
Abstract
Background
The lack of guidelines for early feeding assessment has a significant impact on infants and mothers, as incomplete or inadequate feeding evaluations can result in incorrect diagnoses, making feeding difficulties unmanageable.
Objective
The aim of this systematic review was to analyze the literature on what tools are currently used, how comprehensive and person-centred they are, and which disciplines are currently involved with neonatal feeding assessment during hospital stay after birth.
Methodology
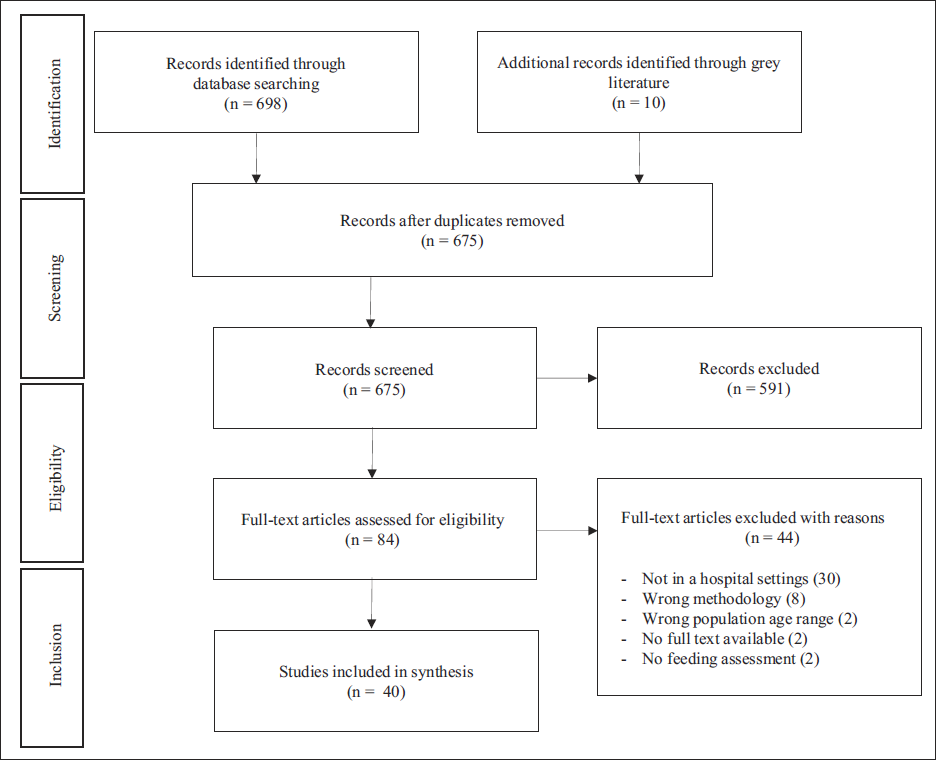
A systematic review was proposed to analyze all articles published between 2012 and June 2022. Databases included PubMed, MedLine, and Web of Science. Included articles assessed feeding difficulties in infants (12 months or younger) during hospital stays after birth in maternity hospitals or neonatal intensive care units (NICUs). Articles in languages other than the primary languages of the authors (i.e., English and Portuguese), review articles, book chapters, commentaries, and letters to the editor were excluded from the present research. The initial search yielded a total of 698 articles for review, with an additional 10 articles found through the gray literature search. Thirty-three articles were removed after deduplication, and the remaining studies (675) were included for title and abstract screening.
Results
Two authors independently conducted 84 full-text reviews, and a total of 40 articles were included in the present study. Thirteen observational assessment tools, five clinical bedside assessments, five questionnaires or interview methods, four instrumental assessments, and four other types of assessment tools or methods were identified.
Conclusion
The variability of feeding assessment methods and tools for infants indicates a lack of standardization in breastfeeding assessment. The results of this research suggest that all described feeding or breastfeeding assessment tools are not comprehensive or person-centered, as they do not include all major aspects that can impact breastfeeding. Therefore, a consistent approach to breastfeeding assessment in hospitals is recommended to increase the incidence of breastfeeding success in the first 6 months of life. Finally, healthcare professionals who would like to promote, assess, and treat breastfeeding difficulties should pursue additional training or credentialing in breastfeeding and maternal-infant health.
Keywords
Introduction
The American Academy of Pediatrics 1 published a policy statement in 1997 describing human milk as the gold-standard nutrient for healthy, term newborn infants, advising it as the only nutrient provided through the first 6 months of life in most cases. This focus on breastfeeding led to the development of the Baby Friendly Hospital Initiative (BFHI), which aims to protect, promote, and support breastfeeding. In Australia, the BFHI focuses on improving healthcare for babies, their mothers, and families by ensuring they receive unbiased information, support, and evidence-based advice before and after birth, despite their feeding choices and circumstances. 2 Currently, approximately two out of three infants are not exclusively breastfed for the recommended 6 months, which has not changed in the last two decades. 3
Globally, three in five babies (78 million babies) are not breastfed in the first hour of life. 3 In Australia, breastfeeding statistics indicate that three-quarters (74.8%) of the babies were initially breastfed, but only 66% were exclusively breastfed for 4 months, and 35.4% were exclusively breastfed for 6 months. 4 There are many factors that can influence breastfeeding and its duration. Maternal factors that contribute to premature weaning include milk production, milk flow, and breast/nipple pain.5, 6 Newborn factors include incoordination of suck-swallow-breathe cycles, swallowing difficulties, reflux, 7 tongue-tie, 8 syndromes, congenital health diseases, 9 and low birth weight. 10 Additionally, birth complications such as hypoxia 11 and premature birth 12 are also a risk for difficulties or early cessation of breastfeeding.
Delays in identifying risk factors that can influence breastfeeding efficiency may negatively affect an infant’s development, nutrition, and physical and psychological well-being, as well as the mother’s physical and psychological well-being. 13 Therefore, BFHI recommends that mothers be assisted to initiate breastfeeding within 1 h of birth and be given advice on maintaining lactation. 2 Even though there are many breastfeeding assessment tools and screenings available, their components vary widely, and the majority of them do not include an evaluation of all factors that can lead to breastfeeding failure. 14
Neonatal feeding assessment tools and screenings usually include components of infant behaviors (e.g., alertness state, oral reflexes), maternal characteristics (e.g., nipple type), and technical aspects of breastfeeding (e.g., attachment). A 2018 study by Chapman and Kuhnly that evaluated the limitations of lactation assessment tools described them as too long or time-consuming, not objective enough, difficult-to-assess components (e.g., audible swallowing), and highlighted a single feeding attempt while encouraging an overreliance on numbers. 14 Another study indicated that there was some accordance between the breastfeeding tools’ components, but just a few tools achieved comprehensive coverage, and many important components were frequently neglected. 15 Additionally, the findings of both studies outlined that the reliability and validity of those tools should be reassessed.14, 15
Incorrect diagnoses can be harmful, as they might prevent or delay appropriate treatment and lead to unnecessary or even harmful treatment, 16 impacting both mother and infant. 17 A large variety of assessment screening tools and methods is being used, in combination with substantial diversity in the types of healthcare professionals involved with breastfeeding, and this might represent a significant problem for infants and mothers. 18 Even though there are a large number of published studies describing the reliability and validity of those tools, there is currently no research outlining how comprehensive and person-centered the most used assessment tools are. Therefore, this systematic review was conducted to answer the research question: what tools are currently used for the assessment of feeding skills in neonatal children, how comprehensive and person-centered these instruments are, and which disciplines are currently involved with neonatal feeding assessment during hospital stay after birth.
Methodology
Search Design
This systematic review followed guidelines for systematic reviews and meta-analyses, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements, 19 including the synthesis without meta-analysis (SWiM) guidelines. 20
Eligibility Criteria
Included articles assessed feeding difficulties in infants (12 months or younger) during hospital stays after birth in maternity hospitals or neonatal intensive care units (NICUs). Articles in languages other than the primary languages of the authors (i.e., English and Portuguese), review articles, book chapters, commentaries, and letters to the editor were excluded from the present research.
The initial search strategy was developed in PubMed and is outlined in Table 1. This strategy was then adapted as needed for each individual database. The main subject headings included feeding, infant, NICUs, and maternity. Additional search terms included feeding methods, feeding behavior, breastfeeding, bottle-feeding, feeding and eating disorders, enteral nutrition, parenteral nutrition, newborn, newborns, neonate, neonates, maternity hospitals, maternal-child nursing, and birthing centers.
Search Per Database.

Systematic Review
An electronic literature search was conducted by three authors (ACLB, MCLP, SRK) on June 7th, 2022, to identify all articles published from June 2012 to June 2022. The databases searched included PubMed, MedLine, and Web of Science. Reference lists of included articles were manually screened using forward and backward citation chasing to identify additional relevant publications. Duplicated articles were removed using the Bramer method. 21
Following deduplication, four authors (ACLB, MCLP, PKS, and SRK) independently assessed the eligibility of the remaining articles through abstract screening. If unclear from the title and/or abstract whether an article met the inclusion criteria, it was advanced to a full-text review. Full-text assessments were conducted independently by two reviewers (MCLP and SRK) using predefined inclusion and exclusion criteria. Any discrepancies in reviewers decisions were resolved through discussion with a third reviewer (PKS) to reach a consensus.
A gray literature search was completed by two independent researchers (ACLB and SRK) via keyword search in OpenGrey, Trove, and Proquest Central for articles or theses that may have contained/led to relevant published studies. Keyword searching in the reference list of all included articles and in Google Scholar was also conducted.
Data Extraction and Synthesis
Data including study design, population (n), feeding method, offered liquid, feeding assessment description, when assessment was performed, who assessed the infant, description of feeding problems, feeding management if any, when feeding management was performed, who provided the feeding management, and the hospital ward where the patients were assessed were extracted from each eligible study. To minimize errors in data extraction, two reviewers (MCLP and SRK) independently extracted the data from the included studies. In cases where the reviewers’ answers differed, a third reviewer (ACLB) was used to achieve consensus.
Methodological Quality
The quality of the eligible studies was evaluated using the Joanna Briggs Institute (JBI) 22 critical appraisal tools. JBI is an international organization that supports evidence-based decision-making aimed at improving health outcomes and healthcare service delivery. Given the objectives of the present study, the JBI system was deemed the most appropriate. Three independent reviewers (MCLP, PKS, and SRK) assessed each eligible study using the relevant appraisal indicators for its study design, assigning one point per criterion met. The reviewers then compared their assessments, and any discrepancies were resolved through joint discussion to reach a consensus.
Results
Selection of Studies
The initial search yielded a total of 698 articles for review. An additional 10 articles were found through the gray literature search. Thirty-three articles were removed after deduplication, and the remaining studies (675) were included for title and abstract screening. Two independent reviewers (MCLP and SRK) conducted 84 full-text reviews, and a total of 40 articles met the inclusion/exclusion criteria and were included in the present study. The PRISMA flow chart is shown in Figure 1.
Study Selection Process Flowchart.
Study Designs and Quality Assessment
Of the 40 studies included in this review, 11 (27.5%) articles were cohort studies, 10 (25%) were cross-sectional studies, six (15%) were randomized clinical trials, six (15%) were diagnostic test accuracy studies, two (5%) were case-control studies, two (5%) were quasi-experimental studies, and one (2.5%) was a case series. The JBI critical appraisal tools indicated that the majority of the studies (57.5%) had high-quality methodologies with scores equal to or higher than 70%, 10 studies (25%) had medium-quality methodologies with scores between 51% and 69%, and seven (17.5%) of the 40 studies had significant methodological shortcomings with scores lower than 50%.
Patient Population
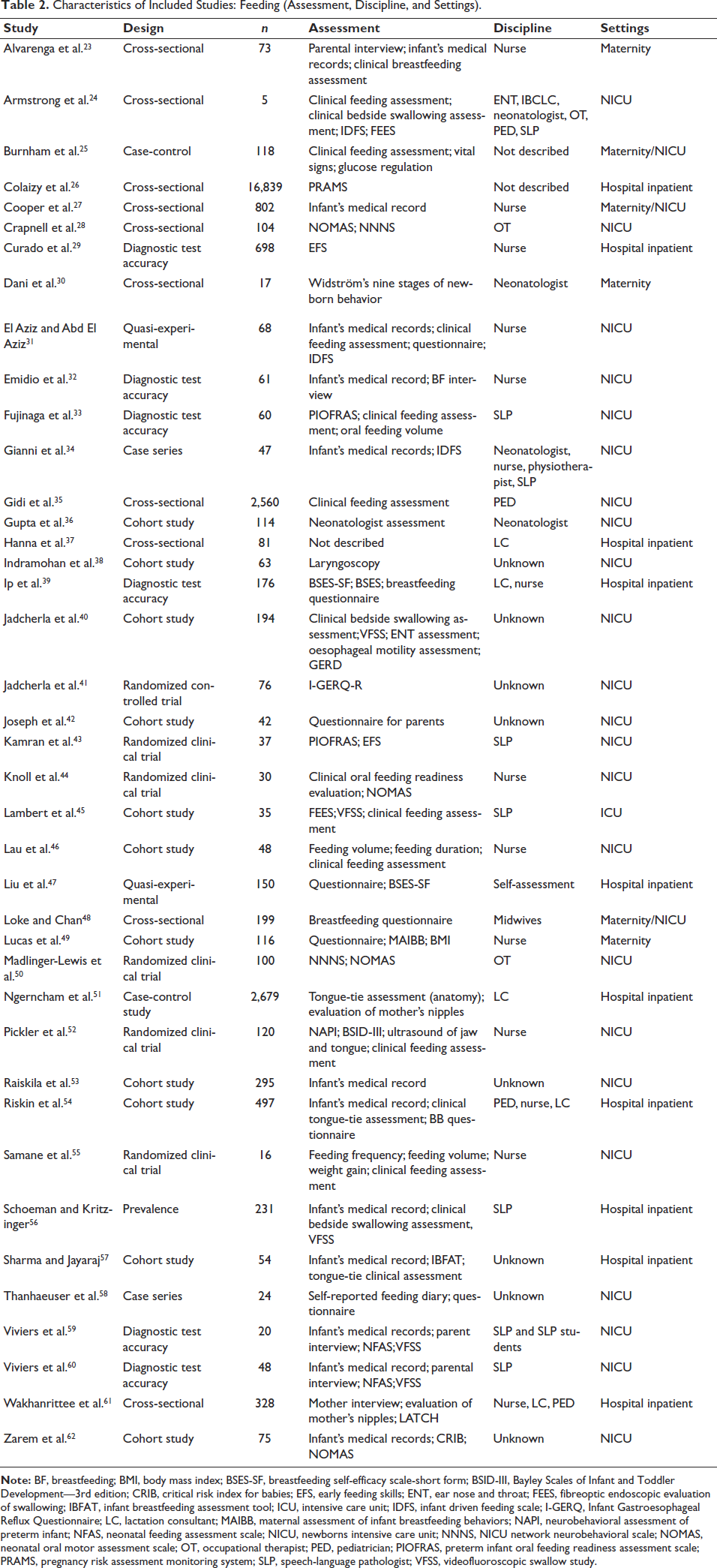
A total of 27,265 infants from 24 weeks of gestational age (GA) to full-term infants (40-42 weeks GA) were described across the 40 included studies. Regarding the settings where the feeding assessment occurred, 26 studies were in the NICU, 10 were described as “hospital inpatient” but did not define the ward in which the assessment was performed, and six were performed in the maternity ward. Additionally, three studies included both the NICU and maternity ward as settings for assessment (Table 2).
Characteristics of Included Studies: Feeding (Assessment, Discipline, and Settings).
Feeding Assessments, Outcomes, and Discipline
The most studied feeding method was breastfeeding (67.5%), which was described as the only feeding method in 11 studies (27.5%). Bottle feeding was included in 15 (37.5%) studies, and it was the only feeding method in two studies (5%). Additionally, 11 (27.5%) studies included infants in enteral feeding (oral or nasal tube or gastrostomy), and one study included infants in parenteral feeding (2.5%). Thirteen studies included both breast and bottle feeding but did not describe if this meant mixed feeding or not (32.5%).
In this review, nurses were responsible for the feeding assessment in 13 studies (32.5%), followed by speech-language pathologists (20%) and lactation consultants (12.5%). However, 22.5% of the included studies did not describe who the feeding assessor was. Additionally, half of the studies had a single profession assessing feeding. The nurses were solo in nine studies (22.5%), the speech-language pathologists in five (12.5%), the occupational therapists in two (5%), the neonatologists in two (5%), the lactation consultants in two (5%), the pediatricians in one (2.4%), and the midwives in one (2.5%). Only four studies (10%) had three or more healthcare professionals involved with the feeding assessment (Table 2).
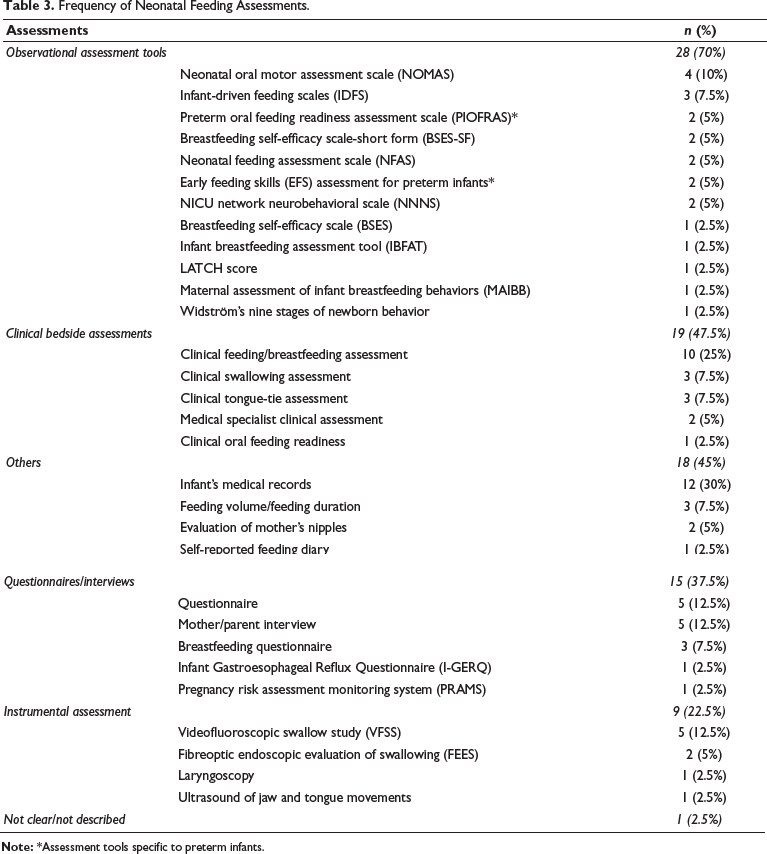
The frequency of each feeding assessment tool/method is described in Table 3. The majority of the studies (60%) included an assessment method or tool to evaluate oral feeding. A total of 29.2% of the studies assessed feeding through a method or assessment tool that was not included in any other study. Twelve studies (29.2%) included the infant’s medical record as part of the evaluation, and six studies (14.6%) included an instrumental assessment of swallowing.
Frequency of Neonatal Feeding Assessments.
Discussion
This systematic review revealed a lack of consistency across assessments used by clinicians to indicate and diagnose feeding difficulties in infants. Sixty percent of the studies included an observational assessment tool; however, there were 13 different feeding assessment tools described, and five of them were not used in more than one study. Moreover, 27.5% of the studies only used one assessment method or tool, and only 10% provided a multidisciplinary assessment (i.e., two or more disciplines were involved in the feeding assessment). That is notable, as it is well described in the literature that causes and associations of feeding difficulties in infants are extensively diverse, and the majority of the feeding problems are multifactorial,63–65 and that a multidisciplinary approach is crucial for the assessment of feeding difficulties.10, 66
A multidisciplinary approach in pediatric feeding should start with a thorough parent interview or questionnaire, which is extremely important to the formation of a differential diagnosis. 67 Through sharing their unique experience with symptoms, concerns, and questions, parents help the clinician to make diagnoses. 68 Therefore, it was expected that all studies would include a mother or parent interview as part of the feeding assessment; however, less than 40% of the studies included this method of evaluation. The literature indicates that patient interviews are clinically significant in identifying the need for specific examinations and assessments, which can directly influence the quality of the medical treatment. 69 Failure to collect this important piece of data can significantly impact all aspects of patient care.
Information from medical records provides essential data for monitoring patient care, clinical checks, and assessing patterns of care and service delivery. 70 It can also include important background history in the absence of a parent interview or questionnaire. It was expected that all studies that did not include a medical interview or parent questionnaire as part of the feeding assessment would include the data available in the infant’s medical records. However, only six studies that did not provide a parent interview or questionnaire included the infant’s medical records. In total, 30% of the studies included information provided in medical records. That was also not expected, once all included studies were hospital-based.
In addition to parent interviews/questionnaires and the infant’s medical records, it was expected that the most frequent assessment included would be a clinical feeding assessment, as the literature describes it as the most widely used method to assess an infant’s ability to feed safely and efficiently. 71 However, only 25% of the studies included a clinical feeding/breastfeeding assessment, and 40% of the studies assessed one specific aspect of feeding, such as tongue-tie or reflux. Even though tongue-tie and reflux are highly related to feeding issues in infants, there is a long list of medical and developmental conditions in infants (structural abnormalities of the aerodigestive system, neuromuscular and developmental disorders, cardiorespiratory disorders, and gastrointestinal disorders), 63 as well as mother-related conditions (structural abnormalities of the breast, pain with breastfeeding, nipple trauma, milk supply, breast infections, postpartum complications, and psychological issues) 72 that are associated with difficulties in feeding. Therefore, a more comprehensive feeding assessment was expected.
According to the American Speech and Hearing Association (ASHA), 73 feeding is described as the process involving any aspect of drinking or eating, including gathering and preparing food and liquid for intake, sucking or chewing, and swallowing. The swallowing component of feeding is described as a complex process in which saliva, liquids, and foods are transported from the mouth into the stomach. Even though swallowing assessment was not a keyword included in the present study search, it was expected that, as an important part of feeding, it would be included in the feeding assessment in the majority of the studies. Accordingly, it could be implied that a swallowing assessment was provided to all infants who were clinically assessed for feeding. However, a clinical swallowing assessment can only be provided by speech pathologists, which were included in just 7.5% of studies. Moreover, the literature indicates that the prevalence of swallowing disorders is up to 40% in premature infants 74 ; 39% in infants with congenital heart disease 74 ; up to 99% in children with cerebral palsy, 75 and up to 83% in children with craniofacial disorders. 76 The exact prevalence of neonatal feeding or dysphagia is unknown, but it is estimated to occur in approximately 25%-45% of typically developing children. 77 Therefore, it was expected that all studies that involved a speech pathologist would include a bedside swallowing assessment, which was not evidenced by the current review.
ASHA’s 73 proposed infant clinical feeding and swallowing assessment highlights recommendations for children aged from birth to 1 year of age and infants in the NICUs. It is suggested that a clinical evaluation should start with a case history based on a comprehensive review of medical records and interviews with the family and healthcare professionals. 73 Next, the speech pathologist should assess: overall physical, social, behavioral, and communicative development; gross and fine motor development; cranial nerve function; structures of the face, jaw, lips, tongue, hard and soft palate, oral pharynx, and oral mucosa; functional use of muscles and structures used in swallowing; head/neck control, posture, oral and pharyngeal reflexes, and involuntary movements and responses in the context of the child’s developmental level; observation of the child eating or being fed; functional swallowing ability; skill maintenance across the feeding opportunity; impression of airway adequacy and coordination of respiration and swallowing; developmentally appropriate secretion management; and modifications in bolus delivery and/or use of compensatory techniques on the swallow. 73
However, the clinical feeding and swallowing assessment proposed by ASHA was not observed in the studies that indicated having included this type of assessment.
The majority of the studies that described a clinical feeding or swallowing assessment only included parts of what is recommended by ASHA, 73 such as the oral motor assessment, which was included in 20% of the studies, and oral feeding readiness, which was included in 7.5% of the studies. Since 52.5% of the studies included preterm infants and 30% included infants in enteral or parenteral feeding, it was expected that most of the studies incorporated those assessments. The oral motor assessments aim to evaluate the functional use of the oral and facial muscles, including muscle movements, coordination, tone, strength, symmetry, and sensation. 73 This assessment is important because the feeding act depends on an integrated sequence of coordinated movements of over 20 different muscles to properly prepare the bolus in the mouth to be swallowed.78, 79 The oral feeding readiness assessments aim to evaluate if the infant has all the necessary functions and skills to start oral feeding safely by assessing the behavioral organization, oral posture, oral reflexes, and non-nutritive sucking before testing nutritive sucking and swallowing. 33 Therefore, oral motor assessments and oral feeding readiness are extremely important when assessing the feeding skills of preterm infants and infants in enteral- or parenteral-feeding.
Breastfeeding assessments and screenings were included in a few studies in the current review. Among the 40 studies that assessed neonatal feeding, only 17.5% included a breastfeeding assessment or screening. Additionally, three studies (7.5%) reported data on feeding volume and duration, and just one study (2.5%) examined maternal nipple condition. That was not expected since 72.5% of the studies assessed infants who were being breastfed. It is unclear if the other studies that provided clinical feeding and swallowing assessments included breastfeeding or not. This data highlighted a discrepancy between the promotion and guidelines for breastfeeding proposed by the Baby Friendly Hospital Initiative 2 and the experience in the hospitals.
Even though swallowing assessment, oral feeding readiness, oral motor assessment, or tongue-tie assessment were not keywords included in the present study search, it was expected that some of the studies would include one or more of those assessments. However, the lack of consistency in those assessment methods and tools was not expected. The findings of 19 different feeding/breastfeeding (12), swallowing (3), oral feeding readiness (2), oral motor (2), and tongue-tie (1) assessment methods, tools, and screenings were described and included to assess feeding skills in neonates. The variety of assessment methods and tools available goes beyond the assessments described in this study. According to the literature, 80 there are around 18 relevant assessment tools for feeding evaluation in infants younger than 6 months, and 15 of those tools did not show up in this systematic review. Furthermore, the majority of the feeding assessment tools used can be applied by any healthcare professional and do not require training to be used; however, not all healthcare professionals are provided with the necessary knowledge about breastfeeding as part of their degree.81–83
Considering the many factors that can influence breastfeeding, many studies suggest that a multidisciplinary assessment is the best approach to evaluate breastfeeding.10, 66, 84–86 However, only 12.5% of the eligible studies had two or more assessors from different disciplines. The consequence of a unidirectional approach is inadequate support for addressing early breastfeeding challenges, based on a lack of collaboration among various healthcare providers and the family. 87 The literature indicates that improving interdisciplinary collaboration could lead to better support and management of breastfeeding problems. 87 Additionally, many studies pointed to the limited knowledge that healthcare professionals have to support breastfeeding,88–91 emphasizing the importance of standardization in breastfeeding education and a multidisciplinary approach to breastfeeding.91, 92
Strengths and Limitations
This review provides valuable insight into the most commonly used assessment tools and methodologies for evaluating neonatal feeding skills, offering a broad perspective on current practices. A major strength of this research lies in its focus on the most frequently utilized instruments, regardless of their validation status, revealing a crucial gap in the field: widely used tools are not necessarily the most reliable or effective. This finding highlights an important disconnect between usage frequency and tool quality, which can have significant implications for the accuracy of assessments and subsequent feeding interventions. However, the primary limitation of this study is that it includes tools and methods based on their frequency of use, rather than limiting the analysis to only those that are validated. As a result, this review may incorporate lower-quality assessments and overlook potentially more comprehensive tools that are less commonly used. Despite this limitation, the inclusion of both validated and non-validated tools underscores a key issue in the field—reliance on frequently used tools without ensuring their efficacy—thus contributing to the broader understanding of how these tools impact neonatal-feeding assessments.
Conclusion
The variability of feeding assessment methods and tools for infants indicates a lack of standardization in breastfeeding assessment. The results of this research suggest that all described feeding or breastfeeding assessment tools are not comprehensive and person-centered as they do not even include all major aspects that can impact breastfeeding. Therefore, a consistent approach to breastfeeding assessment in hospitals is recommended to increase the incidence of breastfeeding success in the first 6 months of life. Finally, healthcare professionals who would like to promote, assess, and treat breastfeeding difficulties should pursue additional training or credentialing in breastfeeding and maternal-infant health.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval and informed consent were not required to conduct a systematic review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.