
Abstract
Objective
Current formulae used by clinicians to estimate the insertion length of umbilical catheters are inaccurate. We aimed to derive a new model that could improve accuracy in estimating the insertion length of umbilical catheters.
Study design
This was a multi-centre prospective observational study of neonates admitted to neonatal units and needing umbilical line(s) inserted for clinical reasons. Demographic data, catheter-related measurements and a new external length measurement—sternal notch to the umbilicus, were collected at three tertiary-level neonatal units in South Wales, UK. Generalised linear models were used to estimate the fit of the external length, birthweight, gestation and head circumference with catheter length and to derive a formula. The best fit was estimated by comparing r2 values for each equation.
Results
Data from 113 infants for each venous and arterial line were analysed for the new mathematical formulae. For both umbilical arterial catheterisation [
Conclusion
Our prospective multi-centre observational study identified a quadratic model based on birthweight as the best fit for estimating the insertion length of umbilical lines in neonates. This is a new finding and further development on earlier birthweight-based linear models.
Introduction
Umbilical venous (UVC) and arterial catheterisation (UAC) in neonatal intensive care provide secure access to deliver fluids and medications whilst allowing monitoring and accurate blood sampling. 1 It also minimises handling and pain associated with procedures. 1 However, several risks are associated with their use and umbilical catheters need to be placed in the correct position, ideally on the initial insertion. Failure to achieve this leads to further catheter manipulation, additional radiation dosage and increased risk of infection, alongside thermal and clinical instability of the sick neonate. 2 Furthermore, catheter malposition has many associated complications including vessel perforation and injuries such as liver haematoma, cardiac tamponade and ischaemic impairment.3–6 The recommended position for UVC is thoracic vertebral level 8–9 (T8–9) outside the cardiac border; low positioning below T10 increases the risk of extravasation harm. 1 For UACs, the range T6–10 is accepted with T8 being ideal to avoid vascular complications.1, 3
Various formulae have been proposed and are in practice to predict the insertion length of umbilical catheters. Most of these are based on an external measurement 7 or birthweight. 8 Our recent systematic review of formulae for estimating insertion lengths and various studies comparing them identified numerous limitations regarding their reliability in predicting correct catheter placement. 9 We found that formulae based on external body measurements predominantly used non-fixed anatomical positions that were complex to use in practice, prone to error due to increased flexor tone in the neonate and resulted in an inconsistent application. Many formulae used birthweight as a linear variable to estimate the insertion length as it is simple to use and readily available. However, the relationship of birthweight to external length may not be linear at all gestations or for infants born small or large for gestational age, reducing the precision of the desired outcome of individual formulae. 10 Additionally, the original studies using birthweight as the explanatory variable included only a limited number of patients and considered the right atrium as the correct placement for UVC7, 8; this would result in an unacceptably high placement position by today’s recommendations. 1 When later studies compared these recommendations in practice, the UVC placement position in particular had low accuracy. 11
We hypothesised that an external length measurement between a clearly defined entry point and a fixed anatomical bony landmark—sternal notch to the umbilicus length (SNUL)—would be less affected by flexor tone, differences in birthweight and gestation and would minimise inter-observer variation in the measurement. To further investigate this hypothesis, we have undertaken a prospective multi-centre observational study to measure the SNUL, head circumference and birthweight across all gestations in both male and female infants, where umbilical catheters were considered appropriately positioned. Regression analysis was performed using this information to identify a best-fit model for the estimation of the accurate insertion length of umbilical catheters.
Methods
Setting
This was a multi-centre observational study conducted in three neonatal units in South Wales, UK. In the neonatal unit in Cardiff, patients were recruited between May 2018 and December 2021, except for a six-month interruption from March 2020 to August 2020 due to the COVID-19 pandemic. The neonatal units in Swansea and Newport started recruiting patients from September 2020 until December 2021. The original study was planned to be completed in December 2020. However, due to interruption by the pandemic and slow recruitment, the study was extended to recruit patients for another year till December 2021. All three units offer the full range of neonatal medical intensive care for all gestations; in addition, the unit in Cardiff offers neonatal sub-speciality services (foetal medicine, surgery, cardiology, endocrinology, respiratory, neurology, etc.).
Participants
The study sample included neonates admitted to the three neonatal units who required UACs and UVCs inserted for routine clinical care. Patients were recruited following confirmation of the appropriate positioning of umbilical arterial and/or venous catheters. Parents were provided with information leaflets and invited to participate in the study.
Inclusion Criteria
Infants admitted to the participating neonatal unit with umbilical arterial and/or venous lines inserted for routine clinical care. Each unit followed its existing guidelines for estimating insertion length based on birthweight; no recommendations regarding insertion length were made to the clinical teams for the research study.
The final acceptable position of the umbilical line (after initial insertion and adjustment) was achieved, that is, UVC between thoracic vertebrae 8–9 (T8–9) and outside cardiac silhouette; UAC between T6–10. Line positions were routinely checked by anteroposterior (AP) X-rays of the chest and abdomen in all three units within 30 minutes of insertion before using the line clinically.
Written informed consent from parents/guardians to participate in the study.
Exclusion Criteria
The final position of the umbilical catheter was outside the accepted range for the study as stated above.
Major abdominal wall defects or abdominal pathology (peritonitis, hydrops fetalis, necrotising enterocolitis) that could potentially affect SNUL measurement.
Suspected or confirmed skeletal dysplasia.
Major congenital abnormalities affecting birth weight or external features that would make an assessment of line position difficult.
Seriously ill infants who were not expected to survive were excluded from the study, and their parents were not approached.
Procedure
Once the position of the umbilical catheter was confirmed as acceptable (as per definitions in inclusion criteria) and written informed consent was provided by parents, the infant’s demographic information was obtained; birth weight, gestation, sex and type of umbilical lines inserted. Additional measurements were obtained from the neonate which included:
The SNUL was measured in centimetres (cm)—this was measured three times independently and recorded on the data collection sheet. The mean of the three measurements was used for data analysis. The length of the umbilical stump was measured in cm. The insertion length of the UVC and/or UAC in cm was identified using the printed markers on the catheter. The marker which was closest to the end of the umbilical stump was recorded. All three units use Vygon catheters with cm markings on them to identify length. For data analysis, the length of the UVC and/or UAC in centimetres was obtained by subtracting the length of the umbilical stump from the insertion length.
All data were recorded on a spreadsheet by staff involved in data collection. Identifiable data was pseudonymised by creating a study ID for each infant. At the end of the study, data were checked at each centre before being amalgamated for statistical analysis.
Statistical Analysis
The sample size was estimated using G*Power statistical software (Version 3.1.9.2, Franz Faul, Kiel, Germany). Using the F test family, a linear multiple regression with a fixed model that tests the R2 deviation from zero was used as the statistical test. A medium effect size was targeted (f2 = 0.15), with an α-error probability of 0.05, β of 0.2 (power of 80%), and 2 predictors (gestation and external length). The estimated sample size was 68 lines (each for UVC and UAC).
Data analysis was conducted on SPSS version 27 (IBM Corporation, New York, USA) and R for statistical computing (R Core Team (2021). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
Results
Over 3.5 years, a total of 167 infants were recruited from the three recruiting centres. Of these, 114 had UACs inserted (66 preterm infants and 47 term infants) and 113 had UVCs inserted (66 preterm infants and 40 term infants). One infant had missing data for UAC insertion and had to be excluded from the study. Thus, 113 infants were included per catheter in the final analysis. A table of baseline demographics collected as part of the study is presented in Table 1. Apart from UVC catheter length, which was shorter in centre 2, no statistically significant differences were observed in any other demographic variables.
Baseline Demographics of the Cohort.
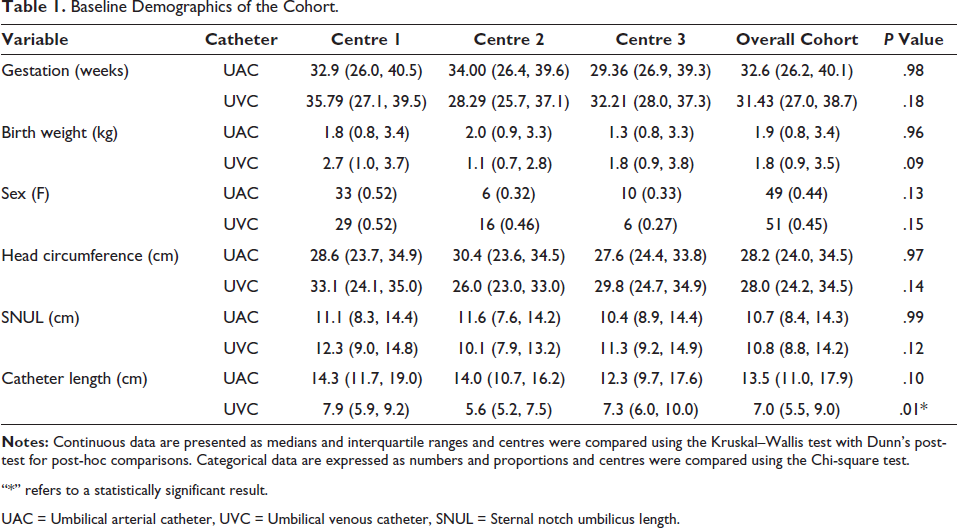
“*” refers to a statistically significant result.
UAC = Umbilical arterial catheter, UVC = Umbilical venous catheter, SNUL = Sternal notch umbilicus length.
All four potential explanatory variables—gestation, birthweight, head circumference and SNUL—were highly correlated with each other (Table 2). Thus, further regression analysis was conducted with each variable individually to avoid overfitting the model.
Correlations of Potential Explanatory Variables with Each Other.
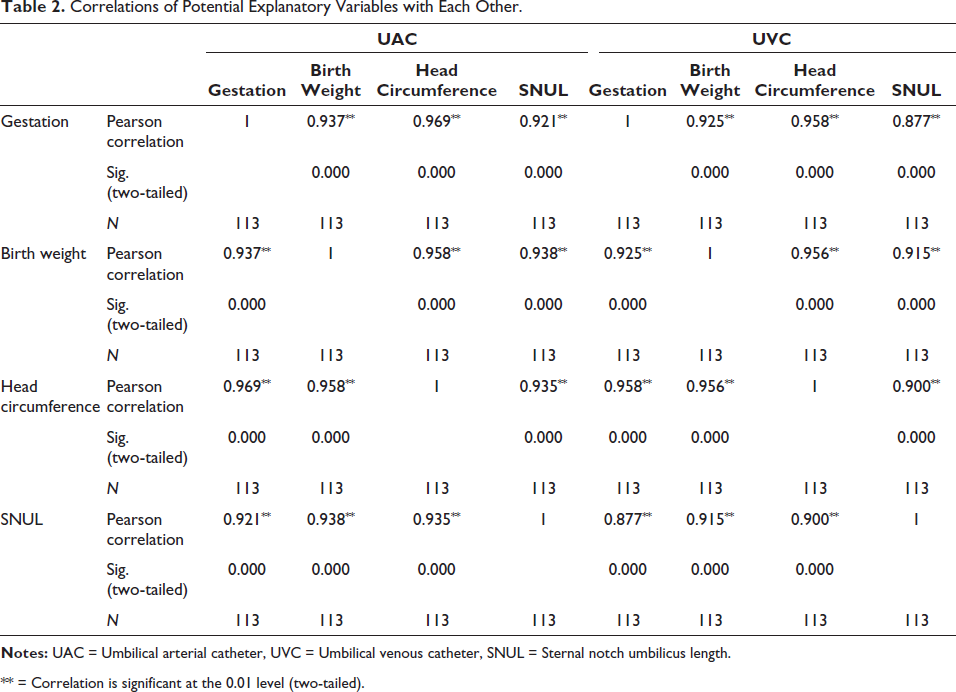
** = Correlation is significant at the 0.01 level (two-tailed).
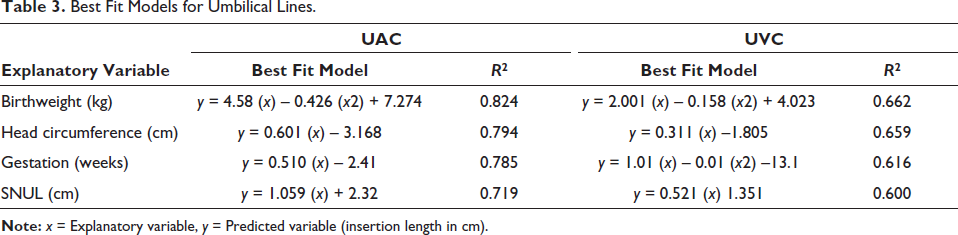
Table 3 summarises the regression analyses for the explanatory variables for each umbilical catheter. For both UAC and UVC, a quadratic model based on birthweight—UAC: y = 4.58 (x) – 0.426 (x2) + 7.274; UVC: y = 2.001 (x) – 0.158 (x2) + 4.023 where x = birth weight in kg and y = insertion length in cm—was found to have the best fit for predicting the insertion length of the catheters, although the overall fit for UVCs was poorer for all explanatory variables.
Best Fit Models for Umbilical Lines.
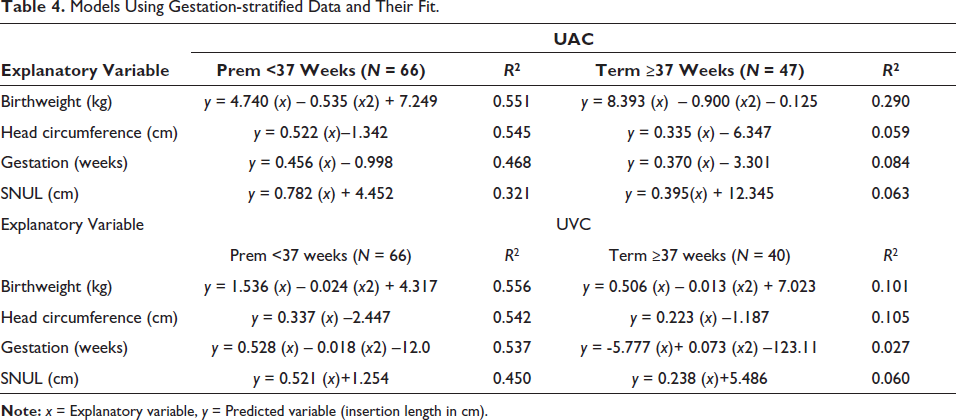
Models derived from subgroups of data (preterm or term infants) are presented in Table 4. A quadratic model using birthweight as the explanatory variable remained the best-fit model as assessed by the r2 values, but the overall fit for each subgroup (preterm or term) and each catheter type (UAC or UVC) was worse than the model using all data. Catheter length (UAC or UVC) from each subgroup of infants (preterm or term) was plotted against predicted length from the overall model or the subgroup model (preterm or term respectively) and is presented in the supplementary information. For UACs or UVCs, no substantial difference in fit was noted between preterm and term infants as assessed by their r2 fit.
Models Using Gestation-stratified Data and Their Fit.
Discussion
Our prospective multi-centre observational study identified a quadratic model based on birthweight to be the best fit for estimating the insertion length of umbilical lines in neonates. Of note, our original hypothesis—an external length between a clearly defined entry point and a fixed anatomical bony landmark would better predict internal length—was disproved. Currently, in all of the units, a birthweight-based linear model is used to calculate initial insertion lengths 8 ; however, we have previously identified unreliability in existing methods. 9 This new quadratic equation using birth weight to estimate the insertion length of UACs and UVCs may improve accuracy in estimating insertion length.
Although we had initially hypothesised that an external linear length would be better at calculating internal length, this was assumed to be on a two-dimensional axis. The catheters traverse a path that is three-dimensional and thus may explain our finding that a quadratic function performed better as a prediction model. This finding is novel and has not been reported before in the literature.
The umbilical vein (persisting left umbilical vein) travels intra-abdominally towards the porta hepatis where it joins the left portal vein. Blood flow continues into the ductus venosus that travels towards the inferior vena cava by entering the left hepatic vein at its confluence. 12 However, multiple anatomical variations of the umbilical vein and its course have been identified, which makes its internal course, and thus internal length, less predictable. 13 Thus, deriving a model of the internal length for an umbilical venous catheter from our observational study seems to be less accurate, although possibly still providing a better prediction compared to current alternatives. 9
As recommended in the BAPM guidelines, 1 all participating units use an AP chest radiograph view to confirm the position of the umbilical line tip. However, as the umbilical venous line has a complex course internally, the accuracy of a chest radiograph has been questioned in earlier studies.14, 15 In contrast, point-of-care ultrasound, which can be used in multiple axial planes, has been shown to have better accuracy in determining the position of the catheter tip immediately after insertion16, 17 as well as be used to detect migration of catheters after insertion. 18 A recent study also demonstrated that neonatal doctors can be trained to conduct real-time ultrasound during insertion to confirm the tip of the umbilical venous catheter. 19 The use of radiographs in our study, which demonstrates the line tip in 2-dimension, could be another reason for the lower accuracy of the model due to the inaccurate position of the line tip in the first place and consideration should be given to training neonatal staff and change the choice of imaging to confirm line position. While aspirational and desirable, it is a challenge in both resource-rich and under-resourced neonatal settings to provide 24-hour access to ultrasound imaging and train staff to reliably acquire and interpret the images for routine use. Until this happens our model may provide a much-improved resource for the accurate positioning of umbilical lines using simple AP views.
Previous studies have used different accepted positions for the tips of the umbilical catheters and have had small sample sizes.7, 8, 20–22 Our study was a multi-centre trial with a large sample size reflecting real-world situations. We have used current guidelines to confirm the appropriate positioning of the umbilical catheters which had been inserted according to the unit’s current protocol. 1 We, therefore, consider these as strengths of our study compared to the existing literature.
Our novel birth-weight-based quadratic equations for estimating UAC and UVC insertion length should be validated in prospective studies before use in clinical practice. In particular, these quadratic equations as formulae need to be compared with existing weight-based linear formulae used in current clinical practice.
Conclusion
Our prospective multi-centre observational study identified that a novel quadratic equation based on an infant’s birth weight may be more suitable for estimating the insertion length of umbilical catheters as opposed to SNUL, our original hypothesis for the study. Using a quadratic equation is more representative of a three-dimensional structure which may allow better estimating of umbilical catheter length being inserted into a newborn. Further validation studies are required to compare this to existing weight-based linear formulae before they can be implemented in a clinical setting.
Footnotes
Acknowledgements
The authors would like to thank all parents at the three neonatal units for agreeing to participate in the study and all staff for helping with data collection.
Data Availability Statement
All relevant data have been published as part of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was received from The Wales Research Ethics Committee 1 (reference number 18/WA/0117). The study was registered on
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Informed Consent
Written informed consent was obtained from the parents of all participants before inclusion into the study.