
Abstract
Introduction:
The prevalence of hyperuricemia is on the rise in specific populations, and there are difficulties in maintaining medication adherence. This study aims to investigate the factors linked to drug adherence in individuals with hyperuricemia.
Methods:
This was a cross-sectional study, which was conducted in 2023 by recruiting respondents with hyperuricemia. The demographic data collected included age, gender, occupation, body height and weight, education, marital status and ethnicity. Furthermore, drug adherence was determined based on the response to the Morisky Medication Adherence Scale-8. Acceptance and knowledge were measured using questionnaires given to the participants. Multivariate logistic regression analysis was then used to obtain the determinants of drug adherence.
Results:
Among 524 respondents who participated in the study, 60.3% and 30.15% had moderate and high adherence to serum uric acid-lowering drugs, respectively. The results showed that older age had a strong association with lower adherence (p < .01), while high disease acceptance significantly predicted higher levels (p < .01). Knowledge about gout symptoms (p = .003; OR: 0.28 [95% CI: 0.12-0.65]), causal factors (p < .001; OR: 2.63 [95% CI: 1.48-4.65]) and uric acid-lowering alternatives (p < .001; OR: 8.17 [95% CI: 4.11-16.25]) also had a positive correlation with higher levels.
Conclusion:
Knowledge and acceptance had a significant correlation with drug adherence among individuals with hyperuricemia in Aceh Province, Indonesia.
Introduction
In healthy individuals, serum uric acid levels are often below 7 mg/dL for men or approximately 6 mg/dL for women. Furthermore, hyperuricemia is a pathologic condition characterised by increased serum uric acid levels beyond the ranges. 1 This metabolic disorder serves as a prevalent underlying factor for several conditions, including gout arthritis, nephrolithiasis, hypertension, heart disease and diabetes. 2 Statistics revealed that approximately 14.4% of adults grapple with the disorder, 3 with the elderly demographic facing a higher susceptibility.4,5 Several secondary data-based studies suggested that individuals of Asian descent exhibit a greater vulnerability to developing hyperuricemia. 6 In the Indonesian context, several factors have been identified as significant predictors, including age, female gender, dietary patterns, stress levels and history of hyperuricemia incidence.7,8 This disorder’s associated economic and health burdens are notably substantial, particularly when it progresses to gout arthritis. According to reports in the United States of America, an afflicted patient can incur medical expenses of at least 3,000 USD annually due to gout-related care. 9 Furthermore, an episode of a gout attack can extend for five days or even longer, significantly impeding the ability of individuals to work. This situation often leads to indirect financial losses amounting to billions of dollars. 10
Xanthine oxidase inhibitors, such as allopurinol and febuxostat, are common medications that are often prescribed to improve hypouricemic conditions. 11 However, it is essential to note that febuxostat has been associated with a higher incidence of cardiac events or related fatalities compared to allopurinol. 12 Within Indonesia, the management method for hyperuricemia without clinical symptoms primarily emphasises lifestyle modifications. Xanthine oxidase inhibitors are typically reserved for cases of recurrent or severe hyperuricemia. 13 Patients with gout are often given colchicine as the first line of therapy, among other alternatives, such as non-steroidal anti-inflammatory drugs and corticosteroids. The prescription of xanthine oxidase inhibitors is recommended once the condition has subsided, typically for two weeks. It is important to note that patients who were already under these medications before the attack can continue consuming them. 13
The prevalence of gout in Indonesia was 7.3% in 2018, with the highest occurrence documented in Aceh, accounting for 13.3% of the total national rate. 7 This high prevalence shows the need to prevent the progression of gout stemming from hyperuricemia. One effective method is enhancing the adherence of patients to medication. Inadequate adherence to serum uric acid-lowering medication has been reported to have an association with the worsening progress of the disease. 14 Demographic characteristics, acceptance and knowledge of the disease and its treatment have been reported to be the significant factors influencing compliance with drug intake. 15 Therefore, this study aims to investigate adherence to uric acid-lowering medication and its associated factors, including knowledge and acceptance, among patients with hyperuricemia in Aceh Province, Indonesia.
Methods
This study aims to measure adherence, knowledge and acceptance of individuals with hyperuricemia in Aceh Province, Indonesia. Furthermore, the study procedures were carried out from March to July 2023. The sample population consisted of individuals aged ≥18 who lived in Aceh province and had been diagnosed with hyperuricemia. Individuals with serum uric acid above the normal levels (>7 for men and >6 for women) were considered to have hyperuricemia conditions. The participants were selected randomly using the probability sampling method, which provided equal opportunities for each member of the population.
Demographic characteristics, such as gender, age, marital status, occupation, education and nutritional status, were collected. Nutritional status was determined using body mass index (BMI), which was calculated by body weight (kg) by squared height (m2). Based on the BMI, the nutritional status of the participants was divided into several categories, including underweight (<17 kg/m2), normal (18.5–25.0 kg/m2), overweight (25.1–27.0 kg/m2) and obese (> 27 kg/m2). Furthermore, acceptance of the prescribed therapy was measured using the Acceptance of Illness Scale (AIS), where the total score was divided into ‘no acceptance’ (0–18), ‘moderate acceptance’ (19–29) and ‘high acceptance’ (30–40). 16 The Morisky Medication Adherence Scale (MMAS)-8 was used to measure drug intake adherence, and it comprised eight questions with ‘Yes’ and ‘No’ responses. Each correct response was given a single score (1) out of 8 scores in total. 17 The MMAS-8 has been validated in the local language, 18 and used in previous similar studies across other centres in Indonesia.19,20
The knowledge on hyperuricemia was measured using a set of questions concerning ‘the cause of hyperuricemia’, ‘the cause of gout arthritis’, ‘type and duration of the uric acid-lowering drug’, and ‘commonly associated diseases’. The assessment consisted of 10 questions, which were used to measure the knowledge; each had four responses with only one correct choice. Each correct answer corresponded to a score of ‘1’, while a wrong answer was given a score of ‘0’. All data in this study were collected through supervised interviews.
Data were pooled into specific categories and were then presented in the form of frequency (n). The statistical analysis was performed using Jamovi version 2.3.21 (
Results
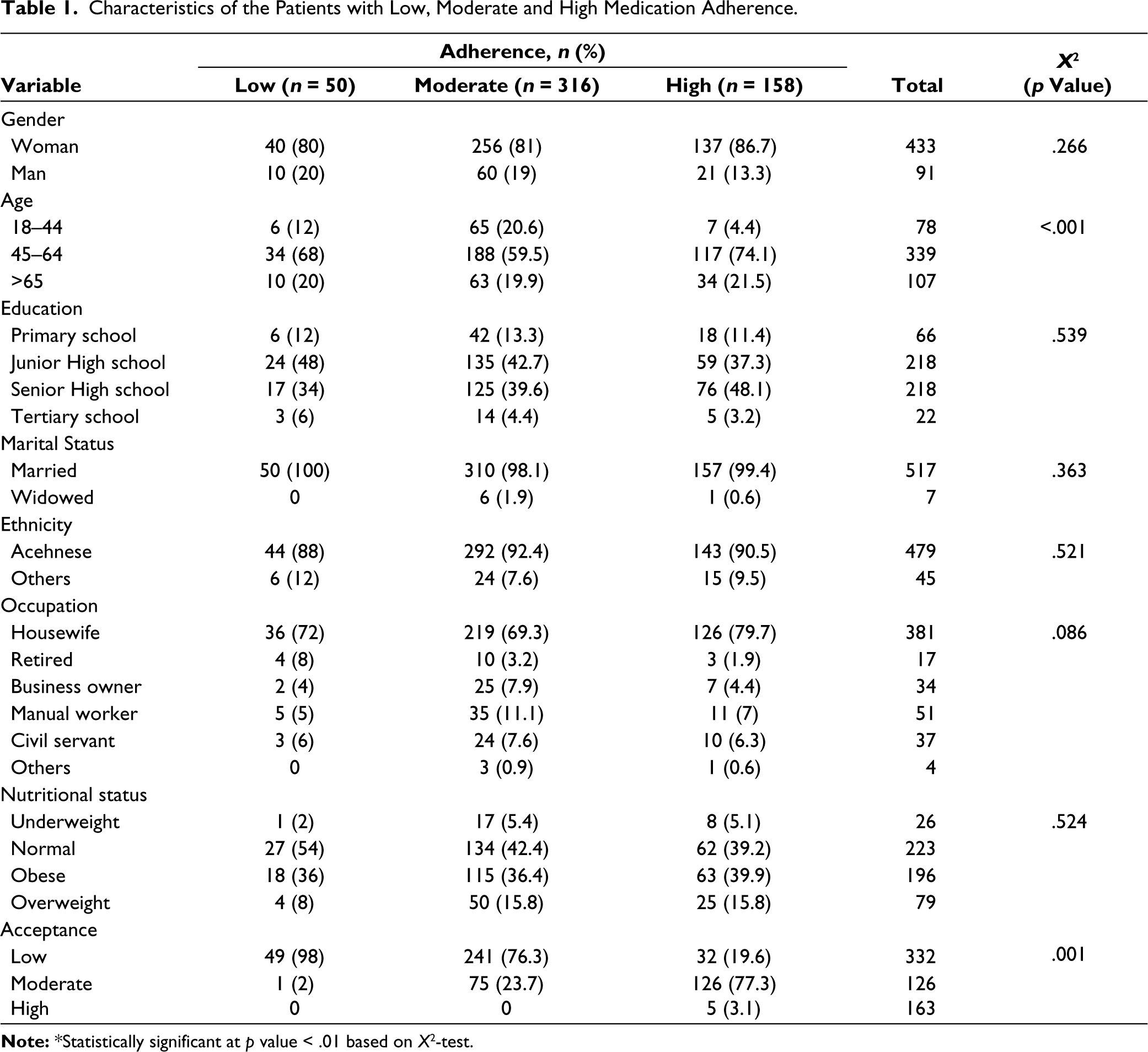
Most participants were females, constituting 80%, 256% and 86.7% of the patients in the low, moderate and high adherence groups. Furthermore, most of them were aged 45–64 years (%), followed by >65 years (n = 107) and 18–44 years (%). Most of the respondents had graduated from Junior (%) or Senior High Schools (%), and only a few attended tertiary schools (%). Approximately, 91.4% were of Acehnese descent, while others were from Bataknese, Javanese and Padangnese. The results showed that only 7 respondents were widows, and the remaining were married.
This study showed no significant association between gender and the level of adherence (p > .05). Education, marital status, ethnicity, occupation and nutritional status were also shown to lack a significant relationship (p > .05). Furthermore, age was the only demographic characteristic with a significant association with the levels of adherence (p < .001). Most of the respondents had low acceptance of the medication (%), and this variable was strongly associated with adherence (p = .001), as shown in Table 1.
Characteristics of the Patients with Low, Moderate and High Medication Adherence.
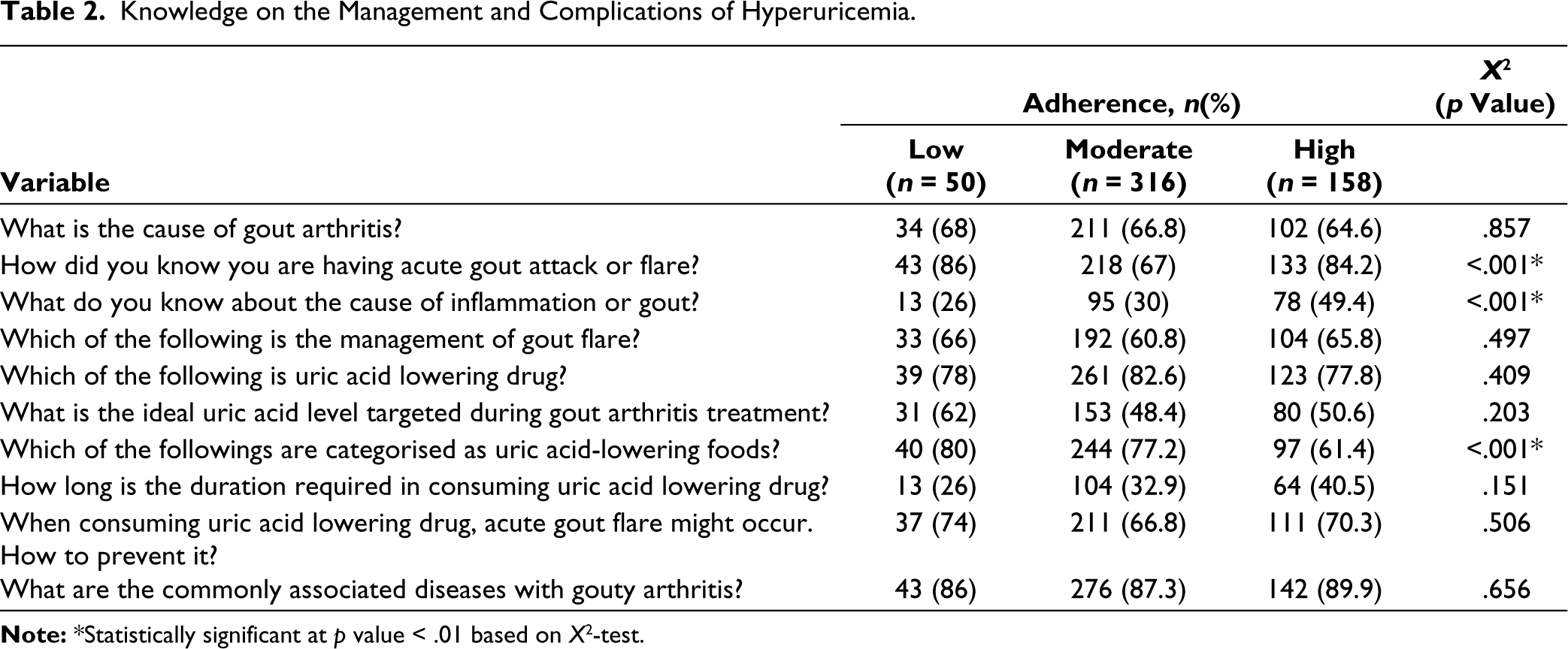
The association between knowledge and medication adherence of hyperuricemia patients in Aceh, Indonesia, is presented in Table 2. The results showed that 3 out of 10 questions had significantly different responses among individuals with low, moderate and high adherence (p < .001). ‘How did you know you have acute gout attack or flare?’ received correct responses from 86%, 67% and 84.2% of patients with low, moderate and high adherence, respectively. A total of 26%, 30% and 49.4% of individuals in the low, moderate and high adherence groups correctly responded to the question ‘What is the cause of inflammation in the case of gout arthritis?’ respectively. Meanwhile, the question ‘Which of the following can reduce serum uric acid level besides drug intake?’ received correct responses from 78%, 82.6% and 77.8% of patients in the low, moderate and high adherence groups, respectively.
Knowledge on the Management and Complications of Hyperuricemia.
The results of the multivariate multinomial logistic regression on age, acceptance and knowledge are presented in Table 3. Age was found to have a positive correlation with adherence. Furthermore, participants aged 45–64 years old (p < .001; OR: 4.92 [95% CI: 1.9–12.43]) and >65 years old (p =.001; OR: 5.51 [95% CI: 1.97–15.38]) were likely to have higher levels compared to those aged 18–44 years old. Acceptance had a significant positive correlation with adherence level, as shown in low-moderate (p = .004; OR: 0.05 [95% CI: 0.01–0.39]) and high-adherence (p < .001; OR: 23.82 [95% CI: 12.36–45.9]) model.
Predictors for Medication Adherence Among Hyperuricemia Patients.
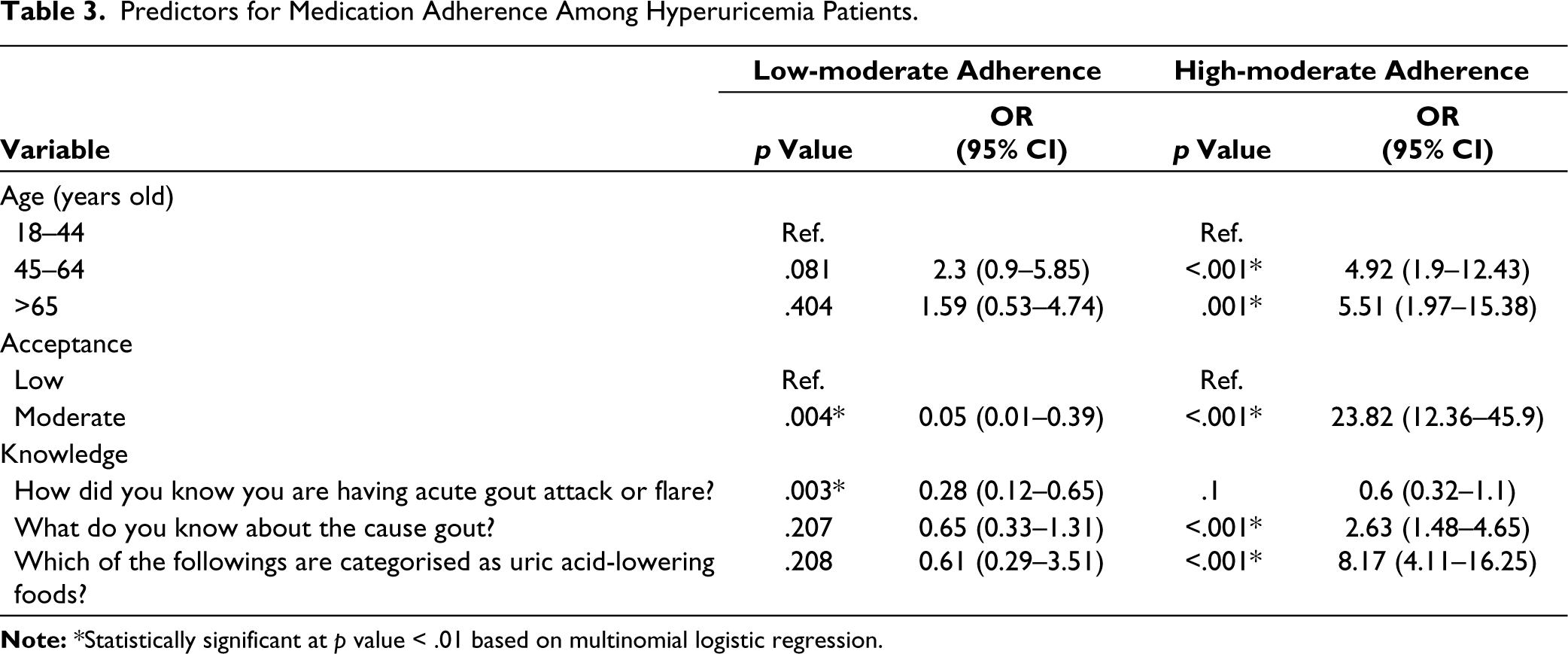
Based on the results, there was a positive correlation between knowledge and medications. Knowledge of the symptoms of gout attack (p = .003; OR: 0.28 [95% CI: 0.12–0.65]) determined the level of adherence in the low-moderate adherence model but had no effect in the high-moderate adherence comparative model (p = 0.1; OR: 0.6 [95% CI: 0.32–1.1]). In the high-moderate adherence model, patients with more knowledge of the causes of gout arthritis (p < .001; OR: 2.63 [95% CI: 1.48–4.65]) and the alternatives to lower serum uric acid (p < .001; OR: 8.17 [95% CI: 4.11–16.25]) were likely to adhere more to drug intake.
Discussion
In this study, older individuals were likely to have high levels of adherence to drug intake compared to the younger age group. This was probably caused by their understanding of the complications of hyperuricemia. However, the results of this study showed that age was a determining variable for the use of medication among individuals with low and moderate levels. Age has also been reported to have an association with medication adherence in various pathologic conditions, including asthma, 21 rheumatoid arthritis, 22 and multiple sclerosis. 23 Acceptance in this current study contributed significantly to both comparative models. Although the variable did not guarantee high compliance with drug intake, it was found to be a contributing factor in several studies.24,25
Knowledge of the onset of gout attack and its pathomechanism positively correlated with adherence. The knowledge of tophi as a sequela of hyperuricemia may enhance patients’ adherence to urate-lowering therapy since tophi are more noticeable, chronic and incurable than gout flares and may impair the patients’ well-being and self-esteem. 14 The awareness of gout arthritis as a complication of hyperuricemia could motivate individuals to follow their medication plan. Patients who had experienced this condition were likely to adhere to the medications to avoid its recurrence. The knowledge of acid-lowering drug alternatives also contributed positively to adherence levels. This suggested that hyperuricemia patients were actively seeking other alternatives to optimise the efficacy of their medications.12,26,27 The ability to adjust to a healthy lifestyle significantly prevented the incidence of hyperuricemia and gout. 28 However, the efficacy was sub-optimal for those with severe hyperuricemia or underlying conditions, such as kidney disease, metabolic syndrome and hypertension. Individuals with persistent hyperuricemia often require a lifelong medication plan. 29
A study on patients who were under uric acid-lowering therapy revealed the occurrence of a high number of interrupted medications (>60 days) among 70% of the respondents. 30 A high occurrence rate was frequently observed in groups new to the treatment (≤ 1-year medication). Other studies also showed that patient adherence to allopurinol intake was consistently below 50%.31,32 In most studies, poor compliance was associated with the non-immediate impact of the drug in lowering serum uric acid.31,33 Apart from adherence to drug intake, compliance with a healthy lifestyle must also be considered. In a large cohort study, adherence to a healthy lifestyle was significantly more likely to reduce the risk of developing hyperuricemia than those with low genetic risk. 28 Lastly, cultural factors may affect medication adherence substantially, as they may determine the patients’ cognitions, emotions and actions concerning their health status and management. Prior research has indicated that cultural factors can modulate different facets of medication adherence, such as illness representation, health literacy, self-efficacy, spirituality and religiosity, and utilisation of complementary and alternative medicine.34,35 Therefore, future studies should consider how the community’s cultural background would affect their adherence to the medication.
Despite the interesting findings, this study has several limitations. The cross-sectional design precludes the inference of causal links between the factors under investigation and medication adherence. The reliance on self-report measures may entail recall bias. The predominance of female participants may compromise the external validity of the findings. The regional specificity of the study may limit the transferability of the findings to other contexts. Furthermore, the medication type used by the respondents was not recorded. Future research could employ longitudinal designs to elucidate the causal mechanisms between the studied factors and medication adherence and examine the effectiveness of a community-based intervention to enhance the community’s medication adherence.
Conclusion
In conclusion, age and the level of acceptance were strong determinants of patients’ adherence to serum uric acid-lowering medication. The results showed that knowledge positively contributed to the occurrence of higher compliance. Furthermore, awareness of gout arthritis symptoms increased adherence from low to moderate levels. In-depth knowledge, such as the pathomechanism of gout arthritis and alternatives for reducing serum uric acid, had a significant correlation with higher levels of adherence among the moderate and high adherence groups. The results of this study are expected to help increase patient compliance in Aceh. Further study with a larger sample size is required to confirm the results obtained.
Footnotes
Acknowledgements
The authors would like to thank the nurses who assisted us during the data collection of this study.
Authors’ Contributions
SA collected data, designed the methods, wrote research proposals and performed data analysis. HS wrote a research proposal for ethical approval and critically revised the manuscript. KH designed the methods and performed critical revision of the manuscript. MS performed data analysis, revised and edited the final manuscript and reviewed and updated the references. All authors have critically reviewed and approved the final version and are responsible for the content and similarity index of the manuscript.
Data Availability Statement
The data supporting this study’s results are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Consent to Participate
This study was approved by the ethics committee of the Faculty of Nursing Syiah Kuala, Banda Aceh, Indonesia (reference number:113020301221). Furthermore, informed consent was collected from the respondents and documented.
Funding
This study was funded by the Ministry of Education, Research, and Technology of the Republic of Indonesia (56/UN11.2.1/PT.01.03/DPRM/2022).