
Abstract
Background
In the era of the 21st Century, Human Milk Bank (HMB) is making its tortoise steps towards revolution. The goals and objectives of this study is to compare five years of data between the Pre Human Milk Bank phase (2018–2021) and Post Human Milk Bank phase (2021–2023) in order to evaluate the morbidity and mortality profile of neonates fed with PDHM (pasteurized donor human milk) or MOM (Mother’s Own Milk).
Methods
A retrospective observational study was done in HMB, Neonatal Intensive Care Unit, Department of Paediatrics, Gmers Medical College, Gandhinagar, Gujarat. Data obtained retrospectively comparing pre-HMB Phase (4th August, 2018–3rd August, 2021) and post-HMB Phase (4th August, 2021–3rd August, 2023).
Results
Around 1822 newborns benefited from the establishment of the HMB and 2.89 lakh ml of milk from 188 donor mothers were gathered during the study. Bacterial contamination of PDHM was reduced. There was a reduction in mortality and morbidity profiles like sepsis rate, NEC/Feed intolerance and ROP. Duration of NICU stay was improved in all preterm babies.
Conclusions
In this study, mortality and morbidity outcomes improved and sepsis decreased after the establishment of the HMB with reduced time to reach full feeds and shorter hospital stay. It helps significantly in NEC cases. We concluded that the creation of an HMB will be more advantageous and useful for all preterm babies in order to achieve better results.
Keywords
Introduction
The greatest way to feed a baby is through breastfeeding since human milk is still the only milk that is specifically formulated and best suited for a baby. It should be encouraged for all mothers to breastfeed their children. When a woman is unable to nurse her child directly for whatever reason, her breastmilk should be expressed and given to the child. Pasteurized donor human milk (PDHM) is the next best alternative if the mother’s own milk is unavailable or inadequate.
Due to high rates of mortality and morbidity among LBW and very low birth weight (VLBW) population, India has special difficulties. About 20% of newborns in this nation’s hospitals have low birth weight, and there is a considerable death and morbidity rate associated with this condition.1, 2
Although human milk banking began technically about a century ago, the first HMB was established in the United States in the middle of the 1980s. The first HMB in Asia, called ‘Sneha’, was established in Mumbai in 1989; however, there are still too few milk banks in India (around 95, most of which are located in private hospitals). 3 The milk bank for this tertiary care centre was founded on 4th August, 2021.
Methods
Aim
The aim of the study is to compare five years of data from the Pre-Human Milk Bank phase (2018–2021) and Post-Human Milk Bank phase (2021–2023) in order to evaluate the morbidity and mortality profile of neonates fed with PDHM.
Objectives
To compare the mortality profile of neonates between pre-HMB Phase and post-HMB phase.
To assess socio-demographic factors among mothers participating in milk donation.
All neonates who are hospitalized and examined (term and preterm) and who are provided early donor human milk before being given their mother’s milk. All mothers who have donated milk in HMB milk.
Babies given MoM (Mothers’ only Milk)/PDHM not having NICU registration. Powder milk-fed babies.
From the data records kept in the HMB and Neonatal Intensive Care Unit at the Department of Paediatrics, Gmers Medical College, Gandhinagar, Gujarat, study period data for donors and recipients were gathered. Retrospective data from pre-HMB phase (4th August, 2018–3rd August, 2021) and post-HMB phase (4th August, 2021–3rd August, 2023) were obtained. STROBE guidelines are followed for reporting of collected data.
In this study, we looked at the basic characteristics of donors (type of delivery, gravida, residence, age and education status) and Day of life of recipients, as well as the quantity of human milk used for collection and processing and the degree to which donor milk was contaminated by bacteria after pasteurization. Data from 2018-2021 (pre-HMB) and post-HMB (2021–2023) were obtained. During pre-HMB phase, Institutionally approved powder milk was used as feeding for newborns admitted to NICU having insufficient Mother’s Milk.
The donor is sent to the appropriate breastmilk collection in the milk bank or in the milk collection facility after receiving the required counselling, determining their fitness for donation, obtaining written informed permission, taking their history, undergoing a physical examination, and collecting samples for laboratory tests. After the donor selects an expression technique for their breastmilk, professional personnel collect the milk while taking aseptic measures. Currently, it is best to avoid collecting breastmilk at home in this nation owing to the possibility of contamination. Before expression, the breast is cleaned with water just as effective as washing with a disinfectant. Milk is put into tiny (30 ml) containers after pasteurization and kept frozen for up to six months.
Pasteurized milk is tested bacteriologically after processing to make sure there is no sign of bacterial development. Each milk sample was inoculated onto a blood agar plate and incubated aerobically for 48 hours at 36°C in the microbiology lab that was approved by the hospital. The tainted milk was completely thrown.
Chi-square test was used for statistical analysis, and a significant result was one with a p value of less than 0.05.
Results
According to our study findings, 2.89 lakh ml of milk from 188 donor mothers was collected in the first two years following the formation of an HMB, helping about 1822 babies. The two organisms from PDHM that were most often detected were Staphylococcus aureus and CONS. The morbidity profile, which includes the rate of sepsis, NEC/Feed intolerance, and ROP profile, decreased as compared to the three-year pre-HMB data.
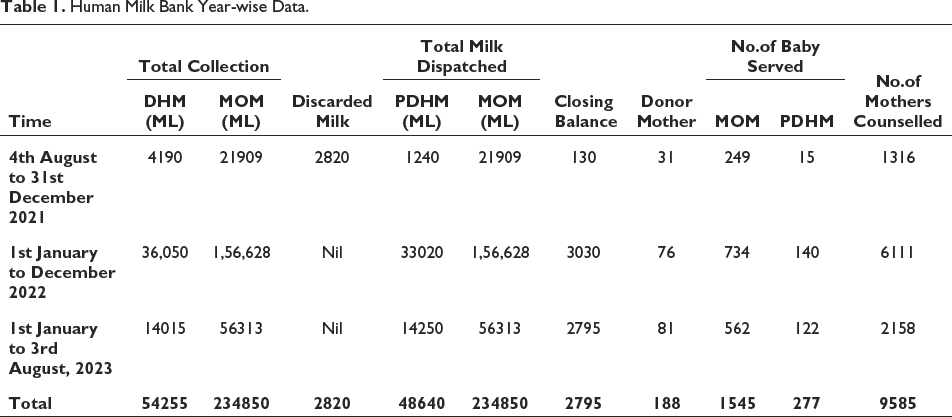
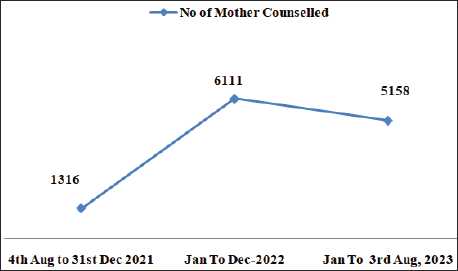
Table 1 reveals that in the last two years of the HMB, there were 188 donors, 2.89 Lakh ml of milk was collected, and 1822 receivers benefited from it. Donor numbers in each year increased subsequently (Figures 1 and 2). The number of recipients also rose in each year. This rise in numbers was brought about by counselling given to lactating mothers regarding the advantages of human milk for neonates.
Human Milk Bank Year-wise Data.
Number of Mothers Counselled Post-HMB Phase.
Number of Donor Mothers Post-HMB Phase.
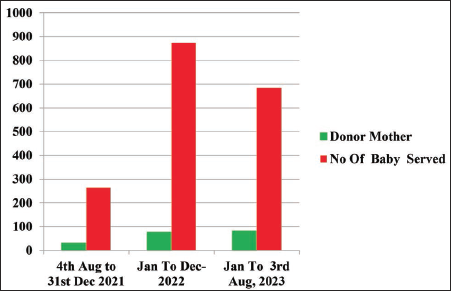
Table 2 lists the characteristics of the donor mother. The majority of the women (64.89%) were in the 20–30 year age group, were from rural areas (57.97%), had more multi-gravida (56.92%), and had more NVD births (75.54%).
Particulars of HMB Donor Mothers (N = 188).
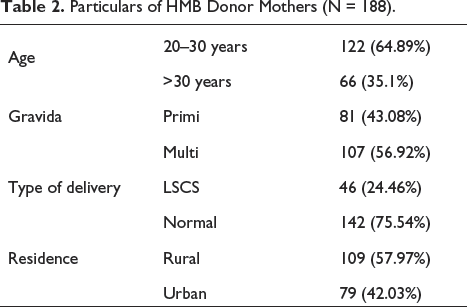
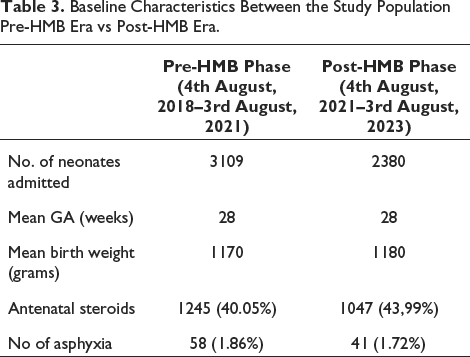
Table 3 shows baseline characteristics between the pre-HMB era vs post-HMB era study population. ANOVA test was performed and there is no statistical significance present.
Baseline Characteristics Between the Study Population Pre-HMB Era vs Post-HMB Era.
Data from two years’ worth of post-HMB were also compared. The contamination rate of PDHM decreased from 9.6% in 2021 to nil in 2023. P value was evaluated using statistical analysis, and the result was (0.0045), which is regarded as statistically significant. The fact that the PDHM contamination rate was lowered may be attributable to adequate storage conditions at the HMB, proper milk collection from donors, awareness of asepsis, and good hand hygiene techniques.
Human milk banks before (pre-HMB) and after (post-HMB) were examined for mortality and Morbidity profiles with regard to sepsis cases and NEC cases in Table 4. In comparison to pre-HMB (36.48%)), the mortality rate was lower in the post-HMB period (26.83%). The p value comes out to be statistically significant.
Analysis of Sepsis and NEC Cases (Pre-HMB and Post-HMB).
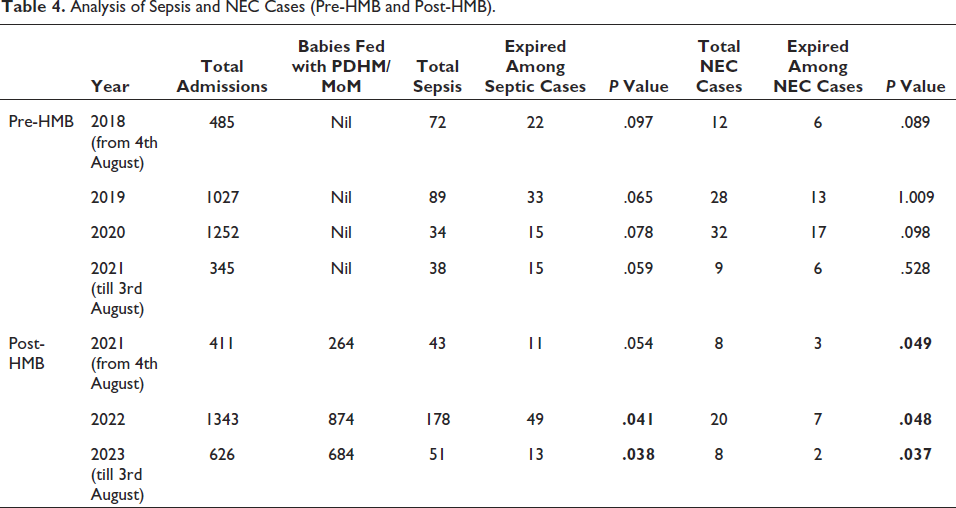
Data relating to the NEC’s morbidity profile were also compared between the years 2018-2023 (before and after the HMB). In comparison to pre-HMB (51.85%), the morbidity profile of NEC was lower in the post-HMB period (33.33%). P value was significant during post-HMB Phase. There were no incidences of bronchopulmonary dysplasia in neonates administered PDHM during the study period.
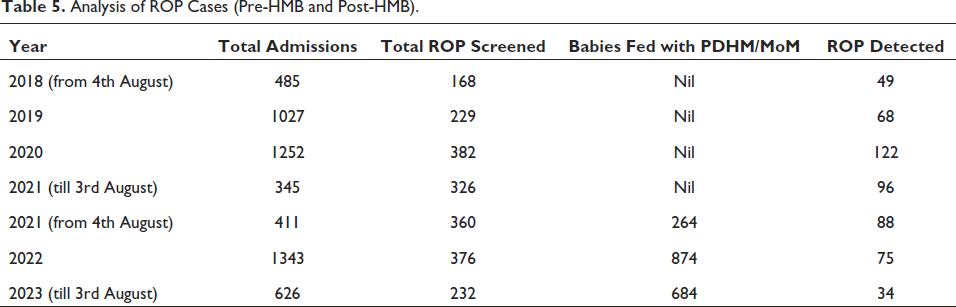
Table 5 and Figure 3 show a comparison of data about the ROP morbidity profile between the years (2018-2021) before HMBs and the years (2021–2023) after HMBs. ROP cases were found to be lower in the Babies fed with PDHM/MoM post-HMB.
Analysis of ROP Cases (Pre-HMB and Post-HMB).
Graphical Representation of ROP Cases Pre-HMB and Post-HMB Phases
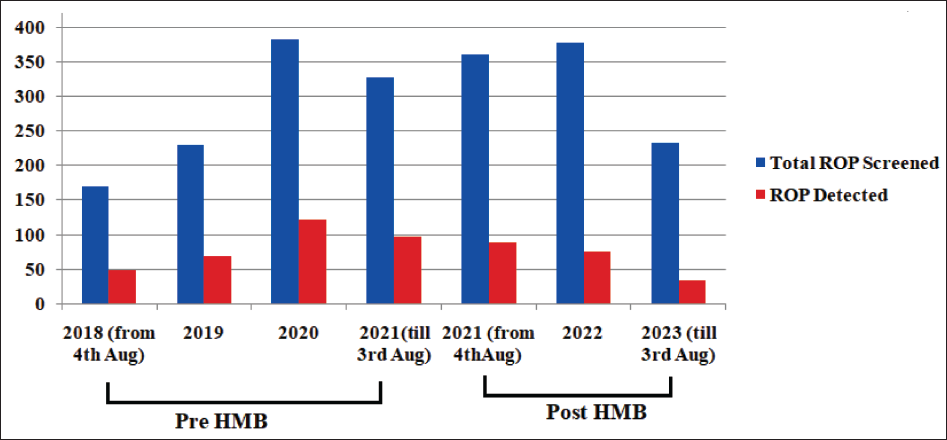
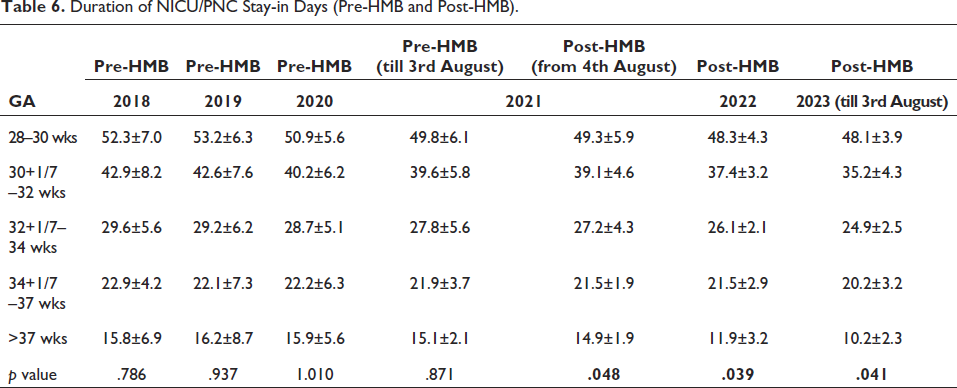
Table 6 shows the comparison of the information on the length of hospital stays between pre-HMB (2018–2021) and post-HMB (2021–2023) shows that post-HMB newborns spent less time in the hospital overall than pre-HMB babies. HMB babies took a shorter period to achieve full feeds than pre-HMB babies in all GA group babies which is also statistically significant.
Duration of NICU/PNC Stay-in Days (Pre-HMB and Post-HMB).
Discussion
Pasteurized human donor milk (PDHM) is suggested because to its well-known benefits for neonate nutrition, gastrointestinal health, host defence, and psychological well-being. 4 ‘Donor breast milk’ is the name given to milk that has been donated by one mother and processed by a milk bank so that it may be used by another mother who is unable to nurse her child.5, 6 A HMB is an organization that provides pasteurized donated human milk collection, screening, processing, storage, and distribution services. Lucas and Cole found that compared to neonates who also got breast milk, formula-fed neonates had a three times greater risk of developing NEC. Additionally, it was shown that neonates who exclusively consumed formula had a 610-fold higher risk of developing NEC than newborns who exclusively took breast milk.7, 8
Other research has shown that neonates who were fed formula had lower IQ scores than those who were breastfed. PDHM is therefore recognized as ‘the next best’ to breast milk from the biological mother.9, 10 Despite the numerous advantages, it is unfortunate that there are some situations where women are unable to breastfeed their neonates. In these situations, commercial baby formula frequently takes the role of breast milk. But donated breast milk can be a great substitute for formula.
We gathered the two years’ worth of data for this study from the HMB registration that would be kept at the NICU, Paediatric Department, we gathered information on the fundamental traits of the donor mother, including her age, place of residence, level of education, gravida, and method of delivery. In contrast to a Korean research by Jang et al., which found that most mothers were between the ages of 30–39, the majority of mothers (60.3%) were between 20 and 25 years old. 11 This can be explained by the Indian subcontinent’s younger marriage age and earlier pregnancy and delivery rates compared to western nations. The majority (79.9%) were urban residents, were first-time mothers (76.9%), and had literacy rates around (84.5%).
The most frequent organisms recovered from the pasteurized donor milk were staph aureus (66.6%) and CONS (33.3%), in contrast to Poonam Singh’s study, 12 where the most prevalent organisms were gram-positive bacilli (88.23%) and CONS (11.76%). 12 The morbidity profile of sepsis rate among newborns fed donor human milk was (26.83%) when compared to all admissions, and the p value (.0045) is regarded as statistically significant. The morbidity profile for NEC was reduced in the post-HMB period when comparing the pre-HMB (2018–2021) and post-HMB (2021–2023) phases. Study by Eun Jeon Kim contrasted with the Preterm formula group. 13
As a result, in this research, neonates that received mother’s own milk (MoM) first and then donor human milk (DHM) second showed reduced rates of morbidity and mortality, shorter stays in the hospital, and shorter periods to complete feeds. The majority of breast milk donations went to premature neonates, and now it seems that this tendency is getting stronger. Most recipients were preterm neonates, but donor milk was also requested for neonates and young infants for a variety of other reasons, including adoption, neonate’s refusal of formula, neonate’s milk allergy, mother’s decreased supply of breast milk, and mother’s chemotherapy for cancer or underlying diseases.
Human milk banking will be especially beneficial for preterm newborns who are at risk for necrotizing enterocolitis and neonatal sepsis, two conditions known to be associated with significant mortality and morbidity. It also makes it possible for them to get full enteral nutrition more quickly than they would be able to without human milk since it has potent trophic effects on the gut. 14 A meta-analysis of trials contrasting formula feeds with donor milk showed that donor milk significantly reduced the risk of necrotizing enterocolitis compared to formula.15–17
According to Hylander MA’s study, ‘Human Milk Feedings and Retinopathy of Prematurity Among Very Low Birth Weight Neonates’, neonates who were exclusively breastfed or whose diet comprised of 80% human milk had a much-decreased incidence and severity of retinopathy of prematurity. 18 Total infection incidence was 47% in the formula group against 29% in the human milk group.
Conclusion
HMBs provide an important function by providing human milk for preterm newborns, unwell or hospitalized babies, and other individuals who, for a variety of reasons, would not otherwise have access to mothers’ milk. In conclusion, as per our study, it clearly shows that early postnatal DHM feeding solely can lessen hospital stays and the time required to achieve full feeds while also protecting against a variety of morbidities, such as NEC and ROP. It also helps in decreasing mortality rate due to sepsis. Therefore, when mother’s own breast milk is unavailable, DHM might be the first choice as an alternative source of nutrition for both term and preterm neonates. We concluded that the creation of more such HMBs will be more advantageous and useful for all preterm babies in order to achieve better NICU outcomes which also in turn helps our Country to achieve SDG target of NMR.
Limitation
We could not assess the knowledge of health care providers, efficacy etc in rendering services in HMB, which might affects the outcome. For which, a futuristic KAP based study or prospective analysis might help to overall improvement of HMB.
Footnotes
Acknowledgement
My Department Faculty Dr Ekta Dalal, Associate Professor, Mrs Sweta HMB Nurse, Mrs Anita Rathore, Data Entry Operator, NICU were extended their helping hands during my study. The authors also acknowledge all the mothers and participants in the study. Dr Parijata Majumdar PhD (CSE) for her innovative ideas regarding presentation and publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Approved by Institutional Ethical Committee (IEC), GMERS MEDICAL COLLEGE, Gandhinagar, Gujarat.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.