
Abstract
Bardet-Biedl syndrome is an autosomal recessive ciliopathy characterized by a combination of physical findings, neurodevelopmental and behavioral components, including speech delay, learning difficulties, and autistic traits. Behavioral and neurodevelopmental symptoms are often overlooked, with either under-recognition of an autism-like phenotype or overdiagnosis of Autism Spectrum Disorder (ASD). A 10-year-old girl presented with speech delay, polydactyly, night blindness, truncal obesity, type 2 diabetes, seizure episode, borderline intelligence, and learning difficulties. She was diagnosed with bardet Biedl Syndrome (BBS) using the established major and minor criteria by Forsythe et al. She was specifically referred for poor social interaction and, in school, irritability and poor communication with peers. She was earlier diagnosed with ASD elsewhere. On further evaluation, she had selective mutism, stereotypical behaviors, such as arranging her books, and lacked pretend play. The Indian Scale for Assessment of Autism (ISAA) yielded a score of 71, consistent with mild ASD. Even though she had a score of mild ASD on ISAA, clinically, she did not fit into the ASD criteria according to the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM 5) guidelines. She had autistic traits: Selective mutism and stereotypical behavior restricted to bookshelf arrangement. This case highlights overdiagnosis of ASD in the presence of autistic traits, whereas she appears to have a distinct behavioral phenotype associated with BBS, not fulfilling DSM 5 criteria for ASD.
Keywords
Introduction
Bardet-Biedl syndrome is an autosomal recessive ciliopathy that occurs in one in 140,000–160,000 children 1 with high prevalence seen in areas with consanguinity, and can have both physical, neurodevelopmental, and behavioral components. The second part is often missed, with either not identifying the autism-like phenotype or diagnosing it as Autism Spectrum Disorder (ASD). ASD is characterized by the presence of persistent social communication and interaction deficits, along with restrictive and repetitive behavior, interests, and activities, according to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM 5). 2 It has been seen that 77% of bardet Biedl Syndrome (BBS) children exhibit autism-related signs, and not full ASD. They can also have obsessive-compulsive behavior, anxiety, labile behavior, and hyperactivity. 3 In this case, the patient did not meet the criteria of ASD; instead had some autistic like traits along with selective mutism and anxiety symptoms. Hence, a thorough and keen eye on such symptomatology can assist in avoiding overdiagnosis, and a multidisciplinary approach suitable to the needs of patients.
Case Details
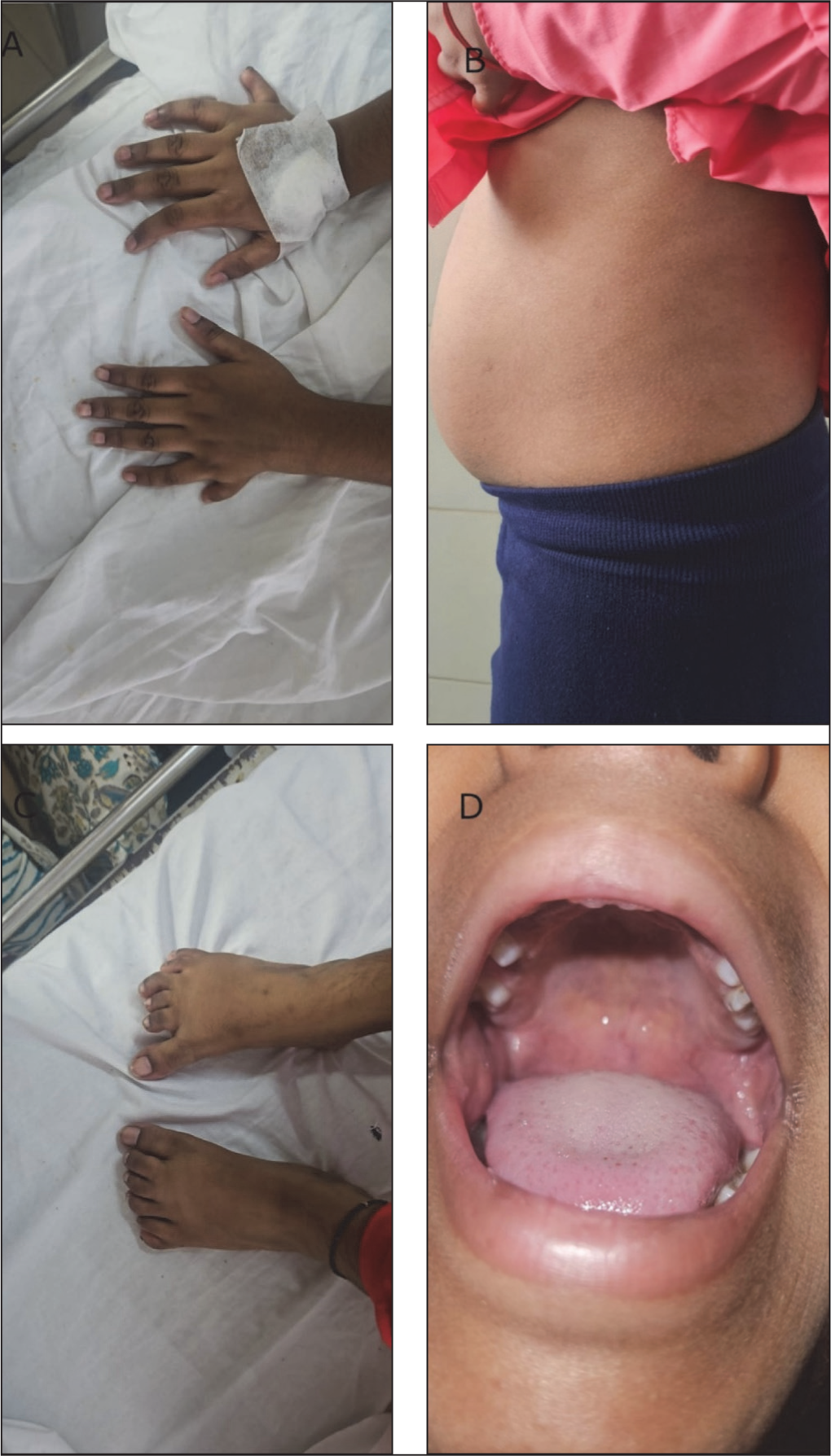
A 10-year-old girl was specifically referred to the child psychiatry unit of a tertiary hospital for poor social interaction, irritability, and poor communication with peers. She was diagnosed elsewhere with ASD and advised intervention for it. She was born out of a consanguineous marriage (second-degree), with a known case of type 2 diabetes for eight years on treatment. The patient also had a history of speech delay, night blindness, high arched palate, polydactyly, truncal obesity (Figure 1A-D), type 2 diabetes, and seizure episodes. On further evaluation, she exhibited selective mutism and repetitive behaviors, such as arranging her books, and lacked pretend play, learning difficulties, irritability, and poor communication with peers as a result of social anxiety.
Clinical signs of BBS.
On psychiatric evaluation, the Indian Scale for Assessment of Autism (ISAA) yielded a score of 71, suggestive of mild autism spectrum disorder. A diagnosis of Bardet-Biedl syndrome was made using established major and minor criteria by Forsythe et al. 1 The major criteria out of (a) retinal dystrophy; (b) postaxial polydactyly; (c) obesity (typically truncal, onset before age five); (d) learning disabilities/developmental delay; (e) hypogonadism; (f) renal anomalies those which were met are postaxial polydactyly, truncal obesity, and learning disability. The minor criteria out of (a) speech delay; (b) brachydactyly or syndactyly; (c) dental anomalies; (d) anosmia/hyposmia; (e) diabetes mellitus; (f) congenital heart disease; (g) ataxia/coordination deficits; (h) behavioral abnormalities (e.g., autistic traits, mood disorders); (i) hepatic fibrosis those which met were speech delay and type 2 diabetes, fulfilling the three major, and two minor criteria. Genetic testing could not be completed due to the financial constraints of the family. The IQ on Mallin’s Intelligence Scale for Indian Children was 75.78 (VS IQ: 84.16; performance IQ:67.4), suggestive of borderline intelligence. The patient also had learning difficulties in language and arithmetic. Detailed assessment and behavioral observation revealed that the patient had avoidant eye contact and selective mutism, but only was found to be toward specific adults, such as teachers, and new people. As the child would start to know, the adult would start smiling and interacting better, hence going against the ASD feature. However, she would interact well with her sibling and parents using both verbal and non-verbal communication. Hence, the deficits in communication and socialization resulted from social anxiety and not core deficits of ASD. Hence, a clinical diagnosis of Bardet-Biedl syndrome along with a distinct autism-like phenotype was made. Psychoeducation of family members was done. Behavioral therapy was advised along with 12.5 mg sertraline, later increased to 25 mg once a day. The patient, after starting on tablet sertraline, showed improvement in her anxiety symptoms within one month of the follow-up period.
Discussion
This case report emphasizes the need to see syndromic conditions for comorbid psychiatric issues with care so that overdiagnosis is avoided. It also points out the difficulty in diagnosing such cases clinically in resource-limited settings, and affordability for genetic testing is a concern. The presence of social anxiety and selective mutism, and the lack of restrictive repetitive behavior, which is typically seen in ASD, such as motor movements, need for sameness, and sensory issues, were not present; a distinct type of autism-like phenotype is reported. However, the presence of selective mutism, social anxiety, developmental delay, and lack of typical repetitive behaviors seen in ASD may suggest a distinct behavioral phenotype in BBS, which looks like autism but does not meet the full criteria for ASD. There are reports of symptoms of autism in BBS, such as Kerr et al. 4 found that 77% of the children diagnosed genetically with BBS were found to have symptoms associated with autism, and recommended that the frequency of autism-related symptoms far exceeded the incidence rate of diagnosed autism in general, and hence it warrants further investigations and screening for children with BBS for ASD. On the other hand, Chatterjee et al. 5 reported a case of autism using Childhood Autism Rating Scale (CARS) and ISAA in an eight-year-old boy diagnosed with BBS in eastern India. Another case report by Güleç et al. 2025, 6 reported a four-year-old boy with BBS and autism spectrum disorder. In this case, it was genetically diagnosed with BBS 10, and the patient met the criteria for ASD. However, a study by Rödig et al. 7 on two rodent models with BBS, Bbs6/Mkks, and Bbs8/Ttc8 knockout mice mutation found deficits in social and anxiety traits, and that it might be based on an altered architecture of the hypothalamus. However, in our case, we could not fully conclude on autism spectrum disorder as the criteria were not being fully fulfilled. According to DSM 5, Criterion B of the presence of at least two types of restrictive repetitive behavior currently or by history was not found, which is one of the necessary points to be present for ASD diagnosis. However, a distinct behavioral phenotype consisting of social anxiety, selective mutism, repetitive behaviors, and poor social interaction, as reported in previous studies, may warrant a distinct diagnosis. Even though the patient had mild ASD according to the ISAA scale in our case, she did not meet the full criteria of ASD according to DSM 5, hence highlighting the gap, and the risk of overdiagnosis of ASD should be kept in mind. The symptoms were not better explained by social communication disorder and mostly fit into an autism-like phenotype. It tells us that there is a relation between ciliopathies and neurodevelopmental disorders, and hence strengthens the need for searching for meaningful behavioral phenotypes in such syndromes, avoiding misdiagnosis.
Conclusion
The above case report gives the message that behavioral features in syndromic conditions are frequently missed; early identification is crucial for prompt psychiatric assessment and integrated care, and to avoid diagnostic overshadowing and masking.
Footnotes
Acknowledgements
Nil.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed consent for publication was obtained from the patient’s mother/legal guardian, as the patient was a minor, and institutional ethical guidelines were followed.