
Abstract
Background:
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder, traditionally seen as a childhood disorder; recent studies show that it persists into adulthood, affecting 2.58% of adults globally. ADHD often runs in families, with genetic and environmental factors contributing to its persistence across generations. The aim of the study was to assess the prevalence of ADHD, neuropsychological functioning, and psychiatric comorbidities in the family members of adults diagnosed with ADHD in childhood.
Methods:
This cross-sectional, analytical study was conducted at a tertiary care hospital. Family members of adult males who were diagnosed with ADHD, including parents and siblings, were assessed for ADHD symptoms and psychiatric comorbidities. Neuropsychological testing for cognitive impairments in attention, memory, and executive functions was done. Statistical analysis was conducted using IBM SPSS, with chi-square and t-tests applied for group comparisons.
Results:
Thirty male adults were the reference group diagnosed with childhood ADHD. Family history of ADHD was positive in 36.7% of the reference group, with 11 members screening positive for ADHD (7 siblings and 4 parents) out of 82. Neuropsychological testing in these family members revealed deficits across multiple cognitive domains, particularly in sustained attention (81.8%), working memory (81.8%), and planning (100%). Psychiatric morbidity was found in 40% of family members, with substance use disorder being the most common (16.7%).
Conclusion:
A significant proportion of family members of adults with ADHD also exhibit symptoms of ADHD, reinforcing the genetic link. Neuropsychological deficits in attention, memory, and executive function were prominent in affected family members.
Keywords
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by impaired levels of inattention and/or hyperactivity-impulsivity, with the worldwide pooled prevalence of ADHD in children and adolescents of 5.29%. 1 Follow-up studies show the prevalence of persistent adult ADHD being 2.58% and of symptomatic adult ADHD being 6.76%. 2
The development of ADHD arises from a complex interplay of biological and psychosocial elements. There is a significant genetic component to ADHD, with higher rates observed in the parents and siblings of affected children. 3 A family assessment in the context of ADHD is crucial for understanding the broader impact of ADHD on the individual and the family as a whole. ADHD affects not only the person diagnosed with it but also has far-reaching consequences for family relationships, dynamics, and functioning. The need for a family assessment stems from the recognition that ADHD can influence multiple aspects of family life and well-being.
Parents of children with ADHD report more symptoms compared to those whose children do not have the disorder. 4 Additionally, the severity of a child’s ADHD tends to be greater when the parents are also affected. Family studies demonstrate that children of adults with ADHD have a higher risk of developing the condition than those from control groups. 5 The heritability estimates for ADHD symptoms are around 30% for overall symptomatology, 35% for inattention, and 23% for hyperactivity. 6
Twin studies reveal a high heritability rate for ADHD, estimated at approximately 76%. Molecular genetic research has identified several genes associated with ADHD, notably those coding for DRD4, DRD5, SLC6A3, SNAP25, and HTR1. Linkage studies have pinpointed genetic loci linked to adult ADHD, leading to the identification of LPHN3 and CDH13 as novel genes associated with ADHD across different life stages. The results showed that 52% of the phenotypic correlation between hyperactivity-impulsivity and inattention (r = 0.43) was explained by genetic influences, whereas non-shared environmental influences explained the remaining part of the covariance. 6
Siblings of adults with ADHD were found to have a strongly increased ADHD risk (41%) as compared to the risk of ADHD among siblings of children with ADHD (15%).7,8
The present study was conducted with the objectives of evaluating the clinical features of subjects with adult ADHD, evaluating family members of the subjects for ADHD and psychiatric comorbidities, and studying their neuropsychological profile.
Material and Methods
The study was initiated after obtaining approval from the institutional research and ethics committee and registration with the Clinical Trials Registry of India.
Study Design and Setting
This analytical and cross-sectional study followed the STROBE cross-sectional reporting guidelines. 9 Participants were recruited from individuals attending outpatient services in the Department of Psychiatry of a tertiary care hospital between February 2017 and June 2018.
The sample (n = 82) consisted of family members of 30 persons with a primary childhood diagnosis of ADHD. At the time of the study, the ADHD group comprised male participants aged 18–35 years with a childhood diagnosis of ADHD, having at least 10 years of formal education, and no history of epilepsy, organic disease (including head injury), or substance dependence (except nicotine).
For the family assessment, a total of 82 family members were assessed: 29 fathers (as 1 subject’s father had expired), 30 mothers, and 23 siblings.
Written informed consent for the study was taken from the participants. All family members consented to the study. Socio-demographic details were recorded using a semi-structured proforma routinely employed in outpatient services. For clinical assessment, the scales used were:
Adult ADHD Self-Report Scale (ASRS-v1.1): The ASRS-v1.1 is a diagnostic instrument designed to assess ADHD in adults as per DSM-IV-TR. The self-report format allows individuals to provide information about their symptoms directly.
10
Wender Utah Rating Scale (WURS): The WURS is a self-report tool used to evaluate symptoms of ADHD from childhood, according to the Utah criteria. The original version of the scale included 61 items, which were reduced to 25.
11
Vanderbilt ADHD Parent Rating Scale (VADPRS)
12
: The VADPRS is a 55-item Likert-type rating scale used by parents to rate the behavior of their child aged 6–12 years. It makes the diagnosis of ADHD and comorbidities as per DSM criteria. Neuropsychological Test Battery: This battery included the Color Trail Test for focused attention, the Digit Vigilance Test for sustained attention, the Triads Test for divided attention, the Stroop’s Test for response inhibition, the N-Back Test for verbal and visual working memory, the Controlled Oral Word Association (COWA) Test for phonemic fluency, the Tower of London Test for planning, and the Rey Complex Figure Test for visual learning and memory.
13
A complete assessment of all the family members, including parents and siblings, for the presence of ADHD was conducted using clinical evaluation, the ASRS-v1.1, and the WURS. One family was contacted telephonically as they were staying more than 1000 Km away. For siblings less than 12 years of age (n = 1), VADPRS was used to assess for ADHD. Detailed neuropsychological testing was conducted for family members who screened positive for ADHD on the ASRS. The diagnosis was recorded in the clinical proforma. Any psychiatric illness so diagnosed was managed as per clinical need. The assessment of each participant took around 150–180 minutes.
Statistical Analysis
The data was initially entered into the Microsoft Excel version and later transferred to a licensed IBM SPSS version 20.0. for analysis. Mean and standard deviation for ordinal variables and frequency tabulation (with percentage values) for nominal variables were carried out. Comparative statistics were applied across 2 groups. Nominal variables were analyzed using the chi-Square test or Fisher’s exact probability test (where the value in any cell was less than 5), and ordinal variables were analyzed using Student’s t-test. As repeated intra-group measurements were generated, the ANOVA test (as a test of variance) was applied to see the degree of change within each group.
Result
The persons with ADHD were 30 males, the majority (63.4%) aged less than 20 years. Eighty percent were students, and 53.3% had 8–12 years of formal education. Of the participants, 96.7% were single, and 53.3% belonged to the upper social class according to the Modified Kuppuswamy Scale.
The mean distribution of ASRS scores in family members of adult ADHD participants was calculated. The father of 1 patient was not alive, so the number was 29. WURS was applied to only those who had screened positive for ADHD on the ASRS scale; hence, there were only 11 family members, whose mean score was 63.5 (Table 1). The sibling of 1 patient was aged 12 years; thus, the Vanderbilt ADHD Diagnostic Rating Scale was applied, and ADHD was ruled out.
Mean ASRS and WURS Scores Obtained Among Family Members (N = 82).
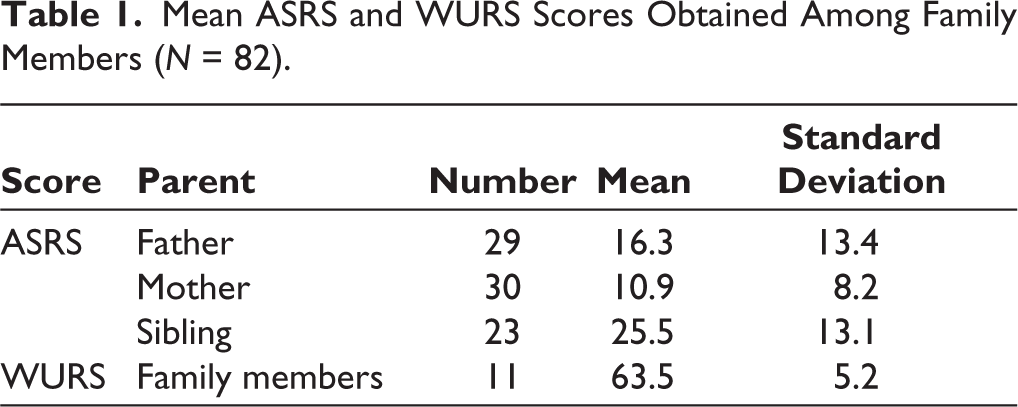
On screening with ASRS, 11 (36.7%) family members of adults with ADHD screened positive for ADHD. Of these, 2 were mothers and 2 were fathers (6.7% each), and 7 (23.3%) were siblings, 1 sister and 6 brothers.
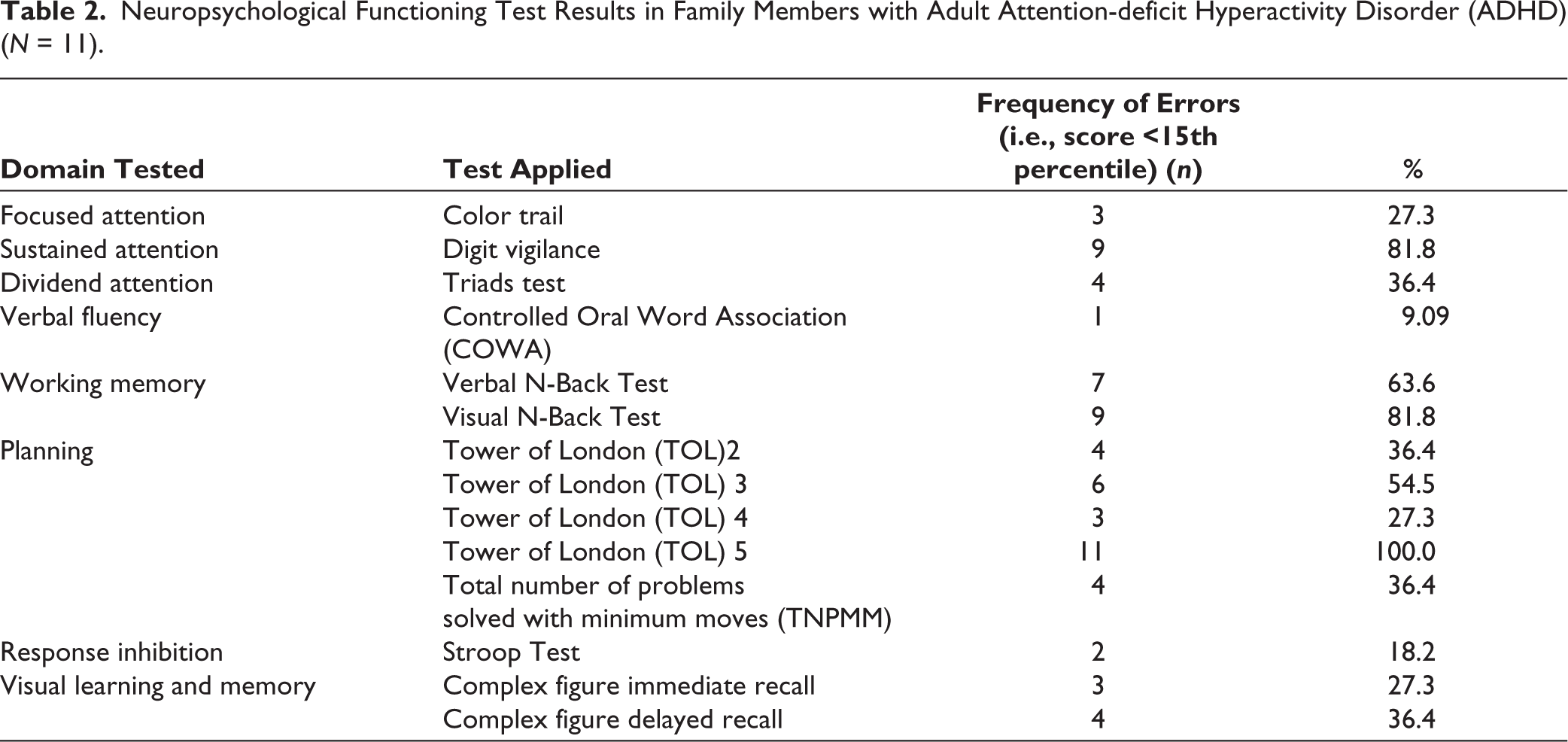
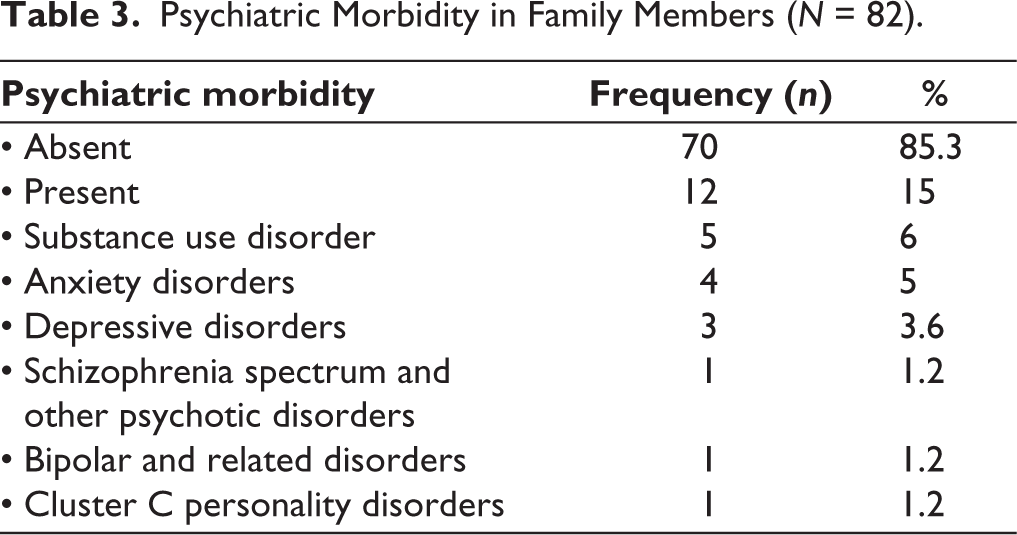
For family members of participants who had screened positive for ADHD on ASRS, neuropsychological testing was done, and results were obtained in the form of impairment (i.e., score less than 15th percentile) on various neuropsychological domains. The highest percentage of errors, defined as scores below the 15th percentile, was obtained on planning (100%), followed by Sustained Attention and Working Memory (81.8% each). Twelve (15%) of the family members had psychiatric comorbidity. The most common psychiatric morbidity was substance use disorder in 5 (6%). (Tables 2 and 3)
Neuropsychological Functioning Test Results in Family Members with Adult Attention-deficit Hyperactivity Disorder (ADHD) (N = 11).
Psychiatric Morbidity in Family Members (N = 82).
Discussion
This study provides valuable insights into the clinical characteristics, familial correlations, and neuropsychological profiles of adults with ADHD and their family members. The findings emphasize the multifaceted impact of ADHD, extending beyond the individual to influence family dynamics, genetic predisposition, and neuropsychological functioning.
In the present study, the reference group comprised only males aged 18–25 years, as the prevalence was twice that observed in females. The diagnosis of ADHD is most likely to be missed in females, along with being protective against the same, 13 with the majority being unmarried, belonging to upper socioeconomic status as per the Modified Kuppuswamy Scale, and residing within the cities.
The family assessment underscored the significant heritability of ADHD, with 36.7% of family members screening positive for ADHD on the ASRS scale. The study’s findings support existing research indicating that ADHD has a strong genetic component, with higher rates of ADHD among siblings (23.3%) compared to parents (6.7%). Among family members, 3 females (27%) and 8 males (73%) had ADHD. Interestingly, siblings demonstrated higher mean ASRS and WURS scores than parents, possibly reflecting the closer generational proximity and shared environmental factors. The observed familial clustering of ADHD symptoms reinforces the role of genetic and shared environmental influences in the disorder’s development. 14
Family members with ADHD demonstrated significant impairments in neuropsychological domains, with planning, sustained attention, and working memory being the most affected. These findings suggest that ADHD’s cognitive impact extends across the lifespan and affects not only diagnosed individuals but also their family members who remain undiagnosed. The 100% impairment rate in planning among family members, as assessed by the Tower of London Test, is particularly striking and highlights the pervasive nature of executive function deficits associated with ADHD. Rommelse et al. found significant heritability of 2 significant genome-wide linkage signals, 1 for the motor timing task on chromosome 2q21.1 (LOD score: 3.944) and 1 for the digit span test on 13q12.11 (LOD score: 3.959) using neuropsychological tests in a genome-wide analysis. 15 The dual pathway model links ADHD symptoms to distinct brain dysfunctions: Inattention and executive deficits to prefrontal-striatal circuits, and hyperactivity to frontal-limbic systems. Another model highlights poor behavioral adjustment due to disrupted bottom-up signaling or inefficient top-down control. 16
These results are consistent with prior research indicating that neuropsychological impairments, especially in executive functions, are central to ADHD. Such deficits can exacerbate challenges in daily functioning, impacting educational, occupational, and interpersonal outcomes. 17
The most common morbidities found were substance use disorder (6%), which can be attributed to shared characteristics such as dopaminergic dysregulation of the motivational and reward system, or decreased functioning in the frontal lobe, followed by anxiety disorder (5%), in which common brain areas are seen to be involved such as dorsolateral prefrontal cortex or the anterior cingulate cortex and lastly depressive disorder (3.6%), with both having low hedonic responsivity and similar pathophysiologic regions of the brain including decreased activity in the prefrontal, amygdala, and hippocampus regions. 18 On the other hand; Cluster C personality disorder, schizophrenia, and bipolar disorder were seen in one case each. The presence of comorbidities underscores the need for comprehensive assessments and integrated treatment approaches that address co-occurring mental health issues.
The study’s findings emphasize the importance of adopting a family-centered approach to ADHD assessment and management. Understanding the familial clustering of ADHD symptoms and associated neuropsychological deficits can guide clinicians in developing more effective and personalized treatment plans. Interventions targeting parenting practices, familial communication, and environmental modifications could mitigate the impact of ADHD on family dynamics. Additionally, the high prevalence of psychiatric comorbidities in family members suggests that screening and treating these conditions should be an integral part of ADHD management.
This study had several strengths, including detailed clinical assessment of all subjects; use of diagnostic tools; neuropsychological assessment; study of clinical course and comorbidities; and assessment of family members. Adult ADHD was examined as a concept. However, it is not without its limitations, such as a relatively small sample size and a lack of generalizability of results due to subjects hailing from North India. The effect of comorbid psychiatric conditions could also affect neuropsychological functioning. Only males were included; hence, the results cannot be generalized to females. Additionally, current or past treatment for the condition was not taken into account.
Conclusion
The study underscores the critical role of family assessments in understanding and managing adult ADHD. By examining familial patterns, psychiatric comorbidities, and neuro-psychological deficits, the research highlights the hereditary and environmental dimensions of ADHD. The findings reveal significant ADHD prevalence among family members, particularly siblings, alongside notable deficits in executive functioning such as attention, working memory, and planning. Additionally, a substantial portion of family members exhibited psychiatric morbidity, emphasizing the broader impact of ADHD on familial mental health.
This study demonstrates the need for a holistic approach to the management of ADHD, including the family. It suggests that targeted interventions addressing family dynamics, comorbidities, and shared vulnerabilities can enhance treatment outcomes for individuals with ADHD and their families.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors attest that there was no use of generative artificial intelligence (AI) technology in the generation of text, figures, or other informational content of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Written informed consent was obtained from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. Ethical approval was granted by the Institutional Ethics Committee of Government Medical College and Hospital, Chandigarh (Approval No. EC/2016/0052; dated December 28, 2016). CTRI Number: CTRI/2018/01/011397.