
Abstract

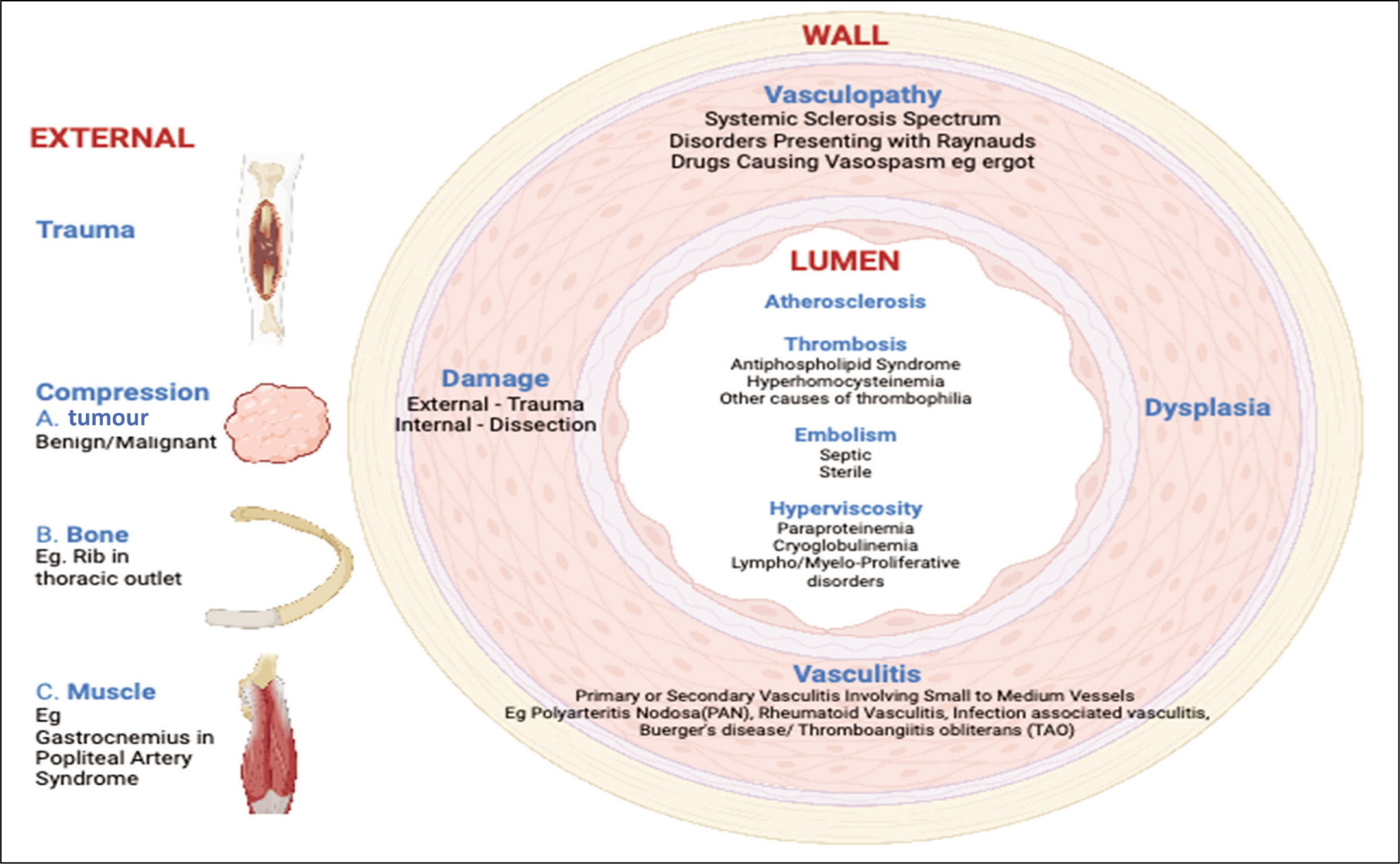
Digital gangrene is a devastating complication of peripheral limb ischaemia. Even with appropriate treatment, this can result in digit or limb loss. Atherosclerosis, thromboangiitis obliterans and infections are well-documented aetiologies of digital gangrene. However, digital gangrene might be the first indicator of a more complex multi-system disease. It is imperative for physicians to recognise that digital gangrene can also emerge as a manifestation of rheumatic diseases. Before hastily categorising gangrene as idiopathic, it is imperative to consider autoimmune aetiologies (Figure 1). The hastened classification of gangrene as idiopathic without considering autoimmune aetiologies is a missed opportunity for intervention. It is worth noting that rheumatic disease-related gangrene is not an untreatable enigma. On the contrary, early detection and prompt intervention can be pivotal, averting severe consequences such as amputation.
Myriad Aetiologies of Peripheral Gangrene (Created Using BioRender.com ).
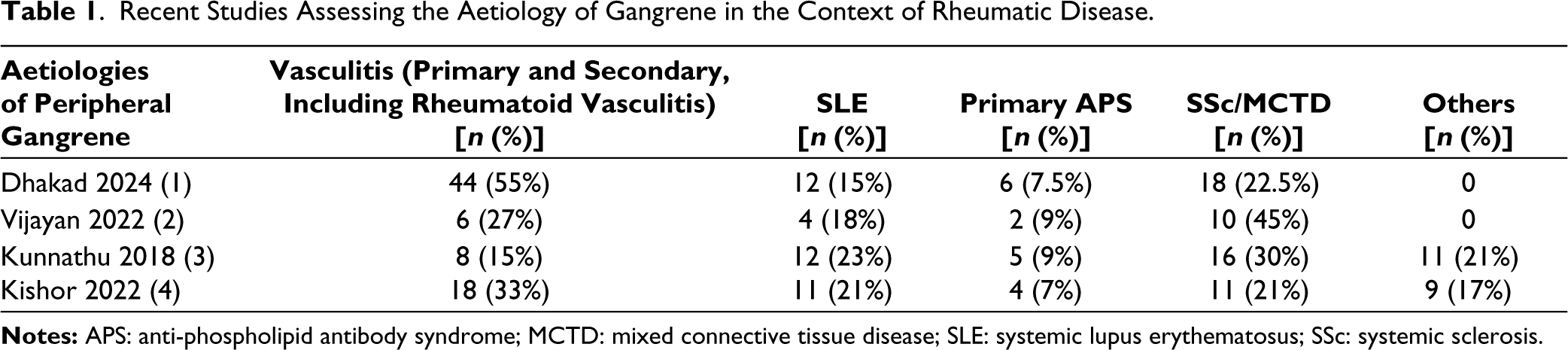
In this context, the study by Dhakad et al discussing the aetiology of patients presenting with peripheral gangrene to a tertiary care hospital is relevant. In nearly four-fifths of the patients in this study, an underlying rheumatic disease could be identified as the potential cause of gangrene. Although referral bias was likely the reason for such a large proportion of aetiologies as rheumatic diseases, this study underscores the importance of actively seeking rheumatic diseases as an aetiology for gangrene as this has therapeutic connotations. A few other studies had also evaluated the aetiologies of gangrene in the context of rheumatic diseases (summarised in Table 1).1–4
Recent Studies Assessing the Aetiology of Gangrene in the Context of Rheumatic Disease.
The prevalence and prognosis of peripheral gangrene vary with the underlying rheumatic disease. As an example, in patients with systemic sclerosis, data from the EUSTAR cohort reveal that nearly a tenth of patients experience digital gangrene. Those with a longer history of the disease, diffuse cutaneous systemic sclerosis, current or previous digital ulcers and diabetes or prior cardiovascular events are at heightened risk of digital gangrene. Furthermore, recurrent digital gangrene in a proportion of patients with systemic sclerosis underscores the need for ongoing vigilance. 5 In anti-phospholipid antibody syndrome, digital gangrene occurs in 2%–4% of patients, with arterial thrombosis in the lower limbs being the more common. 6 Contrary to the rarity of gangrene in Western populations with systemic lupus erythematosus, Indian studies report higher incidences of gangrene in lupus.7,8 Risk factors for peripheral gangrene in lupus include the presence of anti-phospholipid antibodies, lupus vasculitis and other clinical features such as Raynaud’s phenomenon, pulmonary artery hypertension and a history of thrombosis.9–11 Gangrene might also occur in the context of rheumatoid vasculitis, particularly in the presence of smoking, a longer disease duration, seropositivity, rheumatoid nodules or poorly controlled erosive arthritis. 12 Up to a third of patients with polyarteritis nodosa might experience peripheral gangrene, which is more prevalent in those from Asian countries. 13 The presence of gangrene in the context of a polyarteritis nodosa-like presentation should lead one to suspect a deficiency of adenosine deaminase 2. 14 In Takayasu’s arteritis, a disease which most often affects young women, gangrene is extremely rare with isolated case reports. In these reports, gangrene was noted to be more common in the lower limbs, often linked to type V (pan-aortic) disease with large vessel inflammation, thrombosis and coexisting anti-phospholipid syndrome. 15 Among ANCA-associated vasculitis, gangrene was most often observed with granulomatosis with polyangiitis, predominantly in male patients with multi-system disease and in the presence of antibodies to proteinase 3. 16
Treatment strategies for peripheral limb gangrene are diverse and should be tailored to the underlying cause. Vasodilators might help to address vasculopathy, while antiplatelets and anticoagulants are beneficial in thrombosis, including anti-phospholipid antibody syndrome. In the context of systemic vasculitis, immunosuppressive therapy with corticosteroids and disease-modifying anti-rheumatic drugs might be effective to halt the progression of peripheral gangrene. In the context of an acutely ischaemic limb or digit, treatment with heparin for 48–72 hours in the absence of any contraindications for the same may be warranted for its endothelial stabilising action. The findings by Dhakad et al 1 underscore the urgency of expedited referrals and treatment initiation. The sobering fact that over half of this patient cohort required amputation underscores the consequences of delayed medical intervention and late hospital presentation, often occurring when gangrene is already established, which invariably leads to poorer outcomes.
To conclude, the acumen to suspect, diagnose early and rapidly commence appropriate immunosuppressive, vasodilatory or antithrombotic therapy is indispensable for the preservation of digits in patients with gangrene. The study by Dhakad et al 1 serves as a critical reminder and reinforces the necessity of prompt action by rheumatologists faced with these ischaemic complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.