
Abstract
Introduction
Neonatal mortality is the major contributor for under five mortality. WHO and UNICEF have mentioned that it is vital to initiate breastfeeding within the first hour of birth for reducing mortality. In India, it has been reported that only 42.7% babies receive breastfeeding within 1 hour of birth, and at our institute, we noticed only 61% of stable babies delivered vaginally received breastfeeding within 1 hour of birth. So, we planned a quality improvement study at our hospital using POCQI (point of care quality improvement).
Aims and Objectives
To increase the early initiation of breastfeeding (EIBF) practice in neonates born through vaginal delivery at or above 36 weeks of gestation from the observed baseline of 61% to >85% over 3 months period.
Methods
The study was conducted in Labor Room of a tertiary care hospital over a period of three months (Dec 2022–Feb 2023) and a sustenance phase from April 2023 to June 2023. A root-cause analysis was done using the fishbone framework focusing on various barriers related to mothers, hospital staff, policy, place, and practices. Based on this, a comprehensive early breastfeeding initiation intervention was planned utilizing Plan-Do-Study-Act (PDSA) cycles.
Results
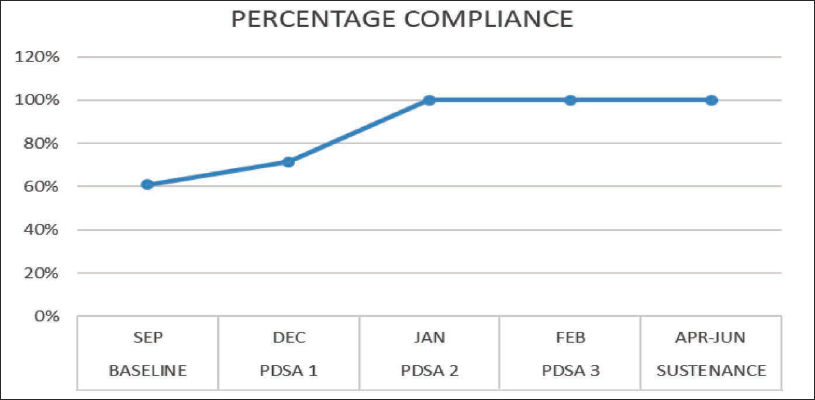
At the end of the 3 months, we were able to achieve 100% compliance in EIBF from baseline of 61% and same compliance was maintained during sustenance phase. Run charts used for interpretation showed increase in compliance and reduction in time of initiation of breastfeeding.
Conclusion
This study brought out various hurdles to EIBF and demonstrated that it can be improved by using simple quality improvement model.
Abbreviations
EIBF: Early initiation of breastfeeding
SSC: Skin-to-skin contact
POCQI: Point of care quality improvement
PDSA: Plan-do-study-act
SOP: Standard operating procedure
NRP: Neonatal Resuscitation Program
Introduction
It is noted that every year one million infants die and nearly same number have disabilities of some kind because of inadequate breastfeeding. 1 Under-five deaths are mainly contributed by neonatal deaths. 2 WHO and UNICEF have mentioned that it is vital to initiate breastfeeding within the first hour of birth for reducing mortality in infants and under-five children. 3
As per systemic review and meta-analysis done by Smith et al, linear relation is found between risk of neonatal mortality and time of initiation of breastfeeding; those babies in whom breastfeeding was started at 2–23 h of life were found to have nearly 33% more risk of mortality and those babies who were fed >24 h after birth had 2.19-fold increase in mortality in comparison with those in whom the feeding was initiated within 1 h. 4
This reduction in mortality may be because of immunoprotective agents present in colostrum or avoidance of prelacteal feeds, which may act as potential pathogen carrying vehicles. 5 Early initiation of breastfeeding (EIBF) also helps in the prevention of hypothermia 6 and gastroenteritis during infancy. 7 It also exposes the infant to microbiome of maternal skin which in turn helps in colonization of baby’s skin and gut with beneficial flora, which protects the baby against harmful pathogens found in surrounding environment. 8 Early breastfeeding also helps in the stabilization of breathing and heart rate. 9 It is also beneficial to the mother as early suckling stimulus induces oxytocin secretion, which reduces the risk of postpartum hemorrhage. 10
Despite these benefits, majority of newborns do not receive breastfeeding within 1 hour of birth. The current global data reveals that 17.7%−57.6% prevalence of EIBF among various countries and only 50% prevalence is found among developing countries. 11 In India, it has been reported that only 42.7% babies receive breastfeeding within 1 h of birth as per the fifth National Family Health Survey (NFHS-5). 12
EIBF has reduced deaths by 22% in Ghana 13 and by 19% in Nepal. 14 Therefore, initiating breastfeeding within 1 hour of delivery is need of an hour.
Various barriers for early initiation have been mentioned in different studies such as maternal lassitude and uncomfortable breastfeeding position due to post-delivery pain, 15 late transfer of mother from delivery room to the observation area, and high delivery load. 16
At our institute, we noticed only 61% of stable babies delivered vaginally received breastfeeding within 1 hour of birth. Our hospital being tertiary care Centre more than 1000 deliveries occur annually and most of them included high risk mothers with some complications. Thus, staff involved were more focused on managing emergencies and monitoring mothers, which made it challenging to focus on EIBF.
To bring out an improvement, one must have a knowledge of local factors, brain-storm ideas from stakeholders, and systematically expand these ideas with proper monitoring. 17 With this idea, we planned this study to improve the status of EIBF among newborns delivered vaginally at our hospital using POCQI (point of care quality improvement) model of root-cause analysis and the Plan-Do-Study-Act (PDSA) cycle, which include systematic method of identifying barriers and then addressing those barriers one by one in a stepwise manner.
Aims and Objectives
To increase the EIBF (within 1 hour of birth) practice in neonates born through vaginal delivery at or above 36 weeks of gestation, and who cried immediately after birth and did not have respiratory distress, from the observed baseline of 61% to >85% over 3 months period by quality improvement method.
Methods
The study was conducted in Labor Room of a tertiary care hospital over a period of three months (Dec 2022–Feb 2023) and a sustenance phase from April 2023 to June 2023. We had included all newborns ≥36 weeks born through vaginal delivery in our hospital during this study period who cried immediately after birth and did not have respiratory distress. We excluded those newborns with major congenital anomalies or gastrointestinal malformations, those delivered through LSCS, those who were hemodynamically unstable and requiring NICU admission, those whose mothers were unstable or unable to feed, and those for whom breastfeeding was contraindicated due to any cause.
The Institute Ethics Committee (IEC) approved the study and granted a waiver of individual consent. The baseline assessment was carried out during the month of September 2022 and data was collected from medical notes and entered in a predesigned excel form for 4 weeks with the help of resident doctors attending delivery at labor room. Key personals involved in maternal and child care in the first hour, such as mothers, family members, and hospital staff (obstetricians, neonatologists, pediatricians, and nurses) as well as delivery place were identified and their knowledge and the entire process were observed for various causes contributing to delayed initiation of breastfeeding.
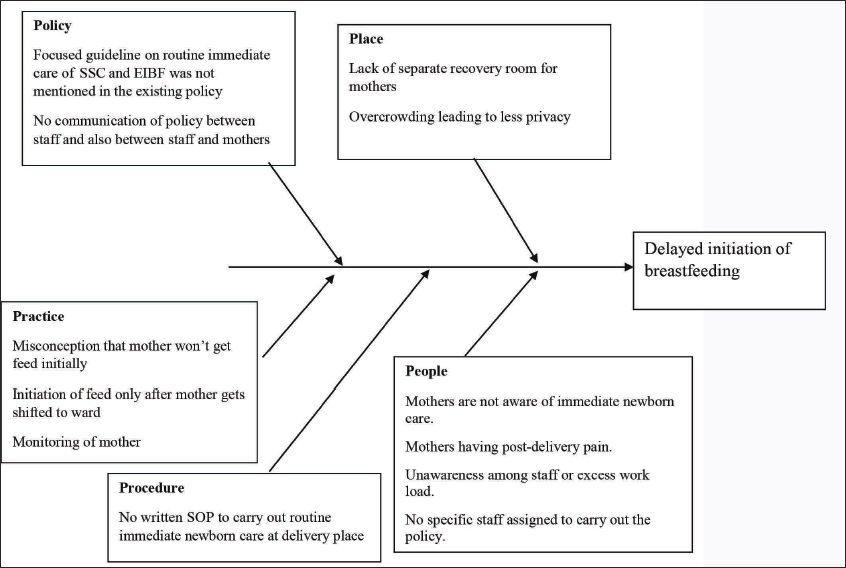
A root-cause analysis was done using the fishbone framework focusing on various barriers related to mothers, hospital staff, policy, place, and practices (Figure 1). Based on this, a comprehensive early breastfeeding initiation intervention was planned utilizing PDSA cycles. A combined meeting of the study team involving in charge staff, staff nurses, and doctors from neonatology, pediatrics, and obstetrics was conducted in the implementation phase. After discussion with study team, it was noted that lack of awareness among the hospital staff was one of the important reasons and also no written care plan was available at delivery place; written policy on routine immediate care was not focused on EIBF and breastfeeding policy of our hospital did not mention the exact timeframe within which the breastfeeding should be initiated.
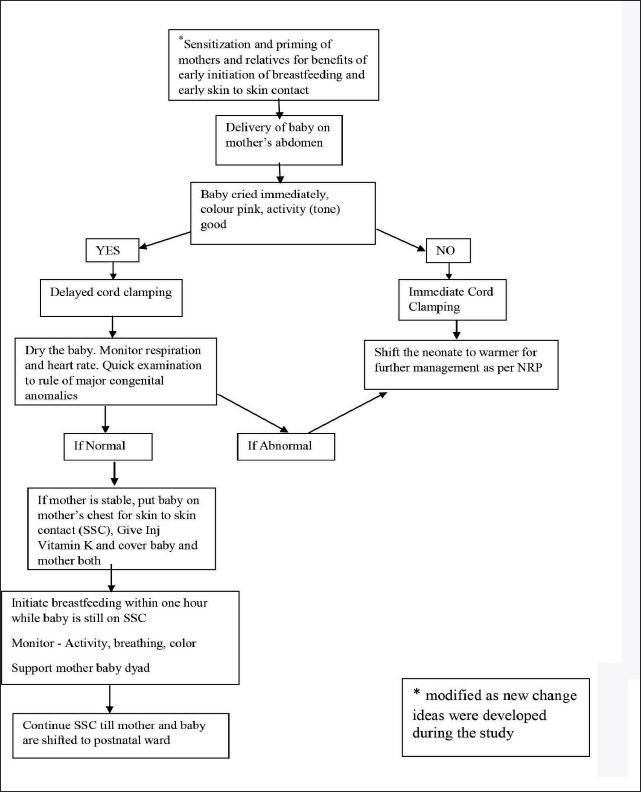
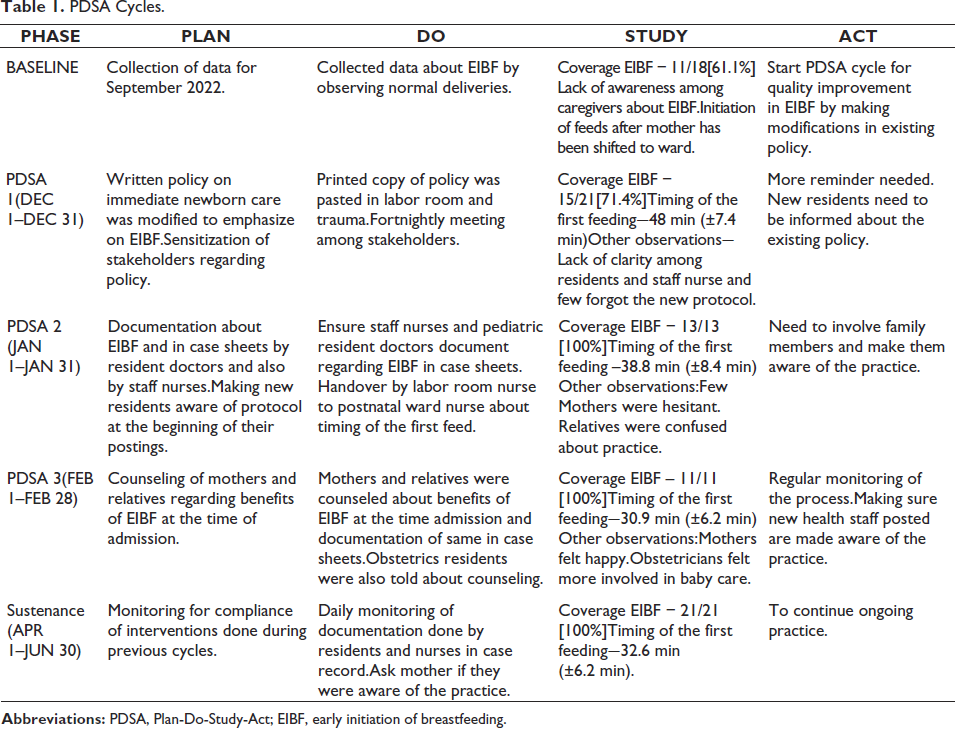
With this information, we started our first PDSA cycle; a process map was prepared indicating all steps preceding the initiation of early breastfeeding and breastfeeding policy were modified and a simplified flowchart was made. Same was discussed with obstetricians, staff nurses of delivery room, residents, and staff of pediatrics and neonatology. After acquiring ideas from team members, flow diagram (Figure 2) was prepared and was pasted at delivery places (delivery room and trauma). All stakeholders involved in normal delivery were made aware of this and monitored for compliance of EIBF. The flow diagram was modified as new change ideas were developed during the study. Various hurdles were identified during each phase and next PDSA cycle was planned accordingly. Details of each PDSA cycle are given in Table 1.
PDSA Cycles.
Descriptive statistics were used to describe variables; continuous variables were presented as mean (SD) and median (interquartile range) and categorical variables were presented as proportions. Run charts were used to display and interpret the serial measurement of indicators and to study the impact of changes.
Results
Baseline data collected over the month of September 2022 showed that out of the 18 eligible newborns, 11 (61%) received breastfeeding within 1 hour.
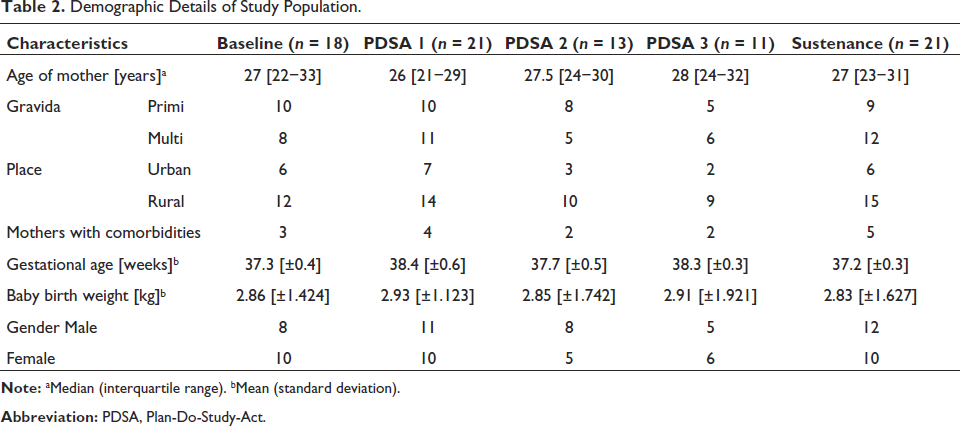
The baseline demographics of study population during baseline phase and post-intervention phase are described in Table 2.
Demographic Details of Study Population.
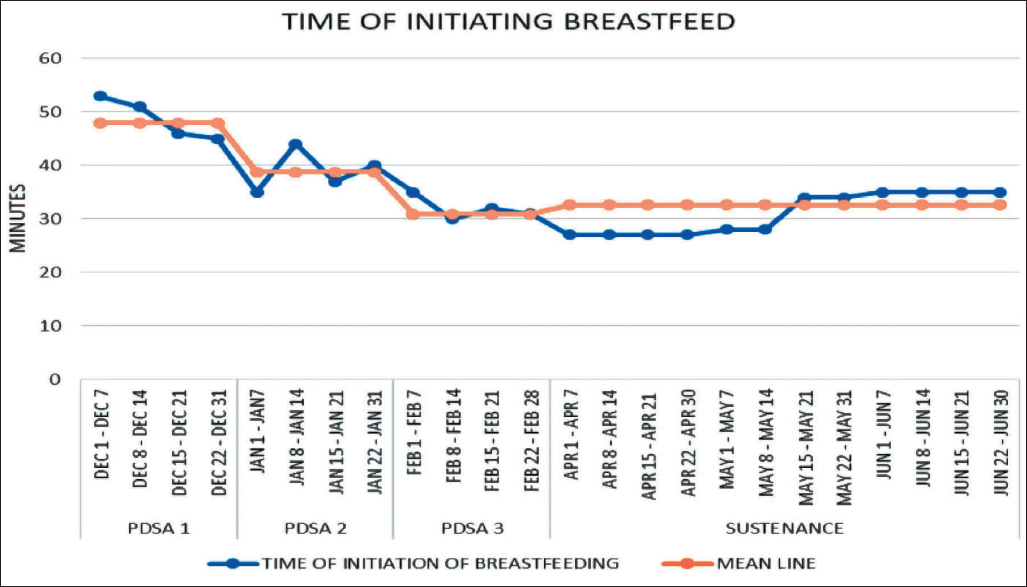
At the end of the 3 months, we were able to achieve 100% compliance in EIBF. PDSA 1 included 21 eligible newborns and 15 of them received EIBF with percentage compliance of 71.4%. PDSA 2 and PDSA 3 included 13 and 11 eligible newborns, respectively, and all of them were breastfed within 1 hour, improving compliance to 100%. The time of initiation of the first feeding was noted during each PDSA cycle, average time of 48 min (±7.4 min) was noted during PDSA 1, and the duration reduced with subsequent cycles with average time of 38.8 min (±8.4 min) in PDSA 2 and 30.9 min (±6.2 min) during PDSA 3, respectively.
After the gap of one month, sustenance phase was started, where eligible newborns were monitored for EIBF practice for the duration of 3 months. During this phase, 21 babies received EIBF out of 21 eligible newborns, maintaining 100% compliance.
Run charts used to display and interpret the serial measurement of indicators and to study the impact of changes showed increase in compliance and reduction in time of initiation of breastfeeding (Figures 3 and 4).
Discussion
Through this quality improvement study, we were able to improve EIBF at a tertiary care institute using standard root cause analysis and PDSA cycle model. We achieved the target compliance without any additional resources. Initially, there was hesitancy among healthcare staff to follow the new idea as with any change in practice, but gradually everyone adapted to it well.
This quality improvement model enabled us to observe and extract information from obstetricians, nursing staff, patients, helping staff, thus involving multiple personals and delivering the overall care rather than focusing on single point of view. This way everybody felt empowered to be part of a team and enabled to integrate the change within the existing practice resulting in sustainability of the change.
Breastfeeding is known to offer multiple benefits for both mother and newborn. For establishing successful breastfeeding, skin to skin contact (SSC) soon after birth, limiting maternal-infant separation, and frequent on demand feeds are important and EIBF forms the key pillar. 18
Similar quality improvement model was used by frontline delivery team in one of the medical colleges of New Delhi to improve early SSC and EIBF. Some successful change ideas tested were pre-delivery counseling, avoiding separation of mother and newborn at birth by providing SSC, and continuing it in the post-delivery observation area and getting family member’s help with the first breastfeed. This resulted in the improvement of EIBF to 61% over a 36-month period. 16 In contrast to our study, this study was conducted over a period of 36 months, and also, the improvement noted was less; reasons may be being a government institute delivery rates were high and had more workload on staff involved.
Another study was conducted in one of the government hospitals of central India, Gajra Raja Medical College, Gwalior, Madhya Pradesh. The rate of the first hour initiation of breastfeeding increased from 21% to 36.7% over the study period of 30 days. The lesser impact of study on compliance may be due to the following reasons: time given was less and needed more time for PDSA cycles, needed more training of team members, and lack of communication among team members as mentioned by authors themselves. 19
Counseling of parents and family members also plays a vital role in maintaining the practice as noticed in our study. During the second PDSA cycle, it was noticed that few mothers were hesitant to hold babies in SSC contact and also relatives were confused regarding placing baby on mother’s chest and initiating breastfeeding while baby is still on SSC. Thus, we included counseling at the time of admission as a part of next PDSA cycle and noticed better response from mothers and supportive attitude from relatives. This was similar to observation made by a retrospective study conducted at Bangalore, India, where mothers who received antenatal counseling regarding EIBF during the third trimester had better compliance with EIBF than national standards. 1
Limitations
The normal deliveries were less, still this study can be relevant to other health facilities and can be easily tested as it did not require additional resources. We had not included caesarian deliveries, which may offer more difficulty in implementing changes, nevertheless some of the measures taken here can be applied in caesarian deliveries too. We did not include stable preterm babies, which would have posed a unique challenge in process implementation.
Lessons learnt: The findings from this study urge the healthcare staff, who often tend to think that EIBF happens by default in vaginal deliveries as it is less time consuming compared to caesarian deliveries, to focus on vaginal deliveries too. Through this study, we came to know that lack of knowledge among the healthcare staff and effective communication of the knowledge among them were the main hurdles.
Conclusion
This study brought out various hurdles to EIBF. The vital areas of improvement were related to gaps in knowledge of caregivers, individual ideas about the practice, and immediate postpartum care. This study has demonstrated that EIBF can be improved by using simple quality improvement model. This quality improvement study did not require additional resources and had simple methods, and hence, it may be used for other resource limited setup.
Footnotes
Authors’ Contributions
Dr. RP and Dr AH conceptualized the study. Dr AH conducted the study. Dr. RP supervised the work and finalized the manuscript. Dr. DP and Dr. SMN modified the manuscript. Dr AH collected the data and Dr. SP recorded all the details.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The institute ethics committee (IEC) approved the study and granted a waiver of individual informed consent.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.