
Abstract

To The Editor,
Relapsing polychondritis (RP) is a rare autoimmune disease with recurring manifestations primarily affecting the cartilage and proteoglycan-rich tissues present in the ear, eye, and tracheobronchial tissues as well as non-cartilaginous tissues, and has an unpredictable disease course. The estimated incidence is <5 per million people/year. 1 The largest published case series from India describes 26 patients with ear chondritis as the most common manifestation in 25/26(96.1%) and laryngotracheal involvement in 3/26(11.5%) which is lower (11.5% vs. 50%) compared to other larger published case series worldwide. 2 Tracheobronchial involvement is associated with high mortality and warrants timely diagnosis and aggressive treatment. 3 Recently published guidelines on the management of RP advocate methylprednisolone pulses (1–3 grams/day) followed by high-dose oral corticosteroids (0.5–1 mg/kg/day prednisolone equivalent) for 3 weeks and tapering, followed by remission maintenance with Mycophenolate mofetil (MMF)/Azathioprine. The use of biologics including TNFa inhibitors (TNFi) has shown only transient and inconsistent efficacy. 4 We present a case of severe and refractory RP with bronchial involvement who was successfully treated with adalimumab at our centre. The patient gave written informed consent before the inclusion of details in this case report.
Case Presentation
A 50-year-old gentleman with a history of chronic tobacco consumption presented to the Rheumatology clinic with complaints of recurrent swelling and pain in his left ear for the past 3 years, for which he had consulted multiple doctors without significant relief in symptoms. For 1 year, he had noticed deformity of the left ear along with bilateral worsening hearing loss and progressive deformity of the nasal bridge. Also, he had noticed hoarseness of voice for the last 1 month, which had not improved with antibiotics. There was no history of fever, weight loss, skin nodules, ear discharge, nasal discharge, ocular complaints, cough or haemoptysis. On evaluation, he was breathless and had a saddle nose deformity along with a swollen, tender and deformed left ear with a spared lobule (Figure 1), B/L mixed hearing loss (Left>Right) confirmed on Pure tone audiometry. Blood investigations showed ESR 88 mm 1st hour (<10) and CRP 72 (0–6 mg/L) along with negative MPO and PR3 and normal mean corpuscular volume. Chest radiograph and high-resolution CT chest were normal. A diagnosis of RP was made. As the aetiology of dysphonia was still unclear, FDG PET was done, which showed FDG avid uptake in the ala of the nose, nasal septal cartilage, left auricle and auditory meatus, costal cartilages, trachea with focal luminal narrowing at D1/D2 vertebrae level (SUV max-2.7) and significant luminal narrowing in B/L main bronchus [left (SUV max-3) > right] (Figure 2A–C). In view of the critical narrowing of B/L main bronchus and impending respiratory failure, the patient was given pulse methylprednisolone (15 mg/kg/day) for 3 days followed by oral prednisolone at 0.5 mg/kg along with monthly cyclophosphamide pulse therapy (600 mg/m2) for 6 months. Post-treatment, his hoarseness of voice improved only marginally, so he was started on MMF (maximum 2 gm once daily for 6 weeks - stopped in view of intolerance) initially, followed by azathioprine (2.5 mg/kg for 6 months) and later injection adalimumab 40 mg s.c every 2 weeks in view of non-response. On follow-up after 1 year, patient’s hoarseness had improved completely with no further attacks of the ear or nasal chondritis. Repeat FDG PET (Figure 3D–F) showed a significant reduction in FDG avidity in all the previously involved areas except residual uptake in the trachea (SUV max –1.0) and left main bronchus (SUV max –1.2).
Arrows Depicting Saddle Nose Deformity and Cauliflower Ear.

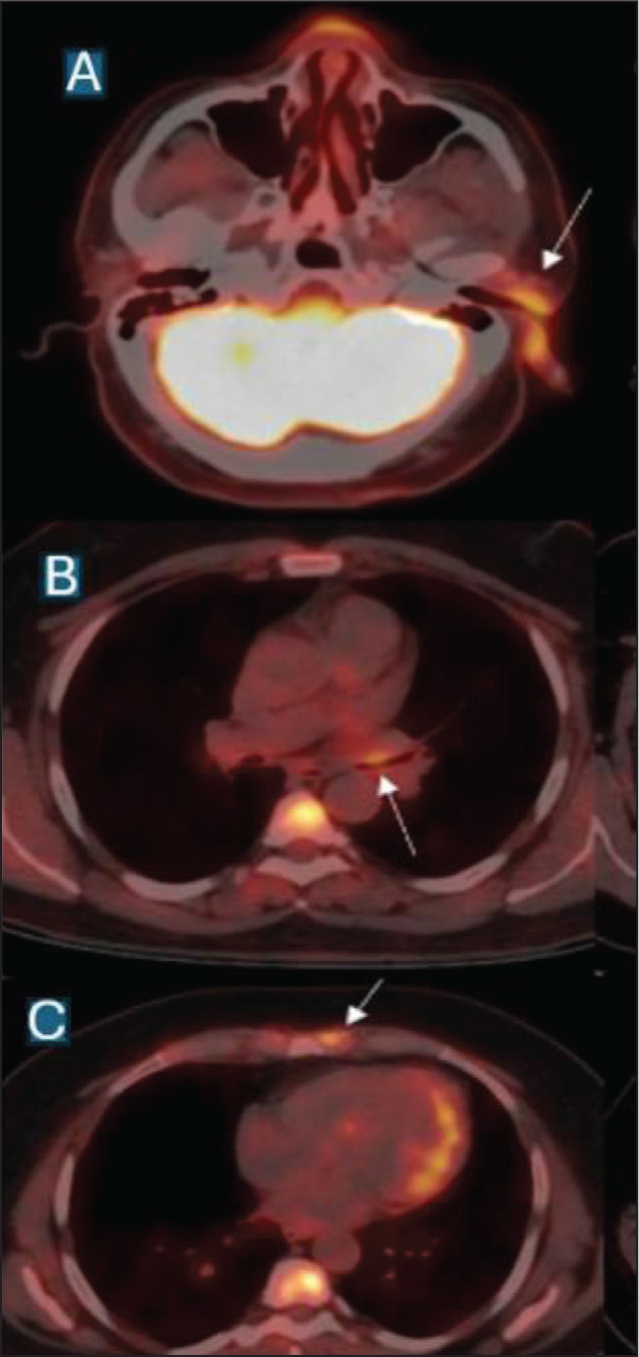
A,B,C: FDG PET Depicting Avidity in the Left Ear, External Auditory Meatus, Tracheal Cartilage, B/L Main Bronchus and Left 1st Intercostal Cartilage.
D,E,F: FDG PET Depicted no Avidity in Previously Involved Areas Except Mild Residual Uptake in Trachea (SUV max –1.0) and Left Main Bronchus (SUV max –1.2).

Tracheal involvement in RP has been shown to be a risk factor for disease recurrence and subsequent damage in a recent study and benefits from early initiation of immunosuppression. 5 Biologics including TNFi have been shown to be efficacious and safe in patients with RP who are corticosteroid refractory or dependent. 6 Recent data from a French National multicentre study suggest that 64% RP patients achieved clinical remission within 6 months of adalimumab therapy, including 6/8 (75%) patients with tracheobronchial involvement. The overall response rate with biologics was 62.9% with a low complete response (CR) of 19%. 93% (38/41) of patients received non-biological DMARD prior to receiving biologic therapy. The response was transient, leading to withdrawal in 18.1% of cases. 7 FDG-PET was useful for monitoring treatment response and detected a clinically inaccessible site in our patient. It has been shown to be useful for assessing disease activity, treatment response, and follow-up in patients with RP, and particularly in the detection of clinically inaccessible sites such as the trachea, which can be life-threatening. 8 A written consent was taken from the patient for publishing this case. Our case highlights the importance of systemic evaluation of patients with a saddle nose deformity and ear chondritis, which are like the tip of the iceberg in RP.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical Approval was not obtained from local ethics committee or institutional review board. It is because Adalimumab (TNF alpha inhibitors) used in this case is based on the evidence from a French National multicenter study (
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient’s written Informed consent was taken.