
Abstract
Background
Breast crawl is known to be the most natural, spontaneous, and logical method of initiating breastfeeding; however, not practiced routinely in many labor rooms.
Objective
The study’s primary objective was to examine the effect of breast crawl on breastfeeding in the first 48 hours.
Method
60 mother-infant dyads were included. Thirty infants were assigned to either Group 1 (breast crawl) or Group 2 (standard care) using a quasi-experimental design. All babies were observed for 1 hour. A blinded investigator did the LATCH (Latch Audible Swallowing Type of Nipple Comfort Hold) score and IBFAT (Infant Breast Feeding Assessment Tool) score at 24 and 48 hours.
Result
Out of 30 babies in the breast crawl group, 25 (83.3%) successfully completed breast crawl. 20 (80%) of 25 babies completed breast crawl within 45 minutes, and 5 (20%) completed within 60 minutes. LATCH and IBFAT scores were significantly higher in the breast crawl group than in the standard care group at 24 and 48 hours (p > .01). Scores were significantly higher after 48 hours compared to 24 hours in both groups (p > .01).
Conclusion
Most babies in the study successfully crawled the breast and took their first feed within 60 minutes. The breast crawl group had better LATCH and IBFAT scores, indicating a positive impact in the early postnatal period.
Introduction
Breastfeeding is the most cost-effective intervention in reducing neonatal morbidity and mortality. World Health Organization (WHO) recommends exclusive breastfeeding to lower neonatal mortality. 1 Neonatal deaths account for 47% of under-five child deaths globally and India contributes more than a quarter of it.2, 3 The NFHS 5 (National Family Health Survey 5) revealed that only 41.8% of infants are breastfed within 1 hour of birth, and 63.7% are exclusively breastfed at six months. 4 Early initiation is crucial to promote exclusive breastfeeding. Current evidence supports the practice of early skin-to-skin contact (SSC) for improving breastfeeding outcomes. It is classified as immediate if achieved within 10 minutes of birth and early if achieved between 10 minutes and 24 hours of birth. A Cochrane systematic review, which included 38 studies from 21 countries supports the use of SSC to promote breastfeeding. However, they did not find any difference in outcome between immediate versus early initiation or the contact length, 60 versus 90 minutes. 5 One recent WHO study found that 90 minutes of uninterrupted SSC maximizes the chance of breastfeeding. 6
A healthy newborn can crawl unaided toward the mother’s nipple and suckle successfully within 60 minutes of birth. 2 Both the mother and the newborn are mutually responsive in the most sensitive period of the half to 1 hour following delivery. Immediate and continuous SSC with the mother in the first hour induces a rise in oxytocin resulting in improved parent behavior. Newborn infants have a catecholamine surge immediately after birth due to the stress of the birth process. This results in heightened sensitivity and alertness, making the infant very receptive to odor cues and other senses, causing the baby to move toward the source. 7
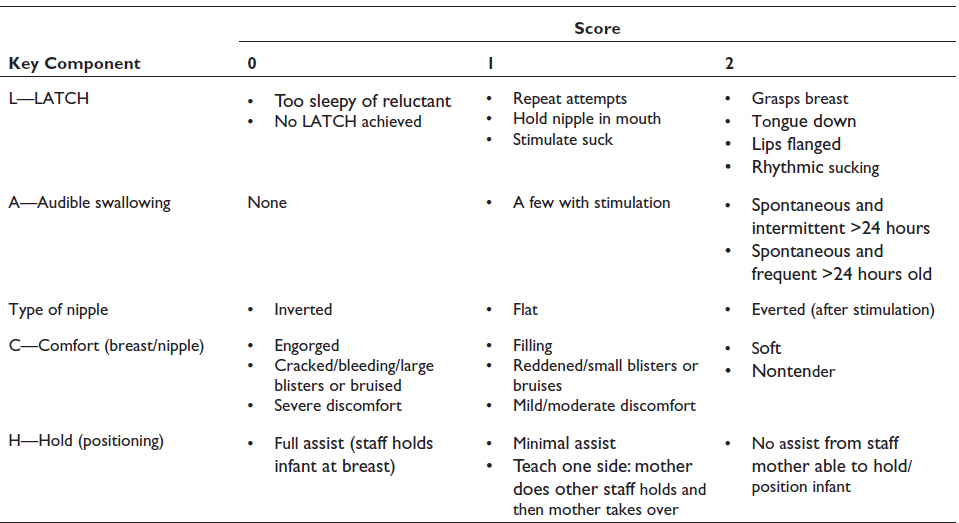
Tools like LATCH (Latch Audible Swallowing Type of Nipple Comfort Hold) and IBFAT (Infant Breast Feeding Assessment Tool) scores have been used to assess the effectiveness of breastfeeding objectively.8, 9
Despite the robust evidence pointing to the beneficial effects of early SSC, it is not commonly included within the standard care in many hospitals. Acceptability of breast crawl as a routine practice in the labor room remains a challenge due to various reasons like lack of awareness and training, hesitancy on the part of mothers and staff, inadequate staffing, etc. It is also not well studied whether all babies successfully crawl the breast and take their first feed within 60 minutes.
The primary objective of the study was to examine the effect of breast crawl on breastfeeding in the first 48 hours. The secondary objectives were to find the proportion of babies who succeed in breast crawl and the time taken to initiate and complete breast crawl.
Methodology
Participant. Recruitment
This quasi-experimental interventional study was conducted at a Medical College Hospital in Western Maharashtra, India. We employed convenience sampling to recruit study participants. Inclusion criteria comprised infants born by normal vaginal delivery, gestational age more than 35 weeks, an APGAR score (at 1 minute) greater than 7, and a birth weight above 1,800 g. Infants exhibiting respiratory distress, cyanosis, poor cry at birth, major congenital anomalies, and whose mothers could not be counseled regarding breast crawl or were unwilling to participate were excluded from the study. Pregnant women were explained the study protocol and the technique of breast crawl at the time of admission, and informed consent was taken before enrolment.
Subsequently, participants were allocated to either of two groups: Group 1 (breast crawl) or Group 2 (standard care). This allocation was primarily based on the self-selection by mothers, and it is essential to note that the assignment of infants to their respective groups was not randomized. Those mothers unwilling to participate in breast crawl were automatically considered in the standard care group.
The study included a total of 60 mother-infant dyads, with 30 in each group.
The study duration spanned from January 2021 to December 2021, with data collection occurring from March 2021 to August 2021. Ethical approval for the study was obtained from the Institutional Ethics Committee.
Training and Preparation
The hospital primarily serves high-risk pregnancies, with an annual average of 1,000 deliveries. Within the labor room, a sufficient nurse-patient ratio is maintained. Mothers and infants are routinely discharged after 72 hours following normal delivery. Before the study, labor room nurses were trained in breast to crawl through a lecture and demonstration through video by investigators. As part of our standard protocol, mothers receive comprehensive breastfeeding support, including counseling from nurses and doctors and two daily visits from lactation consultants until discharge. These consultations encompass guidance, addressing inquiries, demonstrating and monitoring breastfeeding techniques, and aiding with issues like inverted nipples. Thus, our hospital ensures comprehensive standard care to promote successful breastfeeding practices to all mothers.
Study Procedure
In Group 1, a baby who was vigorous at birth was dried properly except for the hands, Apgar scoring was done, and the infant was quickly examined for congenital malformations. The umbilical cord was cut after it stopped pulsating. The infant was then placed on the mother’s abdomen. The baby’s back was covered with a pre-warmed blanket and a dry head cap to prevent heat loss. The baby was kept on the mother’s abdomen for a maximum of 60 minutes and observed for crawling movements and latching. During this period, the researcher actively communicated with the mother regarding the importance of breastfeeding. The mother was guided to support the baby gently, if required. The infant’s heart rate, respiratory rate, and temperature were recorded at birth and at 60 minutes. The environmental temperature of the labor room was maintained at 28 ± 2 degrees centigrade. The mother was kept in the labor room for 1 hour till the first feed was given. Those babies who failed several attempts to latch (i.e., within 10 minutes) were given minimal assistance. The infant was dressed and weighed only after 1 hour.
The baby assigned to Group 2 (standard care) was managed according to the existing hospital protocol. They were received in a tray covered with a sterile towel and started with immediate care. The baby was then handed over to relatives and returned to the mother only after she was shifted to the observation room which took around 45 minutes if the mother had an episiotomy, and 30 minutes otherwise. Breastfeeding was initiated within 1 hour.
LATCH and IBFAT scores for both groups were simultaneously done at 24 and 48 hours by a single certified lactation consultant (GB) who was blinded to the allocation of participants.
Assessment Tools
LATCH score: This assessment comprises five components:
IBFAT score (Infant Breastfeeding Assessment Tool):
LATCH stands for Latch, Audible swallowing, type of nipple, comfort, and Hold. Each component is scored from 0 to 2. A score below eight is considered unsatisfactory. 10 Better LATCH scores in the early postnatal period correlate positively with exclusive breastfeeding at discharge and six to eight weeks.9, 11 IBFAT assesses a baby’s readiness to feed, root, fix, and suckle. It rates an infant’s suckling competence. Every component is assigned a numerical value of 0–3, and a score less than 10 is considered suboptimal infant breastfeeding behavior. 12
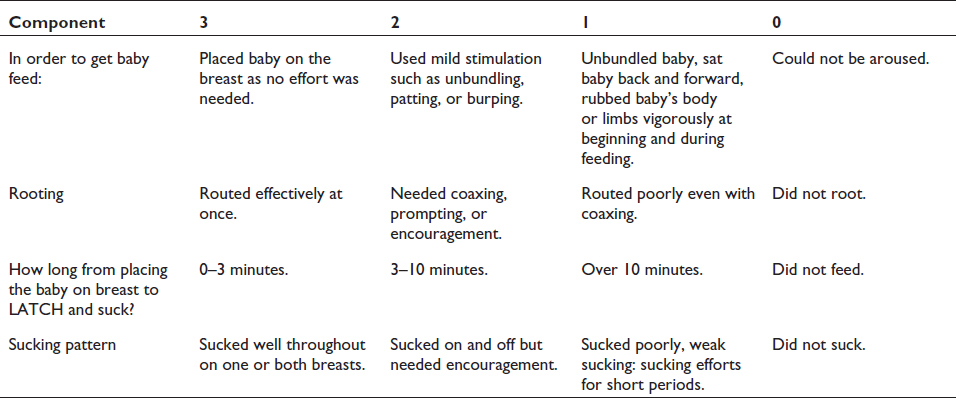
We employed both assessment tools simultaneously to enhance the depth of our observations. IBFAT, in addition to LATCH, provides valuable insights into the infant’s feeding behavior, including readiness to feed, rooting, and the time taken to latch.
Observations and Corrective Measures
A total of 60 breastfeeding sessions were observed in each group. Corrective measures were implemented for infants with a LATCH score of 7 or lower or an IBFAT score of 9 or lower. These measures included tactile stimulation and the use of the syringe technique for nipple pulling.
Breast crawl was considered successful when the infant completed the crawl and took the first feed within 60 minutes. Failure was defined as failure to initiate the crawl within 30 minutes, failure to complete the crawl and take the first feed within 60 minutes, or failure to latch.
Statistical Analysis
Descriptive statistics, like frequency, percentage, mean, standard deviation, median, and interquartile range, were obtained. Statistical tests like Chi-square and Mann–Whitney U were applied to compare baseline characteristics in both groups. A non-parametric Mann–Whitney U test was applied to compare the LATCH and IBFAT scores in both groups. Wilcoxon matched-pairs signed-ranks test was applied to compare the 24- and 48-hour scores of LATCH and IBFAT for both groups. IBM SPSS-22 and Microsoft Excel were used for the analysis.
Results
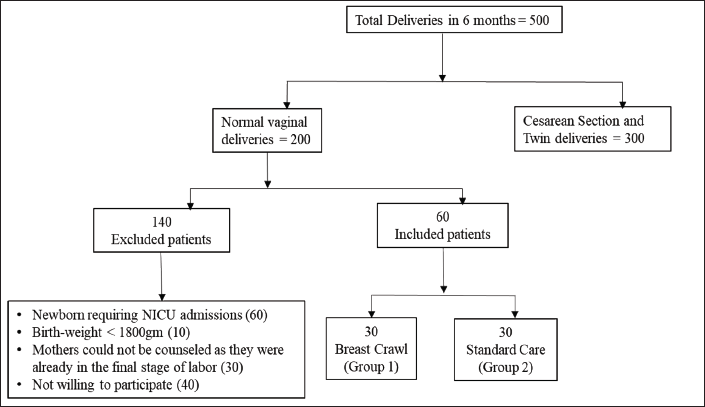
The flow chart of the enrolment of study participants is shown in Figure 1. A total of 30 infants each were included in breast crawl and standard care groups.
Flow Chart Showing Enrolment of Study Participants.
The general characteristics are shown in Table 1. There were nearly equal numbers of primiparous and multiparous mothers, and the majority (80%) were unbooked. Most of the babies weighed above 2.5 kg. Although most mothers knew about breastfeeding, none had heard about breast crawl or SSC. Inverted/flat nipples were observed in 40% and 46%, respectively, in Groups 1 and 2.
General Characteristics.
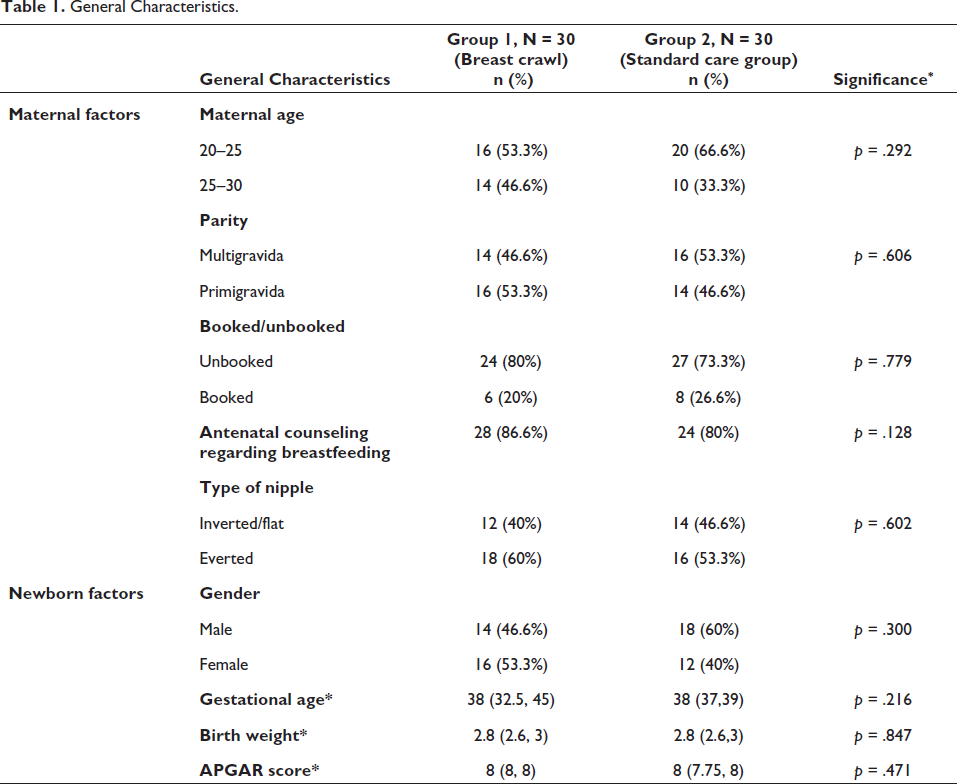
*Expressed in median (IQR).
Out of 30 infants in Group 1, 25 (83.3%) completed breast crawl within 60 minutes, and 5 (16.6%) failed breast crawl. Out of the 25 infants, eight required minimal assistance for positioning and latching. Among the five infants who failed to breast crawl, two did not complete the crawl, and three failed to latch. All the mothers whose infants either required assistance for latching or failed to latch had flat or inverted nipples. The median (IQR) time to initiate the breast crawl was 15 (10, 20) minutes, and to complete the breast crawl was 40 (32.5, 45) minutes.
LATCH and IBFAT scores at 24 and 48 hours were compared in both groups to assess the effectiveness of breast crawl. The breast crawl group had significantly higher median latch scores at both 24 and 48 hours than the standard care group, suggesting a positive impact of the breast crawl on breastfeeding (p > .01) (Table 2). Similarly, IBFAT scores at both the 24 and 48 hours were higher in the breast crawl group (p > .01) (Table 3).
Comparison of LATCH Score Among Breast Crawl and Standard Care Groups at 24 and 48 Hours.

Comparison of IBFAT (Infant Breast Feeding Assessment Tool) Score Among Breast Crawl and Standard Care Groups in 24 and 48 Hours.

The LATCH and IBFAT scores were significantly higher in both groups at 48 hours as compared to 24 hours, which is explained by the timely intervention and improvement in breastfeeding technique (p > .01).
Discussion
One of the most studied benefits of early SSC is its impact on breastfeeding. We evaluated the effect of breast crawl on breastfeeding in the first 48 hours using breast feeding assessment tools like LATCH and IBFAT scores.
In the study, 83.3% completed the breast crawl successfully, and 16.6% were unsuccessful. There is a wide variation in the success rates reported by different researchers. Girish and colleagues reported 100% success, whereas a study by Nair et al. reported successful breast crawl in 93% and Tiwari et al. in 83% of babies.13–15 Lower success rates ranging from 58% to 73% were reported by various other investigators.16–19
Most (68%) babies initiated breast crawl within 15 minutes, and all within 30 minutes. The majority (80%) completed breast crawl within 45 minutes, and the remaining (20%) within 60 minutes. The median time to initiate and complete the breast crawl was 15 minutes and 40 minutes, respectively. A study by Girish et al. reported an average time of 20 minutes to initiate a breast crawl and 40 minutes for completion. 13 Similarly, the average time taken for a breast crawl was 45 minutes in a study by Heidarzadeh et al. 19
There is limited data on failed breast crawl and its possible causes. Some studies have reported pain due to operative deliveries/episiotomy suturing, maternal sedation, and failure to latch as essential factors for unsuccessful breast crawl.14, 19 The factors that positively influenced breastfeeding were “having information about the importance of breastfeeding” and “having prior experience of breastfeeding.” 19 Few infants in the breast crawl group required assistance for positioning and latching, and some failed to latch despite reaching the breast. We observed flat/inverted nipples in nearly half the mothers, which appeared to be the main reason for the poor latch. This indicates the lack of antenatal breast examinations and corrective approaches, as most mothers were unbooked. Simple interventions like tactile stimulation or nipple-pulling techniques should be practiced to prevent nipple problems.
There are nine distinct and observable developmental stages of newborn infants during the first hour. This is described as birth cry, relaxation, awakening, activity, resting, crawl, familiarization, sucking, and sleeping. The resting stage can be intertwined with all other stages. 16 It is important to keep in mind this resting stage as often this is misinterpreted by parents and staff, resulting in the infant being removed from SSC and labeling it as an unsuccessful crawl. Infants who still show foraging signs like opening their mouth, putting a hand in the mouth, etc., after 1 hour should be observed until they first begin autonomous feeding.
LATCH and IBFAT are two commonly used breastfeeding assessment tools. These methods focus on the mother’s positioning and attitude, breast condition, infant placement, latching, efficient feeding, baby’s health, and maternal experiences. 20 However, there are no clear and well-defined cut-off points. A recent study from Pune evaluating LATCH score at discharge reported a score of more than six predictive of weight gain and exclusive breastfeeding at six weeks. 9 Similarly, Vernekar et al. reported a LATCH score of less than six as a red flag for intervention. 8
We used both tools simultaneously to strengthen our observation. Schlomer et al. studied the association of the scores of the above two tools with maternal satisfaction. They found increased maternal satisfaction and lesser feeding problems with increased LATCH and IBFAT scores. 21 Altuntas et al. studied the validity and reliability of breastfeeding assessment tools and found a positive correlation between LATCH and IBFAT. 22 We observed satisfactory scores in the breast crawl and standard care groups at both time points. This is attributed to the strong breastfeeding support measures practiced as part of standard care in our hospital.
LATCH scoring can be used as an educational tool to improve the technique of breastfeeding and thus improve exclusive breastfeeding.8, 23 Higher scores of LATCH and IBFAT in both groups at 48 hours compared to 24 hours indicate the positive effects of timely intervention and correction of erroneous practices by our lactation support group. Though the difference in the median scores between the two groups was only one, improved scores suggest improved maternal satisfaction and a positive impact. Various studies from developing countries have reported the positive impact of early SSC.13, 24, 25 Though evidence supports the use of early SSC to promote breastfeeding, there is insufficient data to say whether it definitely promotes exclusive breastfeeding for up to six months. 5 This needs further validation. Improving awareness and training of health care professionals are crucial to make breast crawl a routine practice.
Conclusion
The majority of babies in the study successfully crawled the breast and took their first feed within 60 minutes, though some required minimal assistance for positioning and latching. Higher LATCH and IBFAT scores in the breast crawl group suggest a positive impact on breastfeeding in early life.
Footnotes
Limitation
The main limitation of the study is the non-randomized allocation of infants to the groups, creating the potential for selection bias. Second, the small sample size may limit the confidence and generalizability of the result. Third, scoring was done by a single researcher, so the inter-observer agreement could not be assessed.
Acknowledgment
We thank Mrs. Alka Gore, Assistant Professor, Biostatistics for her technical help.
Author Contributions
SSD conceptualized the study, critically evaluated and revised the manuscript. RC and GB were involved in data collection, analysis, and initial draft of the manuscript. All authors have approved the final version of the draft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online:
Ethical Approval
Study was approved by Institutional Ethical Committee (IEC no: 408/21).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.