
Abstract
Objectives:
Ankylosing spondylitis (AS) is an axial skeleton-related auto-inflammatory arthritis. Interleukin 6 (IL-6) and its receptor (IL-6R) play a role in the etiopathology of AS. The recent genome-wide association studies (GWASs) revealed that rs4129267; an intrinsic variant of IL6-R is associated with the risk of AS. We aimed to study the rs4129267 IL6R variant in Iranian AS patients and the correlation of this variant with the soluble interleukin-6 receptor (sIL-6R) serum level.
Materials and Methods:
In this case-control study, we genotyped rs4129267 IL6-R variant in extracted DNA from 498 AS patients and 495 matched healthy controls by Amplification-Refractory Mutation System Polymerase Chain Reaction (ARMS-PCR). The serum level of sIL-6R and IL-6 was also analysed in 39 controls and 42 AS patients by the ELISA method. The correlation between rs4129267 IL-6R variants and patients’ clinical manifestations and sIL-6R level was also investigated.
Results:
In comparison to the AS individuals, C allele were significantly less prevalent in the healthy control group (OR = 1.23 [1.01 –1.48], P value = .034). Patients had significantly elevated levels of IL-6 serum levels. There was a significant correlation between the presence of the rs4129267 T allele and increased sIL-6R level.
Conclusions:
Our study confirmed the significant association between the rs4129267 T variant and the protection against AS disease susceptibility. Increased IL-6 level and reduced frequency of sIL-6R rs4129267 T allele in patients which contributes to reduced sIL-6R serum level, highlights the significant role of IL-6 signalling pathway in AS pathogenesis.
Introduction
Ankylosing spondylitis (AS) is an inflammatory rheumatic condition that often affects the sacroiliac joints, spine, and hip joints. Typically, AS is characterised by spondylitis and sacroiliitis accompanied by severe joint pain, stiffness, and functional disability in damaged joints. In the severe form of the disease, persistent inflammation of these areas causes osteogenesis in intervertebral discs and fusion of the vertebrae together. The result of these changes will be a loss of movement and flexibility in these parts. 1 AS is more common in young people between the ages of 16 and 36 and usually lasts a lifetime. Although it’s less prevalent and the symptoms are milder among women, the involvement of joints other than the spine is more likely in women than in men. In 5% of patients with AS, the disease begins in childhood. 2 A study of the Iranian population shows that the disease is 3 to 1 more common in men. Besides, the average age of onset of symptoms is 24.7 years and the incidence of the disease in the south of Iran was reported approximately 8.03 per 100,000 people. 3
While the cause of AS is unknown, studies have shown the contribution of both genetic and environmental factors in the development of AS. There is a strong genetic relationship between the incidence of the disease and the presence of human leukocyte antigen (HLA)-B27 polymorphisms. About 90% of patients are HLA-B27 positive, nonetheless only about 5% of respective patients develop the disease.4,5 Genome-wide association studies (GWAS) suggested that genetic variants in both HLA and non-HLA genes are associated with susceptibility to AS and its progression. 6
Genetic studies reveal that several variants in key genes of the pro-inflammatory IL-23/IL-17 pathway are associated with AS disease and its pathogenesis.6,7 Interleukin (IL)-6, an important cytokine related to the IL-23 pathway, is involved in the pathogenesis of AS. IL-6 pro-inflammatory properties are mediated by binding to the IL-6 receptor (IL-6R). IL-6R has two forms by alternative splicing 8 : (a) The membrane-bound form (mIL-6R) that is expressed in neutrophils, monocytes, CD4+ T cells, B cells, and hepatocytes; (b) The soluble form (sIL-6R) circulating in body fluids which are mostly generated by proteolysis from the mIL-6R. The IL-6/sIL-6R complex could be a mediator for the IL-6 signalling pathway in non-expressing mIL-6R cells by binding to gp130 transmembrane glycoprotein.9,10
Many studies have reported elevated serum levels of IL-6 in AS patients and its association with the severity of patients’ clinical manifestations.11,12 Although targeting IL-6 signalling in AS patients by tocilizumab (an IL-6R antagonist) has been repeatedly investigated, the results were inconsistent and some studies demonstrated tocilizumab as a non-efficient treatment.13,14 The differences in clinical responses to tocilizumab could be due to variations in the IL-6R gene.
The rs4129267 single nucleotide polymorphism (SNP) of the IL-6R gene is a candidate risk variant for AS and consistently, GWAS studies revealed that the T allele of this SNP is significantly associated with increased susceptibility to AS progression,15-17 which is a non-synonymous intronic variant that has a gene-regulatory effect. 18 This non-coding variant had an impact on sIL-6R availability and serum levels. 19 In previous studies, rs4129267 showed a strong association with AS risk in a European cohort including European, South Asian, and Latinx populations 19 and a Chinese cohort. 20 Moreover, a significant association with asthma is reported, while a negative association with AS. 21
In this study, we aimed to examine the association of the rs4129267 variant of the IL-6R gene, as a susceptible loci, with the risk of AS in the Iranian population, to check the reproducibility of the results in a population from the Middle East and investigate the correlation between rs4129267 variants and sIL-6R serum level.
Materials and Methods
Participants
A total of 498 AS patients (388 men and 110 women, mean age: 37.5 years) were referred to the rheumatology clinic of Shariati Hospital of Tehran University of Medical Sciences between November 2013 and June 2015 based on modified New York criteria 22 plus 495 ethnicity-, age- and sex-matched healthy controls (mean age: 36.8 years) without any familial history of autoimmune diseases participated in this study. Clinical and demographical characteristics of AS patients and healthy individuals were gathered at the time of sample collection in a questionnaire (Table 1). Informed consent was taken from all participants before enrollment.
Baseline Characteristics of AS Patients and Healthy Controls.
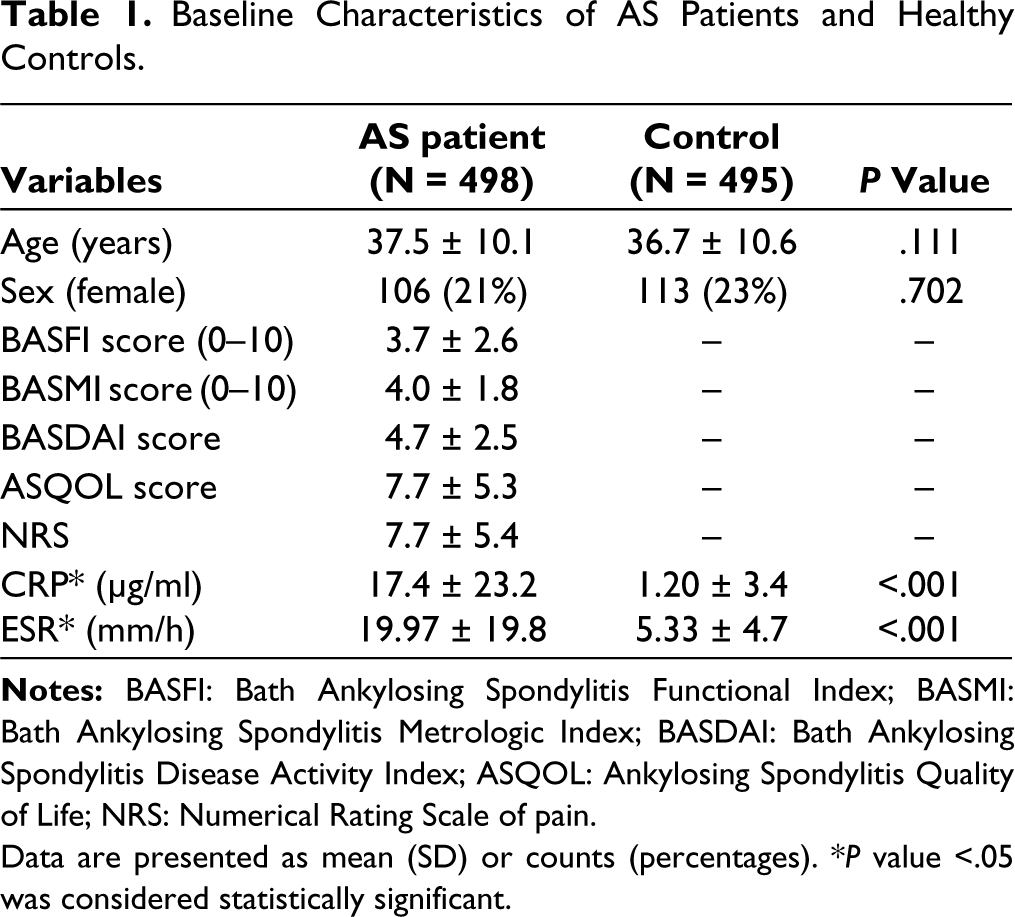
Data are presented as mean (SD) or counts (percentages). *P value <.05 was considered statistically significant.
DNA Extraction and Genotyping
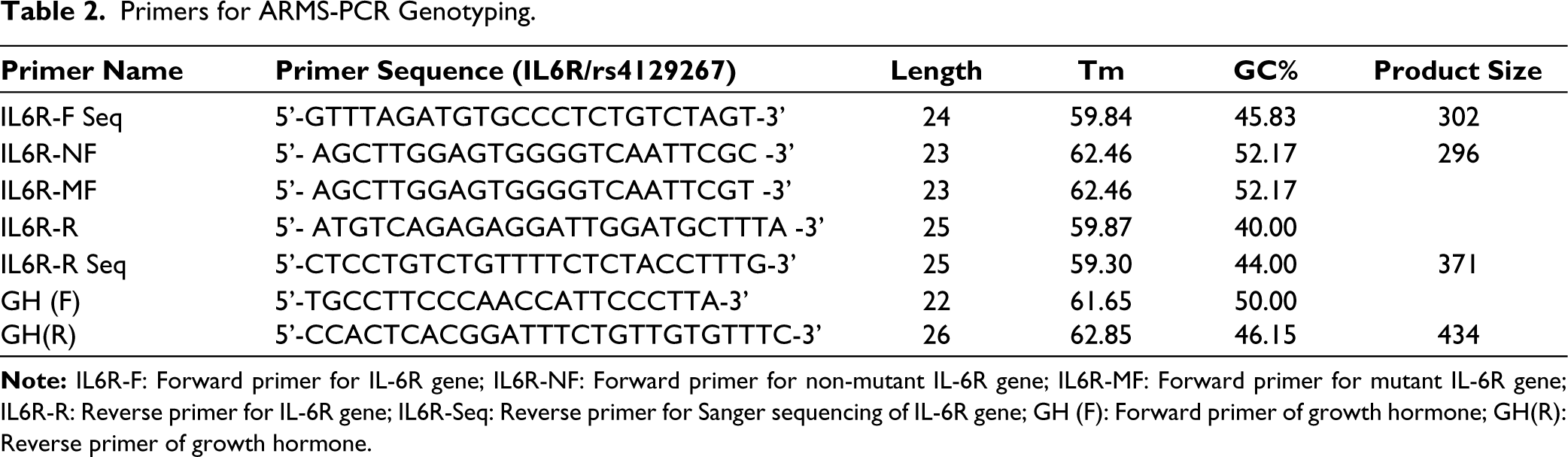
Whole DNA was extracted from 4 mL venous blood samples by phenol-chloroform method. 23 The optical density values were used to evaluate the concentration and purity of the extracted DNA (NanoDrop 2000C). Subsequently, it was stored at -20°C. The rs4129267 is located on position 154453788 (intron variant) of chromosome 1 and we employed the ARMS-PCR technique for its genotyping. To design the assay, three primers were used: two forward primers (one for the mutant and one for the wild-type) and a single reverse primer common to both, which were created using web-based allele-specific PCR (WASP). The ARMS-PCR was carried out in a reaction mixture with a total volume of 15 µL, which included 1.5 µL of genomic DNA (150 ng), 7.1 µL of distilled water, 0.25 µL of 10 mM dNTP mix, 1.2 µL of each specific primer at a concentration of 10 pmol/µL, 2.5 µL of 10X PCR buffer, 0.75 µL of 1.5 mM MgCl2, and 0.3 µL of Taq DNA polymerase. Additionally, two internal control primers for growth hormone (GH) were added at a volume of 0.1 µL each (with a concentration of 10 pmol/µL) to every reaction. The PCR cycling conditions were consisting of the initial denaturation (94°C, 3 min) followed by 40 cycles of 94°C for 30 s, 62°C for 30 s, 72°C for 30 s, final extension at 72°C for 10 min and eventually 10 min of storage at 4°C. Amplified DNA products were separated on a 2% agarose gel, stained with a DNA-safe dye, and visualised using a UV transilluminator. To verify the accuracy of the amplification, Sanger sequencing was performed on the PCR products. The sequence of primers for ARMS-PCR genotyping and Sanger sequencing is listed in Table 2.
Primers for ARMS-PCR Genotyping.
Serum Protein Measurements
Serum was isolated from 10 ml blood samples of 42 AS patients and 39 healthy controls by centrifuging at 4,500 rpm for 7 minutes. The ELISA kits (R&D Systems, Minneapolis, MN, USA) were utilised to measure sIL-6R and IL-6 levels based on the manufacturer’s procedures.
Statistical Analysis
Data were described as mean ± SD or n (%). We used the Shapiro-Wilks test to assess the normality distribution for continuous variables. Association between categorical variables was assessed by Chi-square test, odds ratio (OR), and 95% confidence interval (CI). The genotype distributions of SNP were examined for statistical deviation from Hardy-Weinberg equilibrium. We used the Kruskal–Wallis test and one-way ANOVA to compare the means of continuous variables among groups; Also, the Bonferroni post hoc test was used for pairwise comparison if needed. We performed this statistical analysis using SPSS software (version 27.0, IBM SPSS Inc., USA), and a P value less than .05 was considered statistically significant.
Results
Clinical Features and Inflammatory Markers
Clinical features of AS patients and healthy individuals are presented in Table 1. There is no notable difference between patients and healthy individuals regarding their age and sex (P = .111 and P = .702, respectively). The AS group had significantly elevated levels of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) (P <.001 for all) as expected.
The rs4129267 Genotyping
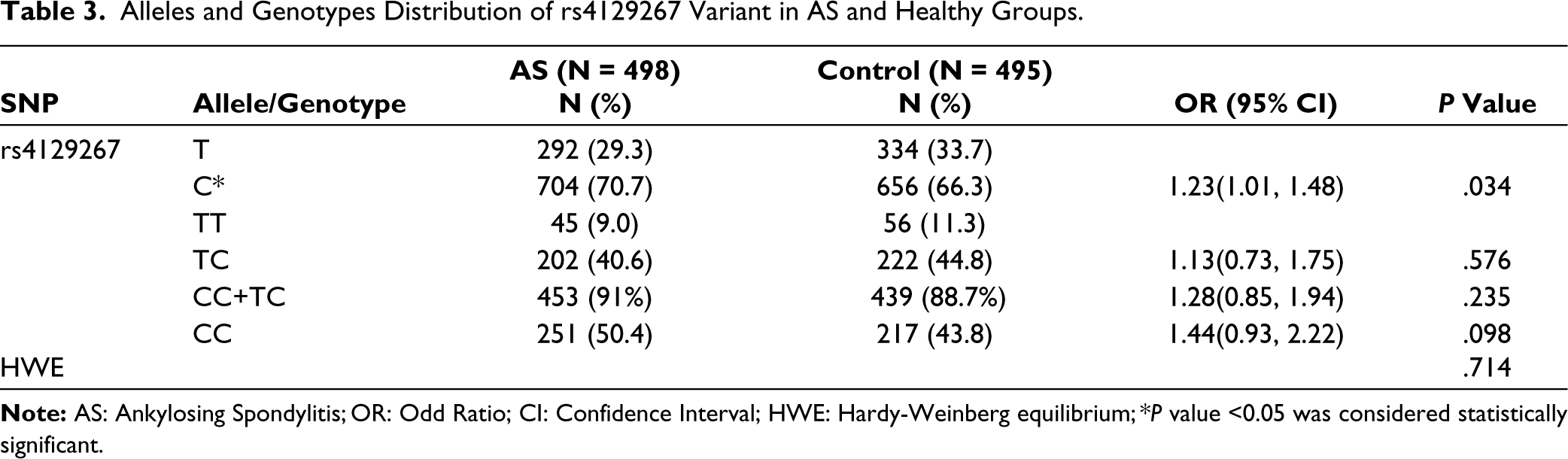
Table 3 displays the associations between rs4129267 alleles and genotype frequency with AS susceptibility. In the healthy group, there was no significant deviation from the Hardy-Weinberg Equilibrium for rs4129267 genotypes distribution (P = .714). According to our results, the CC genotype is significantly more common in the AS group (CC vs. TT+TC P = .038), and the C allele is significantly increased in AS patients [P = .034, OR (95% CI) = 1.23 (01.01–1.48)] (Data not shown).
Alleles and Genotypes Distribution of rs4129267 Variant in AS and Healthy Groups.
IL-6 and sIL-6R Serum Level
We also assessed the level of IL-6 and sIL-6R in serum samples of 39 healthy and 42 randomly selected patients. Although IL-6 level was significantly upregulated in AS patients (P <.001) there was no statistically significant difference in the level of sIL-6R between the two groups (P = .182) (Table 4).
IL-6 Cytokine and sIL-6R Levels in AS Patients and Healthy Controls.

Association of rs4129267 Genotypes and Clinical Features
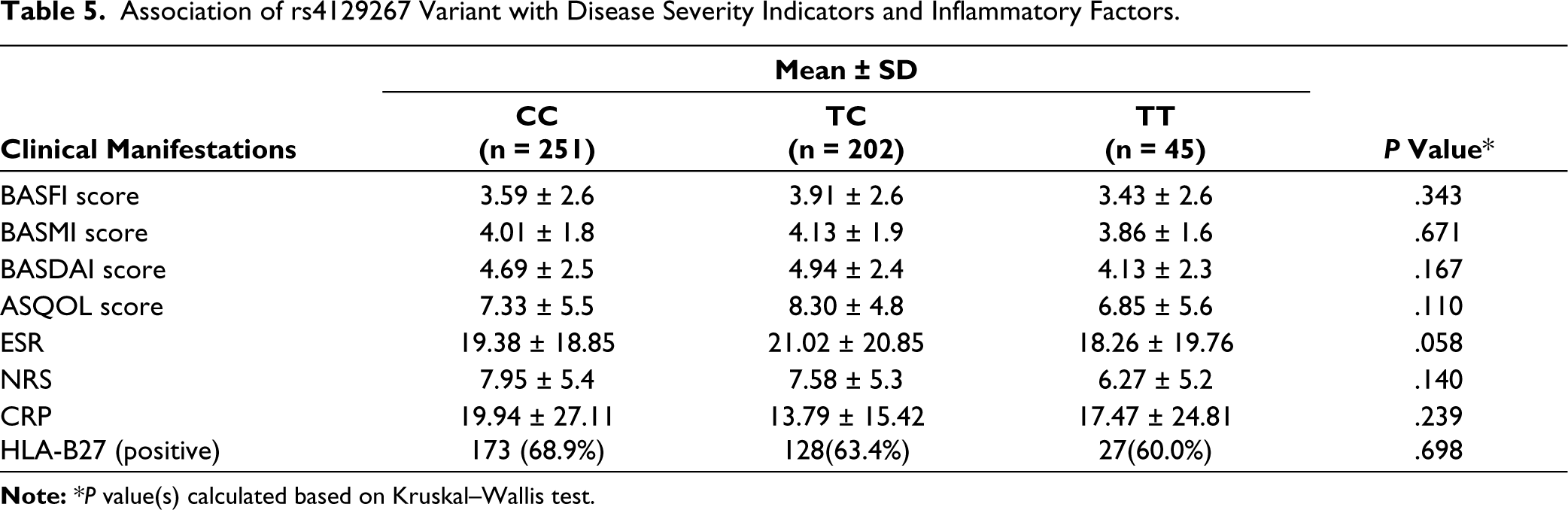
The association between rs4129267 genotypes with HLA-B27 positivity and the score of patients’ clinical features by Bath Ankylosing Spondylitis Metrologic Index (BASMI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Ankylosing Spondylitis Quality of Life (ASQOL), Numerical Rating Scale of pain (NRS), ESR and CRP were analysed and are shown in Table 5. No significant association between the mentioned clinical indices with different genotypes of rs4129267 was observed.
Association of rs4129267 Variant with Disease Severity Indicators and Inflammatory Factors.
Association of CRP Levels with IL-6 and sIL-6R in Different rs4129267 Genotypes
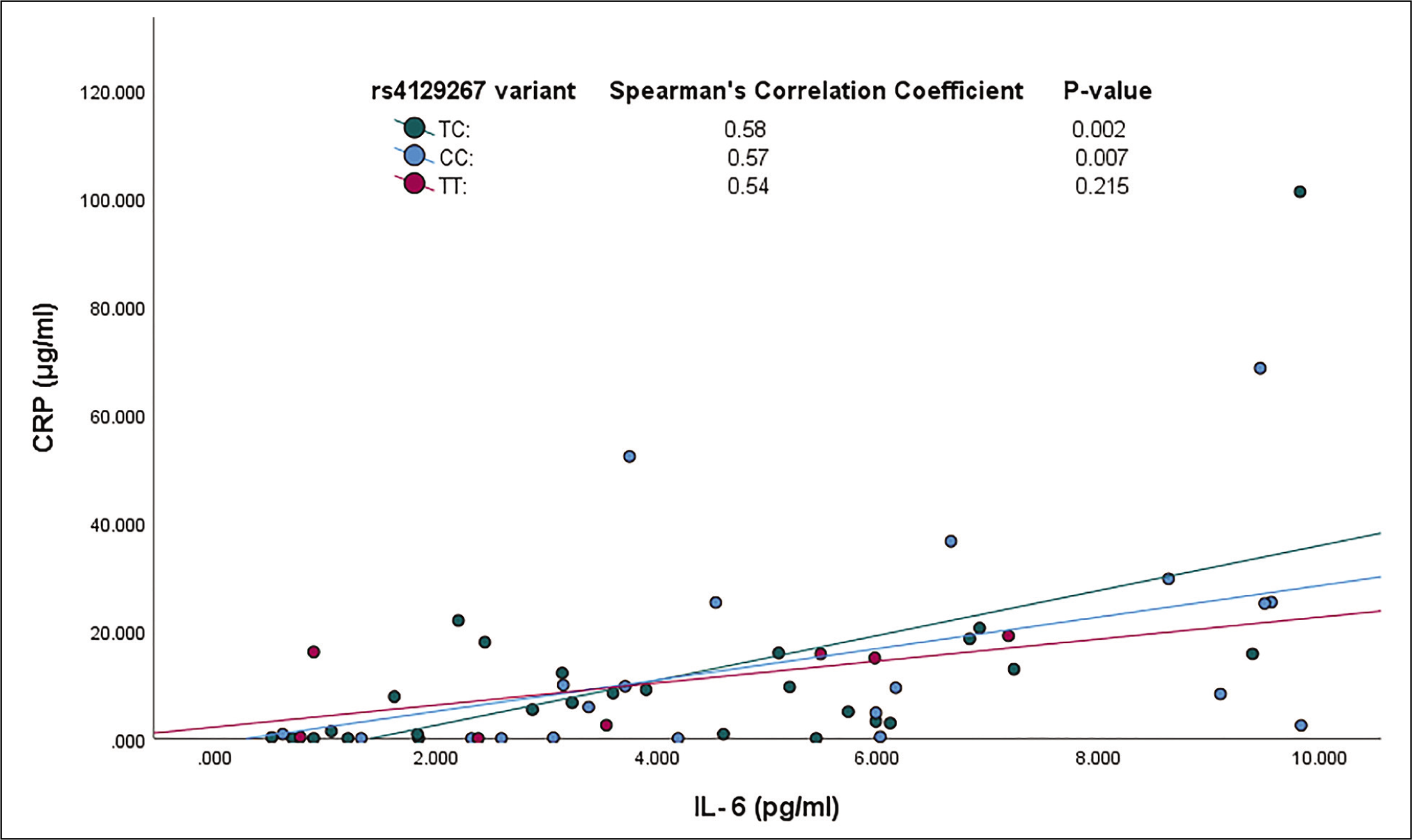
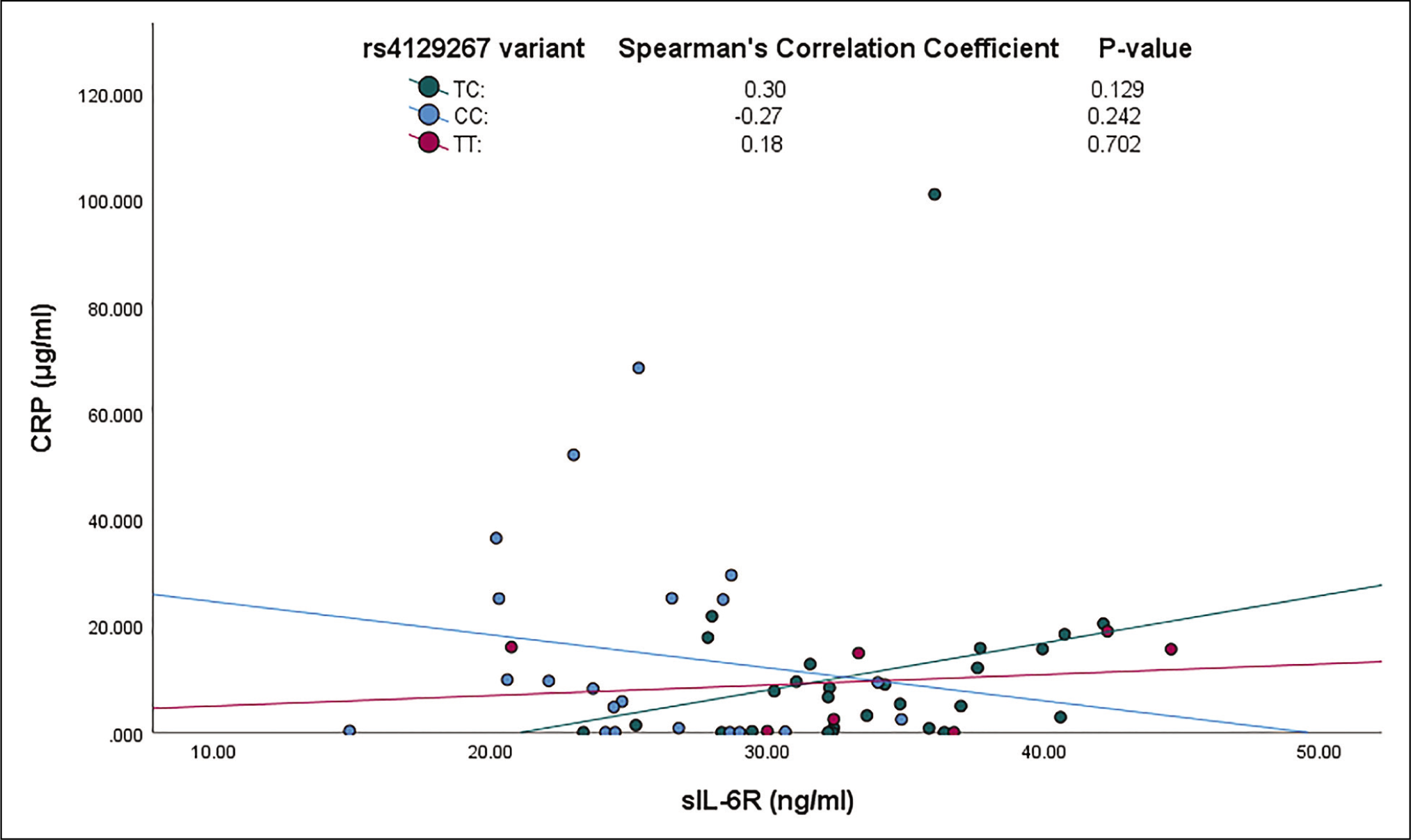
Figure 1 shows that, unlike TT, levels of CRP and IL-6 are significantly correlated (P <.05) in patients with CC and TC genotypes. However, no significant association was observed between CRP and sIL-6R levels in different genotypes (Figure 2).
The Association of CRP and IL-6 Levels Divided by Different Genotypes.
The Association of CRP and sIL-6R Levels Divided by Different Genotypes.
Association of rs4129267 Genotypes with sIL-6R and IL-6 Level
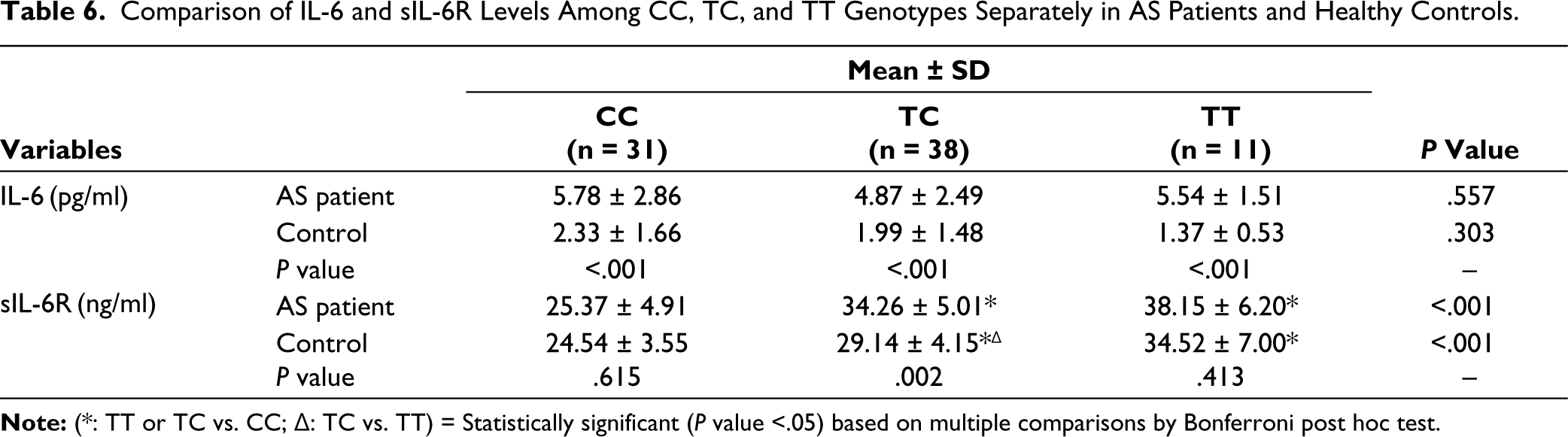
Later on, we investigated the association between rs4129267 variants and sIL-6R level in participants. The findings indicated a significant correlation between the rs4129267 variants and the levels of sIL-6R in the serum. In particular, those possessing the TT genotype were observed to have the highest levels of sIL-6R, whereas individuals with the CC genotype exhibited the lowest levels. Furthermore, there was a noteworthy decrease in the serum levels of sIL-6R among AS patients and control subjects who have the TC genotype compared with TT.
Conversely, while the genotype did not display a significant link to the serum levels of IL-6, AS patients, regardless of their genotype, had a significantly higher concentration of IL-6 in their serum compared to the control group (Table 6).
Comparison of IL-6 and sIL-6R Levels Among CC, TC, and TT Genotypes Separately in AS Patients and Healthy Controls.
Discussion
Several GWASs reveal that IL-23 pathway-related genes are associated with susceptibility to AS disease. 24 IL-6R is an effector signalling molecule in the IL-23 pathway25,26 and implicates in the pathogenesis and auto-inflammatory responses of AS. 5 Association of IL-6R rs4129267 intronic variant with AS was previously reported. 17 Here, we studied the association of rs4129267 with the susceptibility to AS in the Iranian population for the first time and our findings highlighted the role of the IL-6R gene in AS disease.
The IL-6R variant rs4129267 is described as a biomarker for inflammation in a GWAS study in the Italian population. 27 Ferreira et al. also reported the association of rs4129267 with the susceptibility of asthma in an Australian population and found that T allele increases the risk of asthma. 18 Cortes et al. studied 10470 AS patients and 12338 controls, of European, South Asian, and Latin American origin. They found that the rs4129267 C allele is significantly associated with an elevated risk of AS in individuals of European ancestry individuals, while the T allele plays a protective role. Besides they observed that this variant is associated with significantly higher concentrations of CRP in the TT genotype than CC, which highlights its impact on the severity and clinical features of AS. 17 Furthermore, Ruan et al. found the frequency of TT genotype rising significantly in the AS group of the Chinese population from Wuhan. Additionally, in line with clinical characteristics, significantly elevated BASFI scores were observed in the TT genotype compared to CC. Apart from the genotype, they found out that the rs4129267 T allele could also serve as a prognostic factor for AS pathogenesis because of its influence on the worsening of treatment response during the follow-up. 15 In our study, the frequency of the T allele is significantly reduced in the AS group, and consistent with Cortes et al., our results showed that the T allele has a protective role against AS incidence in the Iranian population.
Previously it was found that rs4129267 is a regulatory variant and has an impact on the level of sIL-6R. 17 The study by Melzer et al. showed sIL-6R serum concentration to be higher in people with rs4129267 TT genotype than other genotypes and each T allele increases 1.4-fold the serum concentration of sIL-6R. 28 Consistent with previous reports, we showed a strong correlation between increased serum concentration of sIL-6R and rs4129267 TT genotype and found that each T allele increases the receptor serum concentration. Although the small sample size for this measurement was one of our limitations in this study; considerable significant results were achieved that could be increased with enhanced power of analysis by enrolling more serum samples of participants. In a study by Aparicio-Siegmund et al., it was found that sIL-6R and sgp130 protein act as IL-6-neutralising buffers and are reduced in diabetic patients. 29 They found that the higher level of sIL-6R can bind to IL-6 and neutralise low amounts of it and consequently block IL-6 signalling through the mIL-6R. 29 These findings confirmed the regulatory role of the rs4129267 variant on the sIL-6R level.
In our study, we found that the T allele, which is reduced in AS patients, is strongly and significantly associated with an elevated level of sIL-6R serum level. It seems that the rs4129267 T allele by increasing the serum level of sIL-6R, acts as an IL-6 neutralising buffer and by blocking the IL-6 signalling pathway may prevent AS disease incidence. Blocking of IL-6 signalling using its anti-IL-6R antibody (tocilizumab) is one of the treatments for this rheumatic disease; however, the response to tocilizumab for AS is still obscure. A Pharmacogenetics study of the correlation between IL-6R genotypes and response to tocilizumab could help to resolve ambiguities.
However, we observed an increase in sIL-6R levels with increasing T allele; the effect of this increase is not propagated in disease severity indicators or inflammatory factors. This rather indicates that rs4129267 does not have an impact on AS pathogenesis.
Conclusion
In conclusion, we identified the association between the rs4129267 T variant and the protection against susceptibility to AS disease in the Iranian population for the first time. We found that AS patients had significantly elevated IL-6 levels compared to healthy individuals. Increased IL-6 level and reduced frequency of IL-6R rs4129267 T allele in patients which contributes to reduced sIL-6R serum level, highlights the regulatory role of this variant and the importance of IL-6 signalling pathway in AS pathogenesis. However, more investigations are necessary to determine the exact function of IL-6R variants in AS pathogenesis.
Footnotes
Authors’ Contributions
SE, MA, FD, NA, SM, YV, and EM: Acquisition of data, drafting the article, analysis and interpretation of data, and final approval of the article. EF, MA, AJ, and MM: The conception and design of the study, revising the article critically, interpretation of data, final approval of the article.
Availability of Data and Material
All data generated or analyzed during this study are available upon request.
Consent to Participate
The written informed consent was signed by all participants before enrolling in the study.
Consent for Publication
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The procedures were approved by the ethics committee of the National Institute for Medical Research Development (Approval No: IR.TUMS.MEDICIN.REC.1397.774).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Deputy of Research, Tehran University of Medical Sciences (Grant No. 93-11-28-8001).