
Abstract
Aim:
To study the clinical and serological predictors of radiological progression at one year in a cohort of Indian patients with early rheumatoid arthritis (RA).
Methods:
In this prospective open-label observational study, consecutive patients with early RA (<six months) were examined at baseline and at each visit (0, 3, 6, 9 and 12 months) for disease activity, DAS ESR 28 and European League Against Rheumatism response. Radiography of the hands and feet was performed at baseline and at one year of treatment, and radiologic progression was assessed using van der Heijde’s Sharp score. The prognostic factors were evaluated using a logistic regression model.
Results:
Fifty-one eligible patients were analysed for disease outcomes, whereas 43 were eligible for radiographic progression. The mean duration of RA was 3.4 ± 1.85 months. At baseline, 96% of the patients had moderate to high disease activity. The proportion of patients with erosions increased from 16.3% to 37.2% at one year, whereas that of patients with joint space narrowing (JSN) increased from 21% to 39.5%. At one year, the mean increase in total Sharp’s score was 1.67, while 32.5% of patients had radiological progression. Age of onset, presence of erosions, JSN, anticitrullinated protein antibody (ACPA) titre and tender joint counts at baseline were associated with radiographic progression at one year. However, in the multivariate analysis, none of the variables predicted radiographic damage. Only JSN was positively associated with progression at one year.
Conclusion:
Age at onset, presence of erosions, JSN, ACPA titre and tender joint counts at baseline were associated with radiographic progression at one year, but further studies are required to confirm these results.
Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory disorder characterised by symmetrical polyarthritis that affects both small and large joints. This leads to cartilage destruction and bone erosion, especially in seropositive patients. Uncontrolled diseases can lead to deformities and functional impairments. However, not all patients with RA progress at the same rate. Some patients have indolent courses, while others progress rapidly. An increasing body of evidence suggests that early initiation of treatment before the disease process has been established can prevent permanent damage and improve overall outcomes. 1 To recognise these patients at an early stage, we need some predictors to titrate and optimise treatment. Moreover, the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria help diagnose RA early. 2 In order to target treatment appropriately (under treatment) and avoid exposing patients with mild disease to potentially toxic drugs (overtreatment), it would be helpful to predict at baseline which patients are likely to develop erosive RA.
Several retrospective and prospective studies have identified possible baseline predictors associated with the worst outcome (erosive disease) in early RA (ERA).3–7 However, the prediction accuracy for erosive disease of these individual factors is low. There are many discrepancies between studies that explain the current lack of internationally accepted prognostic criteria for RA. Furthermore, there is a scarcity of Indian data regarding the predictors of erosion in ERA. Therefore, the present study was conducted.
Materials and Methods
All consecutive patients with ERA (disease duration ≤six months),8, 9 satisfying the 2010 ACR criteria, seen in the rheumatology OPD of a tertiary care hospital in western India, were enrolled in this prospective open-labelled clinical observational study. The enrolment period was six months (October 2012 to March 2013). The patients were followed up for one year (up to March 2014). All the patients provided informed consent to participate in the study. The study was approved by the Institutional Review Board (704-12-CB/Date 10 December 2012). All included patients were treatment-naïve and were above 18 years of age. Patients with RA who had overlapping inflammatory conditions, hyperthyroidism, bisphosphonate use or alternative medication therapy were excluded.
Sample Size
Sample size calculation was performed using SPSS version 10.0. Based on previous studies,10, 11 the proportion of radiological progression was 41.3% with an accepted margin of 15%.
Based on the above assumptions, a sample size of 112 cases would be needed to assess the study objective at 80% power and a 5% level of significance. Considering a 20% dropout rate, we calculated that 140 patients should be enrolled in this study.
Evaluation
Patients included in the study were evaluated at each visit (0, 3, 6, 9 and 12 months). At baseline, the patient’s demographic data, including age, sex, disease duration and clinical details, including duration of morning stiffness, co-morbidities, family history of RA or connective tissue disorders and extra-articular features, were recorded. The patient’s weight, blood pressure and respiratory, cardiovascular, and abdominal examinations were performed at each visit as part of routine care.
Disease Activity and Functional Assessment
Disease activity was assessed using the Disease Activity score 12 (DAS 28 ESR) at each visit. Functional status was assessed by the Indian Health Assessment Questionnaire (HAQ) at baseline and at each visit. 13
Laboratory Parameters
CBC, ESR (0–15 mm/h) using the Westergren method, Serum Glutamic Pyruvic Transaminase (SGPT) and serum creatinine were performed at baseline and at every follow-up visit. Rheumatoid Factor (RF) (range 0–20 µ/L, by latex agglutination) and anticitrullinated protein antibody (ACPA) (range 0–15 µ/L, by ELISA) were performed at baseline. CXR (PA) was performed at baseline in all patients. X-rays of the hands with wrists (PA view) and feet (PA view) were performed at baseline and at the end of one year for all patients.
Treatment
All the patients were treatment-naïve. Along with Disease-Modifying Anti-Rheumatic Drugs (DMARD), either a single intramuscular dose of methylprednisolone 120 mg intramuscularly or a short course of Non-Steroidal Anti-Inflammatory Drugs (NSAID) was administered as bridging therapy.
Oral or subcutaneous methotrexate was administered at a dose of 15 mg/week, which was increased to 25 mg/week in cases of an inadequate response. Leflunomide (10–20 mg/day), hydroxychloroquine (200–400 mg/day) or sulfasalazine (1.5–3 g/day) was added to the anchor drug methotrexate if the disease activity was persistent or was used as the first drug in case of methotrexate intolerance or contraindication. A combination of any of these three DMARDs with methotrexate was used, and a triple-drug combination was also allowed, as judged appropriate by the treating rheumatologist. At every visit, treatment was assessed and modified if required. Intramuscular methylprednisolone 120 mg, oral steroid taper, or a short course of NSAID was used as treatment during flares.
Radiological Assessment
X-rays were evaluated according to van der Heijde’s modification of Sharp score (SvdH). 14 Radiologic progression, according to the outcome measures in RA clinical trials committee recommendations, 15 was defined by a change in radiologic scores of at least 3.2, 2.9 and 3.4 in the erosions score, narrowing score and total Sharp score, respectively. Radiographic progression was computed by subtracting the initial SvdH score from the one-year SvdH score. Scoring was performed at the end of one year by a single rheumatologist (experienced in RA radiology) who was blinded to the X-ray sequence. Intraobserver variability in radiographic assessment was limited by the fact that the same experienced rheumatologist assessed the radiographs both at baseline and follow-up.
Outcome
Primary Outcome
To determine the progression of radiographic damage at one year, defined 15 as a change in radiologic score of at least 3.2, 2.9 and 3.4 in the erosion score, joint narrowing score and total damage score, respectively, and to identify baseline variables predicting this radiological damage progression.
Secondary Outcome
Improvement in DAS 28 (ESR) scores ( <2.6 defined as remission) with treatment.
Improvement according to EULAR response criteria (good/moderate/no response) in RA. 16
Improvement in Indian HAQ scores 13 with treatment (HAQ scores 0–3). HAQ was further classified as (≤1 mild functional disability), (1.01–≤2 moderate functional disability) and (>2 severe functional disability). Minimal Clinically Important Difference (MCID) was defined as 0.22.
Statistical Methods
Statistical analyses were performed using the SPSS version 10.0. Outcome variables were dichotomised into qualitative variables: presence or absence of radiological progression. Univariate analysis of the relationship between all baseline values and outcome measures was performed using the chi-squared test. All continuous baseline variables (disease duration, age of onset, duration of Early Morning Stiffness (EMS), number of tender joints, swollen joints, DAS 28 and ESR) were converted to categorical variables, using median values as the cut-off point. RF/ACPA status and baseline radiographic damage (erosion or joint space narrowing [JSN]) were entered as categorical variables (present or absent). RF and ACPA titres were converted to categorical variables using a value of >three times the ULN 2 -RF (>60 IU), ACPA (>45 IU) and Indian HAQ score >1 as the cut-off points. The prognostic variables included in the multivariate model were selected using univariate analysis (p < .20). A stepwise multiple logistic regression model was used to identify relevant independent prognostic variables. The Student’s t-test for numerical data and the chi-square test for comparison of categorical data were applied (p < .05 was taken as significant).
Results
Of the 84 patients screened, 63 patients satisfying the inclusion criteria were assessed during the six months. These patients were followed up for one year. Of these, 12 patients were excluded from the analysis—(six patients discontinued after two follow-up visits, three switched to alternative treatment, one went into remission after two months and discontinued treatment and two outstation patients could not follow-up regularly). In 51 (81%) patients completed the study. Of these 51 patients, radiographs at baseline and one year were available for 43. In 8 (15%) patients, one-year radiographs were incomplete or missing; thus, data for 43 (75%) patients were available for radiologic analysis, while for all other outcomes, 51 patients were analysed.
Demographic Data
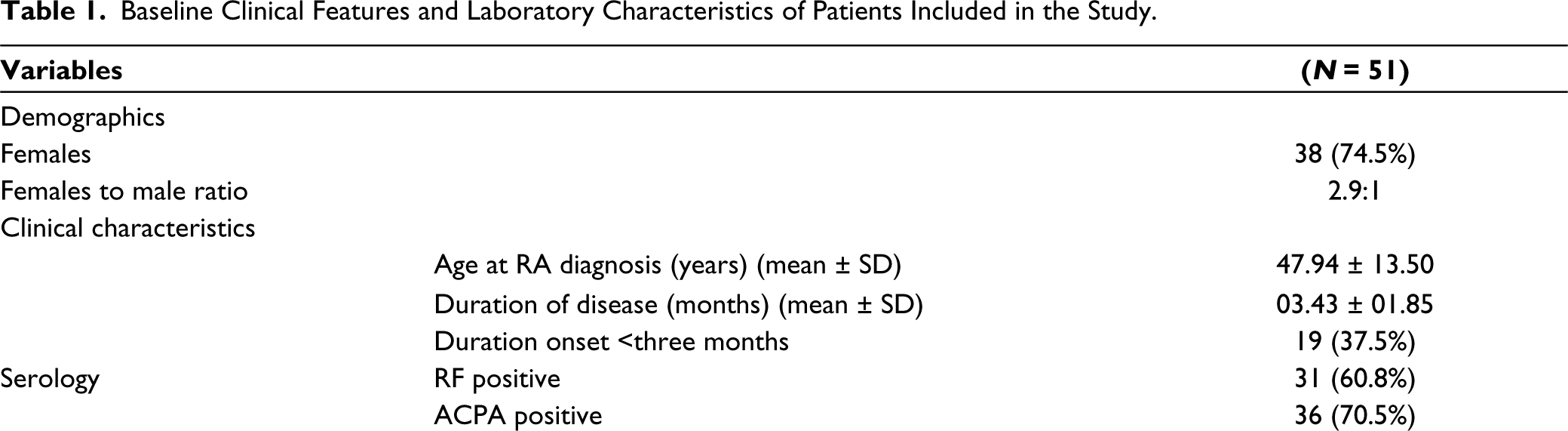
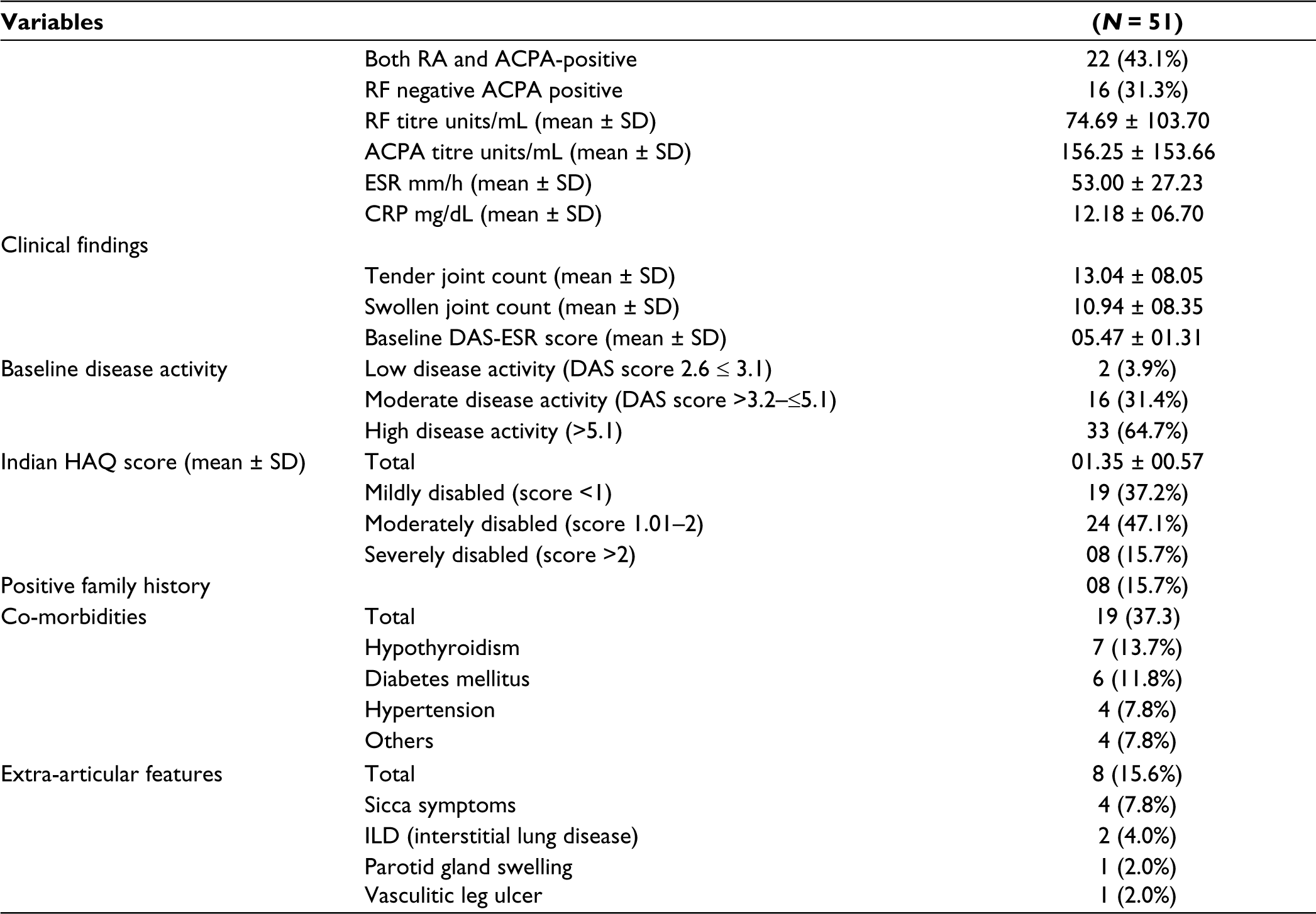
Of the 51 patients, 38 (74.5%) were female and 13 (25.5%) were male. The female-to-male ratio was 2.9:1. Co-morbidities were present in 19 patients (37.2%). The most common co-morbidity was hypothyroidism (13.7%) followed by diabetes mellitus (7.8%). Various extra-articular features alone or in combination were present in 8 patients (15.6%). The most common extra-articular manifestation was sicca symptoms in 4 (7.8%) patients.
Baseline Disease Status
The baseline characteristics of the patients included in the study are shown in Table 1. This cohort of patients with ERA had a disease duration of less than six months. The mean duration to the onset of RA was 3.4 ± 1.85 months. RF and ACPA were positive in 60.7% and 70.5% of the patients, respectively. All patients had active RA at baseline, with 49 (96.1%) having moderate to high disease activity. The mean DAS 28 (ESR) score was 5.4 ± 1.31. The mean Indian HAQ score was 1.35 ± 00.57, with 32 (62.8%) having moderate-to-severe disability. At baseline, 16.3% of patients had erosions, and 21% had JSN with a baseline total Sharp score (TSS) of 1.37 ± 2.34.
Baseline Clinical Features and Laboratory Characteristics of Patients Included in the Study.
DMARDs Treatment
At baseline,65% were on monotherapy, and 36% were on combination DMARD treatment. Of the 33 (65%) patients on monotherapy at baseline,13 (40%) remained on monotherapy, while 20 (60%) were stepped up for combination treatment. Most of the patients who stepped up to combination treatment did so at the three-month visit. Overall, 25% of the patients continued only with monotherapy throughout the study, while 35% of the patients who were started on combination DMARDs continued in the same group at one year.
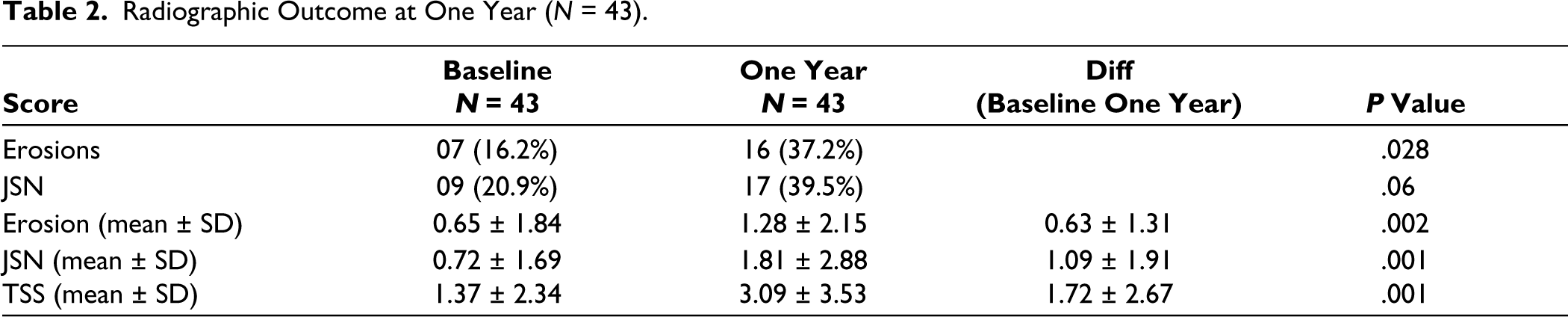
Radiological Progression (Table 2)
At baseline, 16.3% of the patients had erosion, increasing to 37.2% at one year, whereas those with JSN increased from 21% to 39.5% at one year. Radiologic progression was observed in 14 (32.5%) patients, defined by a change of at least 3.2, 2.9 and 3.4 in the erosion score, narrowing score and total Sharp score, respectively. Progression occurred in 9 (20.9%) patients according to the total Sharp score, in 4 (9.3%) patients as indicated by the erosion score, and in 12 (27.06%) patients as demonstrated by JSN. The mean TSS progression at one year was 1.67.
Radiographic Outcome at One Year (N = 43).
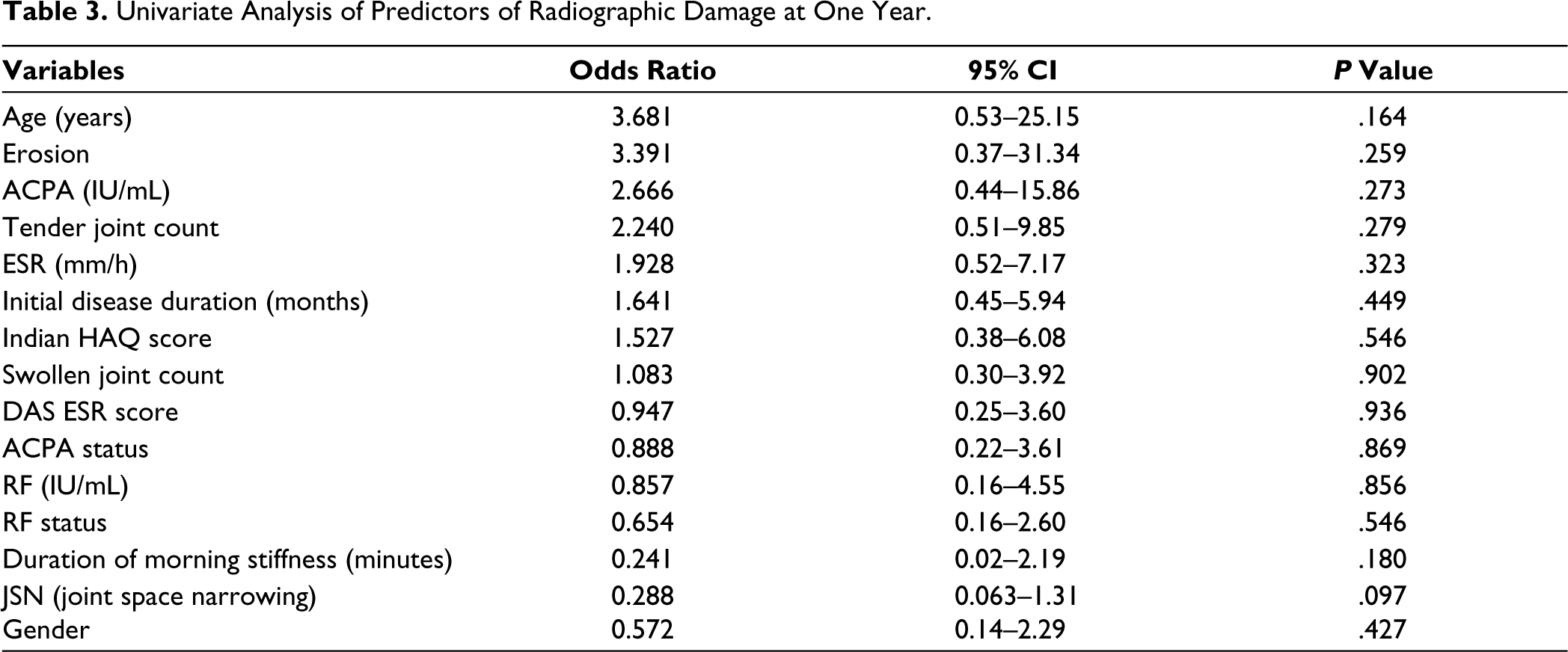
Predictors of Radiological Damage (Tables 3 and 4)
Univariate analysis was used to identify baseline variables that predicted radiological progression, and those with p < .20 were entered in logistic regression. The association between the age of onset (odds ratio 3.68), presence of erosion at baseline (odds ratio 3.39), ACPA titre (odds ratio 3.39), tender joint count at baseline (odds ratio 2.24) and radiological progression was noted and, to a lesser extent, with ESR (mm/h) (odds ratio 1.928), disease duration (odds ratio 1.641) and the Indian HAQ score (odds ratio 1.527). None of these variables were statistically significant. Only JSN at baseline showed a marginal trend (p = .097) towards significance in the univariate analysis.
Univariate Analysis of Predictors of Radiographic Damage at One Year.
Logistic Regression Analysis of Predictive Factors of Radiological Progression.

JSN at baseline, age at onset and duration of morning stiffness were factors identified by univariate analysis, with p < .20 and were entered into the multivariate analysis. However, none of these factors independently predicted radiographic progression using multivariate analysis. Only JSN at baseline was positively associated with radiographic progression but did not reach significance.
Clinical and Functional Outcomes at 12 Months
The mean DAS 28 score decreased significantly from 5.47 at baseline to 3.22 at 12 months (Figure 1A). The Indian HAQ score decreased significantly from 1.3 at baseline to 0.51 at one year (Figure 1B). At 12 months, 43 patients (84.5%) achieved a significant decrease in the Indian HAQ score (MCID = 0.22). At one year, 27.5% of patients achieved remission, 25.5% achieved low disease activity, and 24 (40.7%) patients had moderate (MDA) to high (HIDA) disease activity.
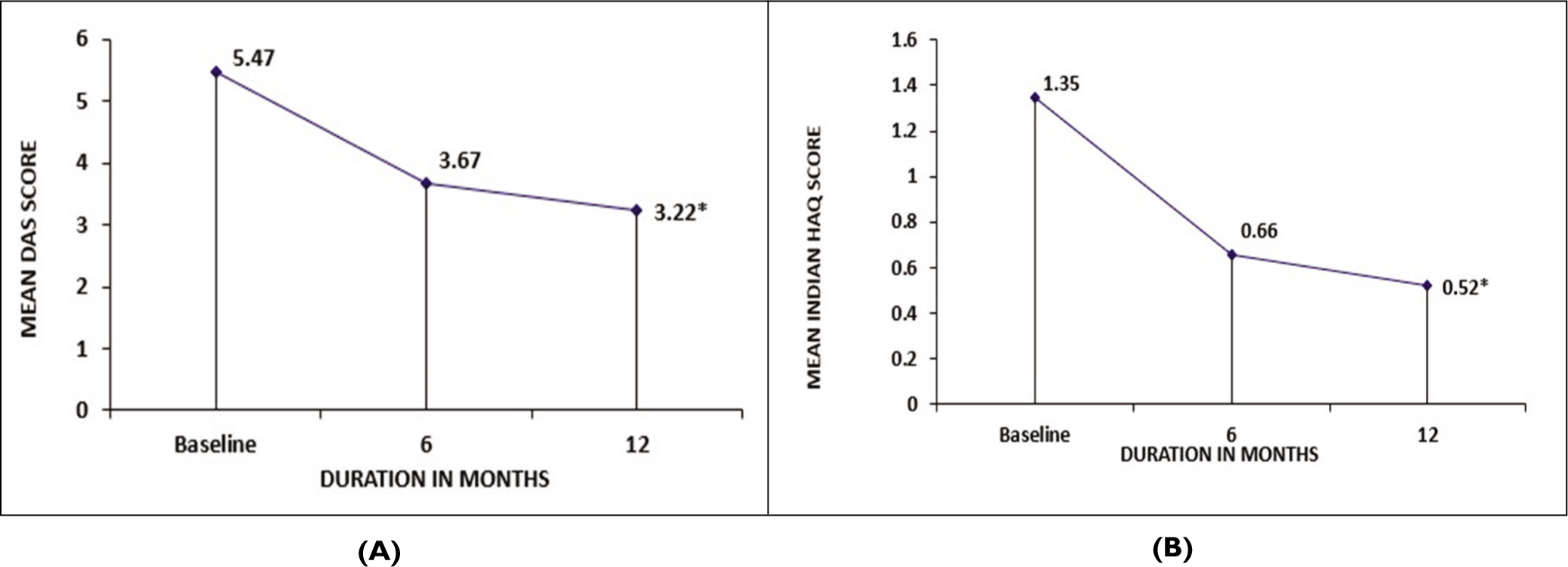
(A) Change in Mean DAS Score at 6 and 12 Months.
Discussion
This study enrolled a cohort of ERA patients with less than six months of disease duration. The majority of the patients had moderate to severe disease activity and moderate to severe functional impairment, as reported by other studies.4, 17 The demography, clinical features and baseline laboratory tests were as expected, with some significant differences due to the variable study design. Our cohort was slightly older, 18 had more morning stiffness4, 6 and more ACPA positivity. 19
Despite early disease, approximately 20% had radiological damage at baseline. The presence of erosions in our study’s ERA patients was influenced by the limitations of the ACR/EULAR 2010 criteria and the challenges in accurately diagnosing ERA. The ACR/EULAR criteria have limitations in terms of their sensitivity and specificity. The presence of erosions at baseline in our study highlights this limitation and justifies the use of the EULAR definition of erosive disease. 20 It is important to note that the duration of three to six months for diagnosing RA does not guarantee the absence of erosions, as studies have shown erosions developing as early as eight weeks with advanced imaging techniques. Additionally, recall bias in reporting symptoms and disease duration can affect diagnostic accuracy. Despite these limitations, we included patients with erosions based on standardised symptom onset criteria, providing valuable insights into ERA management and disease progression.
The baseline erosion, JSN and total Sharp scores were much lower than those in other studies.6, 21 The probable reason for the much higher baseline SvdH scores in the other studies could be twofold: first, these studies have included patients with disease duration <one year rather than <six months, which is the inclusion criteria in this study and second, RA in these other studies was diagnosed based on 1987 ACR criteria, where the presence of radiological damage was required for diagnosis in contradistinction to the 2010 ACR criteria used here.
Progression during the first year is a strong predictor that should be considered when treating and monitoring RA patients. At one year, 32.5% of the patients had radiological progression comparable to the 25%–35% reported in other studies.22, 23 At one year, the mean TSS progression was 1.67, which is comparable to the value of 1.60, as observed in the study by Fautrel et al. 22 A few other studies4, 17 have shown higher progression at one year, which may be related to differences in treatment or inclusion criteria.
Despite the small sample size, this study shows a possible association of some of the factors (erosion/JSN at baseline, age of onset, ACPA titre and tender joint count) with radiographic damage. However, only JSN at baseline showed a positive association (OR, 3.39) with radiographic progression at one year, and none of these variables were statistically significant.
Baseline JSN was associated with a non-significant trend p = .09 in univariate analysis but not in multivariate analysis. Early radiologic abnormalities 6 (erosions or JSN) have been related to a more severe disease course in many studies and have been considered important markers because of their predictive value for both long-term radiologic damage and long-term functional impairment.17, 23 However, none of these factors independently predicted radiographic progression using multivariate analysis.
Over a one-year follow-up period, only 25% stayed on monotherapy, and most had another DMARD added during follow-up. At one year, although most responded to the prescribed treatment regimens, more than 40% continued to have moderate disease activity (DAS 28—3.2–5.1). Overall, 85% of patients in the monotherapy group and 66% in the combination DMARD group achieved low disease activity compared with 15% in the step-up group at one year. The mean value of the Indian HAQ was reduced significantly one year after DMARD treatment.
There has been no consensus regarding the poor prognostic factors of rheumatoid, as there is no universally accepted definition for ERA, which can last anywhere from six months to five years. 24 Also, most of the studies done in the past for evaluating predictive factors in ERA used the ACR 1987 criteria.4, 22, 25 However, these criteria do not perform well in ERA. 26 Our study is one of the few studies that have used the 2010 ACR/EULAR criteria for RA patients, thus reflecting truly ERA patients.
The limitations of the study include a small sample size, which reduced the statistical power for multivariate analysis. In addition, the study did not account for some other confounding parameters that may have contributed to radiological progression, including obesity, smoking and age. Another limitation is that a single reader scored the radiographs. Additionally, the study is a decade old, which limits the ability to generalise its results to current clinical practice. However, the strengths of our study are the structured longitudinal follow-up, ACR 2010 criteria for cohort, and pragmatic study setting for clinical practice.
Conclusions
In conclusion, this is the few Indian study that has looked at radiological progression in patients with ERA. Approximately 32.5% of our patients had radiological progression at one year. Age of onset, presence of erosion, JSN, ACPA titre and tender joint counts at baseline were associated with radiographic progression at one year; however, none of these reached statistical significance in the multivariate analysis. Further studies are required to confirm these results. Significant improvements were also noted in the DAS 28, EULAR response and Indian HAQ. Most of the patients achieved good response at one year with DMARD treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable
Funding
The authors received no financial support for the research, authorship and/or publication of this article.