remission at one-year follow-up with MRI showing resolution, although two patients necessitated escalation of treatment to rituximab due to severe disease.
1. Ronquillo Y, Zeppieri M, Patel BC. Nonspecific Orbital Inflammation. [Updated 2024 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
Image and Bar Table 1

Image and Bar Table 2

POS447
Takayasu Arteritis Masquerading as Seronegative Arthritis: A Rare Presentation
1. Kwon OC, Lee SW, Park YB, Oh JS, Lee SH, Hong S, Lee CK, Yoo B, Kim YG. Extravascular manifestations of Takayasu arteritis: focusing on the features shared with spondyloarthritis. Arthritis research & therapy. 2018 Dec;20:1-7.
2. Tomelleri A, Campochiaro C, Sartorelli S, Bandini V, Baldissera E, Dagna L. 273. TAKAYASU’S ARTERITIS: BEYOND THE VESSELS. Rheumatology. 2019 Mar 1;58 (Supplement_2):kez062-047.
Image and Bar Table 1

POS448
Inflammation Down Under
Image and Bar Table 1

POS449
The Mighty Mite
Patient was strictly advised to adhere to lowered doses of prednisolone and treated with topical ivermectin. This showed no response and then patient was switched to oral metronidazole 400 mg bd for 14 days. After a month, the itching and irritation had subsided however the erythematous macular rash of lupus and palatal ulcers had resurfaced. Patient is currently following up with 5 mg of prednisolone and Mycophenolate 1500 mg a day. The papules associated with rash have diminished but lupus rash persists.
In patients with cutaneous lupus, they may be considered as etiology in severe, difficult to treat or unexplained cases.
Image and Bar Table 1

Image and Bar Table 2
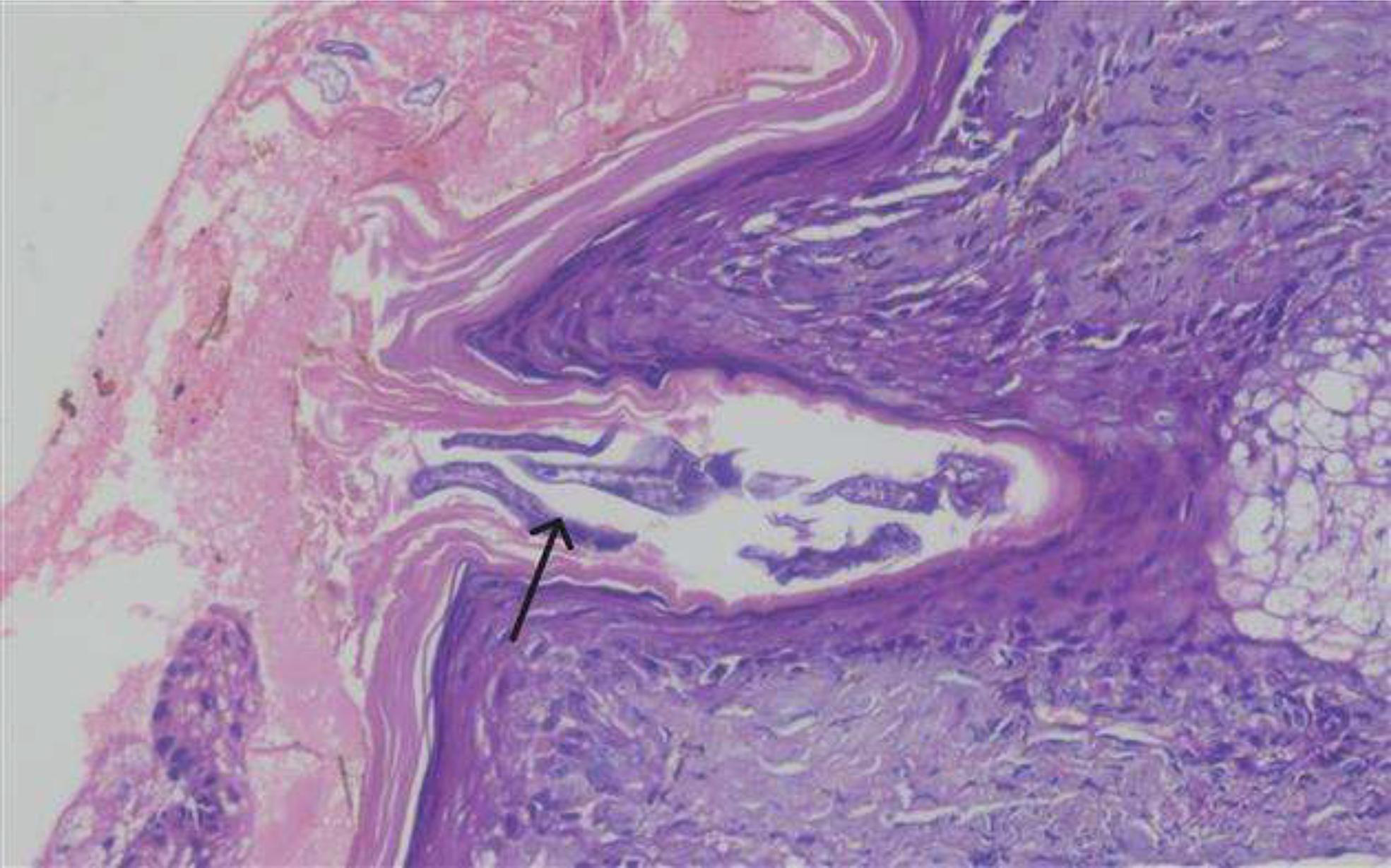
POS450
Obesity in Eyes of Beholder
POS451
Prevalence and Clinical Implications of Hyperuricemia in Systemic Sclerosis
POS452
A Challenging Case of Overlap Syndrome: SSc-AAV
POS453
Unveiling the Uncommon: Aneurysm of Mitral-Aortic Intervalvar Fibrosa as A Rare Manifestation of Takayasu Arteritis
Takayasu arteritis (TAK) is large vessel vasculitis characterized by granulomatous inflammation of mainly aorta and its branches manifesting with diverse clinical features often in young females.
Takayasu arteritis can have varied cardiac manifestations, most of which are life threatening if left untreated. Here we present one such case of severe aortic regurgitation with a rare cardiac manifestation of Takayasu arteritis.
A 29-year-old female presented with history of palpitation and exertional dyspnoea for two weeks. She was evaluated elsewhere and was diagnosed to have severe anaemia and treated for the same. The TT echo showed aneurysmal sac in left atrium communicating with left ventricular outflow tract below the level of aortic valve, compressing left atrium. Colour Doppler evaluation showed flow into the cavity during systole. Also, we noted non coapting aortic leaflets with severe aortic regurgitation with dilated ascending aorta. Turbulent flow was noted in left carotid, left subclavian, coeliac and superior mesenteric arteries. Biventricular function was normal. 3D-TEE showed sub aortic aneurysm extending into and compressing left atrium, with severe aortic regurgitation, mild MR and normal left ventricular systolic function. Cardiac MRI with MR aortogram showed similar findings along with mild circumferential wall thickening with calcification extending from ascending aorta to bifurcation. Left common carotid artery ostial stenosis for a length of 5mm followed by occlusion, diffuse moderate stenosis in right common carotid artery, diffuse moderate stenosis in bilateral subclavian arteries, fusiform dilatation of distal abdominal aorta before bifurcation-features suggestive of Takayasu arteritis (Numano type V). Inflammatory markers were elevated. she was started on steroids and DMARDS and was planned for surgery, resection of aneurysmal sac and aortic valve repair, however 3 months into treatment she developed hemoptysis and underwent resection of aneurysmal sac with aortic valve repair and patient presently on DMARD and steroids and is doing good with no relapse of symptoms.
A TEE showing Aneurysmal sac protruding into left atrium communicating with LVOT.

POS454
Pancreatitis, Panniculitis, and Painful Polyarthritis: A Triple Threat in Tandem
The patient exhibited panniculitis, with inflamed nodules over the legs, suggestive of subcutaneous fat necrosis. MRI and CT confirmed pleural and pericardial effusions, as well as necrosis in the pancreas.
CBC showed leucocytosis and thrombocytosis, and mild transaminitis. Renal function and urine analysis were normal. Autoimmune markers, including ANA, ANCA (PR3 and MPO), serum ACE, and IgG4, were negative, and HLA-B27 was also negative.
Given the presentation, differential diagnoses like spondyloarthropathy, sarcoidosis, polyarteritis nodosa, and tuberculosis were ruled out. A diagnosis of Pancreatitis, Panniculitis, and Polyarthritis (PPP) syndrome was made.
PPP syndrome is characterized by fat necrosis from pancreatic enzyme leakage, causing panniculitis and polyarthritis. Synovial fluid aspiration from the left knee (60 cc) revealed birefringent lipid crystals with a Maltese cross pattern, confirming PPP syndrome. The presence of these crystals in the synovial fluid highlights the systemic inflammatory response.
PPP syndrome is rare, with only about 70 cases reported by 2020. Early recognition and treatment, including corticosteroids and supportive care, are essential for preventing complications.
1. Pichler H, Stumpner T, Schiller D, Bischofreiter M, Ortmaier R. Pancreatitis, panniculitis and polyarthritis syndrome: A case report. World J Clin Cases. 2023;11 (18):4412-4418.
2. Kashyap S, Shanker V, Kumari S, et al. Panniculitis-polyarthritis-pancreatitis syndrome. Indian J Dermatol Venereol Leprol. 2014;80:352-354. doi:10.4103/0378-6323.132244.
Left ankle and left knee (post-aspiration) swollen and erythematous nodule over the left shin.

Synovial fluid aspirate showing birefringent Maltese cross-like appearance of lipid crystals under polarized microscopy.

POS455
Fever in the Elderly: Unmasking Giant Cell Arteritis as A Hidden Culprit
All patients showed significantly elevated ESR and CRP levels, suggesting inflammation. After ruling out common causes of fever, vasculitis was considered. Temporal artery doppler revealed a halo sign in three patients, a key feature of Giant Cell Arteritis (GCA). PET CT in two patients showed extracranial large vessel involvement.
Temporal artery biopsies confirmed GCA in three patients, revealing inflammation, fibrosis, and calcification. All were treated with corticosteroids and methotrexate, and two patients received methylprednisolone pulses due to seizures and optic involvement. While all patients showed significant improvement, the one with vision loss did not regain sight in one eye due to delayed treatment.
This series highlights the need to consider GCA in elderly patients with fever and elevated inflammatory markers, particularly when accompanied by headache or visual disturbances. Early diagnosis and treatment are crucial to prevent irreversible damage, such as vision loss.
Image and Bar Table 1
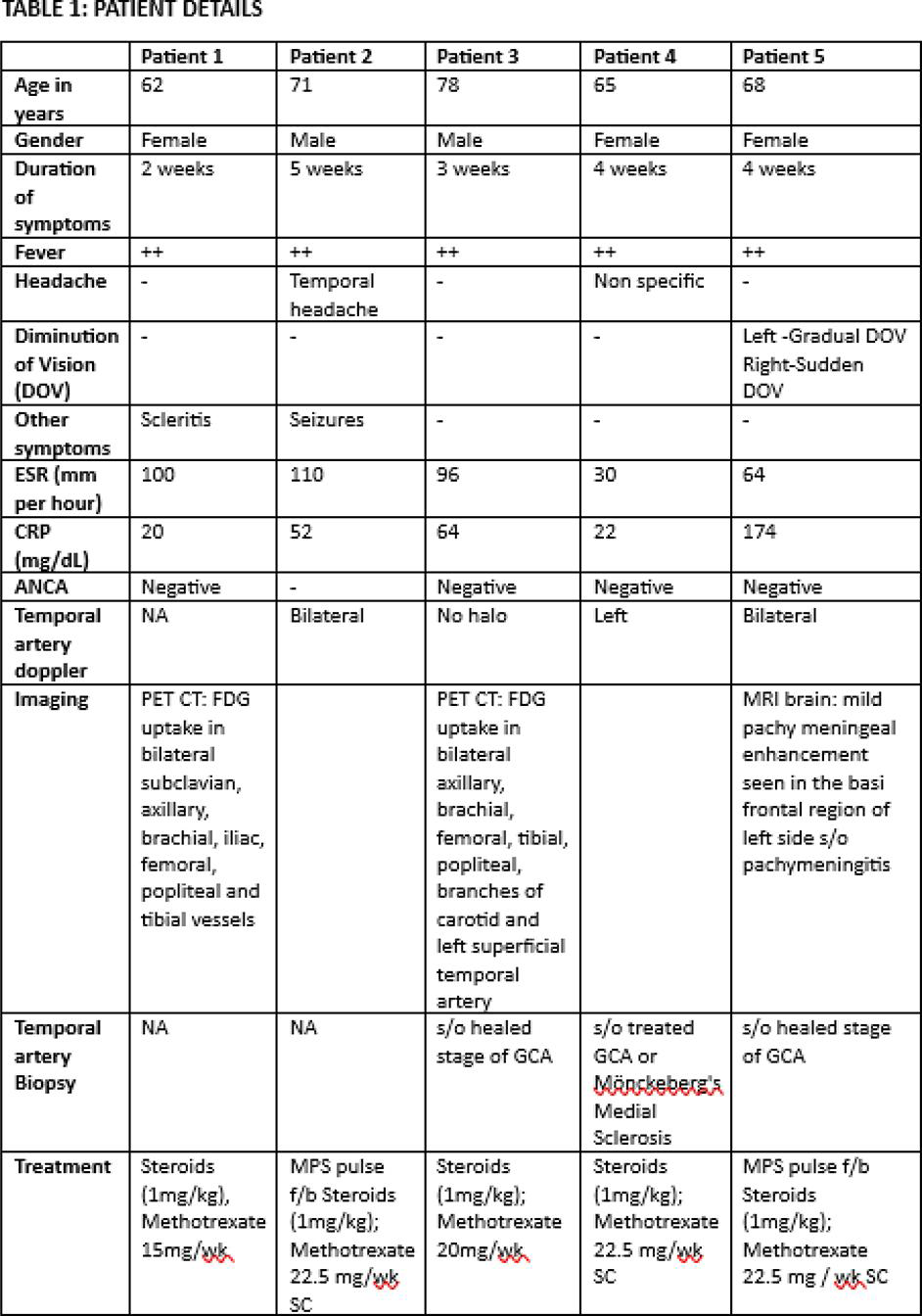
POS456
Stroke in Young with Multiple Aneurysms: Unraveling The Diagnostic Challenge
On follow-up, her neurological deficits worsened with the development of new-onset nystagmus, 7th cranial nerve, lower cranial nerve palsies and features suggestive of bilateral cerebellar involvement. Blood pressure asymmetry was noted between the upper limbs. Left carotid, brachial and radial pulses were feeble. Repeat imaging revealed acute and chronic cerebral infarcts, multiple saccular aneurysms affecting cerebral and abdominal arteries (Fig 1) and mild circumferential wall thickening of the abdominal aorta. Routine lab investigations were insignificant except for elevated CRP (15.2mg/L) (Table 1)
This multifaceted presentation, including young stroke, multiple large and medium vessel saccular aneurysms, and elevated inflammatory markers, led to a differential diagnoses encompassing Takayasu arteritis, Antiphospholipid syndrome, Polyarteritis nodosa, Deficiency of adenosine deaminase 2 syndrome (DADA2), Fibromuscular dysplasia (FMD), and Ehlers-Danlos syndrome (EDS). Whole exome sequencing identified a homozygous mutation in the ADA2 gene, confirming the diagnosis of DADA2 syndrome.
Image and Bar Table 1

Image and Bar Table 2

POS457
An Intriguing Case of Overlapping IgG4 and Rosai Dorfman Disease
CBC, Renal Function, Liver Function Tests: Normal ESR: 20 mm/hr CRP: Negative IgG4: 40 mg/dL (Normal range < 40 mg/dL) ANCA (IF): Negative
Imaging and Histopathological Findings:
Figure 1: MRI revealed a mass in the left parapharyngeal space encasing the left internal carotid artery (without narrowing) and compressing the proximal internal jugular vein without thrombosis. Figure 2: An additional lesion in the right paramedian upper lip, involving the inferior part of the right maxillary sinus, showed erosion, sclerotic changes, and remodeling of the sinus floor. Histopathology: Findings were suggestive of IgG4-related disease. Biopsy results indicated the presence of emperipolesis with IgG4-positive cells ranging from 10% to 50% per high-power field (HPF) and an IgG4/IgG ratio of 10% to 20%. Immunohistochemistry demonstrated S100+ and OCT2+ staining
1. Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Blood 2018; 131 (26): 2877–2890. doi:
Image and Bar Table 1

Image and Bar Table 2

POS458
Wolf in Sheep’s Clothing - Vasculitis Presented as Avascular Necrosis of Hip
Preceding steroid exposure did raise the possibility of glucocorticoid induced AVN but it was short term low steroid. He did not has any features of SLE.
A possible association between cutaneous vasculitis & AVN was considered but considering the rarity of this association, other causes of AVN were considered more likely. APLA profile and thrombophilia profile were normal.
Ulcer biopsy was suggestive of LCV & serological work up was non contributory. Due to raised diastolic BP & lower limb ulcers, Polyarteritis nodosa (PAN) was also considered. He was seronegative for Hepatitis B, DADA2 was considered. Immunosuppressants started & he responded to treatment.