
Abstract
Background:
In India, only 56% of mothers breastfeed exclusively for the first six months, as recommended. Given India’s extraordinarily high rates of preterm births, infant mortality, neonatal deaths and maternal fatalities, exclusive breastfeeding becomes even more crucial. There are many advantages of breastfeeding, but there are lots of barriers that need to be addressed. These problems need a proper objective assessment.
Aims:
To assess optimum positioning and attachment in mother-infant dyads, infant breastfeeding behaviour in the early neonatal period and early breastfeeding skills in mothers.
Methods:
A prospective cross-sectional study was conducted in the postnatal ward of a tertiary care hospital. In total, 208 full-term neonates (Age - 24 hours to 7 days) who were admitted to a postnatal ward of a tertiary care hospital and who were on direct breastfeeding were observed for breastfeeding. Objective assessment of breastfeeding was done by using the Bristol Breastfeeding Assessment Tool, Infant Breast-Feeding Assessment tool and LATCH tool. Statistical analysis was done by using SPSS version 25 with appropriate statistical tests.
Result:
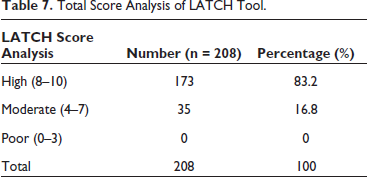
For the BBAT tool, 110 (52.9%) infants were well supported while feeding and 118 (56.7%) had proper latching or attachment. For IBFAT Score Analysis, 109 (52.4%) infants were effective vigorous feeders and 95 (45.7%) and 4 (1.9%) were moderately effective feeders and poor feeders, respectively. For LATCH Score Analysis, 173 (83.2%) mother-infant dyads achieved a high score and 35 (16.8%) achieved moderate score.
Conclusion:
Objective assessment of breastfeeding by using these tools will help to identify the problem related to breastfeeding for both baby and mother. Addressing a particular problem in a timely manner will help the mother and the baby to establish, initiate and sustain exclusive breastfeeding. Caesarean-delivered mothers as well as primiparous mothers both needed more focused counselling for breastfeeding positioning, motivation for early initiation breastfeeding, a strong supportive relationship, adequate assistance during the early neonatal period for breastfeeding and proper guidance to sustain exclusive breastfeeding.
Keywords
Introduction
Breastfeeding is a gift of nature to mammals and humans are one of them. It is an elixir of life for the baby’s growth and development. Breast milk provides neonates with the best nutrition, immunity, proper growth, development as well as metabolism. 1 One of the health interventions which is considered to be the safest and most effective for achieving Millennium Development Goal 4 (MDG - 4) is breastfeeding which decreases child death rates. 2 Non-modifiable breastfeeding determinants include maternal age, socioeconomic status, place of residence, parity and infant birthweight, while modifiable breastfeeding determinants include delivery method, self-efficacy, attitudes (influenced by religion), prior breastfeeding experience and social and professional support. 3 According to a review of Exclusive Breast Feeding (EBF) trends, the proportion of newborns in India who were exclusively breastfed rose from 46.4% to 54.9% over the course of the previous 10 years. 4 In India, only 56% of mothers breastfeed exclusively for the first 6 months, as recommended. As per data from NFHS-5 from the Union Health Ministry, in India as a whole, the percentage of infants exclusively breastfed has increased from 55% in 2015–2016 to 64% in 2019–2021. 5 Given India’s extraordinarily high rates of preterm births, infant mortality, neonatal deaths and maternal fatalities, EBF becomes even more crucial. 6 There are many advantages of breastfeeding, but there are lots of barriers that need to be addressed. These problems need a proper objective assessment. There is often use of a subjective “well/fair/poor” system to assess and document breastfeeding. To identify the factors associated with breastfeeding behaviour and to identify the problems related, the use of a valid and reliable measuring tool is important in providing guidance in breastfeeding education. The findings from the literature review show that there were studies performed using different assessment tools such as BBAT (Bristol Breastfeeding Assessment Tool), 7 IBFAT (Infant Breastfeeding Assessment Tool) 8 and LATCH tool 9 for understanding breastfeeding in detail. Consequently, it was observed that each tool tends to focus on different components and factors associated with breastfeeding. An intensified study involving all the components of assessment of breastfeeding was lacking. The present study was conducted with an aim of using the objective system to assess and document breastfeeding.
Aims
To assess optimum positioning and attachment in mother-infant dyads, infant breastfeeding behaviour in the early neonatal period and early breastfeeding skills in mother, to assess maternal and infant variables and to define areas of needed interventions.
Material and Methods
A prospective cross-sectional study was conducted among neonates admitted in the postnatal ward of an academically affiliated urban tertiary care hospital in western India. Data were collected from September 2021 to August 2022.
Inclusion Criteria
All full-term neonates (Age – 24 h to 7 days) were admitted to a postnatal ward of a tertiary care hospital and were on direct breastfeeding.
Exclusion Criteria
(1) All full-term neonates who were being fed expressed breast milk and formula feeds.
(2) All full-term neonates with age <24 h
Ethical Clearance
The study began after the approval of the study protocol by the Smt. NHL Municipal Medical College Institutional Review Board.
Data Collection
Initially, the mother was explained about the study, and written informed consent was taken from all the mothers entering the study in their local language for the same. After obtaining consent, neonates who were >24 h of life were observed for breastfeeding for a duration of 5 minutes. Simultaneously, all three breastfeeding assessment tools were filled. Breastfeeding observation was done for only one time. The breastfeeding assessment tools include the Bristol Breastfeeding Assessment Tool (BBAT). 7 Infant Breastfeeding Assessment Tool (IBFAT) 8 and LATCH tool. 9 Components of the BBAT tool are Positioning, Attachment, Sucking and Swallowing, and each component has a score of 0–2 with a maximum score of 8. Components of IBFAT are: In order to get a baby to feed, Rooting, How long from placing baby on the breast to latch and suck? and Sucking pattern. Each component has a score of 0–3 with a maximum score of 12. Based on the IBFAT total score, babies are categorising as Effective Vigorous Feeders (score: 10–12), Moderately Effective Feeders (score: 7–9) and Poor Feeders (score: 0–6). 8 Components of the LATCH tool are Latch, Audible swallowing, Type of nipple, Comfort (Breast/Nipple) and Hold (Positioning), and each component has a score of 0–2 with a maximum score of 10. Based on the LATCH total score, babies are categorising as High (score: 8–10), Moderate (score: 4–7) and Poor (score: 0–3). 10 Socio-economic status was assessed by using modified Kuppuswamy Classification-2020. In Kuppuswamy Classification, we took Occupation, Education and Income (per month) of the head of the family. 11 During the entire session, the confidentiality of the participants was maintained, and 1 female attendant was present.
Statistical Analysis
The data obtained from the participant’s mother were organized and analysed. Data were collected with the use of the proforma, and the extracted data were then entered in Microsoft Excel. Then, the study data were entered into the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, United States) software, version 25. Mean, median, and standard deviation were considered to describe continuous variables while frequencies were reported for categorical and nominal variables. Appropriate statistical evaluation was carried out as per the type and distribution of the data. Mann–Whitney U test was used for the calculation of the level of significance. Statistically significant results were considered at p-value <0.05.
Result
Table 1 shows that 59.13% of mothers included in the study were between the age group of 25 and 35 years. Regarding parity, 57.69% of mothers were multiparous and 77.4% of newborns were born via lower-segment caesarean section (LSCS). Only 20.67% of newborns were born with low birth weight (LBW). For counselling about breastfeeding, 32.21% of the mothers were counselled for the baby’s attachment and baby’s position for breastfeeding before the birth and 37.02% of the mothers were counselled for the baby’s attachment and baby’s position for breastfeeding after the birth.
Demographic Profile of Mother-Infant Dyads.
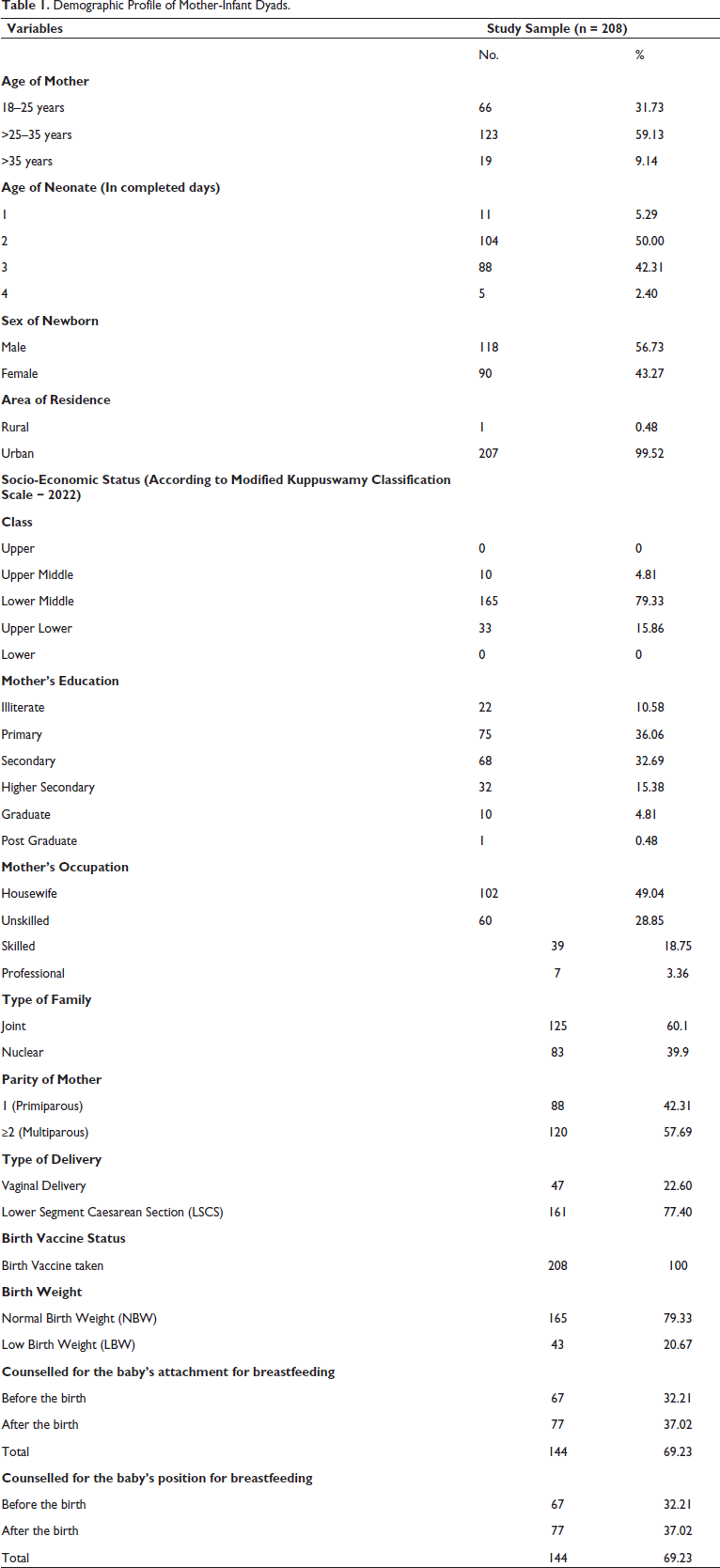
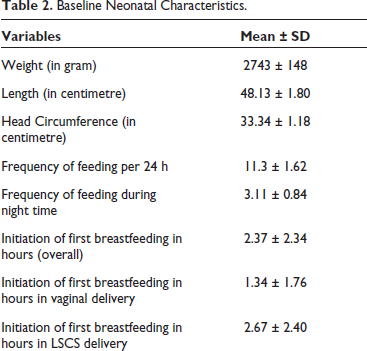
Table 2 displays the neonatal characteristics. The mean weight of neonates in the study was 2743 grams. The mean frequency of feeding per 24 h shows that on average, the babies were fed 11.3 times in 24 h, and the frequency of feeding during night time shows that on average, the babies were fed 3.11 times during the night. The mean time for initiation of first breastfeeding was 2.37 h overall, which was less for vaginal-delivered babies which was 1.34 h and more for LSCS-delivered babies, 2.67 h. Table 3 represents the categorization of study subjects according to the components of BBAT tool. BBAT tool mainly assess breastfeeding regarding babies’ behaviour during breastfeeding.
Baseline Neonatal Characteristics.
Components Analysis of Bristol Breastfeeding Assessment Tool (BBAT).
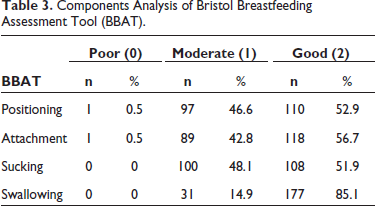
Table 4 represents the distribution of study subjects according to the components of IBFAT tool. This tool also assesses breastfeeding behaviour of baby in different way.
Components Analysis of Infant Breast-Feeding Assessment Tool (IBFAT).
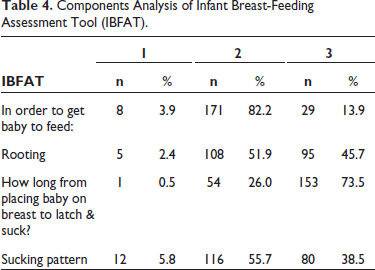
Table 5 represents the categorization of infants based on the overall IBFAT scores.
Total Score Analysis of Infant Breast-Feeding Assessment Tool (IBFAT).
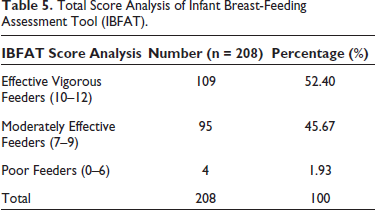
Table 6 represents the effectiveness of breastfeeding according to LATCH tool. This tool assesses breastfeeding considering the mother-infant dyad.
Components Analysis of LATCH Tool.
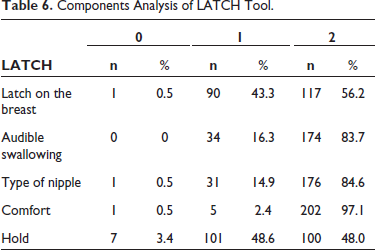
Table 7 represents the effectiveness of breastfeeding based on the overall LATCH score.
Total Score Analysis of LATCH Tool.
In different tools like BBAT, IBFAT and LATCH score, normal weight neonates performed better in terms of latching, sucking, stimulation for feeding, rooting and overall total score of that tool when compared to low birth weight neonates.
Discussion
The factors that influence breastfeeding are perceived seriousness/perceived susceptibility, perceived benefits, perceived barrier, maternal age, maternal education, maternal occupation/employment, maternal economic status, parity of mother, antenatal care, multiple births, type of delivery, birth weight/infant size and previous experiences with breastfeeding. 12 The four signs of good attachment are more of the areola is visible above the baby’s top lip than below the lower lip, the baby’s mouth is wide open, the baby’s lower lip is curled outwards and the baby’s chin is touching or almost touching the breast. The four signs of good positioning are with the infant’s head and body straight-facing her breast, with the infant’s nose opposite her nipple, with the infant’s body close to her body and supporting the infant’s whole body, not just neck and shoulders. 13
It was observed that the mean values of individual components of all three tools were higher among infants whose mothers underwent vaginal delivery; a significant difference was not observed when compared to the LSCS type of delivery. As the overall mean score was high in vaginal delivery indicating mothers were more comfortable in breastfeeding their babies than LSCS-delivered mothers who had some issues like pain at the sutural site, post anaesthetic effect, restriction of mobility for a few days, etc.
Cakmak et al. study found that significance with the mode of delivery in three components of the LATCH tool namely Latch on the breast, Comfort and Hold, and Sorkhani et al.’s study observed significance with the mode of delivery in all five components of the LATCH tool, while in our study, we found only one component (type of nipple) which was statistically significant. In the current study, the mean value was more for comfort and hold in caesarean delivery, while in Cakmak et al. study, the same mean value was high for vaginal delivery. Cakmak et al. study found a significant p-value in the overall LATCH tool score with respect to the mode of delivery, but our study did not find the same. In the present study, the mean total LATCH score of the vaginal delivery group was 8.66 and that of the caesarean section group was 8.65. Thus, no statistical significance was found (p value –0.95) but Sorkhani et al.’s study observed that the mean total LATCH score for vaginal delivery was 9.33 and for caesarean births was 7.21 which was statistically significant. (p-value −<0.00).14, 15
Multiparous women had previous breastfeeding experience which will help them to provide proper position and better attachment to baby in subsequent pregnancy. Primiparous is a lack of handling the baby so the baby to achieve the right position and attachment is late. As parity increases, the mother was more confident about breastfeeding with proper attachment and positioning. Baby care was better taken by multiparous mothers when compared to primiparous mothers. If the mother had a flat nipple, then proper syringing and adequate breastfeeding in first pregnancy (primiparous) will improve the outcome in further pregnancy.
In comparison to full-term, normal birth weight newborns, full-term, low birth weight babies fell under the Small for Gestational Age (SGA) group and had poor sucking and poor attachment for breastfeeding. Full-term, low birth weight babies were classified as SGAs because they lacked a well-developed buccal muscle and fat pad, had limited energy reserves, took longer to latch on to the breast, sucked ineffectively and required more stimulation while breastfeeding. Thus, these special LBW babies should be helped by putting them in Kangaroo Mother Care (KMC) which will not only decrease their energy expenditure for maintaining their temperature but also would improve mothers’ lactation. In order to begin breastfeeding, ensure milk transfer and avoid breastfeeding issues, an efficient sucking technique is thought to be crucial. Low birth weight babies experienced poor attachment and ineffective suckling, according to Goyal et al. 16 Our study also found similar results for low birth weight neonates, who had a poor latch on the breast when compared to normal birth weight babies.
Conclusion
Breastfeeding initiation and continuation are affected by multiple factors that are related to mothers and neonates. Objective assessment of breastfeeding by using these tools will help to identify the problem related to breastfeeding for both baby and mother. Addressing a particular problem in a timely manner will help mothers and babies to establish, initiate and sustain exclusive breastfeeding. Low birth weight babies should be helped by putting them in Kangaroo Mother Care which will not only decrease their energy expenditure for maintaining their temperature but also would improve mothers’ lactation.
Strength of Study
By using appropriate breastfeeding tools in the early neonatal period, one can identify the problem in breastfeeding for the baby as well as the mother, and timely intervention after assessment will result in sustained and exclusive breastfeeding.
Limitation of Study
This is a small pilot study from one tertiary care centre which uses three different breastfeeding assessment tools as no single tool can assess every aspect of breastfeeding. One can expand the study by involving multiple centres as well as different personnel like obstetricians and nurses.
This was a cross-sectional study, so the breastfeeding assessment was done only once. No data were collected after counselling of mothers whose babies achieved low scores while breastfeeding assessment during data collection. They can be further expanded by a prospective cohort study.
Footnotes
Authors Contribution
MBM: Concepts, Design, Definition of intellectual content, Data collection and analysis, and Manuscript writing. BDA: Concepts, Design, Definition of intellectual content, and Manuscript writing. RYD: Design, Definition of intellectual content, Data collection, and Manuscript writing. MVT: Design, Definition of intellectual content, and Manuscript writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study began after the approval of the study protocol by the Smt. NHL Municipal Medical College Institutional Review Board.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.