
Abstract

A 35-year-old lady consulted us in 2022 for the inflammatory type of back pain of 4 years duration, positive HLA B27 and bilateral inflammatory sacroiliitis on MRI (Figure 1). She improved at that time with two to four weeks of treatment with anti-inflammatory medications. A year later she developed severe pain in the left groin region. On examination, there was pain near the left pubic symphysis on resisted adduction of left hip adductors. ESR was 72 mm/hour. Repeat MRI of the pelvis (Figure 2a and b) showed ill-defined enhancing oedema seen in the left pubic bone in the entire anterior to the posterior extent and in the enthesis of the origin of the pectineus, obturator externus and adductor brevis muscles, focal T2 weighted intermediate signal intensity thickening of the adductor longus tendon and subtle asymmetrical soft tissue thickening along the inferior aspect of the junction of the body and the superior pubic ramus on the left side at the enthesis. There was no focal collection, erosion, destruction or fracture. The right pubic bone was unremarkable. All these were suggestive of left pubic bone enthesitis. As this had not responded to two weeks course of NSAIDS, she was given tofacitinib 5 mg BD, to which there was significant clinical improvement in a few weeks. Repeat MRI (Figure 3a and b) done three months later showed a significant reduction in the previously seen ill-defined T2 hyperintensity and enhancement in the left pubic bone, there were residual smaller signal changes with mild irregularity and linear signal changes mainly in the anterior portion of the pubic bone and the hyperintensity and enhancement in the adjacent muscles.
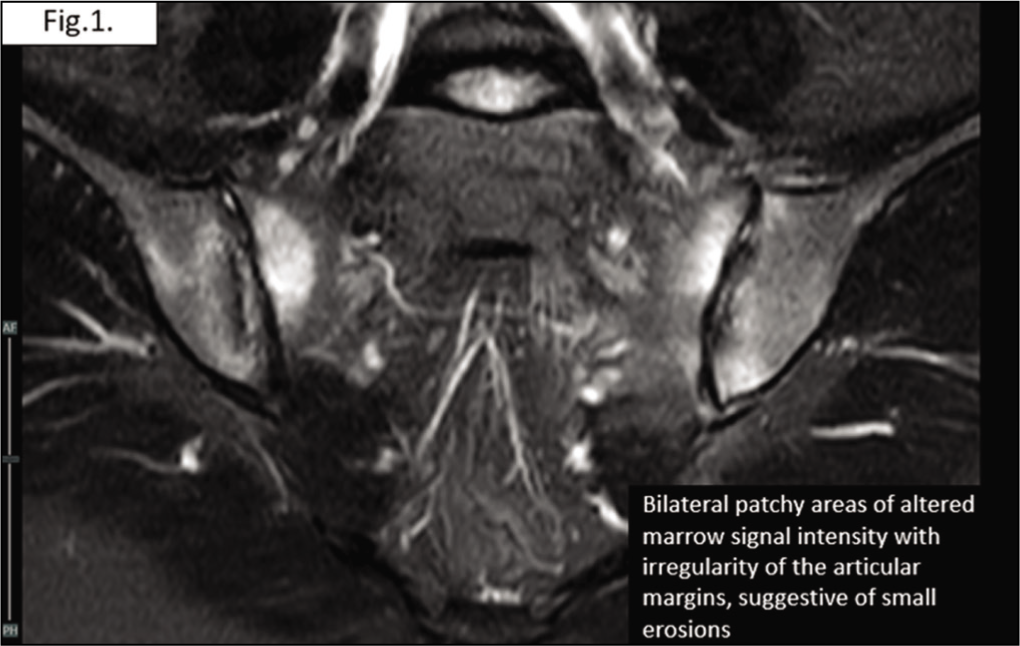
MRI of Sacroiliac Joints was Suggestive of Bilateral Patchy Areas of Altered Marrow Signal are Seen Adjacent to the Sacroiliac Joints, Which Show Irregularity of the Articular Margins, with Possible Small Erosions, Findings Suggest of Bilateral Inflammatory Sacroiliitis.
MRI Showed Ill-defined Enhancing Oedema is Seen in the Left Pubic Bone in the Entire Anterior to Posterior Extent and in the Enthesis of the Origin of the Pectineus, Obturator Externus and Adductor Brevis Muscles. Focal T2 Weighted Intermediate Signal Intensity Thickening of the Adductor Longus Tendon is Noted. Subtle Asymmetrical Soft Tissue Thickening Along the Inferior Aspect of the Junction of the Body and the Superior Pubic Ramus on the Left Side at the Enthesis. No Focal Collection. No Erosion or Destruction. No Obvious Evidence of Fracture. The Right Pubic Bone Appears Unremarkable. Finding Suggestive of Left Pubic Bone Enthesitis (a & b).

MRI Showed a Significant Reduction in the Previously Seen Ill-defined T2 Hyperintensity and Enhancement/Oedema in the Left Pubic Bone, Now Showing Residual Smaller Signal Changes with Mild Irregularity and Linear Signal Changes Mainly in the Anterior Portion of Pubic Bone. The Surrounding Hyperintensity and Enhancement in the Adjacent Muscles have Also Significantly Reduced (a & b).

Enthesis is now thought of to be an ‘organ’ and is one of the prime sites where inflammation is thought to originate in patients with spondyloarthropathy (SpA). 1 Enthesitis occurs in up to 41% of patients, especially with axial SpA. 2 Characteristic pathology at the enthesis, in SpA, consists of inflammation of the enthesis coupled with adjacent inflammatory non-infectious bone oedema called osteitis. The importance of enthesitis in SpA can be gauged by the fact that many composite scoring systems for SpA also have a section for it. 3
Multiple muscles attach themselves to the pubic bone and pubic symphysis (Figure 4), making it an important site for enthesitis. In the past, NSAIDs were the mainstay for the treatment of enthesitis, as conventional DMARDs had a negligible effect on it. 4 However with the advent of biologic DMARDs, the prognosis of patients with enthesitis has improved. Anti-TNF and IL-17 inhibitors have both been well-documented to control enthesitis. 5
Various Muscular Attachments Around the Pubic Bone and Symphysis Pubis.

Recently JAK inhibitors have also been shown to help control enthesitis. 6 In our patient, whose pubic symphisitis was resistant to NSAIDS, Tofacitinib controlled the inflammatory symptoms and also reduced the need for NSAIDS. Further, on repeat MRI imaging, it was heartening to see the significant resolution of the active bone marrow oedema. In Indian settings, since Tofacitinib is an oral formulation and is far cheaper than other biologic DMARDs, it should probably be tried first for patients with SpA and resistant enthesitis.
Footnotes
Author Contributions
Contributed to the case. Contributed to radiology image reporting. Contributed to the discussion writing, and treatment of the patient and mentor.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Informed consent was obtained from the patient and is included in the text.