
Abstract
Objective:
To estimate the level of urinary C-terminal telopeptide of type II collagen (uCTX-II) as a biomarker of cartilage turnover and to determine its correlation with radiological grading, pain, and functions of patients with knee osteoarthritis (OA).
Methods:
A descriptive cross-sectional study was conducted between September 2017 and August 2019 on 102 patients suffering from knee OA. Detailed demographic data were collected. uCTX-II level was measured for each patient. Radiological grading, pain and functional assessments were performed using Kellgren-Lawrence (K-L) grading, visual analogue scale (VAS), and Western Ontario and McMasters Universities Osteoarthritis Index (WOMAC).
Results:
The mean age of 62.3 (6.4) years and most patients (n = 56, 54.9%) were 61–70 years old. Females constituted 80.4% (n = 82). Among the occupations, housewives were more affected (55.9%, n = 57). Out of 102 patients, 32 (31.4%) had VAS pain 4, 25 (24.5%) had 5 and 45 (44.1%) had 6; 9 (8.8%) had K-L score 1, 51 (50%) had 2, 41 (40.2%) had 3 and 1 (1%) had 4; 35(34.3%) had WOMAC score <30, 59 (57.8%) had 30–40, and 8 (7.8%) had >40; 55 ( 53.9%) had uCTX-II level <50 ng/mmole, 25 (24.5%) had between 50 and 200 ng/mmole and 22 (21.6%) had >200 ng/mmole. There was a positive correlation between uCTX-II and WOMAC (P = .006) and VAS (P = .042).
Conclusion:
The present study findings highlighted that higher levels of uCTX-II were associated with higher levels of pain and greater difficulty with daily activities (measured by WOMAC disability score). This suggests that uCTX-II could be a useful biomarker for monitoring cartilage turnover in patients with knee OA and its relationship with pain and functional abilities.
Introduction
Osteoarthritis (OA) is a degenerative joint disease, occurring primarily in older persons, characterized by erosion of articular cartilage, osteophyte formation, subchondral sclerosis, and a range of biochemical and morphological alterations of the synovial membrane and joint capsule. 1 Among the rheumatologic diseases, OA is the second most prevalent joint disease in India, with a prevalence of 4.39 (95% CI: 3.30, 5.61). 2 There is a greater prevalence of OA in women than in men, and its prevalence increases with age.3-5
Individuals with OA generally describe pain in the joint(s) that is worse with activity, with limited morning stiffness (<30 minutes), and pain and stiffness with rest. There is a need for reliable and accurate biomarkers to detect OA at an early stage. Such biomarkers include serum Cartilage Oligomeric Matrix Protein (COMP), serum hyaluronic acid, and urinary C-terminal telopeptide of type II collagen (uCTX-II). Type II collagen is predominantly found in cartilage and is the most abundant protein in the articular cartilage extracellular matrix. 6 CTX-II has been detected in both synovial fluid and urine. An advantage of urine analysis is that urine can be obtained more quickly than synovial fluid, which facilitates a more robust research design.
For more than four decades, Kellgren-Lawrence (K-L) radiographic grading scheme and atlas have been used as reference standards for OA assessment. Most studies have reported that radiographic OA (ROA) is poorly correlated with knee symptoms, and most risk factors for ROA do not predict knee pain well.7,8 We are therefore interested in exploring the extent to which the uCTX-II marker could be considered independent of known risk factors for ROA, such as age, sex, and body mass index (BMI). Furthermore, it is conceivable that a dynamic change in cartilage metabolism could be detected in combination with factors that might reflect an ongoing OA process, such as the presence of joint pain. As such, joint pain might be considered a potential effect modifier of the relationship between C‑terminal telopeptide of collagen type II (CTX-II) and ROA. A recent study from China highlighted that CTX-II and IL-1β would be promising biomarkers for early diagnosis and treatment of knee OA. 9 However, there is a paucity of data providing an association of uCTX-II with radiological grading and pain in patients with primary knee OA in Indian settings.
Therefore, the present study aimed to estimate uCTX-II collagen and its correlation with radiographic grading, function, and associated knee pain in Indian patients with primary knee OA.
Methods
A descriptive cross-sectional study was conducted at the Department of Physical Medicine & Rehabilitation, Regional Institute of Medical Sciences, Imphal between September 2017 and August 2019. Patients with knee OA fulfilling the 2016 ACR (American College of Rheumatology) revised criteria 10 for early diagnosis of knee OA (Clinical and Radiographic) were included in the study. Patients having any of the following conditions were excluded from the study: severe co-morbid conditions such as stroke, uncontrolled diabetes mellitus, heart disease, and vascular diseases; inflammatory disease of joints like rheumatoid arthritis, recent knee trauma, metabolic bone diseases, history of knee trauma or surgery, history of current knee intra-articular steroid injection or hyaluronic acid within the last six weeks; cognitive impairment. The study was approved by Research Ethics Board (REB), RIMS, Imphal. A signed informed consent form was obtained from all patients in this study.
The symptomatic knees were assessed by an X-ray of both knee joints and using a weight-bearing anteroposterior radiograph of the knee. The severity of the disease was graded radiologically by K-L grading. 11 The functional assessment was done using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) subscale Index, a self-administered questionnaire designed to assess lower extremity pain and function in knee and hip OA. 12 The pain assessment was carried out using the Visual Analogue Scale (VAS) 13 consisting of a 10 cm line with two end-points representing ‘no pain’ and ‘worst pain imaginable’.
Second-void morning urine samples were collected within two hours of waking. Samples were immediately placed on dry ice and transported for storage at –20°C until analysis. The uCTX-II level was measured using Human Cross-Linked CTX-II, CTX-II ELISA Kit, Chongqing Biospes Co., Ltd., China (Catalog No: BYEK2806). A monoclonal antibody specific for CTX-II fragments is used in the competitive enzyme-linked immunosorbent assay to measure uCTX-II. The concentration of CTX-II (ng/litre) was standardized to the total urine creatinine (mmole/litre), and the units for the corrected CTX-II concentration were ng/mmole. 14 Quantitative detection of creatinine in urine was done by Human Creatinine ELISA Kit Chongqing Biospes Co., Ltd. (Catalog No: BYEK2883).
The corrected concentration of uCTX-II for urinary creatinine concentration was calculated using the formula:

Sample Size
Calculation of sample size was done using power (1-β) of 90% with a significance level (α) of 0.05. Using the following formula: N=[(Zα+Zβ)/C]2 +3, Where Zα=1.96 Zβ=1.282 at power of 90%. C value was calculated by using the following formula:

Where r=correlation coefficient between uCTX-II and patients with OA according to study conducted by Majachunglu G et al. 15 A minimum sample size of 67 was needed.
Statistical Analysis
Data were analysed using the statistical package for the social sciences (SPSS) version 21. The qualitative data were expressed as numbers and proportions, while the quantitative data were expressed as mean (standard deviation [SD]). Categorical and continuous variables were compared with the chi-square and Fischer exact tests, respectively. Pearson correlation and ANOVA were used to find the correlation between variables and the association among variables. Differences were considered statistically significant if the P value <.05.
Results
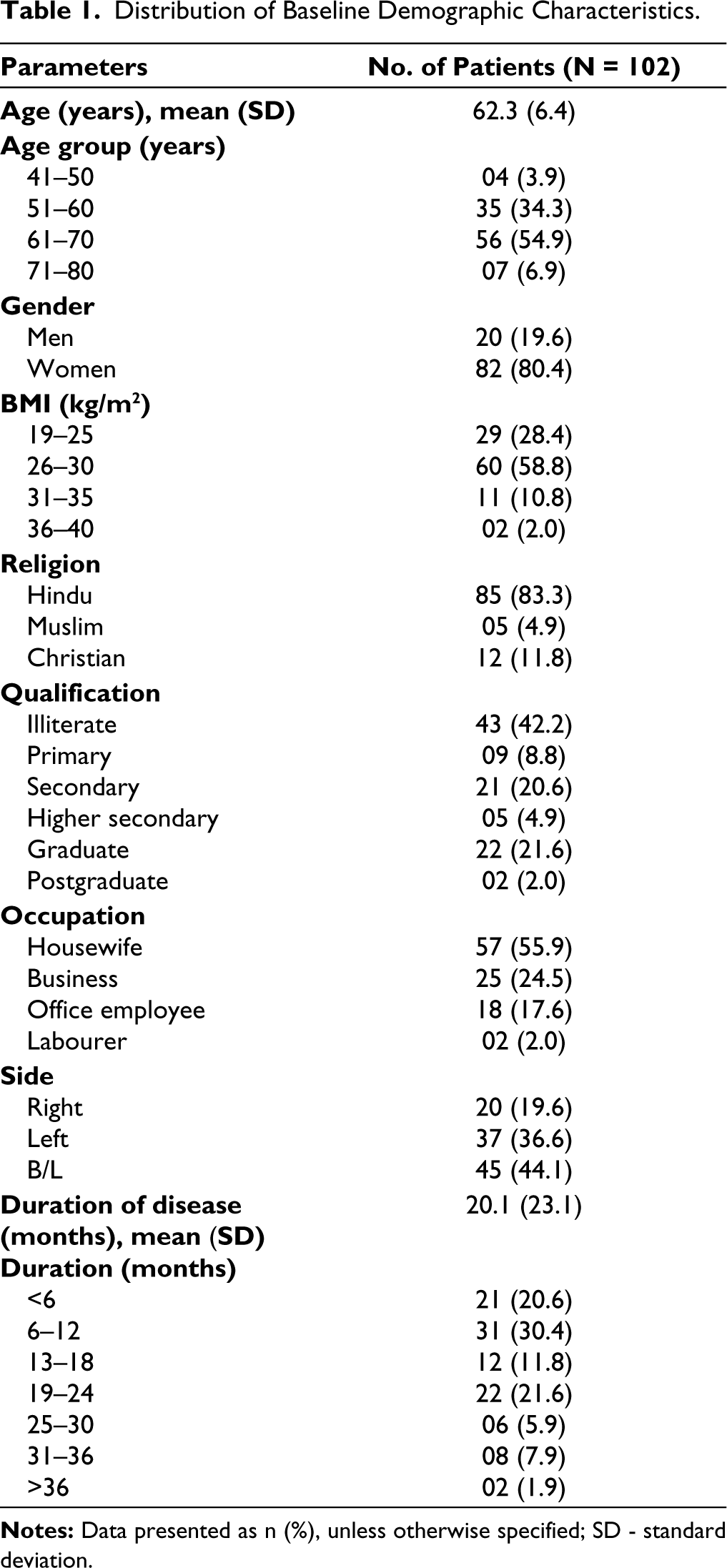
One hundred two patients, comprising 82 (80.4%) women and 20 men (19.6%) with primary knee OA, were included in this study. The mean (SD) age was 62.3 (6.4) years, and the majority of patients (n = 56, 54.9%) belonged to the age group of 61–70 years. The BMI of most patients (58.8%) was between 26 and 30 kg/m2. The mean duration of the disease was 20.1 (23.1) months (Table 1).
Distribution of Baseline Demographic Characteristics.
About 45 (44.1%) patients had a VAS score of 6. More than half of the patients (n = 59 [57.8%]) presented WOMAC scores between 30 and 40. On radiographic assessment using the K–L grading scale, nine (8.8%) patients were of grade 1, 51 (50%) patients were of grade 2, and 41 (40.2%) patients were of grade 3. About 55 patients (53.9%) had uCTX-II level <50 ng/mmole, followed by 25 patients (24.5%) and 22 (21.6%) patients having uCTX-II level 50–200 ng/mmole and >200 ng/mmole, respectively (Table 2).
Distribution of Clinical, Radiographic and Laboratory Results.
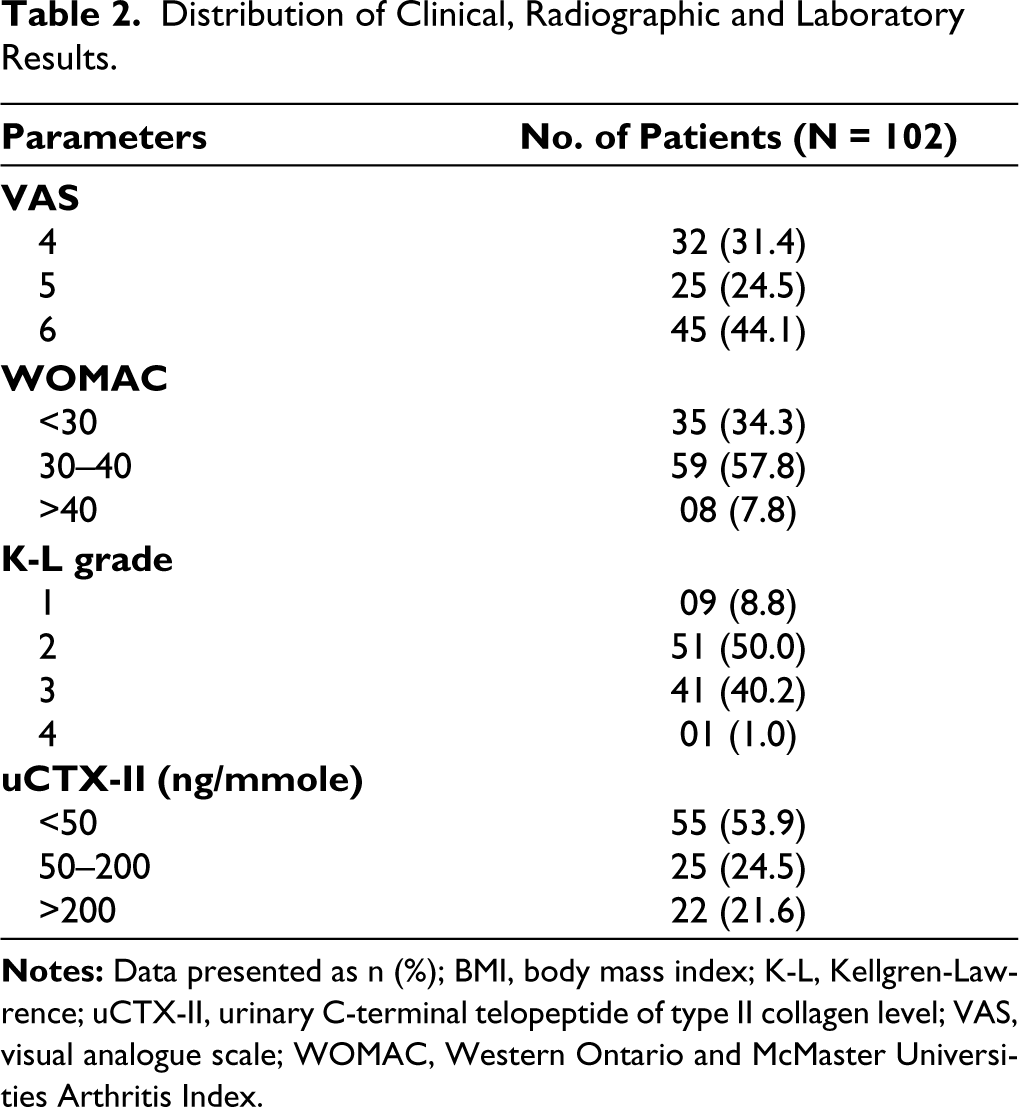
Table 3 shows the correlation of uCTX-II with WOMAC and VAS and the correlation of VAS with WOMAC. A positive correlation was observed between uCTX‑II and WOMAC (R = 0.272, P = 0.006) and between uCTX-II and VAS (R = 0.203, P = 0.042). However, there was no correlation between VAS and WOMAC (R = 0.124, P = .215).
Correlation Between WOMAC, VAS and uCTX-II.

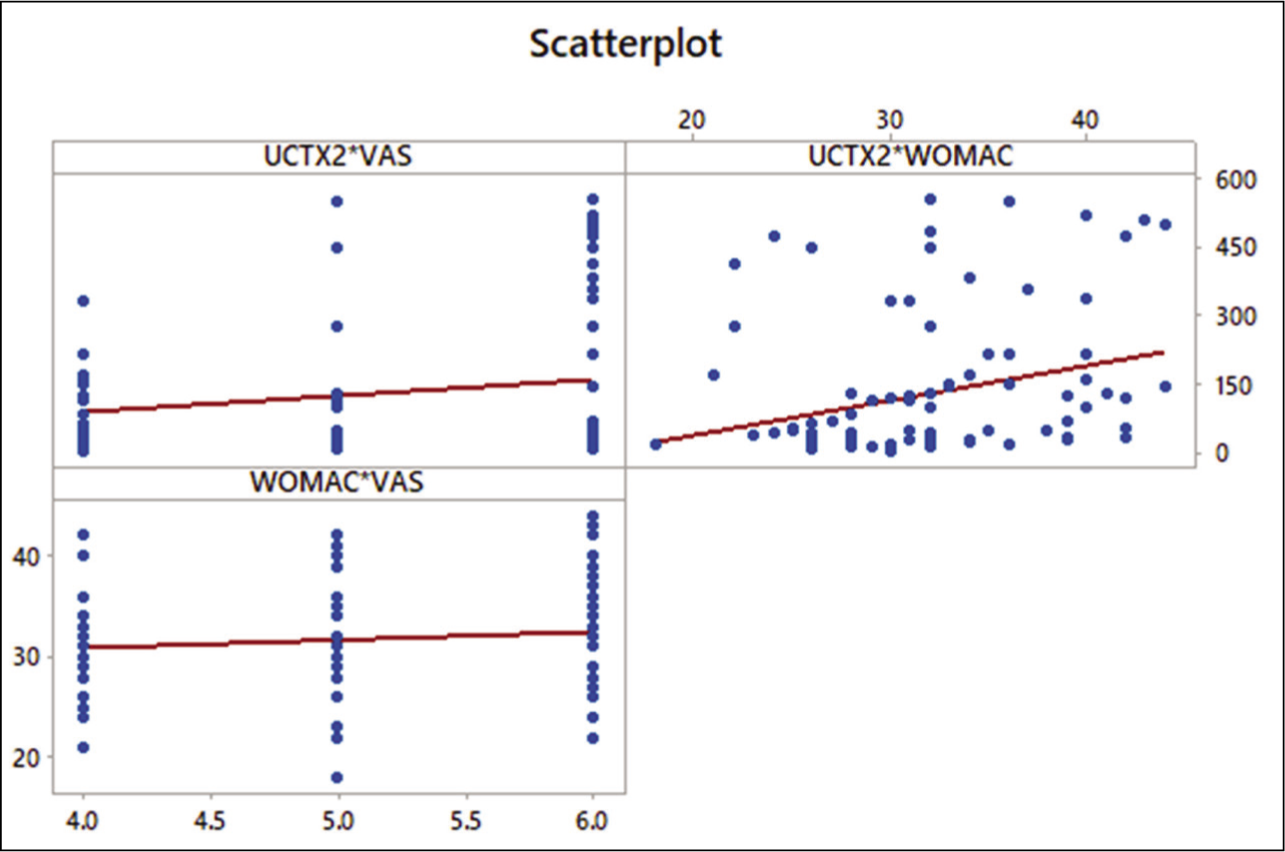
Figure 1 shows a positive correlation between (a) uCTX-II and VAS: the higher the score of VAS, the higher the uCTX-II level and is linearly correlated; (b) uCTX-II and WOMAC: linearly correlated; and (c) No correlation between WOMAC and VAS.
Scatter Plot Showing a Correlation Between uCTX-II Versus VAS, uCTX-II Versus WOMAC and WOMAC. Versus VAS. uCTX-II, Urinary C‑terminal telopeptide of type II collagen; VAS, visual analogue scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
The comparison of VAS, WOMAC, and uCTX-II with KL grades is represented in Table 4A. KL grade 4 had the lowest mean VAS score (4.0 [0]), while KL grade 3 had the highest mean VAS score (5.2 [0.9]). KL grade 3 had the highest WOMAC score (32.1 [5.9]) and uCTX-II level (134.9 [162.8]). KL grades 1 and 4 had the lowest mean WOMAC score (30.9 [4.5]) and uCTX-II level (41.9 [0]), respectively. However, the comparison between K-L grades was not statistically significant.
Comparison of VAS/WOMAC/uCTX-II According to KL Grades and BMI.
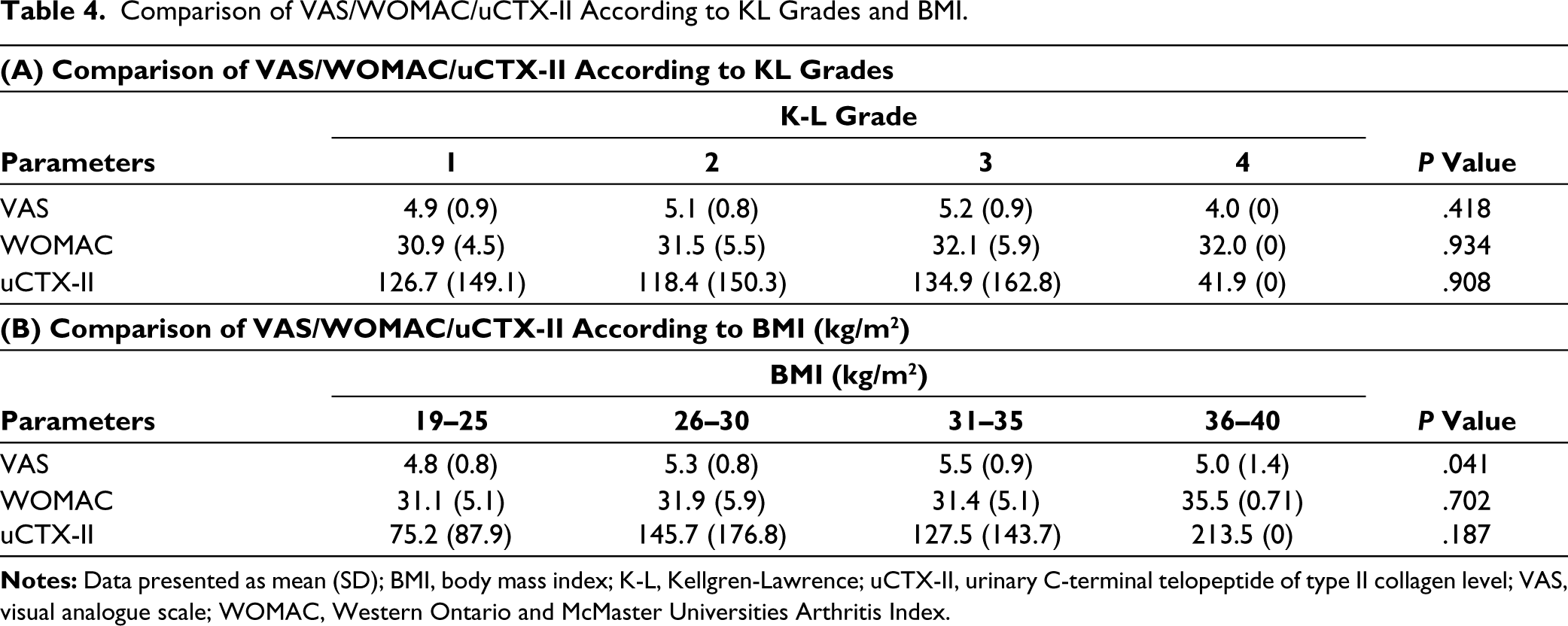
The highest mean scores of WOMAC (35.5 [0.7]) and uCTX-II (213.5 [0]) were in the BMI range of 36–40 kg/m2, indicating grade II obesity. No statistical significance of WOMAC and uCTX-II scores with BMI categories was observed. However, the VAS pain score was found to be significantly correlated with BMI (P < .041) (Table 4B).
Discussion
Chronic pain and disability are often associated with OA, which occurs most frequently in the knee joint.16,17 In OA, the complexity makes the development of biomarkers challenging since genes, trauma, biomechanics, and exercise all play a part in the onset of the disease, and different pathophysiological mechanisms may favour different phases of the disease. As of now, uCTX-II levels can be used to differentiate knee OA patients from healthy controls, which could serve as a biomarker for the disease.15,18,19 In the present study, we found a positive correlation between uCTX-II and VAS and uCTX-II and WOMAC in clinical patients with primary OA of the knee. This indicates that uCTX-II can be used as a biomolecule marker for early diagnosis of patients with primary OA of the knee.
The mean age of patients in the present study was 62.3 (6.4) years, and the majority of patients belonged to the age group of 61–70 years, showing an increased incidence after the age of 50 years. Similar findings were observed in the previous studies, where the median age of symptomatic knee OA was 48–69 years.9,20 In contrast, a recent study from India reported that the mean age of patients with and without knee pain was 44.72 and 42.71 years, respectively. 21
In the present study, knee OA was more prevalent in females than males. Previous studies reported that knee OA occurs commonly in females, especially those above 45 years of age; however, contradictory results are identifying the link between oestrogen and the prevalence of OA in women after menopause.15,21-23 Females with a higher incidence of OA knee may be related to post-menopausal oestrogen deficiency. Articular chondrocytes possess functional oestrogen receptors that suggest their regulation by oestrogen. 24
In this study, 22 (21.6%) patients had uCTX-II levels >200 ng/mmole. The mean value of uCTX-II was 125.04 (153.51) (ng/mmole). Whether patients with OA had higher values of uCTX-II than healthy normal individuals was not ascertained since we did not include the control group in the study. However, the mean value of uCTX-II observed in the present study was comparatively lower than the previous study conducted by Majachunglu G et al. 15 A recent study by Liu-CX et al. reported that the mean uCTX-II level was significantly increased by 3.31, 7.15, and 8.38 folds in mild, moderate, and severe knee OA patients compared to the control group. 9 This indicates that the level of uCTX-II depends on the severity of knee OA. In the present study, the lower level of uCTX-II may be because most patients observed mild knee OA.
According to K-L radiographic grading, most patients were of grade 2 (50.0%) and 3 (40.2%). Similarly, Ram p, et al. reported that the majority of Indian patients with knee OA had KL grade 2. 21 Plain X-rays are limited to detecting cartilage degradation if significant cartilage degradation has occurred. 25 In the current study, uCTX-II was positively correlated with VAS (r = 0.202, P = .042) and WOMAC (r = 0.272, P = .006) scores. Similar findings were also observed in the study conducted by Abdel Ghany HM, et al., in which there was a correlation between uCTX-II and WOMAC but not with the radiological findings in patients suffering from primary OA. 18 These findings suggest that the more cartilage degradation, the more biomarkers, pain, and disability will be released even before the radiographic assessment changes.
However, the exact mechanism behind the cause of pain and disability due to cartilage degeneration in patients with OA is unknown. Since cartilage is aneural, it cannot cause pain directly. 26 The changes in articulation caused by structural and associated changes in extracellular matrix turnover in articular cartilages, shown by cartilage degradation biomarkers25,27,28 may manifest pain in other joint tissues. The presence of synovitis may result from altered joint mechanics leading to structural changes elsewhere or the generation of joint debris. Patients with OA experience pain in the subchondral bone, osteoperiosteal, synovium, ligaments, and joint capsule due to their rich innervation and nerve endings. The involvement of subchondral bone can be confirmed by an increase in uNTx, the bone resorption marker. There may be potential remodelling at the interface between subchondral bone and articular cartilage in OA. A recent discovery indicates that CTX-II is also derived primarily from calcified cartilage at this site, 29 which is of great interest since this biomarker has been associated with joint pain and is also associated with knee pain in K/L grade 2 patients.
Our study showed no significant correlation between VAS pain and WOMAC score. It is explained by a study by Serban O et al., 30 which showed that cartilage damage was the only independent predictor for the VAS pain scale. Instead, there were several predictors for the WOMAC score: cartilage damage, medial osteophytes, and lateral meniscal protrusion. They found that pain intensity increased with the severity of these pathological findings.
On the other hand, there was no correlation observed between uCTX-II and the K-L grading scale. Many studies have been conducted to research the connection between radiographic severity and disability in knee OA. This study did not correlate with K-L grade and severity of pain and disability. Possibly, this is due to the patient’s characteristics since they were primarily categorized as mild-to-moderate by radiographs. Radiographs demonstrate only structural changes rather than disease severity. As a result of conventional radiography, knee compartments (medial, lateral, and patellofemoral compartments) can only be assessed in a limited way.
Limitations
The small sample size limited the present study. Moreover, there was no control group in the study. This was a cross-sectional observational study that might have introduced some bias into the results. The present analysis results are limited by the shortage of radiographic assessments of non-knee joints, potentially confounding the extent of uCTX-II by the presence of underreported or unknown non-knee OA.
In conclusion, the present study findings highlighted that higher levels of uCTX-II were associated with higher levels of pain and greater difficulty with daily activities (measured by WOMAC disability score). This suggests that uCTX-II could be a useful biomarker for monitoring cartilage turnover in patients with knee OA and its relationship with pain and functional abilities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Committee Approval
The study was approved by Research Ethics Board (REB), RIMS, Imphal. A signed informed consent form was obtained from all patients in this study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.