
Abstract
Introduction
Human milk has many antioxidants like Docosahexaenoic acid (DHA), inositol, and vitamin E that combat oxidative stress deregulating VEGF which is implicated in the pathogenesis of retinopathy of prematurity (ROP). Thus, it is biologically plausible that human milk is protective towards ROP.
Aim and objective
The study aimed to find the association between ROP and breast milk feeding.
Methodology
The prospective cohort study was carried out for 18 months at the Newborn unit, SJH. In our study, mothers were asked to maintain a feeding diary (type of milk fed) and history was taken from the mother regularly. Each neonate was later assigned a feeding category including exclusively breast milk fed, more than 50% breast milk fed, more than 50% top milk-fed, and exclusively top milk fed. At four weeks of age, all these neonates were called to undergo screening for ROP. In the case of immature retina, neonates were followed up for repeat fundus exams and results were included in the study.
Result
A study on 521 neonates between birth weight of 1–1.8 kgs found that predominant breast milk feeding reduces the chance of any stage ROP (needing repeat screening or intervention). The total incidence of any stage ROP in this study was noted to be 16.2% where 4.1% of total neonates from the predominantly breastfed group as compared to 37.8% from the predominantly top-fed group developed any stage ROP.
Conclusion
Breast milk feeding has a significant benefit in reducing any stage ROP and ROP needing intervention, thus it has the potential to prevent a significant cause of childhood blindness.
What is already known
– Breast milk feeding may be protective towards ROP
What the study adds
– Breast milk feeding is independently protective towards ROP
Introduction
The rationale of the study was to determine the risk factors for retinopathy of prematurity (ROP) in preterm babies and to find the association between ROP and breast milk feeding. It is biologically plausible that human milk is protective to the development of ROP.(del - In our study, it was hypothesised that Breast milk feeding is protective against ROP and severe ROP.) Many studies relate the association of the incidence of ROP with breast milk intake but the results are conflicting and there is a very small amount of published data from India on the topic.
Developing countries including India are facing the third epidemic of ROP due to various factors such as increased survival of preterm babies, inadequate quality of neonatal care, and low coverage of screening and treatment services for ROP. 1 ROP is a dynamic, time-bound disease that is not present at birth. Several studies have proved early gestational age ≤30 weeks and low birth weight ≤1500 g as important risk factors in the development of ROP, there are also other factors such as poor weight gain, reduced insulin-like growth factors, increased percentage of oxygen in the inhaled air, hypoxia, respiratory distress syndrome, anaemia, blood transfusion, sepsis, etc., which have a significant impact. 2 While several studies have proven that proper oxygen saturation targets and reduction of large fluctuations of oxygen saturations help in reducing ROP, the data on the benefit of practices like breastfeeding to promote weight gain, use of kangaroo mother care, and measures to reduce the rates of sepsis in reducing ROP is still lacking or if present conflicting. 3
Human milk has many antioxidants like inositol, vitamin E, catalase, glutathione peroxidase, taurine, carotenoids and superoxide dismutase that combat oxidative stress from free radicals. Of these antioxidants, carotenoids are found in human milk but not in most formulae, and are preferentially accumulated in the eyes. By combating oxidative stress, these antioxidants down-regulate vascular endothelial growth factor which in turn halts neovascular proliferation implicated in the pathogenesis of ROP. Interestingly, oxygen toxicity is also reduced in infants fed human milk as compared with infants fed formula, supported by the finding that urinary 8-hydroxydeoxyguanosine, a marker for oxidative DNA damage, is significantly lower in infants fed human milk compared with infants fed formula. Docosahexaenoic acid (DHA) and IGF-1 in human milk have been seen to decrease the severity of ROP in VLBW infants. Thus, it is biologically plausible that human milk is protective to the development of ROP. 4
The association between BM intake and ROP has been studied with inconsistent results. Hylander et al., 5 Kao et al., 6 and Manzoni et al. 7 found breastmilk to be beneficial while Heller et al. 8 found no evidence that Breast milk (BM) intake reduces the risk of ROP. While in the study by Heller et al human milk feeds were initiated after the first week of life Kao et al. used either maternal or donor milk with no data on the proportion used and Manzoni et al. was a secondary analysis of the data. In a cohort study conducted by Fonseca et al., 9 the statistical significance was maintained only during the sixth week of life. While some studies were directly suggestive breast milk is protective against ROP, no published study from India supported this and some studies could not prove any protective effect of human milk intake on ROP.
Methodology
The prospective cohort study was carried out for 18 months duration at the Newborn unit, Department of Paediatrics, VMMC and Safdarjung Hospital in New Delhi. Ethical clearance was obtained from the institute’s ethics committee before the start of the study. Written informed consent was obtained from the parents of the enrolled neonates.
All these neonates need admission to the NICU at birth and mothers are assisted for feeding. Milk is initially fed via an orogastric tube to begin with and gradually shifted to cupfeeds followed by feeding from the breast. Breastmilk is preferred for all babies. If breast milk is not available, then LBW formula is fed.
In our study, mothers were asked to maintain a feeding diary (type of milk fed) and history was taken from the mother regularly. Each neonate was later assigned a category depending on the type of milk fed. Feeding categories included: exclusively breast milk fed, more than 50% breast milk fed, more than 50% top milk fed, and exclusively top milk fed. At 4 weeks of age, all these neonates were called for a follow-up examination to undergo screening for ROP.
The presence or absence of ROP was decided by the ophthalmologist by indirect ophthalmoscope who was unaware of the perinatal course of babies. Babies were examined after prior informed and written consent from attending parents.
If no ROP was detected at the initial examination, the infants were re-evaluated once every two weeks until their discharge from the hospital. Thereafter, the eyes were examined once in four weeks until 42 weeks of age when retinal vascular development was complete.
If ROP were detected, the examinations were performed every week till the disease started resolving or progressed to a threshold level. In such cases, treatment was provided after taking informed parental consent and in proper consultation with the ophthalmologist.
The neonates assigned as immature retinas by the ophthalmologist were called up again for ROP examination every two weeks (or sometimes weekly as deemed fit by the ophthalmologist). They were followed up in the study till an outcome ROP was assigned by the ophthalmologist.
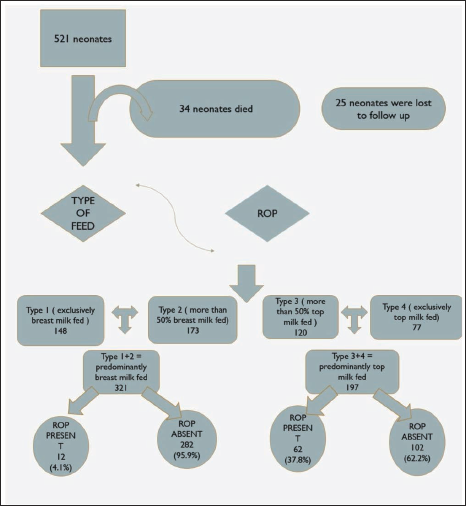
The same has been illustrated in Figure 1 along with the distribution of study paring each group.
Methodology Flowchart.
Inclusion Criteria: All live newborns with birth weight less than 1800 gm or below 34 weeks of gestation were enrolled in the study.
Exclusion criteria: Patient with ocular malformation. Sample size calculation: Considering the prevalence of ROP to be 13% from the previous study from our Centre on ROP: Risk Factors and Role of Antenatal Betamethasone in Indian Preterm Newborn Babies 10 conducted in the year 2014 in VMMC and SJH; alpha error of 0.05 and power of 80%, mortality as 15% and loss to follow up as 10% the number of babies required to be screened to detect any ROP was calculated as 520.
Study objective: A cohort study to compare the incidence of ROP in newborns less than 1800 gm belonging to the four respective feeding categories. Incidence and risk factors for ROP in preterm babies. Effect of breast milk feeding on regression of ROP. Effect of breast milk feeding on ROP requiring treatment.
Data Collection
Data regarding maternal factors was collected from maternal records. All the post-natal events were carefully recorded from the infant’s discharge record. All perinatal and neonatal data (including the ROP status) collected from each infant and maternal medical records were fed into a standardized data collection sheet for this study. The type of milk fed was recorded by verbal method & and later divided into four categories.
Statistical Methods
Analysis was done using the licensed statistical software package SPSS 21.0 version. A sample size of 521 was taken for the study. Data was entered into a predesigned Performa. The final data after the recording was entered into an Excel spreadsheet. For continuous variables, mean ± SD was calculated. For categorical variables, frequency tables and percentages will be calculated. For analysis enrolled neonates were divided into two groups: Predominantly breast milk-fed and predominantly top milk-fed. Predictors of ROP were evaluated using Univariate and Multivariate Logistic Regression Analysis. Variables that were significant in Univariate analysis will be entered into backward stepwise regression models in multivariate analysis. Odds Ratios (O.R.) and 95% Confidence Intervals (C.I.) were calculated for significant variables. All p values were two-tailed and values <.05 were taken as significant.
Result
A total of 521 neonates meeting the inclusion criteria (less than 1800 grams of birth weight or less than 34 weeks of gestation or both) were included in the study. None had to be excluded based on exclusion criteria. During the study, 32 neonates (30 during the initial assessment and 2 during follow-up) died and 24 neonates (18 during the initial assessment and six during follow-up assessment of immature retina) were lost to follow-up. This was well within the error percentage: mortality—6% against 15% taken into calculation and loss to follow up 4.5% against 10% taken into calculation.
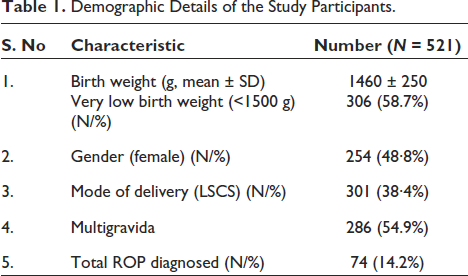
Demographic Details of the study participants have been demonstrated in Table 1. The mean birth weight of study participants was 1460 ± 250 gm and the mean gestation was 32 weeks with 306 LBW neonates.
Demographic Details of the Study Participants.
At the end of four weeks (i.e., at the time of ROP assessment), the study participants were assigned a category based on the type of milk fed—recorded as Type 1 (exclusively breast milk fed), Type 2 (more than 50% breast milk fed), Type 3 (more than 50% top milk-fed), Type 4 (exclusively top milk-fed) and later combined for ease of study into two groups Type 1+2 = predominantly breast milk-fed and Type 3+4 = predominantly top milk fed.
In our study, a total of 74 participants developed any ROP (64 during initial assessment and 10 during follow-up). Among these 43 participants developed stage 1 ROP, 23 had stage 2 ROP, 7 developed stage 3 ROP and only 1 had stage 4 ROP. While three participants needed medical treatment nine were given surgical treatment.
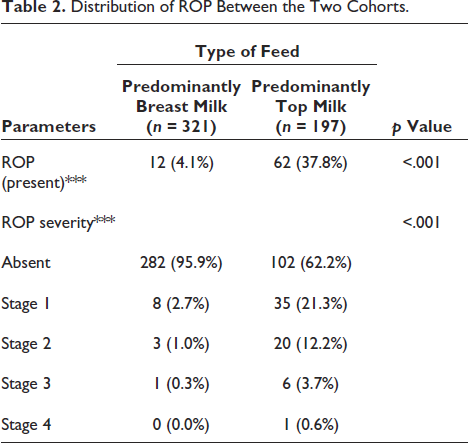
An inverse relation was observed between the type of milk-fed category 1–4 and the severity of ROP with ROP being less severe in the breast milk-fed versus top milk-fed group. The same is summarized in Table 2.
Distribution of ROP Between the Two Cohorts.
There was no significant difference between the various groups in terms of the distribution of ROP (Follow-Up Assessment) (χ 2 = 3.718, p =.105). This pointed out the fact that predominant breast milk feeding had little effect on the regression of ROP. The same has been summarised in Table 3
Distribution of Follow up ROP Among Two Cohorts.
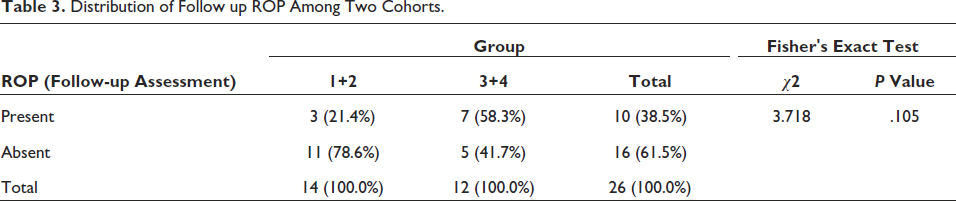
Table 4 looks at the distribution of neonates with ROP among the two cohorts—predominantly breast milk-fed vs predominantly top milk-fed. It is observed that only 4.1% of the neonates developing ROP belong to the cohort predominantly breast milk fed while 37.8% of the neonates developing ROP belong to the cohort predominantly top milk fed. Hence, the type of feed was found to be a significantly associated (p < .001) protective factor not only in the development of any ROP but also in severe ROP.
Risk factors of ROP.
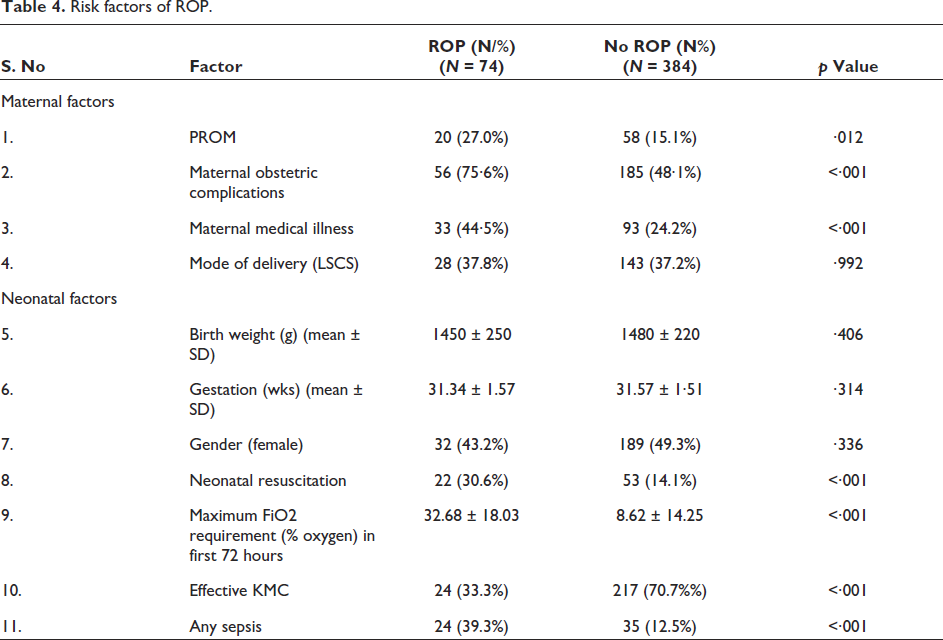
The baseline characteristics of the two cohorts were compared for various risk factors of ROP to determine the effect of confounders and select them for multivariate regression. It is observed that there is a significant difference (p value <.05) in the following parameters between the two groups: Birth Weight (Kgs), Gestation (Weeks), Medical Illness in the mother, Prolonged Rupture of Membrane (>18 hours), Mode of Delivery, FiO2 (%), Sepsis and KMC.
As a secondary objective risk factors for ROP were also studied. In our study following variables were significantly associated (p < .05) with the variable ‘ROP’: Obstetric Complication, Medical Illness in the mother, Prolonged Rupture of Membrane (>18 Hours), Need for Resuscitation at Birth, FiO2 (%) [Risk factors] and Uneventful hospital course (protective).
EOS, LOS, Sepsis Screen and Blood Culture are also significantly associated (p < .05) with ROP, that is, both clinical and culture-positive sepsis were found to be risk factors of ROP. Neonatal sepsis refers to an infection involving the bloodstream in newborn infants less than 28 days old. EOS refers to sepsis in neonates at or before 72 hours of life and LOS is defined as sepsis occurring at or after 72 hours of life. Hospital Course: RD HMD, RD MAS, Anaemia, NNH, SBA, Shock and significantly associated (p < .05) with ROP. Effective KMC has been found to protect ROP. Effective KMC was defined as any Kangaroo Mother Care done for more than six hours in 24 hours, for six consecutive days during the hospital stay or after discharge at home. The same has been summarized in Table 4. Breast milk has been found to protect towards ROP. Breast milk feeding was not found to be helpful in the regression of ROP as highlighted by the similar incidence of ROP in follow-up ROP between the two cohorts.
Six variables have been chosen for regression analysis based on significant differences between the two groups ROP present and absent. Birth weight and gestation are chosen as these two variables though insignificantly associated with ROP in our study are important risk factors of ROP and are unequally distributed among the two cohorts: predominantly breast milk fed and predominantly top milk fed. Table 5 summarizes the regression analysis for the dependent variable using all the predictor variables together in one go.
Multivariate Regression Analysis.
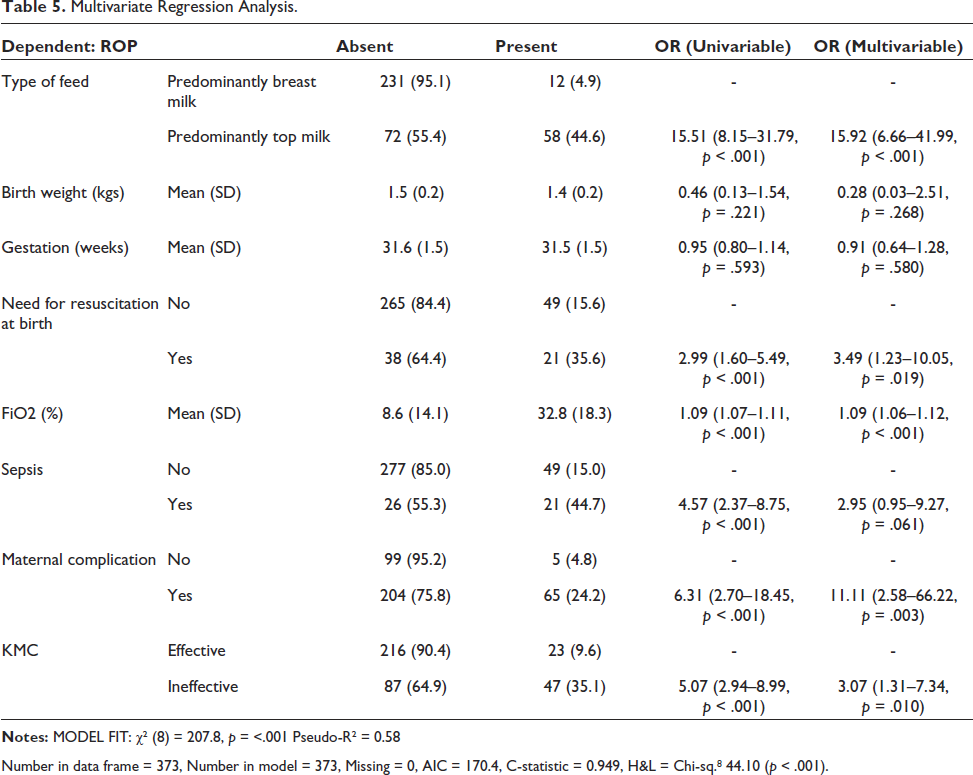
Number in data frame = 373, Number in model = 373, Missing = 0, AIC = 170.4, C-statistic = 0.949, H&L = Chi-sq. 8 44.10 (p < .001).
After multivariate logistic regression analysis, the study results highlight that Breast milk is a significantly associated independent protective factor to the development of ROP. Besides breast milk feeding, effective KMC (protective) and need for resuscitation, high Fio2 exposure and maternal complication (risk factors) were found to be independently significant risk factors for ROP.
Discussion
ROP is an important cause of preventable blindness in children. Improved survival rates of premature infants have increased the incidence of ROP. Approximately 15 million babies are born preterm worldwide each year and India has the highest number of preterm births.2, 5 In 2010, there was an estimate of 3,519,100 preterm births in India. 3 If 30% of these babies have access to neonatal care, about one lakh babies are found to survive each year. These babies are at risk of developing ROP hence increasing the need for augmenting services of ROP screening.
The incidence of ROP reported from India varies between 2.4% and 42% and in a few units, it is as low as 2.3% to as high as 42%, with study population varying from less than 32 weeks to 34 weeks and birth weight reported less than 1500 g and less than 2000 g. The special neonatal care units (SNCUs), which are the cornerstone of sick and low birth weight neonates in India report a 15% incidence of sight-threatening (ST ROP), which is ROP requiring intervention.56 Globally the reported incidence is between 15.2% and 42.7%. In our study, the prevalence of ROP was reported to be 16.2%. This is higher than the 13% prevalence reported in a previous study at our centre which may be explained by the increased survival of preterm and low birth weight babies who are at a higher risk of developing ROP.
ROP to a large extent is preventable by modifying certain risk factors. Though primary prevention of ROP begins with the prevention of preterm births, a multitude of other modifiable risk factors for ROP have been studied in the current literature. A systematic review of risk factors associated with ROP in 2018 identified around 300 published papers on ROP analysing various risk factors; gestation, birth weight and oxygen being the major factors and alternative factors including maternal, obstetric and medical factors, in addition to neonatal factors.1–4 The study from our centre in 2011–2012 found multiple gestation, blood transfusions, antepartum haemorrhage, pregnancy-induced hypertension, mechanical ventilation, and Apgar at 1 minute were found to be independently associated with risk of ROP48. In the present study, the following variables were significantly associated (p < .05) with ROP: Obstetric Complication, Medical Illness in the Mother, Prolonged Rupture of Membrane (>18 hours), Need for Resuscitation at Birth, FiO2 (%), Hospital Course: Uneventful (protective). EOS, LOS, Sepsis Screen and Blood Culture were also significantly associated (p < .05) with ROP suggesting that both clinical and culture-positive sepsis were risk factors for ROP. Hospital Course: RD HMD, RD MAS, Anaemia, NNH, SBA and Shock were also significantly associated (p < .05) as risk factors of ROP. Breast milk intake and effective KMC were found to be protective towards ROP.
Many studies relate the association of the incidence of ROP with breast milk intake but the results are conflicting and there is a very small amount of published data from India on the topic. Fonseca et al. 9 evaluated the association between human breast milk and ROP. The cohort study also showed that the amount of breast milk received in the first six weeks of life was inversely associated with the incidence of ROP of any degree. The study by Baljeet Maini et al. 10 shows, from our institute on risk factors and the role of antenatal Betamethasone in Indian Preterm Newborn Babies but no conclusion was drawn on the effect of breast milk intake on ROP. Heller et al. 8 found no evidence that BM intake reduces the risk of severe ROP (surgically treated) in extremely low-birth-weight (ELBW) infants (BW <1000 grams). Kao et al. 6 compared the incidence of ROP in newborns who received any amount of BM (from their mothers or a milk bank) and those who received only infant formula and found no significant association between the consumption of BM and ROP risk. While some studies were directly suggestive breast milk is protective against ROP, no published study from India supported this and some studies could not prove any protective effect of human milk intake on ROP. In the present cohort, the incidence of ROP was found to be higher in predominantly top-fed babies (37.8%) as compared to predominantly breastfed babies (4.1%).
Human milk has many antioxidants that are missing from most formulae, by combating oxidative stress, these antioxidants down-regulate vascular endothelial growth factor which in turn halts neovascular proliferation implicated in the pathogenesis of ROP. Docosahexaenoic acid (DHA) and IGF-1 in human milk have been seen to decrease the severity of ROP in VLBW infants. Thus, it is biologically plausible that human milk is protective to the development of ROP.
In our study, 28.6% of the participants had Type of Milk Fed: 1 (exclusively breast milk), 33.4% had Type of Milk Fed 2 (more than 50% breast milk fed), 23.2% had Type 3 (more than 50% top milk-fed) and 14.9% had Type of Milk Fed 4 (exclusively top fed). The data was then studied for similarities and differences making 2 cohorts—predominantly breast milk fed (1+2) and predominantly top milk fed (3+4). In our study—Birth Weight (Kgs), Gestation (Weeks), Medical Illness in the Mother, Prolonged Rupture of Membrane (>18 hours), Mode of Delivery, FiO2 (%) and Hospital Course were significantly different between the two cohorts. This is expected as mothers with the absence of any medical or surgical illness will find it easier to feed their babies.
When comparing PT, Very Preterm, and Extreme Preterm neonates the gestation more mother milk-fed the babies but this was not a confounder in our study as the mean gestation age when 1+2 compared to 3+4 was 32 weeks.
Larger babies with higher gestation were found to be more maternal milk fed as they have the necessary skills namely sucking rooting reflex to feed which will in turn increases the output of maternal milk by oxytocin-mediated response. Babies born vaginally as compared to caesarean-born babies were more breast milk fed as explained by the contraindication for sitting post a caesarean section and difficulties of feeding in lying down position. Neonates exposed to more oxygen or having an eventful hospital course (sepsis, respiratory distress, shock, SBA) were less maternal milk-fed—this is expected as the sicker the child more difficult the feeding becomes.
Many studies relate the association of the incidence of ROP with breast milk intake but the results are conflicting and there is a very small amount of published data from India on the topic. In our study, the incidence of ROP was found to be higher in predominantly top-fed babies (37.8%) as compared to predominantly breastfed babies (4.1%).
Two factors that have shown consistent and significant association with ROP in various studies: low gestational age, and low birth weight were not significantly associated with the development of ROP in our study but these two variables were unequally distributed between two cohorts and hence taken up as a part of the multivariate regression along with risk factors and protective factors significantly associated with ROP to determine if the type of feed, that is, breast milk feeding could be established as an independent or significant protective factor for ROP (any ROP including ROP requiring intervention).
In multivariate regression, type of feed: predominantly breast milk versus predominantly top milk fed was found to be significantly (p value < .001) associated with variable ROP. Another major risk factor for ROP: FIO2% was found to be significantly associated with ROP. Sepsis was not found to be significantly associated with multivariate regression.
It was ensured in the study that a trained ophthalmologist screened the neonates for ROP with proper tools, and techniques and in the presence of a nursing assistant and paediatrician in the protected environment of a nursery. The ophthalmologist was unaware of the perinatal course of the babies. The mother was asked about the type of milk fed by recall and diary method but advice to feed any particular type of milk was not given to prevent bias. The notes that were being lost to follow-up were called for the possible next visit. This was all done to ensure the quality of the study.
The strength of the present study lies in the fact that there is limited data analysing the effect of the type of milk fed on ROP in India The present study also takes into record ‘follow-up ROP’. The target population included in the present study, that is, 1–1.8 kg was chosen considering the operational aspect and feasibility of implementation in this group. Being an observational study, we have considered as many confounding factors as possible in both predominantly breastfed and predominantly top-fed groups as well as in ROP versus no ROP groups. The large difference in any stage ROP between the two groups (4.1% in predominantly breastfed versus 37.8% in predominantly top-fed) provides reasonable conviction to derive a rational conclusion despite the low event rate of any stage ROP. But breast milk feeding was not found to be helpful in the regression of ROP as highlighted by similar incidence of ROP in follow-up ROP between the two cohorts.
Limitations of the Study
As per recommendations <28 weeks need ROP screen at two to three weeks, in that scenario four weeks of screening as done in our study is delayed but the data at two weeks was not included in the analysis as it was incomplete many babies were very sick hence a delay in assessment was planned and some were missed at two weeks due to heavy workload at the hospital. According to RBSK all neonates <2 kg should be included in the study but the unit policy recommends less than 1800 gm so keeping in mind the feasibility and much higher incidence of ROP in less than 1800 gm this decision was made. Duration of respiratory support details are not mentioned in the study and it is one of the risk factors of ROP but the oxygen support data is inconsistent.
Reduction in ROP needing intervention is all the more important finding for resource-limited countries where trained ophthalmologists to provide laser therapy are scarce, there is a loss to follow and a large number of preterm births. Hence prevention of severe or sight-threatening ROP would be more effective than treating once ROP is severe. Moreover, laser therapy is not without its harms and long-term adverse effects, including unfavourable visual acuity, anisometropia and strabismus.
These findings of the added benefit of breast milk feeding on reduction in ROP would have a pivotal impact on care provision in various neonatal units especially in resource-limited countries as maternal milk feeding is an economic, viable and easily applicable solution to a problem claiming the eyesight for many babies.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Institute’s Ethics Committee before the start of the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.