
Abstract
Epidemiological studies, referred to as the Community Oriented Program for Control of Rheumatic Diseases (COPCORD) studies, have been conducted under the aegis of the International League against Rheumatism and the World Health Organization to evaluate the epidemiology of rheumatic and musculoskeletal (RMSK) diseases in India. These COPCORD studies conducted in rural Bhigwan and urban Pune in Maharashtra, rural Calicut and rural Trivandrum in Kerala and rural and urban Lucknow in Uttar Pradesh, along with data from the Global Burden of Diseases study have helped to understand the burden of rheumatic diseases in the community. Based on these studies, RMSK diseases, which are amongst the top 25 causes of disability in the Indian population, are prevalent in nearly 25%–30% of the Indian population. The common rheumatic diseases in the community are soft tissue rheumatism, neck and back pain, fibromyalgia and unspecified pains and osteoarthritis (most commonly affecting the knee). These diseases most commonly affect young persons between the third to the fifth decade of life, more often affect females, are prevalent in both rural and urban populations, and account for considerable disability in up to one-fifth of individuals leading to loss of livelihood and dependence on others for self-care. Community-based national healthcare programs to manage RMSK diseases at the community level are urgently needed. There also remains an unmet need to train more doctors to diagnose and manage rheumatic diseases at the primary, secondary and tertiary levels of care.
Keywords
Introduction
Rheumatic diseases refer to diseases affecting the musculoskeletal system, namely joints, soft tissues and bones, where the cause is other than trauma. Such diseases might additionally affect the other organs of the body such as the kidneys, skin, lungs and nervous system.1–3 An aberrantly active immune system whose detrimental influences are exacerbated by increasing age (inflammaging) underlies the basis of a considerable proportion of these diseases. 4 Rheumatic diseases disproportionately affect young individuals who are the most productive towards society. Rheumatic diseases are a major cause of morbidity in the population. With an increasingly ageing population, diseases like osteoarthritis which predominantly affect older adults are also increasingly a cause of disability and impaired quality of life. 5
In this review, we assess the prevalent literature regarding the epidemiology of rheumatic diseases in India. The purpose of this white paper is to highlight the disease burden of musculoskeletal diseases in India to understand the need for advocacy and public health programmes for the control of musculoskeletal diseases in the community.
The Overall Burden of Musculoskeletal Diseases
The Global Burden of Diseases (GBD), Injuries and Risk Factors Study is currently the major source to assess the burden of communicable and non-communicable diseases (NCDs) across the world, including from India. Periodic updates to the GBD data enable the assessment of secular trends of risk factors for both communicable diseases as well as NCDs. Data from the GBD studies was collected through questionnaires and hospital-based registries of diseases. A major update to the GBD published in 2017 reported the prevalence of musculoskeletal complaints as 1,312,131.3 thousand, the annual incidence as 334,744.9 thousand and the disability-adjusted life years (DALYs) lost due to these diseases as 135,881.3 thousand years. DALYs due to musculoskeletal complaints have progressively increased over time, by 38.4% from 1990 to 2017 (within this period, by 19.9% from 2007 to 2017). The major prevalent musculoskeletal disorders were low back pain (576,989.9 thousand) followed by osteoarthritis (303,096.5 thousand, most commonly osteoarthritis of the knee), neck pain (288,718.6 thousand) and others (rheumatoid arthritis [RA], gout, other musculoskeletal disorders). The DALYs attributable to each of these diseases had also increased significantly between 1990 and 2017 and between 2007 and 2017. 6 Thus, the overall burden of musculoskeletal diseases is increasing worldwide with time.
Analysis of secular trends in DALYs was published in 2017 as well as the 2019 updates of the GBD.6, 7 In the GBD 2019, the contribution of different causes by rank as per age group (overall, 0–9, 10–24, 25–49, 50–74, ≥75 years) was presented (Table 1). 7 Overall, the contribution of low back pain and other musculoskeletal complaints to the DALYs increased from 1990 to 2019. Low back pain was a leading cause of disability upwards of 10 years of age, maximum at the age group of 25–49 years. Musculoskeletal complaints other than low back pain, neck pain, RA, osteoarthritis and gout were a leading cause of disability between 25 and 74 years, maximum between the ages of 25–49 years. 7 Thus, musculoskeletal diseases contribute the maximum to disability during the most productive years of life.
Secular Trends in the Contribution of Musculoskeletal Disorders as Leading Causes of DALYs. 7
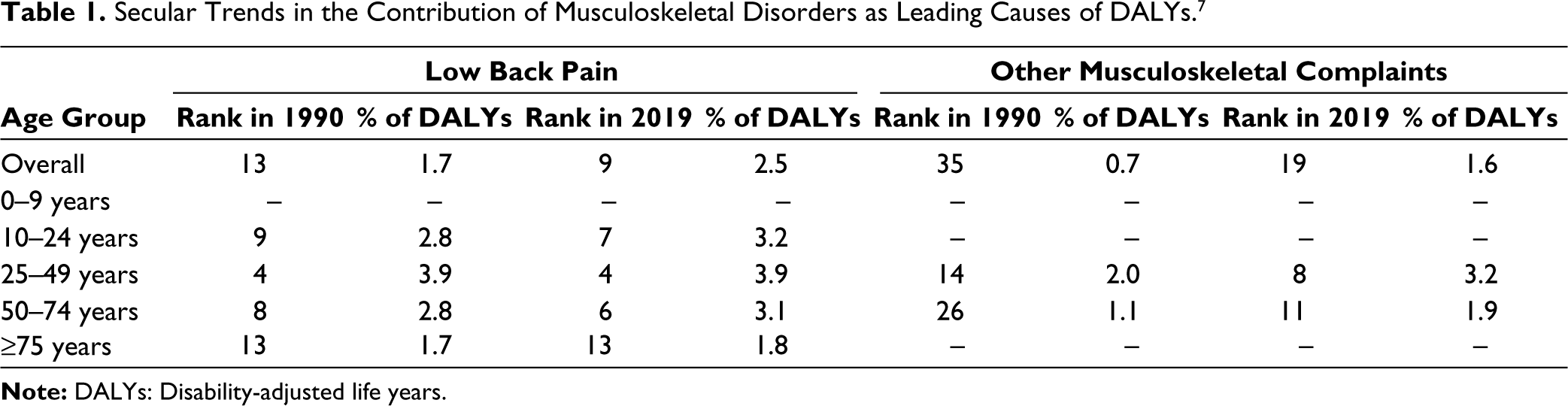
Further analysis of the GBD data reported the key risk factors for DALYs between 1990 and 2016 from India. Of these, low physical activity (rank 14 in 1990, rank 15 in 2016, overall increase of 109.6% between 1990 and 2016) and low bone mineral density (rank 16 in 1990, rank 16 in 2016, overall increase of 127.4% between 1990 and 2016) were directly related with musculoskeletal diseases. Of note, musculoskeletal diseases contributed only 0.1% to the overall mortality due to the various chronic diseases. 8 Thus, individuals with musculoskeletal diseases survive and continue to have a disability. The fact that musculoskeletal diseases majorly affect the populace in the most productive years of their life (25–49 years) emphasises the public health importance of these disorders.
Community Oriented Program for Control of Rheumatic Diseases (COPCORD) and Bhigwan Model of COPCORD
The epidemiology of rheumatic diseases has been scarcely studied beyond the developed world. In this context, the International League of Associations for Rheumatology in conjunction with the World Health Organization launched the COPCORD about four decades back. The intention of COPCORD was to assess the burden of rheumatic and musculoskeletal (RMSK) complaints in the community. 9 Utilising a standardised approach, three stages were laid out. Stage I (comprising three phases in turn) focused on the identification of the burden of RMSK symptoms in the community. Phase I focused on identifying those with RMSK symptoms. Phase II focused on identifying the burden of pain and disability due to RMSK symptoms. Phase III intended to provide a diagnosis for RMSK symptoms after assessment by a rheumatologist. Stage II intended to provide education for rheumatic diseases and assess risk factors for the same in the community. Stage III was meant to develop and implement strategies to manage rheumatic diseases in the community.9, 10
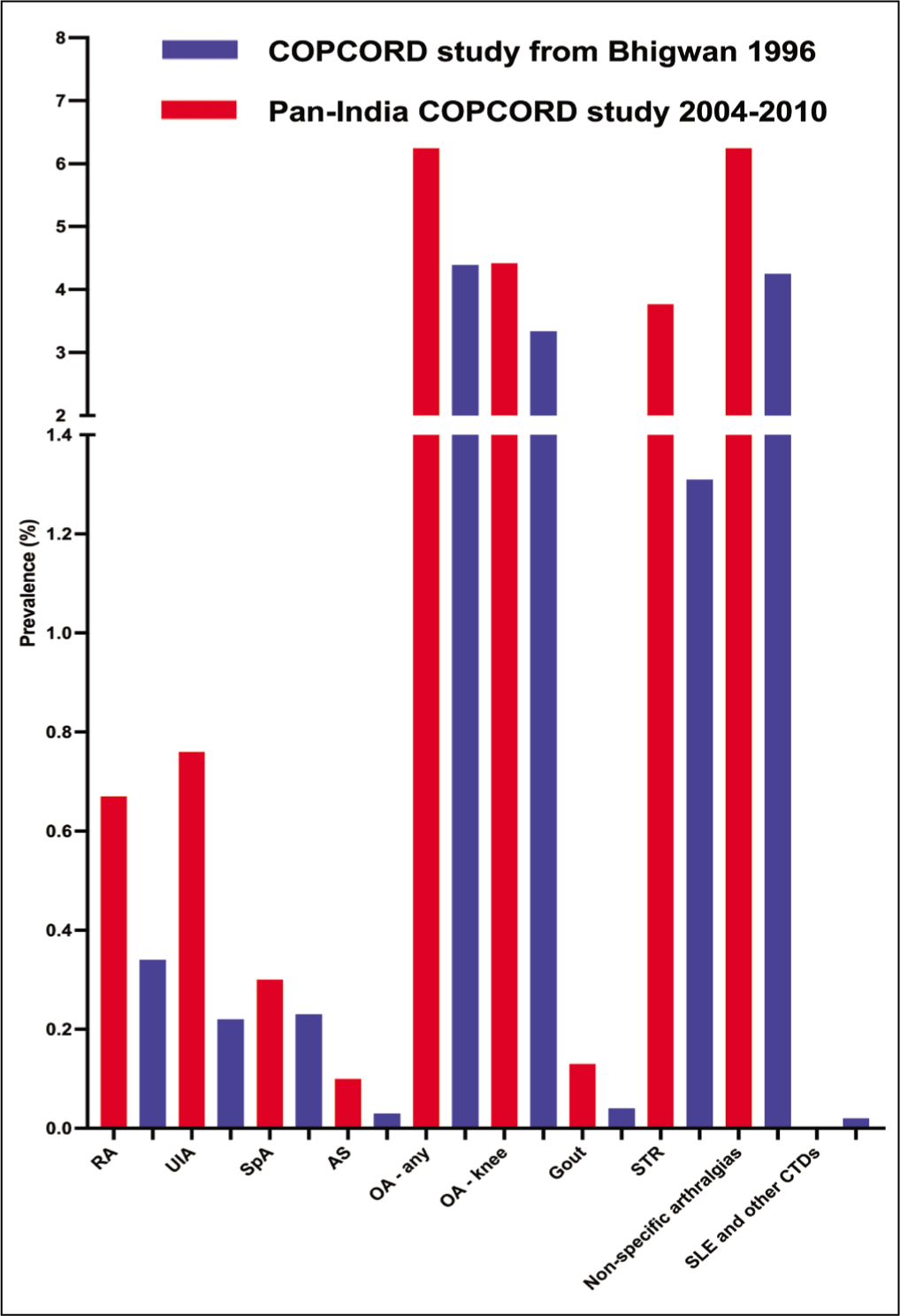
The COPCORD model was pioneered in India by Dr Arvind Chopra in Bhigwan, Maharashtra. What was unique about the Bhigwan model of COPCORD was that all three phases of stage I (from case identification to rheumatologist assessment for diagnosis) were carried out in parallel in a fast-track manner. This provided a quick mechanism to establish the burden of rheumatic diseases in a particular community. The adoption of the Bhigwan model in different parts of India has enabled a more efficient assessment of the epidemiology of these diseases.10–13 Figure 1 summarises the prevalence of different rheumatic disorders in India based on the COPCORD studies. 13
Overall Rheumatic Musculoskeletal Symptoms and Pain
The COPCORD study from Maharashtra compared 4,092 individuals (aged >16 years) from the Bhigwan rural cohort with 8,145 from urban Pune. After adjustment for the age and sex distribution of the population, pain at any site was reported by 11.50 (95% confidence interval [95%CI] 11.03–11.92)% from urban Pune and 19.50 (95%CI 18.97–20.07)% from rural Bhigwan in Maharashtra. 14 The overall age- and sex-standardised prevalence of RMSK from a population-based study of 4,999 individuals aged ³15 years from a rural area of Calicut district, Kerala, was 24.57 (95%CI 23.40–25.78)%. 15 From another population-based study of 5,277 individuals older than 15 years from rural Trivandrum, Kerala, the prevalence of musculoskeletal pain was 30.13 (95%CI 29.09–31.17)%. 16 From a population-based study from Uttar Pradesh involving 5,053 individuals from urban Lucknow and 5,118 individuals from rural Lucknow, the prevalence of musculoskeletal pain was 15.1% in rural and 34.1% in urban areas. 17
Osteoarthritis
Analysis of GBD data up to 2016 from India revealed that osteoarthritis was the 16th leading cause of disability amongst the Empowered Action Group states, 14th amongst North-Eastern States and 14th among other states. 18 A further analysis of GBD data up to 2019 including new information from a systematic review of other studies regarding the epidemiology of osteoarthritis in India was recently published. The prevalence of osteoarthritis in 1990 was 234.6 lakh and in 2019 was 623.5 lakh. The annual incidence of osteoarthritis in 1990 was 22.5 lakh and in 2019 was 54.6 lakh. The age-standardised incidence ratio for osteoarthritis increased by 8% from 1990 to 2019. DALYs due to osteoarthritis also increased from 7.9 lakh in 1990 to 21.2 lakh in 2019. A similar increase in age-standardised DALYs between 1990 and 2019 by 10% was also noted. The increase in age-standardised incidence ratios and DALYs suggests that the actual burden of osteoarthritis in India is increasing with time, rather than simply being an artefactual change due to changes in the age structure resulting in an increasingly ageing population. When ranked as a contributor to years lived with disability (YLD), osteoarthritis ranked 23rd in 1990, increasing to 20th in 2019. The prevalence, incidence, DALYs and contribution towards YLD were consistently greater for females than for males. The knees were most commonly affected by osteoarthritis followed by the hands. 19
Another study evaluated 5,000 individuals aged at least 40 years without any known rheumatic diseases from each of the different zones of India (Central, East, South, North, West) for radiographic knee osteoarthritis (Kellgren Lawrence grading ≥2). This study reported knee osteoarthritis in 28.7% of subjects. Female sex, higher body mass index, older age and decreased physical activity are all associated with a greater prevalence of osteoarthritis on univariable analysis. 20 The population-based study from Calicut district, Kerala reported the age- and sex-adjusted prevalence of osteoarthritis as 3.85 (95%CI 3.35–4.42)%. 15
Few studies have compared the prevalence of osteoarthritis between urban and rural communities in India. The population-based study from Maharashtra reported a greater age- and sex-adjusted prevalence of osteoarthritis in rural (6.25 [95%CI 5.92–6.60]%) than in urban areas (4.01 [3.74–4.29]%). In both areas, knee osteoarthritis was the most common followed by lumbar spine osteoarthritis. 14 Contrary to these findings, the population-based study from Uttar Pradesh reported a greater prevalence of knee osteoarthritis in urban Lucknow (106.07 per 1,000 population) than in rural Lucknow (44.9 per 1,000 population). 21
Soft Tissue Rheumatism
From the population-based study from Maharashtra, the age- and sex-adjusted prevalence of soft tissue rheumatism was 1.20 (95%CI 1.05–1.36)% in urban areas and 3.77 (95%CI 3.51–4.05)% in urban areas. 14 From the population-based study from Calicut district, Kerala, the age- and sex-adjusted prevalence of soft tissue rheumatism was 2.14 (95%CI 1.78–2.58)%. 15
Fibromyalgia
From the population-based study from Lucknow, the prevalence of fibromyalgia was 41.2 per 1,000 in urban and 32.4 per 1,000 in rural populace. 21
Neck Pain and Backache
From the population-based study from Maharashtra, after age and sex adjustment, neck pain was prevalent in 1.90 (95%CI 1.77–2.05)% in urban Pune and 6.80 (6.48–7.19)% in rural Bhigwan. Low back pain was prevalent in 4.60% (95%CI 2.05–5.50)% in urban and 12.60 (12.14–13.16)% in rural areas. Upper back pain was prevalent in 1.70 (95%CI 1.50–1.86)% in urban and 8.40 (7.99–8.77)% in rural populace. 14 Spine-related symptoms (after age and sex adjustment) were reported by 1.23 (0.96–1.57)% of the rural population from Calicut district, Kerala. 15 From the population-based study from Lucknow, the prevalence of neck pain was 1.36 per 1,000 from rural and 21.7 per 1,000 from urban areas. The prevalence of back pain was 36.5 per 1,000 from rural areas and 106.6 per 1,000 from urban areas. 21
Unspecified Aches and Pains
From the population-based study from Maharashtra, the age- and sex-adjusted prevalence of unclassifiable aches and pains was 5.01 (95%CI 4.71–5.33)% in urban areas and 6.25 (95%CI 5.29–6.59)% in rural areas. 14 From the population-based study from Calicut district, Kerala, the age- and sex-adjusted prevalence of unspecified ill-defined rheumatic symptoms was 103.9 (95%CI 9.57–11.26)%. 15 From the population-based study from Lucknow, the prevalence of non-specific pain was 26.5 per 1,000 in rural areas and 31.8 per 1,000 in urban areas. 21
Rheumatoid Arthritis
One of the earliest studies on the epidemiology of RA in India was conducted in a rural population of 44,551 individuals >16 years of age near New Delhi. After a preliminary screening, 0.75% of subjects fulfilled the 1987 American College of Rheumatology (ACR) classification criteria for RA after assessment by a rheumatologist. 22 After adjustment for age and sex, a clinical diagnosis of RA was evident in 0.32 (95%CI 0.24–0.40)% of subjects from urban Pune and 0.67% (95%CI 0.57–0.79)% from rural Bhigwan in Maharashtra. From the same population, 0.19 (95%CI 0.13–0.26)% of urban and 0.54 (95%CI 0.45–0.66)% of rural subjects fulfilled the 1987 ACR classification criteria for RA. 14 The age- and sex-adjusted prevalence of RA in a South Indian population from Calicut district, Kerala was 0.17 (95%CI 0.09–0.33)%. 15 From a North Indian population in and around Lucknow, Uttar Pradesh, the prevalence of RA in urban areas was 4.74 per 1,000 population and in rural areas was 1.56 per 1,000 population. 21
Spondyloarthritis
From the population-based study around New Delhi, 0.36% of individuals had spondyloarthritis. 22 From the population-based studies from Maharashtra, after adjustment for age and sex, spondyloarthritis was prevalent in 0.27 (95%CI 0.20–0.35)% of urban and 0.30 (95%CI 0.23–0.39)% of rural subjects. Ankylosing spondylitis was prevalent in 0.07 (95%CI 0.04–0.12)% of urban and 0.10 (95%CI 0.06–0.15)% of rural subjects. Psoriatic arthritis was prevalent in 0.04 (95%CI 0.02–0.9)% of rural subjects (no cases were identified in the urban subjects). 14 The age- and sex-adjusted prevalence of spondyloarthritis was 0.53 (95%CI 0.36–0.77)% from the population-based study from Calicut district, Kerala. 15
Gout
From the population-based study from Maharashtra, the age- and sex-adjusted prevalence of gout was 0.06 (95%CI 0.03–0.10)% in urban and 0.13 (0.08–0.19)% in rural populace. 14 From the population-based study from Lucknow, the prevalence of gout was 0.98 per 1,000 in urban areas (no cases were identified in rural areas). 21
Systemic Lupus Erythematosus
The epidemiology of systemic lupus erythematosus (SLE) in India has been scarcely studied. A study conducted by the same group which studied the prevalence of RA in a rural area near New Delhi evaluated 91,888 individuals from the same locality (39,826 screened by using a questionnaire, 52,062 screened for antinuclear antibodies). There were three patients with SLE identified from this locality, with a prevalence of 3.2 (95%CI 0–6.86) per one lakh population. 23
Osteoporosis
A position statement from the Indian Society of Bone and Mineral Research reported that about 20% of women older than 50 years (figures from various studies range from 8% to 62%) have osteoporosis. In males older than 50 years, the prevalence of osteoporosis ranges from 8.5% to 24.6%. 24
Few studies have assessed the population prevalence of osteoporosis, mostly from urban areas. A study of 792 males and 808 females (post-menopausal) older than 50 years from urban New Delhi reported osteoporosis in 35.1% (24.6% males, 42.5% females) and osteopenia in 49.5% (54.3% males, 44.9% females). 25 Another study of females between the ages of 30–60 years from an urban area of Hyderabad of low socioeconomic status reported femoral neck region osteoporosis in 29% of subjects. 26 A further study of 250 males older than 50 years from urban Vellore, Tamil Nadu, reported osteoporosis at the spine in 15.2% and at the femoral neck in 10.7%. Osteopenia was prevalent in 47.3% of the spine and 52.7% of the femoral neck. 27
Quality of Life, Disability, Perceptions About Illness and Risk Factors in Individuals with Rheumatic Musculoskeletal Symptoms
Few studies have systematically assessed the quality of life and disability in the community in individuals with RMSK symptoms. From the Bhigwan COPCORD study, the investigators devised and tested the Indian version of the health assessment questionnaire (HAQ) disability index (HAQ-DI) in 724 subjects with musculoskeletal pain. Overall, 18% had significant disability as denoted by HAQ-DI >1.5 (37% with RA, 23% with osteoarthritis, 14% with soft tissue rheumatism and 11% with ill-defined aches and pains). 28 A further analysis of 746 respondents with RMSK symptoms from the same cohort revealed a greater frequency of tobacco use in those with symptoms than without (both for males and females). Female subjects had a higher frequency of pain in the various involved areas than men. Moderate to severe impairment was observed with respect to family responsibilities (7.6%), social responsibilities (5.8%), marital responsibilities (3.5%), workability (22.1%) and finances (18.6%) in a considerable proportion of subjects with RMSK symptoms. From a subset of 409 individuals with RMSK symptoms, 11% were unable to walk, 4% were unable to go to work and 4% were unable to manage their hygiene or self-care. 29
From the Trivandrum COPCORD study, the HAQ-DI was utilised in 1590 respondents with musculoskeletal pain. One in five had moderate disability (HAQ-DI 1–1.5) and one in eight had severe disability (HAQ-DI > 1.5). Factors associated with moderate or severe disability assessed using the HAQ-DI after multivariable-adjusted regression analyses were pain in the hands (odds ratio—OR—2.32), shoulders (OR 1.96), lower back (OR 1.42) and the duration of pain (OR 1.06). 16
Musculoskeletal Pain Following Chikungunya Virus Infection: Insights from COPCORD Studies
RMSK symptoms following the Chikungunya virus epidemics in 2007 and 2009 provide a case study regarding the potential of epidemiological studies to understand changing trends in disease burden. From the Calicut COPCORD study, out of the 5,277 individuals screened during the 2007 Chikungunya pandemic, 1,396 were identified to have clinical evidence of Chikungunya virus infection. Of these, 771 had persistent musculoskeletal pain. On further evaluation of 757 of these individuals, 57.7% (8.3% of the overall population of the region) did not have musculoskeletal pain prior to the Chikungunya pandemic. Knee pain was most frequent (83%), followed by ankle (63%), elbow (59%), lower back (49%), shoulder (47%), hand (26%) and neck pain (9%). Regarding syndromic diagnoses, 57% had post-viral polyarthralgia, 27% had soft tissue rheumatism, 22% had post-viral polyarthritis, 2.5% could be classified as spondyloarthritis and 1.4% as RA. 30
Combining data from the 2007 and 2009 Chikungunya virus epidemics from the Calicut and Trivandrum COPCORD studies (10,286 subjects), out of 2,900 subjects with clinical evidence of Chikungunya virus infection, 44.86% had persistent musculoskeletal pain (46.2% had no prior musculoskeletal pain). The knees, ankles, wrists and elbows were the most frequently affected sites of pain. Those older than 45 years, belonging to a lesser educational or socioeconomic status, with prior history of joint symptoms, with concomitant diabetes mellitus or hypertension, belonging to specific occupations, and with longer duration of pain following Chikungunya virus infection were at a greater risk of persistent pain. Moderate disability by the HAQ-DI was evident in 12.3%. In the Calicut COPCORD cohort, prior to the 2009 Chikungunya epidemic, 29% had RMSK symptoms, which increased to 47.2% after the epidemic. 31
Economic Burden Resulting from RMSK Diseases
A study assessed the burden of rheumatic diseases on healthcare services in India. Based on the National Sample Survey data from 2014, 3.5% of hospital admissions in the one year preceding the data collection and 9.9% of outpatient visits in the preceding fortnight were due to RMSK symptoms. Further in-depth analysis of the population in the Korba district of Chhattisgarh revealed that the cost of management of rheumatic diseases was three times higher in the private sector than in the government sector. Out-of-pocket expenditure in excess of 10% was faced by more than one-half of the households affected with rheumatic diseases. Nearly one-fourth had to resort to borrowing or dispersal of fixed assets in order to meet the expenses of treatment. 32 The cost of spend is often for delays in referral and the failure of the third-party payees (such as the Ayushman Bharat scheme) not recognise rheumatic diseases. Earlier referral might result in lower overall cost of therapy as well as better outcomes of treatment.
Agenda for Further Research and Action
Table 2 compares the prevalence of rheumatic diseases in India and worldwide.33, 34 The reasons for the differences between the epidemiology of rheumatic diseases in India and elsewhere in the world and even in different parts of India can only be speculated as these have not been systematically studied. These could relate to differences in the genetic make-up, environmental influences, dietary influences and other factors.
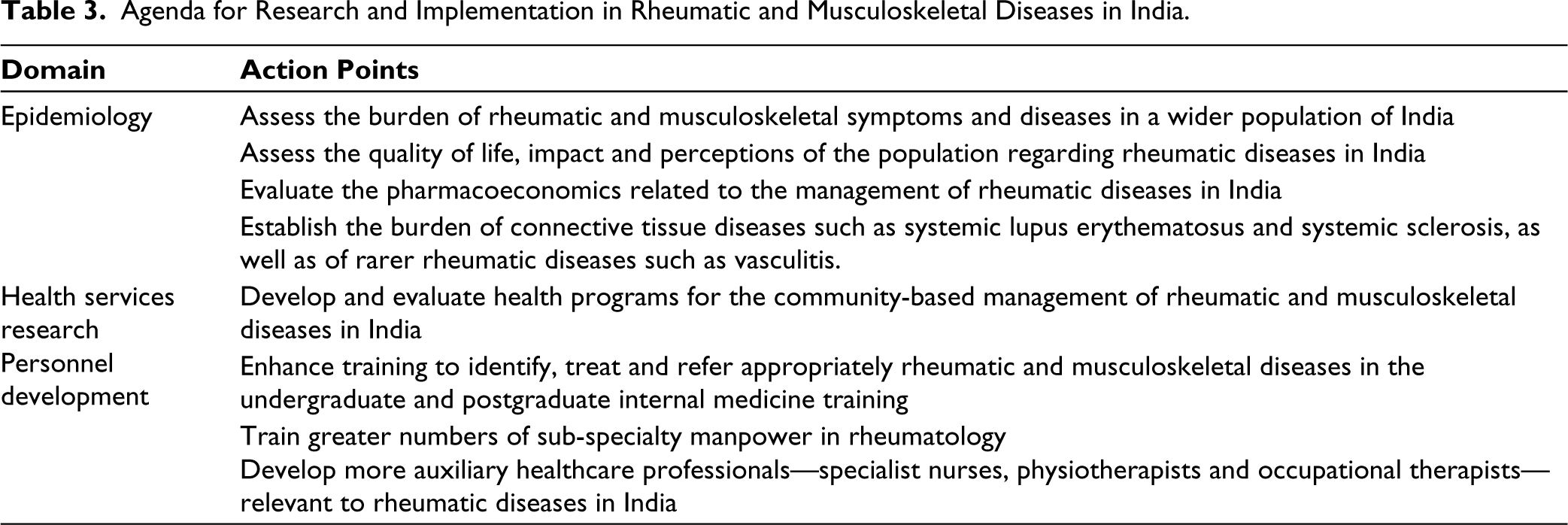
Considering that India is a country with a population in excess of 140 crores, few epidemiological studies regarding the disease burden of RMSK symptoms have been published. Most of the published studies have only assessed the disease burden in stage I COPCORD studies. Assessment of the quality of life, impact and perceptions of the population regarding rheumatic diseases, and the development of health programs (both national and state-wise) for the community-based management of diseases are unmet agendas for research and health services implementation. The epidemiology of systemic vasculitis (of which Takayasu arteritis and antineutrophil cytoplasmic antibody-associated vasculitis are most commonly encountered in India) and Sjogren’s syndrome in India is yet to be studied.35–38 Few studies have assessed the health economics related to rheumatic diseases in India. The problem of manpower to deal with rheumatic diseases is another important consideration. A recent paper estimated that there was one rheumatologist (using a liberal definition) available for nearly two lakh individuals with RMSK symptoms. 39 There is also a paucity of appropriate training for the diagnosis and management of rheumatic diseases at the level of undergraduate (MBBS) and postgraduate internal medicine curricula in India. 39 The development of auxiliary healthcare professionals (specialist nurses, occupational therapists and physiotherapists) to provide holistic care to patients with RMSK diseases is also required. 40 Table 3 lists out agenda for research and action to improve the care of RMSK diseases in India.
Comparison of the Epidemiology of Rheumatic Diseases in India and Worldwide.

Agenda for Research and Implementation in Rheumatic and Musculoskeletal Diseases in India.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable
Funding
The authors received no financial support for the research, authorship and/or publication of this article.