
Abstract
Background
Early Initiation of Breastfeeding (EIBF) reduces neonatal mortality up to three times, particularly in preterm and low-birth weight infants. Existing Lactation Support Program (LSP) of the institute tackles breastfeeding-related issues to achieve EIBF as early as possible for all delivered healthy infants. LSP was reformed by introducing new policy in February 2021 to achieve EIBF <1 hour in all healthy delivered neonates.
Aim
The aim of the study was to study the efficacy of new lactation policy of LSP on rates of EIBF and time to attain the first breastfeeding in late preterm neonates of gestational age 35+0 weeks -36+6 weeks.
Method
A ‘before-and-after’ design was used to study the effect of the new policy on EIBF at a tertiary care institute in India from January 2018 to March 2023. Impact was assessed by comparing baseline data in pre-policy (group A) with that of new policy (group B).
Result
Among 417 babies included, 336 and 81 belonged to group A and B, respectively. EIBF rates were 42% and 99% in group A and group B, respectively (p < .0001). Median time to initiate EIBF was 100 min IQR [85–117] in group A compared to 26 minutes IQR [19–37] in group B (p < .0001).
Conclusion
Lactation support program is an invaluable key practice for attainment of EIBF. Through simple measures, significant improvement in EIBF was possible in healthy late preterm population. This LSP can be considered as ideal model to be adapted at national level to improvise EIBF.
Keywords
Background
Despite 76% of deliveries now being institutional, only 41% neonates are breastfed within one hour 1 ; which is the definition of Early Initiation of Breastfeeding (EIBF). 2 It is considered ‘Essential Newborn care’. 3 World Health Organization has proposed EIBF as one way to reduce infant mortality rate and up to 1/5th of neonatal mortality. EIBF reduces neonatal mortality up to three times compared to those who did not receive EIBF. 4 The benefits are particularly pronounced for preterm and low-birthweight infants. 5 Maternal benefits of EIBF include uterine contraction and early placental separation due to oxytocin release secondary to early suckling and touching by babies. 6 A recent meta-analysis of three large trials conducted in India, Ghana and Nepal found that EIBF was associated with a 44% lower risk of neonatal mortality. 7
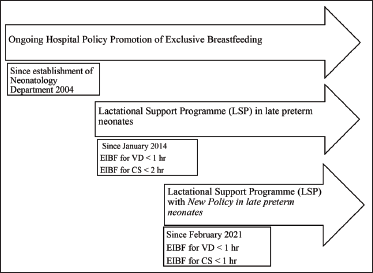
Every year around 15 million infants are born preterm. 8 Late preterm infants make up approximately 7% of the infant population and about 70%–75% of all preterm births. 9 Mothers of late preterm infants are more likely to have medical comorbidities that may adversely affect success of breastfeeding in addition to the anticipated prematurity-related factors. Our institute has achieved and sustained EIBF in full-term neonates 10 as have other institutes in their published data. 11 The Lactation Support Program (LSP) has existed since January 2014 (Figure 1). The components of LSP include counselling, assessment of infant-mother dyads post-birth, daily postnatal assessment, continuing support during follow-up. Interdepartmental coordination with the obstetrics department and nursing department is instrumental and facilitated by monthly internal meetings which are led by the Quality Initiative Chief. Four audits per year are conducted for review of EIBF rates and issues impeding. Three full-time lactation consultants (LC) are instrumental as the ground workers in the program assisted by neonatal consultants, pediatricians, and nursing staff. Studies regarding EIBF attainment in late preterm infants have been far and few, hence we sought to explore this lacunae by assessing the impact of new lactation policy of LSP on EIBF in the late preterm population. Existing LSP was reformed by introduction of a new lactation policy incorporating a standard timeline of attainment of <1 hour for all deliveries irrespective of the mode. We studied the efficacy of new lactation policy of LSP on rates of EIBF and time to attain the first breastfeeding in the late preterm neonates. We also wanted to study the same in different modes of delivery—namely Vaginal Delivery and Caesarean Section.
Timeline for Lactation Support Programme and New Lactation Policy for Late Preterm Neonates.
Methods
This before-and-after study was conducted in a tertiary care institute in India from January 2018 to March 2023. Newborn infants born intramural 35 0/7 days-36 week 6/7 days gestation who were healthy were included. We excluded neonates ineligible for EIBF requiring NICU admission. This was a before-after study design to assess the effect of new lactation policy of LSP on EIBF in late preterms. Prior to February 2021, breastfeeding was aimed to be initiated as early as possible, within two hours in infants born through CS and within one hour in infants born through VD. Breastfeeding was initiated only after mother was shifted to the Post Operative Anesthetist Care Unit (PACU) after completion of CS. Only after this wait period, breastfeeding could be initiated which inevitably led to a delay. In February 2021, LSP was reformed and a new policy was implemented for attainment of EIBF within one hour for all healthy babies including late preterms delivered by both VD as well as CS (Figure 1). Written documents regarding the same were circulated and communicated to the stakeholders. Through multiple discussions, analysis and audits, delay of EIBF was noted particularly in the post CS scenario. New policy planned to achieve EIBF within one hour by enabling support to mother and neonate dyad in the Operating Theatre (OT) with simultaneous closure of CS by surgeons by means of training the various staffs involved. This involved interaction of neonatologists with anesthetists and obstetricians. The training and education of all nurses in OT, PACU and neonatal unit were conducted by the LC. Ambient temperatures were ensured to keep at 26–28°C. Baby was wrapped appropriately and initiated on breastfeeding. Post direct breastfeeding (DBF), monitoring of infants in OT was ensured to prevent hypothermia. Post EIBF, neonate was shifted along with mother to PACU and eventually roomed in at postnatal ward for further routine newborn care.
Data on EIBF was collected by the team of LC. In circumstances when EIBF was not initiated within the stipulated time or delayed, feedback about the same was documented and audited.
Data of all the babies born were prospectively entered by LC, which included the demographic and clinical data of mothers, infants, time of initiation of BF. Demographic data such as maternal age, gravida, mode of delivery, gestational age and birth weight, and time taken for initiation of breastfeeding after birth of all eligible babies were extracted. Study Group A comprised infants enrolled from January 2018 to January 2021 before new policy implementation and study Group B comprised infants enrolled from February 2021 to March 2023—after new policy implementation. Outcomes assessed were the proportions of EIBF and time to initiate EIBF. Clearance from the Institutional Ethics Committee was obtained. Patient consent was waived off.
Statistical Methods
Data were represented as median, mean and standard deviation (SD), or number and percentage as appropriate. Chi-squared test was used for categorical data. Independent t-test and Mann Whitney U-test were used to compare parametric and non-parametric data, respectively. Skewness and kurtosis were used to assess the normalcy of the data. All analyses were performed on SPSS software version 25.0. A p value <.05 was considered statistically significant.
Results
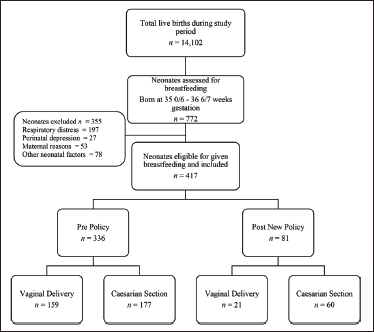
There were a total of 14,012 live births during the study period, out of which 772 were preterm of 35 0/7– 36 6/7 weeks gestation and assessed for eligibility (Figure 2). After excluding 367 infants needing NICU admission, total of 417 infants were evaluated for achievement of EIBF pre and post new policy. We had 336 in the Pre Policy Group, and 81 in the Post Policy Group.
Study Flow Diagram.
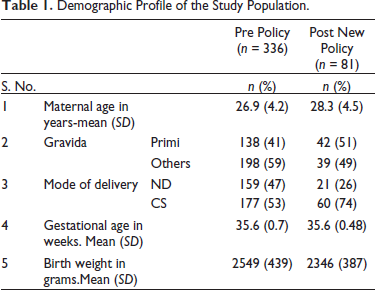
The baseline characteristics of the mothers and neonates were comparable between both groups (Table 1).
Demographic Profile of the Study Population.
Overall percentage of EIBF in group A was 42% which improved to 99% in group B (p < .0001) (Table 2). Overall median time to initiate EIBF was 100 minutes IQR [85–117] in group A which decreased to 26 minutes IQR [19–37] in group B (p < .0001)
Percentage of Achievement of EIBF and Time to Initiate BF.
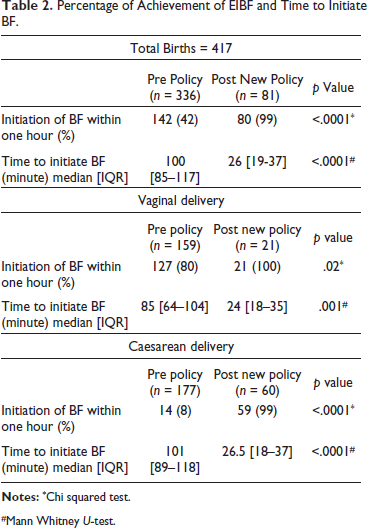
#Mann Whitney U-test.
Analysis was also performed based upon the mode of delivery. In VD, initiation of BF within one hour with VD rose from 80% in pre policy group to 100% in post policy group (p = .02). Median time to achieve EIBF in VD decreased from 85 minutes with IQR of 64–104 to 24 minutes with IQR of 18–35 (p = .001).
With regards to CS, initiation of BF within one hour had increased significantly from 8% in group A to 99% in post policy group (p < .0001). Median time to achieve EIBF in CS decreased from 101 minutes [89–118] to 26.5 minutes [18–37] (p < .0001).
Discussion
Our study shows statistically significant improvement of EIBF in healthy late preterm population from before to after implementing new policy of LSP at our institute. This indicates a successful and efficient implementation of policy through practice change and interdepartmental collaboration. One of the targets of Every Newborn Action Plan (ENAP) is to achieve EIBF in 90% of deliveries, which we could achieve in our study in both VD and CS post new policy. As per global survey across 24 countries including India estimated EIBF ranged from 17.7% to 98.4% (average 57.6%). Twenty facilities have participated in India and the EIBF rate was 65.8%. In this survey, EIBF was significantly lower in those delivered by CS. 12 CS has been reported to be a barrier for EIBF in a systematic review globally; experience of Middle Eastern mothers has similarly been falling short of the recommended duration. 13 Mothers who delivered by CS were less likely to achieve EIBF in various studies. 14 Indian experience has also been similar. 15 However, scope of improvement and roadmap was shown in a Quality Improvement Initiative, at a government hospital in India which demonstrated a significant and sustained improvement in first-hour breastfeeding initiation rates in neonates born by CS from baseline of 0%–93%. 11 Similarly, we were able to achieve EIBF less than one hour in CS as well as VD similar to another quality initiative study to improve first-hour BF.
The odds of EIBF were three times higher for mothers who had vaginal delivery than for those who had CS in various studies. 16 We had a similar experience, as the mother undergoing VD had a shorter median time to EIBF: 85 minutes as compared to 101 minutes in CS in Pre Policy Group. Similar results were observed in the Post New Policy Group. We observed statistically significant improvement in median duration for initiation of BF in VD and CS following New Policy.
The infants with LBW were less likely to be breastfed within one hour of birth. 15 Likewise, the odds of EIBF was 1.19 times higher for large-sized babies as compared to small-sized at birth. 17 LBW was the dominant factor that significantly correlated with delayed breastfeeding initiation. 18
Strengths: Pertinent but vulnerable late preterm population evaluated. Study is a part of an ongoing lactation support program. Post hoc power analysis is 100% for this study.
Limitations: Exclusive breastfeeding rates at six months were not analyzed.
Conclusion
Lactation support program is an invaluable key practice for attainment of EIBF. Through simple measures, significant improvement in EIBF was possible in the healthy late preterm population. Interdepartmental collaboration is crucial for implementation of any perinatal interventions. This LSP can be considered as an ideal model to be adapted at national level to improvise EIBF.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Consent waived off as this study is a retrospective analysis of prospectively collected data of Lactation Support Program quality initiative, and appropriate ethical clearance obtained (attached as supplementary document).
Ethics Committee Clearance Reference number : (IEC-NI/JUN/23/88/40).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.