
Abstract
Purpose of Review:
Attention-Deficit/Hyperactivity Disorder (ADHD) is increasingly recognised as a lifelong neurodevelopmental condition that persists into adulthood, often associated with significant functional impairment and high psychiatric comorbidity. Despite global advances, services in India remain severely underdeveloped. This paper reviews international guidelines—including those from NICE, the Canadian ADHD Resource Alliance (CADDRA), the British Association for Psychopharmacology (BAP), and the Indian Psychiatric Society (IPS)—to identify best practices for the assessment and multimodal treatment of adult ADHD.
Collection and Analysis of Data:
The paper reviews international guidelines on adult ADHD care, highlighting convergent recommendations and their applicability to the Indian context. It analyses systemic gaps in India’s service delivery, including the shortage of trained mental health professionals, low public and professional awareness, lack of culturally adapted tools and materials, and limited access to pharmacological and psychosocial interventions. As an applied example, the paper presents Amaha’s adult ADHD care model—developed in 2022—as a scalable, evidence-based approach tailored to the Indian ecosystem. The model integrates psychiatrist-led assessments using the DIVA-5 tool, structured psychoeducation, cautious pharmacotherapy, and adjunctive psychotherapy within a digitally enabled care framework prioritising, continuity of care, family engagement, and community support.
Conclusions:
This review proposes recommendations to strengthen ADHD care infrastructure in India. These include workforce training, public awareness initiatives, development of India-centric resources, telepsychiatry reforms, and integration of ADHD into public policy and insurance schemes. Addressing adult ADHD in India is both a clinical and public health imperative, requiring scalable, multidisciplinary, and context-sensitive solutions.
Introduction
Attention-deficit/hyperactivity disorder (ADHD), once considered mainly a childhood disorder, is now recognized as a neurodevelopmental condition that can continue into adulthood, often with symptoms that are persistent and disabling. 1 It is also well established that ADHD, like many other mental health conditions, frequently coexists with disorders such as depression, anxiety, other neurodevelopmental issues, bipolar disorder, and substance use disorders. In adulthood, 65%–89% of all patients with ADHD suffer from at least one additional psychiatric disorder. 2
The growing influence of social media and public figures speaking openly about their mental health has led many adults to explore psychological explanations for difficulties they face in daily life. Adult ADHD, in particular, has gained widespread attention online. However, in India, many adult psychiatrists have limited training in identifying and managing ADHD. Despite this, there is a growing demand, especially among younger adults in urban areas, for proper assessment and treatment, often driven by exposure to ADHD-related content on social media and the internet. Many mental health professionals, as a result, express concern about the potential overdiagnosis of adult ADHD and often view its rising visibility as a passing trend or a social media-driven phenomenon. However, underdiagnosis remains a significantly greater concern than overdiagnosis, both globally 3 and more acutely within the Indian subcontinent. 4
In most Indian psychiatric clinics, consultation times are often limited to less than 15 minutes due to high patient volumes. However, best practices for diagnosing and managing adult ADHD, as recommended by organizations such as the Canadian ADHD Resource Alliance (CADDRA), the American Academy of Child and Adolescent Psychiatry (AACAP), the British Association for Psychopharmacology (BAP), and the Indian Psychiatric Society (IPS), include a detailed developmental and birth history, collateral information from family, academic records, and the use of standardized assessment tools. A comprehensive mental health evaluation is also essential to rule out other possible diagnoses and to identify coexisting mental health conditions, which are common in adults with ADHD.
A Brief Review of Global Guidelines for the Management of ADHD
This section provides a brief review of national and international guidelines for the management of ADHD. The following guidelines have been consulted for this review: The IPS Guideline, 5 the National Institute for Health and Care Excellence (NICE) guidelines, 6 the British Association of Psychopharmacology Guideline, 7 the European Consensus Statement, 8 CADDRA guidelines, 9 the RCPsych College Report, 10 Guidelines from the American Academy of Family Physicians (AAFP), 11 and recommendations from centre for disease control and prevention (CDC) 12 (Table 1).
Comparative Table of Guidelines for Management of Adult ADHD.
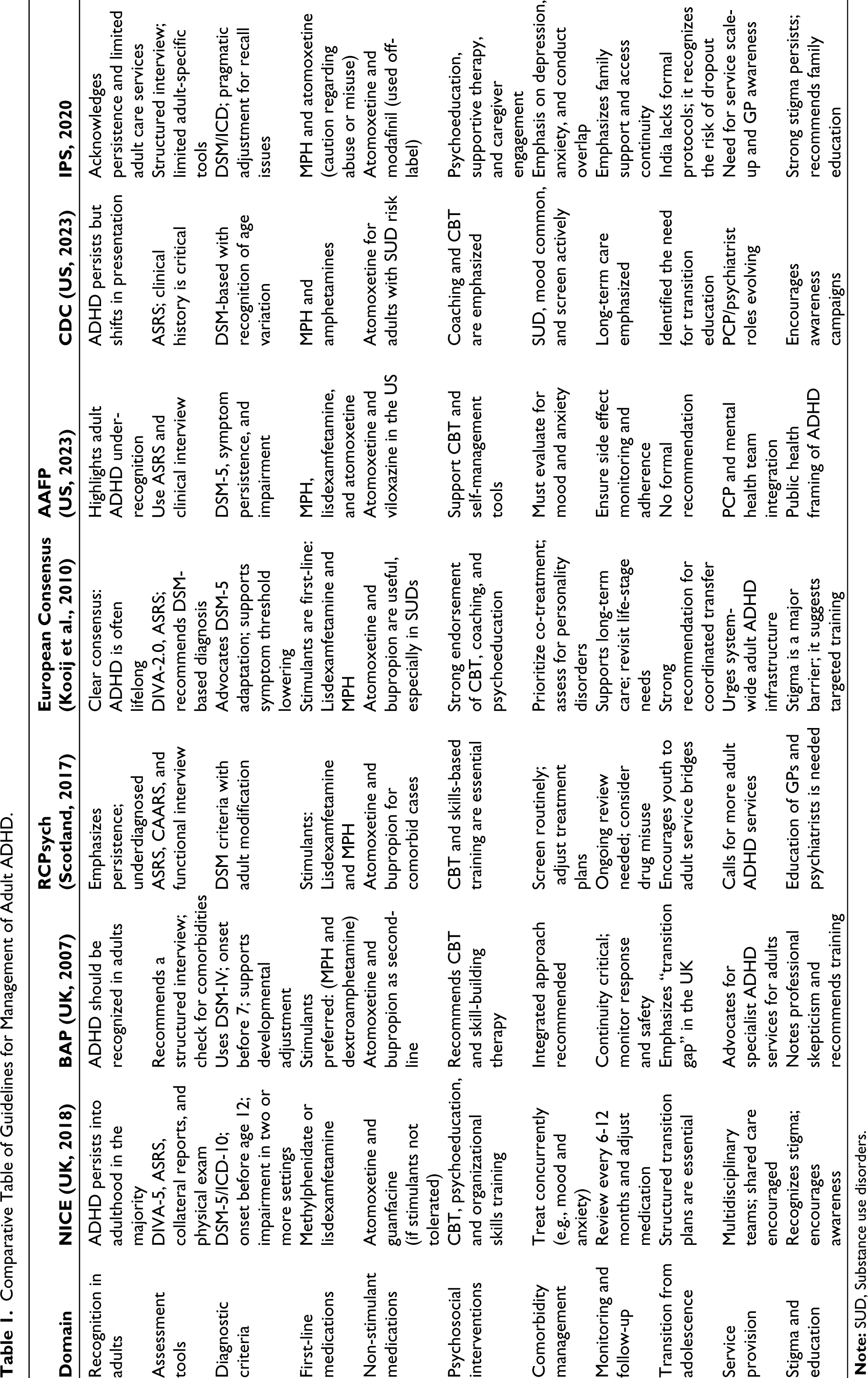
All reviewed guidelines consistently emphasize the need for a comprehensive assessment for the diagnosis of adult ADHD. This begins with pre-assessment and adult-specific screening tools such as the adult ADHD self report scale (ASRS), followed by a full, comprehensive psychiatric assessment. The assessment should include screening for comorbid conditions such as anxiety, depression, personality disorder, other neurodevelopmental disorders, and substance use. Relevant history about physical health conditions should be included. Collateral information from parents, partners, or other relevant (and/or appropriate) informants is considered highly valuable to confirm the diagnosis. The use of structured diagnostic tools, such as the Diagnostic Interview for ADHD in Adults (DIVA), is recommended to enhance diagnostic accuracy.
All guidelines underscore the need for a multimodal approach as the foundation for the management of adult ADHD. They consistently advocate the use of biopsychosocial models of care that integrate pharmacotherapy for ADHD and comorbid conditions, use of evidence-based behavioral interventions, and social support interventions such as organizational coaching, to create comprehensive management plans.
Pharmacological treatment is the first-line intervention in all guidelines. Stimulant medication is preferred, provided there are no contraindications for its use. In India, methylphenidate is currently the only stimulant approved for the treatment of ADHD. Atomoxetine is the preferred non-stimulant medication used particularly in the presence of comorbid anxiety disorder or when there is a heightened risk of substance misuse. The IPS guidelines highlight the need for caution regarding the abuse potential and misuse of stimulant medications in the Indian context. They also highlight the need for ongoing monitoring when prescribing medications for ADHD, particularly when prescribing stimulants. Regular monitoring should include weight, sleep duration and pattern, pulse, blood pressure, cardiovascular status, and overall mental health.
In addition to pharmacotherapy, structured cognitive behavioural therapy (CBT) is effective in improving residual symptoms of ADHD, anxiety, and depression. 13 In a meta-analysis of CBT studies for ADHD, 14 medium to large effect sizes were found for self-reported ADHD symptoms and self-reported functioning. Psychoeducation forms a pivotal part of the comprehensive treatment plan in adult ADHD.
Both the NICE and BAP guidelines highlight the gaps in continuity of care when children with ADHD transition into adulthood. In the Indian context, there is a high risk of treatment dropout among children and adolescents transitioning into adulthood due to an acute lack of specialist resources for this adult population.
Status of Services in India
In India, services for diagnosing and managing adult ADHD remain underdeveloped and fragmented. The general treatment gap for mental health conditions in India is substantial and is estimated to be more than 80%. 15 The IPS has just over 7000 registered psychiatrists nationwide, with more than half practicing in the private sector and urban areas. While some psychiatrists working in tertiary government mental health institutions may have some access to specialists familiar with adult ADHD, many private practitioners have had minimal formal training or clinical exposure in diagnosing and managing the condition.
Although a few private clinical psychologists assess and diagnose adult ADHD, general practitioners and physicians, who are often the first contact point for the patient, typically have limited training in mental health, and the awareness of adult ADHD is far lower.
A widespread lack of awareness about ADHD among the general public, educational institutions, and workplaces means the condition often goes undiagnosed unless it causes severe disruptions in daily life. Adults with undetected ADHD may experience persistent difficulties in meeting academic or occupational goals, despite having the cognitive abilities to succeed. They may also face challenges such as interpersonal conflict, financial instability, substance use, or legal issues. In the absence of a clear diagnosis, such individuals are frequently mislabelled as “lazy,” “irresponsible,” or “difficult,” which exacerbates stigma and delays access to appropriate care. 16
The scarcity of specialists, limited training for psychiatrists in adult ADHD, and poor access to evidence-based treatments, such as behavioral therapy, psychoeducation, and approved medications (both stimulants and non-stimulants), are major challenges in India. Additionally, mental health services are often overwhelmed, with brief consultation times and minimal availability of adult-specific support options such as peer groups, vocational assistance, coaching for managing ADHD, or culturally relevant psychoeducation materials. These gaps highlight the urgent need to develop and establish dedicated, evidence-based services for the diagnosis and management of adult ADHD in India.
Practice Setting
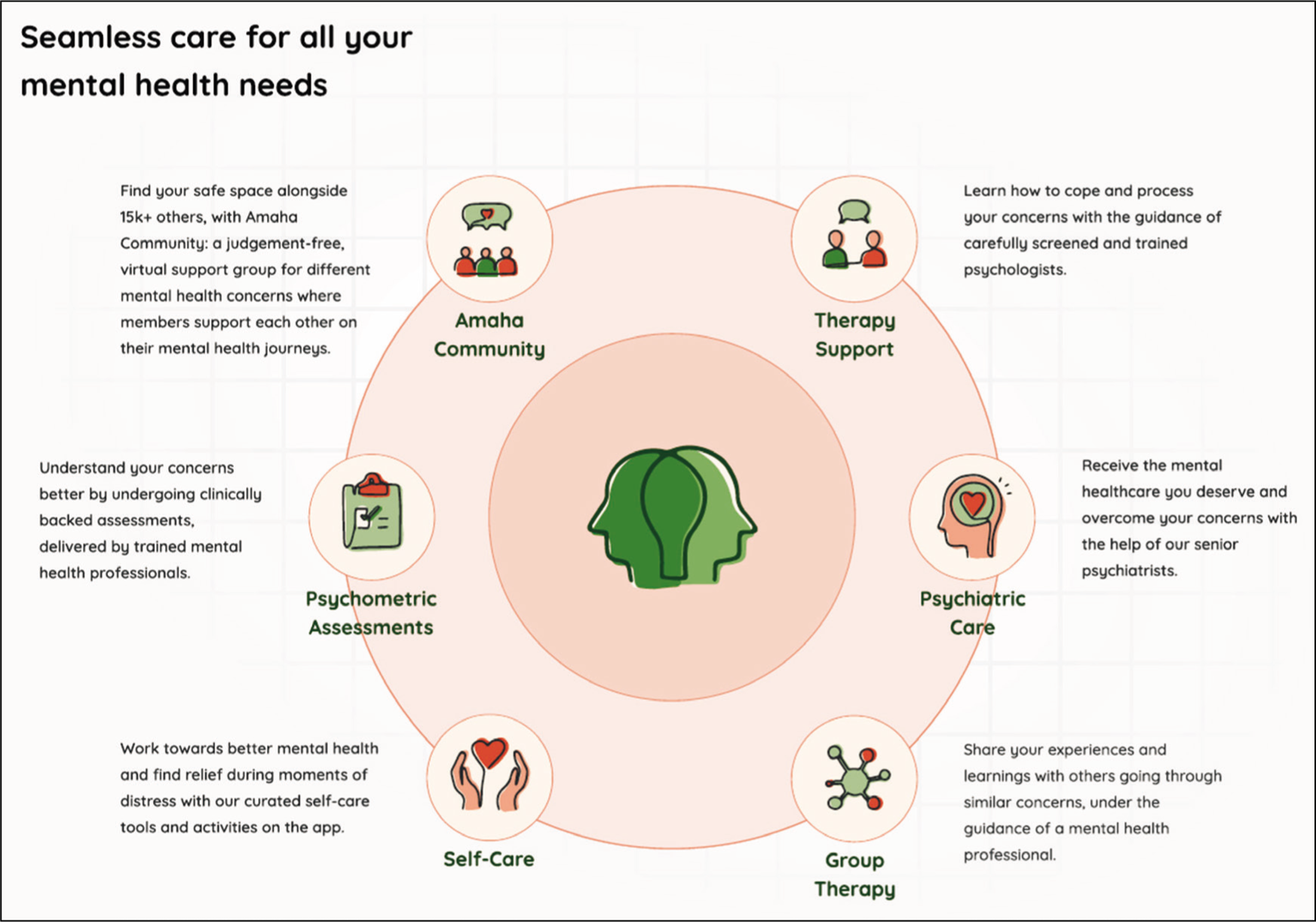
Amaha (formerly InnerHour) is a mental health organization that offers integrated, evidence-based care for a wide range of mental health conditions, including adult ADHD, anxiety, depression, bipolar disorder, OCD, and addictions. Founded in 2016, Amaha’s care model is built on an ecosystem approach, combining psychiatry, psychotherapy, digital tools, and caregiver support into a unified care pathway (Figure 1). Psychiatrists and psychologists work collaboratively to deliver comprehensive assessments and personalized treatment plans. Initial support is facilitated through coach calls, which help individuals and families understand symptoms and navigate appropriate next steps. This integrated model ensures continuity of care while addressing the diverse clinical and psychosocial needs of adults with ADHD.
Care Delivery Channels
Care Delivery Channels at Amaha.
Adult ADHD Services at Amaha: A Structured, Evidence-based Approach
Age Range
Our services cater to adults aged 18 and above. While our services are gender-inclusive, a majority of our clients currently identify as female. However, we are seeing a gradual rise in male and other gender clients seeking support.
Geographic Reach
We provide both physical and teleconsultation-based services. We operate physical centers in Delhi, Mumbai, and Bangalore, serving primarily Tier-1 cities in India. Our teleconsultation services have extended our reach to over 750 cities across the country.
Language Diversity
To support India’s diverse population, we offer services in over 14 languages. At present, our primary languages of delivery, beyond English, are Hindi and Kannada. All brand communications continue to be in English.
ADHD Protocol Development
A comprehensive literature review informed the development of the protocol. Key considerations included the need to address psychiatric and medical comorbidities before initiating ADHD-specific treatment, as well as the importance of obtaining collateral information from individuals familiar with the client’s developmental history. A critical component of the protocol was the adoption of the DIVA as the primary diagnostic tool, given its clinical validity. 17
The essential elements of this protocol included: (a) An initial consultation and screening by a psychiatrist; (b) administration of the DIVA-5 assessment by a trained psychiatrist if ADHD symptoms were indicated; (c) comprehensive diagnostic evaluation including systematic assessment for common psychiatric and medical comorbidities, including substance use; (d) provision of psychoeducation regarding the assessment findings, ADHD and management options; (e) careful consideration of medication prescription under stringent guidelines, accounting for comorbidities and misuse potential; and (f) referral for psychotherapy as appropriate.
Program Development and Clinical Training
The Adult ADHD service was launched in 2022, led by the author herself, who brought her prior experience from the United Kingdom in treating adults with ADHD. Our initial efforts focused on enhancing the knowledge and competence of our clinical team. All psychiatrists and therapists underwent training to recognize and become familiar with ADHD symptoms in adults.
Psychiatrists received in depth training in the diagnostic criteria outlined in ICD-11 and DSM-5, and were also trained in administering the DIVA structured assessment tool. A subset of psychologists with a special interest in ADHD curated support resources tailored to this population.
Awareness and Community Support
We developed a dedicated ADHD landing page on our website and disseminated educational content across social media platforms to improve awareness. An online peer support community, moderated by a psychologist, was created to foster connection and reduce stigma.
Additionally, we designed a self-help workbook that is provided to each community member. This resource includes information on ADHD symptoms and neuroscience, along with practical strategies such as the Pomodoro technique, daily planners, worry diaries, and Specific, Measurable, Achievable, Relevant and Time Bound - goals (SMART) goal-setting.
Clinical Assessment and Diagnostic Process
Diagnosis begins with an initial consultation with a psychiatrist, which involves a comprehensive psychiatric evaluation to screen for ADHD and other co-occurring or differential diagnoses. If an ADHD assessment is deemed necessary, the client is invited for a further 90-minute diagnostic session.
This session includes detailed developmental history gathering, ideally with input from a parent or sibling, and administration of the clinician-led DIVA structured interview. Each symptom is explored in depth across both childhood and adulthood. The session concludes with initial psychoeducation and confirmation (or refutation) of the diagnosis.
Treatment Pathways
Following a formal diagnosis, the psychiatrist provides tailored psychoeducation to the client and their family. For mild to moderate cases, therapy is often the first-line of intervention, especially to address anxiety and self-esteem issues. Pharmacological treatment may be considered for co-occurring conditions such as depression or anxiety.
In moderate to severe cases, or when the client opts for medication, treatment options, including both stimulant and non-stimulant medications, are discussed in detail. Amaha adheres to national regulations for psychotropic prescriptions. Medications are prescribed only in offline settings; online clients requiring pharmacotherapy are referred to local psychiatrists.
Medication Protocol
Atomoxetine is the first-line non-stimulant medication, with bupropion considered in some cases. For clients with active substance misuse, only non-stimulants are prescribed, along with integrated treatment for the addiction.
Methylphenidate is the only stimulant medication currently available for ADHD in India. Before initiation, clients undergo cardiac screening, including an electro cardio gram (ECG), and provide written informed consent. Prescriptions are issued for a maximum of 30 days, with in-person follow-ups required for each refill. Vital signs are monitored before every re-prescription.
Integrated Care Approach
All clients are encouraged to engage in psychotherapy alongside medication. Complementary interventions such as yoga, regular exercise, and bibliotherapy are recommended to promote self-awareness and holistic well-being. This integrated, multidisciplinary approach ensures that clients receive comprehensive and evidence-based care tailored to the unique challenges of adult ADHD in the Indian context.
Proposed Recommendations for Developing Expertise and Services for Adult ADHD
National psychiatry and psychology curricula should incorporate robust, evidence-based training on adult ADHD, including diagnostic criteria, use of assessment tools such as DIVA, and treatment options.
Awareness campaigns targeting both the general public and healthcare professionals are essential to reduce stigma, correct misconceptions, and encourage timely help-seeking.
Assessment tools, psychoeducation material, and self-help tools should not only be culturally adapted but also be made available in multiple Indian languages to improve accessibility and relevance.
Services must integrate psychiatry, psychotherapy, coaching, and occupational support, ensuring a holistic approach to ADHD management that goes beyond symptom control.
Expanding telepsychiatry while simultaneously building robust offline services, especially in underserved regions, will bridge geographical and logistical barriers to care. Re-looking at our tele-prescribing guidelines to help us use telepsychiatry more effectively while managing the risk of misuse of prescription needs to be considered. This will enable platforms such as Amaha to deliver appropriate evidence-based treatments to remote areas of our vast country.
Including Adult ADHD diagnosis and treatment into the National Mental Health Program can support mainstreaming ADHD care into national public health priorities. District Mental Health Programs (DMHPs), which are active across India, can be leveraged to extend ADHD services across the country. This will need focused training of DMHP mental health professionals in adult ADHD diagnosis and management, developing simplified psychoeducational materials in regional languages, and creating pathways for referral to tertiary or digital mental health care specialty clinics.
Adult ADHD is not explicitly included in public insurance frameworks such as Ayushman Bharat, nor is it commonly reimbursed by private insurers. Regulatory changes under the Insurance Regulatory and Development Authority of India are needed to comply with the mandate of the Mental Health Care Act (MHCA) 2017 to prevent non-discrimination.
Establishing moderated community groups and caregiver education initiatives can empower individuals with ADHD and their families, improving long-term outcomes.
Conclusion
Adult ADHD is a complex, often misunderstood neurodevelopmental condition that remains significantly underdiagnosed and undertreated in India. While awareness is gradually growing, driven by an increased discourse on social media, shifting public narratives, and evolving clinical practices, the existing mental health infrastructure is not yet equipped to meet the rising demand for accurate diagnosis and effective, long-term care.
India’s mental health system faces several barriers, including a shortage of trained professionals, limited awareness among healthcare providers and the public, a lack of culturally contextualized psychoeducational materials, and minimal access to evidence-based interventions tailored toward such adults. These systemic gaps contribute to widespread misdiagnosis or delayed diagnosis, exacerbating the functional impairments and psychological distress experienced by adults with ADHD.
Despite these challenges, emerging services such as those offered by Amaha represent a significant step forward. By integrating best practices from international guidelines and tailoring them to the Indian context, Amaha’s structured and evidence-based model for adult ADHD care demonstrates that scalable and impactful interventions are achievable.
India is at a pivotal moment in the recognition and treatment of adult ADHD. By scaling models such as Amaha’s and embedding ADHD care into the broader mental health ecosystem, it is possible to create a future where individuals with ADHD are accurately diagnosed, meaningfully supported, and empowered to thrive.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Not applicable as this article does not report any patient data.