
Abstract
Introduction:
Young people are inherently susceptible to mental health issues, particularly during their adolescent years. Though suicide is more prevalent among older adults compared to younger individuals, it remains one of the leading causes of death in late childhood and adolescence worldwide. It has become important to understand suicidal ideation and behavior in adolescents to identify the risk factors, including depression, and further facilitate its prevention. The present study aims to explore suicidal ideation and behavior and the presence of depression in adolescents. It also aims to see if younger adolescents differ from older adolescents in terms of suicidal ideation and behavior and depressive symptoms.
Material and Methods:
A total of 200 individuals of both genders aged 10–17 years were included in the study. A sample was selected from the clinics and different community areas of Kolkata. Suicidal Behaviors Questionnaire-R and Child Depression Inventory were administered to assess the presence of suicidal behavior and depression, respectively.
Results:
Suicidal behavior was evident in 35.5% of the participants, with younger adolescents being more in proportion. Depressive symptoms were present in 29% of the total sample, with older adolescents being more in proportion.
Discussion:
The findings implicate a significant number of adolescents at risk for suicidal behaviors, warranting attention for early identification and subsequent psychosocial intervention.
Introduction
India has the largest adolescent population in the world at 253 million, and every fifth person is in the age range of 10–19 years. 1 Ensuring these adolescents are safe, healthy, educated, and equipped with information and life skills is crucial for India’s social and economic progress. 2 Adolescence is also a high-risk period for psychological disturbances. Suicide is a global health issue that affects all age groups, but it is most concerning in adolescents, where it ranks as the third greatest cause of death. 3 Although evidence of the influence of under-treatment on suicide risk is limited due to the low base rate of suicide in the community and a lack of adequate data sources.
Suicidal thoughts, while not necessarily leading to suicidal behavior, are major risk factors. Before ideas become actions, a number of circumstances come into play, including underlying mental health conditions and stressful situations like the death of a loved one or academic failure. While these episodes are typical among youngsters, they rarely lead to suicidal behavior unless there are other underlying concerns. The high risk of suicide attempts in depressed adolescents shows the significance of determining the other associated risk factors in this population, which include emotions of hopelessness and alcohol or substance use disorders, which impair judgment, as two common underlying concerns. 4 Poor impulse control, which is common among teenagers with disruptive behavioral problems, is also a risk for suicidal behavior. It is also suggested as one of the important risk factors of suicide attempt among adolescents. 5 Other mental and physical illnesses, such as anxiety, also increase the risk. Rage directed at family or friends, combined with communication challenges, can intensify suicidal impulses when people redirect their wrath inside. Imitation also plays a role, as high-profile suicides can inspire learned behavior, particularly in school-going adolescents. Familial variables also play a role, as suicide rates are found to be higher in families with a history of mood problems or violent behavior. 6 Understanding these multiple risk factors is critical for developing effective prevention methods and offering early interventions to help children and adolescents avoid the consequences of suicidal behavior.
The presence of depression is considered a significant deterrent having a harmful impact on the youth population. Affective disorders such as Major Depressive Disorder (MDD), Recurrent Depression are found to be closely linked to suicide in adults,7,8 and there is also an increased risk of suicidal ideation, attempts, and completion in children and adolescents too. 9 While research on suicidal behavior exists for specific populations like college students10,11 and the elderly, 12 there is a significant dearth of studies exploring suicidal ideation, depression, and their co-occurring conditions in children and adolescents. Attention should be given especially to teenage suicide as it has been increasingly common in recent years, posing a serious public health risk that jeopardizes teenagers’ physical and psychological well-being, as well as their survival. 13 Recently, the COVID-19 epidemic contributed to a rise in suicides among children and adolescents. 14 Hospitalizations for suspected suicide attempts increased by 22% for all teenagers in the summer of 2020 compared to the same period a year earlier and by 39% in the winter of 2021. 15
Various comprehensive studies and research are conducted with respect to suicidal ideation and behaviors, but works related to the suicidal intent and behavior in the adolescent population are still not sufficient. One of the difficulties in predicting and preventing suicidal behavior has been the long-standing reliance on patients’ self-reports of suicidal thoughts and intentions. Some people may be compelled to hide or downplay suicidal thoughts for fear of being stigmatized or hospitalized.
Thus, the present study aims to explore the presence and pattern of depression and suicidal ideation and behavior in young and late adolescents.
Methods and Materials
Study Design
This is a cross-sectional, exploratory study conducted from April to December 2023 to explore suicidal behavior, ideation and depression in young and late adolescents in urban areas of Kolkata. A sample was selected from the mental health clinics and different community areas of Kolkata.
Participants
The sample size was determined considering the sensitivity of the domain (identification of suicidal behavior), the time frame available for data collection, and the need for a sufficiently large sample. The initial sample size was estimated on the basis of the prevalence of adolescents within the age range of 10–17 years and was divided into two groups: young and late adolescents. The final sample comprised 200 adolescents, with 100 in each study group (10–13 years in the young adolescents; and 14–17 years in late adolescents). The purposive sampling method was used. Consent was taken from the parents of the participants from all groups. The study was accorded Ethical Committee Approval vide Ethics Committee No. DRC-AIPSK/ETHICS/March/2023/1 dated 05.03.2023. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. Participants recognized with clinically significant depressive symptoms or suicidal ideation were referred to mental health professionals for further assessment and support. Appropriate psychoeducation was provided to caregivers, and urgent medical attention was recommended wherever necessary.
Measures
Socio-demographic Datasheet and consent form were given to all the participants to collect demographic information regarding their age, sex, educational level and socio-economic status. A consent form was also provided to all the participants, including their parents.
The Suicidal Behavior Questionnaire -Revised (SBQ-R) 16 is a self-report tool used to evaluate suicidal behavior and ideation. It comprises four questions about previous suicide ideation and attempts, as well as the chance of future suicidal behavior. Responses are rated on a Likert scale, with higher scores suggesting a higher risk of suicide behavior.
Although the standard age range for SBQ-R is 13–18 years, its use in this study was extended to 10–12 years because the objective was not a single-case assessment but rather the identification of suicide risk within the child and adolescent population. Evidence suggests that suicidal behaviors can emerge as early as 8 years, highlighting the importance of early assessment. Previous studies have also supported the applicability of SBQ-R in younger populations, with reports indicating that it can be administered from as early as 7 years of age to identify suicidal behavior and initiate precautionary measures. 17
Child Depression Inventory 2 (CDI 2) 18 is a commonly used self-report questionnaire for evaluating depression symptoms in children and adolescents. It contains 27 items that evaluate different elements of depression, such as mood disturbance, interpersonal interactions, and self-esteem. Participants score each item on a scale of 0–2 based on how they have felt over the previous two weeks.
Procedure
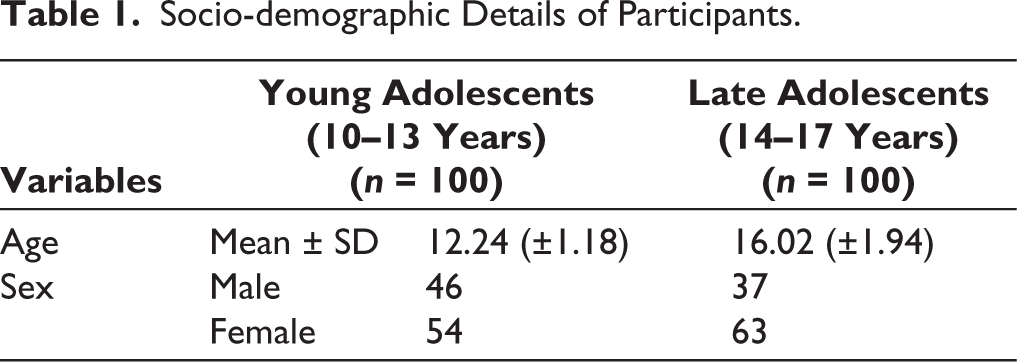
Data were collected by registered clinical psychologists, and the interview was conducted in English. Scores from the SBQ and CDI were analyzed using SPSS 26. Descriptive statistics were used to summarize individuals’ demographic characteristics as well as the prevalence of suicidal behavior and depressed symptoms. Students’ t-test was administered to find out the group-wise comparison in suicidal behavior and depression among the groups. Sociodemographic details of the participants is summed up in Table 1.
Results
Socio-demographic Details of Participants.
Discussion
The present study aimed to explore the suicidal risk behavior and depression in young and late adolescents. The age range of the total sample was 10–17 years, considered as adolescents group, all are school-going and residing in urban areas of Kolkata and were divided into two subgroups, young and late adolescents. Very recent meta reviews have highlighted the increasing concerns regarding adolescents’ mental health in trends. 19 The results suggest that from the total pool of adolescents, young and late combined, more than 35% adolescents scored above cut-off on the Suicidal Behavior Questionnaire, while 29% of the sample scored above cut-off on the depression rating (Table 2). While this is a concerning finding, it was equally concerning to note that the young adolescents in the age range of 10–13 years were more in number (42%) compared to late adolescents (14–17 years) of whom 29% scored above the cut-off on the suicidal behavior questionnaire. While adolescence phase is known to be marred with mental health risks, this comes as an unwanted finding to have young adolescents as early as 10–13 years having suicidal behavior and ideation.
The Center for Disease Control and Prevention’s most current national death figures show a suicide rate of 0.17 per 100,000 youngsters aged 5–11 years, compared to 5.18 per 100,000 teenagers aged 12–17. 20 Early adolescence is time of major change in which adolescents experience the physical changes associated with puberty and confront new problems 21 when they enter middle school, where they face higher peer and academic expectations.
Table 2 shows that, while depression is a known risk factor for suicide and suicidal behavior, interestingly, depression rating was higher in the late adolescents (38%) compared to young adolescents (20%). The findings, while of concern, considering the high percentage of adolescents reporting depressive features, also indicate other variables also which contribute to suicide behavior in adolescents. 22
Total Number of Participants Above the Cut-off Points in SBQ-R and CDI 2 from Both Groups.
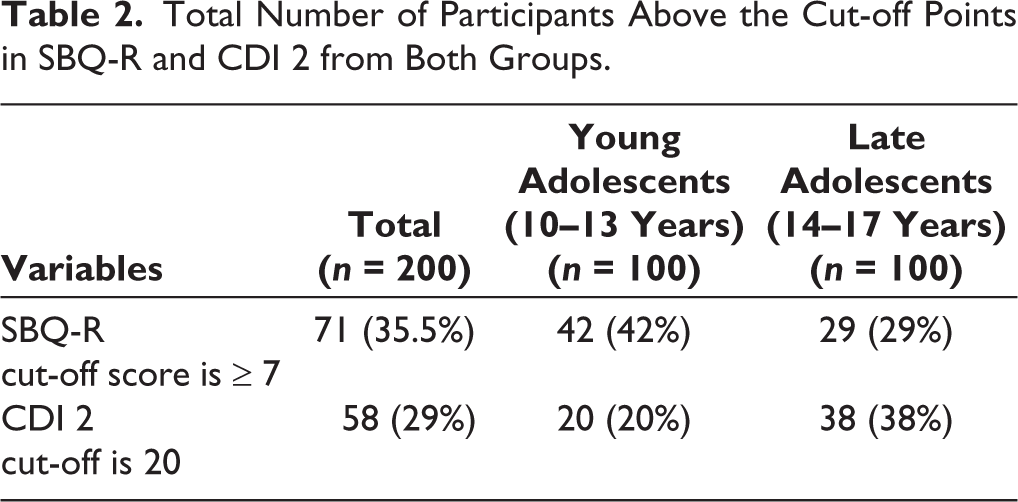
Table 3 showing the age-group-wise comparison in suicide behavior and depression indicates significant differences between the groups (t-value = 12.49; P = .0001), where young adolescents in the age range of 10–13 years reported more suicide behavior compared to late adolescents. While the explanations for this might be vivid, one of the reasons could be that the younger adolescents may have difficulties in articulation or expression, which might lead to poor coping mechanisms. 23 Studies show that young adolescents usually have hormonal changes which fine-tune their neural networks, and they help in managing and articulating emotions. 24 In early adolescence, as this mechanism is still immature, emotional articulation becomes difficult for them. Emotional articulation is one of the components of emotional regulation, whereas suicidal thoughts or death wishes have a strong association with emotional dysregulation. 25
Group-wise Comparison of Suicidal Behavior and Depression.

Further, if we look at the mean scores on the depression rating, there is a significant difference between the two groups (where late adolescents (14–17 years) had a higher score compared to young adolescents (t-value = 13.52; P = .0001). Findings suggest that older adolescents might have better capability compared to younger adolescents to express their distressing thoughts and which might be expressed as low mood, social isolation or even through anger outbursts. Internalization of emotions is not so prevalent among this group. 26
Even though suicide and depression are known to coexist among individuals of different age groups, it is not necessary for both to be equally proportionate in adolescents, as evident from the present study findings. It is important to note that suicide is considered a behavioral act, 27 whereas depressive symptoms are more associated with negative cognitions or distorted cognitions. 28 Developmental theories suggest that the cortical development may not be comprised in the early adolescence period, 29 which might lead to less cognitive processing. In early adolescence, significant physical as well as academic changes are very prominent, which can increase emotional and behavioral problems. Neuroscientific research developments suggest that these changes can be caused by hormonal changes in puberty. Suicidal behavior is one of the manifestations of emotional and behavioral challenges. 30 In this period, adolescents become vulnerable to increased moodiness with distorted interpretation and analysis of self and others, along with self-criticalness, poor decision-making, and judgment. 31 With time, adolescents gradually master or have better perspectives of stressful events around them, and they act more cognitively than behaviorally. 32
Findings of the present study give new insight regarding suicide behavior and depressive phenomenon in adolescents. The presence of depression in a significant number of the total sample supports depression as a risk for suicide behavior, it also challenges the traditional belief that suicidal behavior is mostly driven by depressive symptoms, suggesting other underlying factors also contribute to suicidal intent and behavior in adolescents. Suicidal behavior in adolescents appears to stem from a complex interplay of emotional denial and avoidance of uncomfortable feelings, and not just depressive symptoms. As we find differences in these behavior within different age groups of adolescents, they potentially imply impulsivity as a critical predictor of suicidal thoughts in adolescence, supported by the higher prevalence of impulsivity and risk-taking behaviors at this stage. 33 Suicidal behaviors can also be driven by host of clinical conditions, including anxiety disorders, 34 eating disorders, 35 substance addiction 36 and even due to chronic physical illness or pain. 37 Even when suicidal ideas are prevalent, the presentation varies between younger and older teenagers. Their difficulties with emotional communication may result in anger outbursts, self-harming behaviors, or ambiguous suicide threats 38 in younger teenagers. In contrast, older teenagers (14–17 years old) may communicate suicidal thoughts in a more planned or purposeful manner. This distinction might be attributed to variables such as cognitive development, with older adolescents having a greater sense of finality, or more access to knowledge concerning suicide techniques.
Considering the high prevalence of suicidal ideation among adolescents, early detection and suicide prevention have become important, and more importantly, because children and early adolescents are less likely to disclose suicidal thoughts on their own.
The study findings also highlight that suicidal behavior and intent may exist in people with only a few depression symptoms, which may be difficult to detect without careful evaluation. 39 Thus, screening methods for adolescent suicide behavior should be more spontaneous, concentrating on those in high-risk groups as defined and targeted, while taking into account psychological, physical, and social aspects. 40 Those with mental illnesses, past suicide attempts, or medical conditions, as well as those who are socially isolated, are at a higher risk. 41 Though numerous programs have been focused toward adolescents in high school, most programs are highly generic and aimed at raising awareness; they do not identify or intervene with individuals who are having suicidal thoughts or behavior. Tailored interventions along with family counseling for these individuals are likely to promote reduced stress, peer interaction, and support from family, resulting in a better quality of academic and social life. 42 The study has its own limitations, as it included only urban adolescents from a metro city, limiting generalization of the findings. Further, other associated psychosocial variables such as academic stress, peer pressure, and family conflict were not explored in detail and could be included to get a wider understanding of risk factors of suicide behavior in adolescents.
Implications and Future Directions
The findings challenge our conventional inclination of depressive symptoms as a major indicator of suicidal ideation and behavior, especially in adolescents, and highlight the need to explore suicidal risk in adolescents from a wider perspective appropriate to adolescents. Recognizing and addressing suicidal intent early on allows mental health practitioners and educators to undertake timely interventions to reduce the likelihood of suicide attempts and increase adolescents’ well-being.
While the present study has implications for suicidal behavior and depression among adolescents, a few considerations remain. The sample was drawn exclusively from the urban adolescent population in Kolkata, which provides valuable context-specific findings but may limit broader generalizations. Additionally, including a more detailed account of socio-economic variables in future research could further enhance the understanding of factors contributing to suicidal behavior.
To advance our current knowledge about suicidal intent and depressive symptoms among adolescents, there is a need to conduct a comparative study into the nature of suicide intent and depressive symptoms throughout infancy and adolescence, and it holds potential for improving our understanding of the complex connection between these phenomena. Understanding how suicidal cognitions develop and change through developmental stages might give information on their significance as possible antecedents to depression.
Conclusion
It is important to recognize that suicidal behavior among children and adolescents is complicated, and there is no definite profile of suicidal behavior. While there may be multiple warning signs signaling suicidal thoughts, such as a preoccupation with death, an obsession with violence, and giving up valued items, it is important to recognize that these signals are not always obvious or constant among individuals, especially adolescents, who differ in their impulsivity and emotion processing capabilities within their slightly elder peers. Adolescents considering suicide may display depressive symptoms such as withdrawal, apathy, rage, and risk-taking behaviors, complicating detection and intervention attempts. Recognizing the interconnectivity between suicide behavior and depression is critical, but it is also crucial to understand that the two may not always coexist. Therefore, it is necessary to treat both concerns independently and thoroughly and consider other warning signs, too.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Written/verbal informed consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. The study was accorded Ethical Committee Approval vide Ethics Committee No. DRC-AIPSK/ETHICS/March/2023/1 dated 05.03.2023.