
Abstract
Objective:
Patients with rheumatoid arthritis perceive reduced quality of life in several domains, such as physical health, level of independence, environment and personal beliefs, compared with the healthy population. There is an increasing interest in quality of life in clinical and medical interventions. Few studies have explored patients’ individual conceptions of quality of life, and interviews can thus complement quantitative studies. There is a need for a deeper understanding of the patients’ experiences of quality of life, with regard to living with a long-term condition such as rheumatoid arthritis. The aim of this study was to explore the variation of ways in which patients with established rheumatoid arthritis understand the concept of quality of life.
Methods:
The study had a qualitative design with a phenomenographic approach, which was used to describe variations in how individuals experience their quality of life. The study is based on interviews with 22 patients with established rheumatoid arthritis enrolled in the BARFOT (better anti-rheumatic pharmacotherapy) study.
Results:
The concept of quality of life could be understood in three different ways: (1) independence in terms of physical functioning and personal finances, (2) empowerment in how to manage life and (3) participation as an experience of belonging in a social context.
Conclusion:
The different conceptions of quality of life reflect the complexity in the concept, including physical, psychological and social aspects. This complexity is important to have in mind when health professionals support patients in enhancing their quality of life.
Introduction
Rheumatoid arthritis (RA) is a long-term, fluctuating, inflammatory and systemic disease of unknown etiology. 1 In recent years, there has been an increasing interest in incorporating the concept of quality of life (QoL) in the evaluation of clinical and medical interventions. 2
The World Health Organization (WHO) 3 defines QoL as ‘a broad ranging concept incorporating in a complex way the person’s physical health, psychological state, level of independence, social relationships, person’s beliefs and their relationship to salient features of the environment’. QoL can be measured in various ways, and several generic and RA-specific questionnaires have been used.4–6 Patients with RA report reduced QoL in several domains, such as physical health, level of independence, environment and personal beliefs, compared with the healthy population. QoL in RA is affected by fatigue, pain, stiffness and impaired physical functioning.7–9 In addition, QoL is also influenced by socioeconomic factors such as age, employment, economic status and lifestyle habits. 10
There are few qualitative studies exploring RA patients’ perceptions of the concept of QoL. One previous study found that the patients’ understanding included not only freedom from disease and good physical functioning but also psychosocial aspects of life. 11 There is a need for a deeper understanding of the patients’ experiences of QoL, especially with regard to living with a long-term condition such as RA. This could be achieved by using qualitative research methods as a complement to previous quantitative research. 12 The aim of this study was to explore the variation of ways in which patients with established RA understand the concept of QoL.
Method
Design
The study had a qualitative design with a phenomenographic approach to describe the different ways the studied phenomenon of QoL could be understood.13,14 The variation in conceptions is important, because the conceptions are founded on the lived experience of the individuals. Phenomenography proposes that a phenomenon is understood by individuals in qualitatively different ways and that a group of individuals create an understanding of the phenomenon on a collective level. 13
Participants
The study was based on interviews with 22 patients with established RA, defined as having more than 2 years of disease duration. 15 All of these patients were enrolled in the BARFOT (better anti-rheumatic pharmacotherapy) study, in which 2800 adult patients with early RA were included from 1992 to 2006. The patients were registered at diagnosis (baseline) and at follow-up at 3, 6 and 12 months and 2, 5, 8 and 15 years. Details of the study have been published elsewhere.16,17 For this study, participants were selected by using a strategic sampling procedure in order to gain variations in the following: gender (14 females and 8 males); age (30–84 years); disease duration (8–23 years); marital status (15 married/co-habiting and 7 single); education (8 compulsory comprehensive school, 9 upper secondary school and 5 undergraduate studies); employment (8 employed and 14 on sick leave or retired); physical function assessed by health assessment questionnaire (HAQ) = 0–1.38; health-related QoL assessed by Euroqol5D (EQ-5D) = 0.52–1.0 and originating from all 6 BARFOT centres (2–7 participants/centre) which cover both urban and rural patient referral areas.
Data collection
Individual interviews were performed at the participant’s BARFOT clinic in a private room, between May 2014 and June 2015. The interviews started with the main author (K.M.), clarifying the aim of the study. In line with the phenomenographic method, 18 all interviews were initiated with three open-ended questions aimed at ensuring similar data from all participants: ‘What does QoL mean to you?’, ‘How do you conceive your QoL?’ and ‘How has your RA affected your QoL?’ The aim of the interviews was to capture the participant’s fundamental and genuine conceptions about QoL. The interviewer therefore returned to the main questions several times during the interview and by probing questions and reflecting comments encouraged the participants to focus on their own lived experience. Finally, the interviewer summarized the interview with the participants. Each interview lasted between 30 and 70 min, was audio-recorded and then transcribed verbatim by K.M. Two pilot interviews were conducted in order to check the questions. As no revision was necessary, these interviews were included in the study.
Data analysis
The aim of the phenomenographic method is to identify various ways of understanding a phenomenon, in this case, QoL. The analysis was performed manually in seven steps according to Larsson and Holmström 19 by K.M., with the last author (I.L.) acting as co-assessor:
The entire text was read several times in combination with listening to the audio-recorded interviews.
When rereading, the whole text marks were made where participants gave information corresponding to the aim of the study.
The marks were then compared and discussed to identify the participant’s dominant way of understanding QoL and how this was described, formulating a preliminary description of each patient’s dominate way of understanding his or her QoL.
Based on similarities and differences, descriptions were categorized into three descriptive categories. These are reported in the form of text and illustrated by quotations.
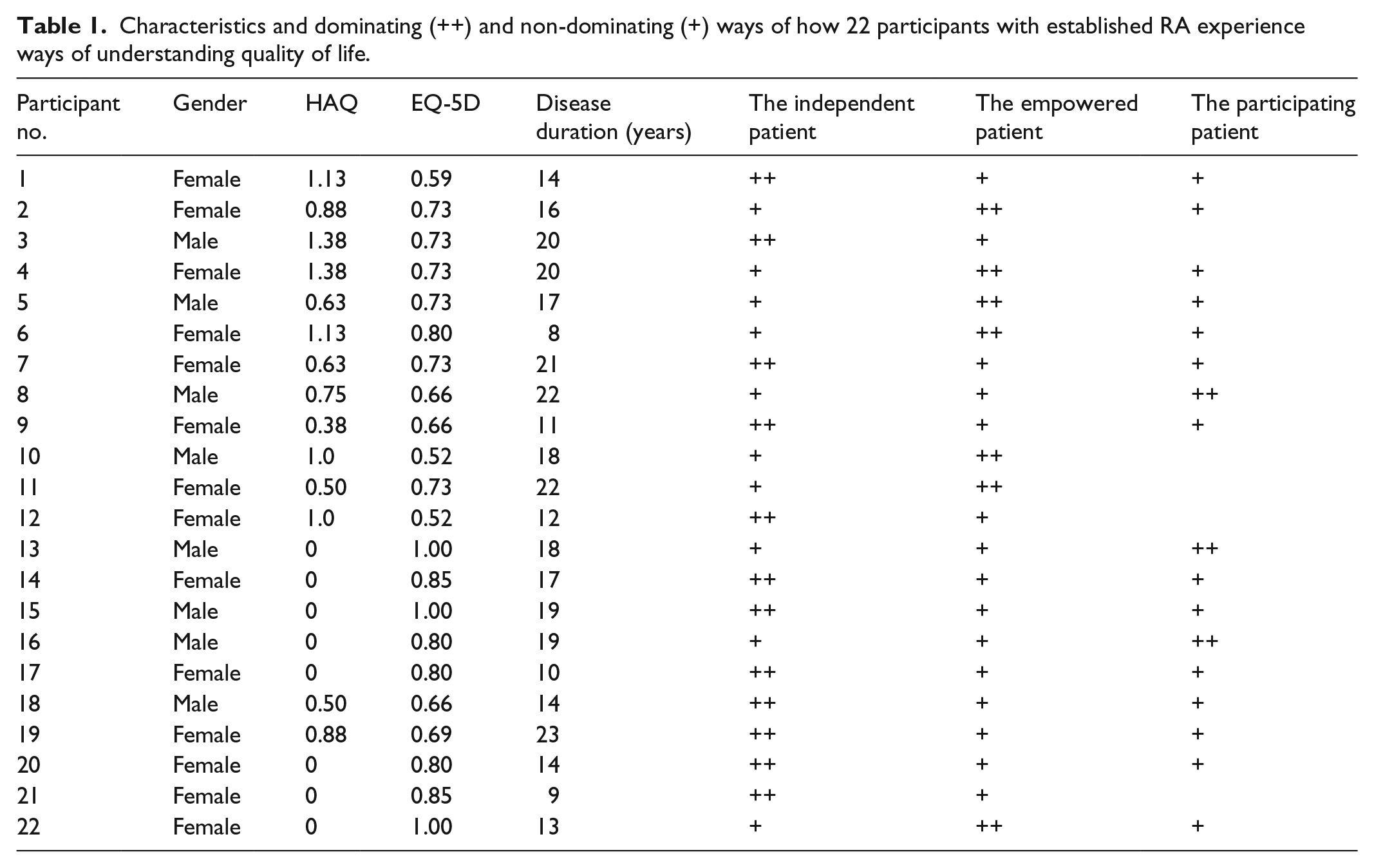
The participant’s non-dominant ways of understanding of the phenomenon were identified. This was undertaken to ensure that no aspect was overlooked (Table 1).
A structure was created of descriptive categories in order to find the internal relationship between the three categories, which created the outcome space, constituting the result of the phenomenographic study (Figure 1).
To each of the three descriptive categories, a metaphor was assigned.
Characteristics and dominating (++) and non-dominating (+) ways of how 22 participants with established RA experience ways of understanding quality of life.

The outcome space illustrating the relationship between the categories independence, empowerment and participation and described physical, psychological and social aspects that influence the quality of life in patients with established RA. The categories are related as parts of a whole and the variations that emerged are not hierarchically related.
To attain rigour and consensus in the data analysis, the authors, who had extensive experience of rheumatology and qualitative methodology, took part in several discussions regarding each step in the data analysis. The patient perspective was also taken into account by inviting a patient research partner to participate in the design of the study and in the data analysis. 20
Ethical considerations
The participants received a letter regarding the aim of the study, its design and voluntary nature of participation and signed an informed consent. The participants were guaranteed confidentially and informed that they could withdraw at any time without giving an explanation. The study was carried out in accordance with the ethical principles of the Declaration of Helsinki 2013. 21 The Regional Ethical Review Board at Lund University, Sweden, approved the study (LU 2016/896, KI 2014/1986-31/1).
Results
The patients spoke of a number of different ways of understanding the phenomenon of QoL in established RA, although one way of understanding was more dominant for each individual (Table 1). The following three ways of understanding emerged: the independent patient, the empowered patient and the participating patient.
The independent patient
In this descriptive category, the conceptions were focused on various physical aspects as being independent in terms of physical functioning and personal finances, and the metaphor of the independent patient emerged. The independent patient experienced QoL when being free and independent in the ability to choose and manage daily activities of living at home, at work and in their leisure time. The patients could manage their life plan without asking for help. The independent patient talked of the importance of maintaining physical functioning, so they could remain physically active and have the ability to be outside the home. QoL for the independent patient entailed not being limited:
… physical activity means quite a lot to me, because I also relate it to quality of life … (P20, female, 37 years, 14 years with RA) … independence is thus also quality of life and then it’s not having pain. Being able to cope oneself, stopping asking for help or not having to ask for help. (P19, female, 58 years, 23 years with RA)
QoL also entailed having financial security and possibilities for choosing where and how to live, in an apartment or in a house, what to eat and to be able to afford to continue with a self-chosen hobby, such as travelling or going to the theatre:
… I don’t want to have a financial situation that means I’m unable to buy the food I like and so on or unable to go to some event if I like it, then it would be miserable. If I need to buy some clothes or something then I’d like to have the money for it. (P14, female, 77 years, 17 years with RA)
Being independent also meant not having the need to take medication or to be able to take as little medication as possible, but the patients could, on the other hand, conceive a sense of dependency by having the need to have a routine, a plan to take medication at a certain time of the day. When travelling abroad, some medications needed special handling, which was conceived as limiting:
… [quality of life] yes, to get rid of the pain, and avoid to use a lot of medication. (P1, female, 63 years, 14 years with RA) … not being limited, yes, that’s quality of life for me. it’s not being limited. Yes being able to do what I feel like doing. Actually, it, that’s quality of life. (P12, female, 51 years, 12 years with RA)
Variations in conceptions of QoL emerged with patients expressing that their freedom was restricted due to being dependent in their daily activities, which led to practical consequences such as being forced to cancel planned activities and stay at home. The patients felt that they became dependent because of fatigue, pain or limitations in their functioning, which affected how they handled and performed their everyday life activities:
… when it was the worst possible when I could hardly turn over in bed then I thought – shit is life going to be like this? This is completely worthless. (P15, male, 38 years, 19 years with RA)
The empowered patient
In this descriptive category, the conceptions were focused on different psychological aspects of how to manage life, and the metaphor of the empowered patient emerged. The empowered patient experienced that QoL meant to take charge of and use different resources, such as positive thinking, in order to manage fatigue, pain and physical functioning. The patients’ conception of being empowered was to believe in their own capacity to self-manage their everyday life, to be flexible and to influence their situation:
… positive thinking, particularly even in difficult situations, so I always think there’s a light at the end of the tunnel and then it is being a, yes how shall I answer, quality of life, yes that’s what I’m doing. (P10, male, 63 years, 18 years with RA)
There were also conceptions about the empowered patient, that QoL entailed being able to see opportunities and to be able to continue with planned activities by using ordinary routines, and to accept the need for help in specific situations. The empowered patient talked of a sense of security in mind and body in order to cope with a situation in an individual way:
… Yes, but it’s that I choose, I do easier things so that I don’t have to feel sad that I am unable to do what I can’t do. (P4, female, 65 years, 20 years with RA)
The empowered patient’s conception of QoL was to adjust the use of medication to manage symptoms such as pain and fatigue in order for it to fit the plans for the day, and to take charge of the negative side effects such as nausea:
… quality of life, the only thing I can think of about that is taking tablets when I have pain, it sounds stupid or take a bath as I will feel better, yes. (P2, female, 52 years, 16 years with RA)
The empowered patient also described that QoL depended on the absence of other diseases, and that the family was healthy and felt well. Being empowered was described as having the knowledge and experience to adjust and create ordinary daily routines in order to handle everyday life.
The participating patient
In this descriptive category, the conceptions were focused on different social aspects, such as having the experience of belonging and participating, and the metaphor of the participating patient emerged. The participating patient experienced QoL in terms of being part of a social community, participating in different projects at home, at work or in the community. QoL also entailed having the ability to meet old and new friends, and to have meaningful things to do. The participating patient took part in different contexts with other people of different ages and gender:
… being able to be together with younger people, I’ve always thought that it is fun to sort of keep my head above water [be alert and keep up with what is going in the world], that I’ve not only thought like a 65-year old but can understand how a 25-year old thinks and a 40-year old and perhaps even younger. I think that’s also quality of life to be able to meet people of all ages. (P16, male, 68 years, 19 years with RA)
QoL for the participating patient entailed a sense of belonging to a family, a group of colleagues and friends, and being appreciated and valued:
… be together with friends and acquaintances. That’s quality of life. (P13, male, 84 years, 18 years of RA)
The participating patient also conceived that QoL entailed being outside the home, in the garden or on a daily walk around the neighbourhood, talking to neighbours and being seen as a person:
… it’s also quality of life being able to give back, pick up the kids at day nursery etc. We’re actually busy with taking care of children. (P16, male, 68 years, 19 years with RA)
Variations emerged and were described as fears of not being able to participate in social relationships because of symptoms, such as limitations in functioning, fatigue and pain. The participating patient described conceptions of loneliness and a fear of not being needed and being left out. The conception of QoL was adversely affected if the patients always needed to eat and cook by themselves, not being able to visit family, friends or to have dinner at a restaurant:
… my quality of life has deteriorated through me being alone now so that … well, in any case the one I lived with, then the quality of life is worse, I think. (P8, male, 65 years, 22 years of RA)
Outcome space
The result of this phenomenographic study does not only contain the categories but also the relationship between the categories, termed the outcome space. The categories are related as parts of a whole and the variations that emerged are not hierarchically related. The categories independence, empowerment and participation are physical, psychological and social aspects of the concept of QoL in established RA, reflecting the complexity of QoL in a long-term condition. Physical aspects included independence in terms of both physical and financial aspects. QoL was also influenced by psychological aspects, such as management and empowerment. Social aspects entailed having a sense of belonging and participation. The outcome space can be divided into three parts: independence, empowerment and participation with no overlap, representing the collective understanding of the participants’ ways of understanding QoL (Figure 1).
Discussion
The study showed that patients with established RA understood the concept of QoL in three different ways: independence, empowerment and participation. These categories can be described as physical, psychological and social aspects and are in line with the WHO 3 definition of QoL.
In this study, being independent was spoken of as a conception of freedom, a physical feeling of maintaining independence without bodily symptoms. Being able to continue with physical activities and exercise depended on the current level of physical functioning. To be independent in this study meant functioning physically and being physically active. These aspects have also been found to be very important for QoL in other studies,22,23 which report physical activity as an opportunity for experiencing independence and QoL. A variation in the conceptions of independence was dependence, experienced as limited physical functioning due to deformities and pain affecting QoL. A previous study has described how physical limitations in the lower extremities affect independency and reduce QoL. 24 It emerged in this study that the participants were aware of the benefits of being physically active and how physical activity affected QoL, which is consistent with the findings of previous research. 25 The ability to influence life and not having to plan ahead made life easier and was expressed as independency. It was also important not to feel limited in terms of medication administration, and the association between the conception of independence and the medication administration has been previously described. 26 Physical functioning was expressed in this study as being vital for maintaining mobility and being able to have leisure activities, as well as continuing with a self-chosen hobby. The latter was associated with QoL and expressed as a measure of independence. This is also in line with other studies where hobbies were described as an important domain for QoL in RA. 27
The independent patient’s QoL was negatively affected when having to be dependent on help from family or friends in everyday activities. This is supported by other studies where it is reported that patients who were married or cohabiting sometimes had feelings of gratitude and guilt for being dependent.27,28 The independent patient described the value of having sufficient financial resources to be able to travel and to stay active in various hobbies, even if the hobby was an expensive one that entailed travelling or riding a horse or a motorbike. The financial situation could be affected by the disease, since inadequately treated RA leads to sizable economic costs for the patients and their families, which has also been described in other studies.29,30
The experience of living with a long-term condition such as RA makes the patients strive to accept to live with the fact that RA is a part of who the person is. The empowered patient described how to manage everyday life and how to use different psychological strategies, in order to be empowered to take care of yourself and learn to live and cope with different symptoms. 28 In a previous study, the patients’ self-perception and identity were affected by reduced physical functioning, and the patients described a process of coping with physical barriers as a struggle between the mind and the body and the need to adjust new routines to handle different situations. 31 The empowered patients used their knowledge of having had a long-term condition for several years, and had a belief in their own ability to manage different situations, and how to reset goals and expectations. A previous study about the experience of living with RA reported that the patients became their own experts in managing and coping with disease symptoms, which could be interpreted as empowerment. 32 Another finding in our study is that the empowered patient expressed a need to take active choices and change priorities to enhance QoL. This indicates the importance of strengthening empowerment, and that health professionals continue to develop problem-based learning and give the patients individual support to enhance awareness and understanding of the consequences of their self-managing. 33 Empowerment helps the patients think critically to have the opportunity to make autonomous and informed decisions so they can get what they need, handle everyday life and enhance QoL. 34 The latter was affected if individual expectations could no longer be achieved and if previous presumptions about life could not be fulfilled, which was described in a study of everyday life in patients with RA as being a disruption in the individual’s life project. 31 The empowered patients spoke of having a sense of control and the knowledge to use ordinary everyday routines to handle different symptoms, which enhanced QoL, such as walking around the neighbourhood, relaxation techniques and how to ask for and receive help from others. This is in line with two qualitative studies that highlighted personal empowerment and individual resources for overcoming disease-related restrictions.35,36
To be able to participate in different contexts was experienced as an aspect of QoL, and to be a part of a social context gave a sense of belonging. The participating patient expressed the importance of being part of a family and having friends to achieve QoL. A variation in the concept participation was described as a sense of loneliness and not being needed. To belong in a social context has been expressed as important for retaining QoL in patients with RA. 37 Overcoming conceived restrictions and limitations by having social support in everyday life improves QoL, which is in accordance with previous findings about the accessibility of different social relationships and participation with family, friends and colleagues.10,38 Most work situations involve social contacts, which enhance social participation. 40 Companionship at work or different types of social or voluntary networks appear to be important social arenas for social participation, and these findings are confirmed by other researchers.22,31,35 These studies indicate the importance of remaining in employment and being able to continue with self-chosen hobbies. Patients with RA become work-disabled at a greater rate than the general population, which affects QoL. 39 As can be found in previous research, our study confirms the importance of having the ability to meet people on equal terms in different contexts, and one consequence of impaired physical functioning could be a reduced social participation and thus isolation. 40 Furthermore, symptoms such as pain and fatigue also affect the ability to participate. 25
The categories are separated parts of a whole, and occur in varying degrees for the same individual. In order to enhance QoL, it is important that the whole person is seen and heard, and supported in all the aspects described in the three categories: independence, empowerment and participation. By using a qualitative design, the patients’ perspective is highlighted. The participants have the opportunity to describe with their own words the phenomenon, QoL, from personal experiences of living with a long-term condition, instead of being restricted to answer standardized questionnaires. 12
Methodological considerations
The phenomenographic approach was chosen in order to gain variation in ways of understanding QoL in patients with RA. 18 In qualitative research, trustworthiness should be based on four criteria: credibility, dependability, confirmability and transferability.41,42 Credibility was strengthened by two pilot interviews, and that a total of 22 interviews were conducted. The fact that the interview text was deemed rich and that the descriptive categories covered the data also increases credibility. Credibility was enhanced by careful description of data collection and analysis, and that the researchers worked both individually and together in the data analysis. Dependability was strengthened by using the same open-ended questions to all the participants to assist them to reflect and explain their understanding of the phenomenon of QoL. The strength was that the main researcher performed all interviews in the same way. Confirmability was demonstrated by the systematic and conscientious data analysis, where all steps have been reported. Including a patient research partner in the design and data analysis enhanced the confirmability of the study. Quotations of the participants’ ways of understanding enhanced and illuminated the content. The transferability was strengthened since the study was performed among a national sample of BARFOT clinics in Sweden. A qualitative approach does not attempt to generalize the result to a whole population, but it is probable that the categories could be transferable to other patients with long-term condition. All the participants were born in Sweden, and this could be a limitation in the study with regard to transferability.
Conclusion
QoL in patients with established RA was conceived as independence in terms of physical functioning and financial resources, as empowerment in how to manage life and as participation in the experience of belonging in a social context. This reflects the complexity in the concept of QoL, including physical, psychological and social aspects that are in line with the WHO definition. This study suggests a holistic approach from the health professionals, which is important when supporting patients with RA in different situations to increase their QoL. Research in QoL within rheumatology that focuses on narrative interviews from patients with both early and established RA is scare and further qualitative studies are necessary. It would also be interesting in a clinical practice to investigate how independence, empowerment and participation can be maintained and enhanced in patient with RA.
Footnotes
Acknowledgements
The authors thank the participants for generously sharing their experiences, and their patient research partner Maria Nylander and the BARFOT study group.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study was approved by the Regional Ethical Review Board at Lund University, Sweden (LU 2016/896, KI 2014/1986–31/1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Swedish Rheumatism Association, the County Council of Halland Research fund, and the Norrbacka-Eugenia Foundation.
Informed consent
Written informed consent was obtained from all subjects before the study.