
Abstract
Background:
Psychiatric disorders and emotional abnormalities are frequently encountered in pediatric referrals. Parenting stress is considered to be a significant factor leading to disrupted children’s appointments in general pediatric clinics.
Methods:
We conducted this retrospective descriptive study to observe the sociodemographic and clinical profile of patients referred to a rural hospital’s Child Guidance Clinic. The rationale for the study was to analyze the rates of psychiatric disorders, referral patterns, and psychiatric diagnoses in the Child Guidance Clinic, as patients with psychiatric disorders—especially children and adolescents—tend to visit non-mental health clinics for their symptoms rather than mental health clinics. The study was conducted at a rural medical college in Central India, where the Child Guidance Clinic is run twice a week. Case files of all children and adolescents (up to the age of 18) referred to the Child Guidance Clinic of a Psychiatry Outpatient Department between 2018 and 2023 were analyzed. A semi-structured proforma was used to collect sociodemographic and clinical information. Descriptive and statistical inferences were applied using Epi Info-7 software.
Results:
The study included data from 750 pediatric referrals to the Child Guidance Clinic, referred for irritability, restlessness, aggressive behavior, self-harm attempts, sadness, and poor scholastic performance. A significant proportion of referrals originated from the pediatrics department (48%), followed by medicine (22%) and surgery (11%). Among the International Classification of Diseases, Tenth Revision psychiatric diagnoses, mental retardation was found to be the most common (25.8%). The study focused on pediatric psychiatric referrals. The most common cause for referral was externalizing problems, and the most common psychiatric disorders were mental retardation, conduct disorder, and attention deficit hyperactivity disorder.
Conclusions:
Age group comparison showed that children were more likely to be diagnosed with hyperkinetic and developmental disorders, while adolescents were more likely to be diagnosed with depressive disorder.
Keywords
Introduction
Epidemiological research suggests that more than 10% of children and adolescents in the community suffer from psychiatric disorders, yet very few of them receive expert care. 1 Patients with psychiatric disorders tend to visit nonmental health clinics for their symptoms rather than mental health clinics. 1 Psychiatric comorbidities in young children are frequently undiagnosed and therefore undertreated. 1
Most pediatricians notice psychological disturbances in children admitted to their wards, and this becomes the most common reason for their referral to the Child Guidance Clinic (CGC). However, parental cooperation is found to be poor in subsequent follow-ups. 2 The prevalence of psychiatric disorders among rural children is comparable to that of urban children (7%–20%), but a lack of mental health specialists and evidence-based treatments renders healthcare systems inadequate to meet the mental health needs of rural children. 2 In recent years, a few community and clinic-based epidemiological studies in India have been undertaken, which are critical for service planning, resource allocation, assessment of service utilization, and follow-up. 3 New innovations in pediatric practice, as well as increased interest in genetic and neurological factors in child behavioral issues, now necessitate collaboration between the two professions. 4
The attitude of hospital staff toward children and adolescents suffering from mental health issues is of utmost importance, as it plays a significant role in the prognosis of disease. 5 Psychiatric disorders and emotional abnormalities are frequently encountered in pediatric referrals. 6 Family stress, particularly parenting stress, is considered to be a significant factor leading to disrupted children’s appointments in general pediatric clinics. 6 Child and adolescent psychiatric symptoms may be present as associated or background features in children with somatic manifestations, although physician detection of these behavioral disorders is limited. 6 Studies have shown that 40% of adults with medical problems have established psychiatric comorbidity, but issues in children and adolescents have received less scientific focus. 6
Children and adolescents with behavioral disturbances tend to visit the Pediatric Outpatient Department (OPD) before being referred to Psychiatry. Pediatric consultation-liaison comprises all consultations, liaison, diagnostic, therapeutic, teaching, support, and research activities carried out by psychiatrists and other mental health professionals. These services can be effectively utilized to bridge treatment gaps. Hence, we conducted this study with the rationale to observe clinical and sociodemographic profiles and to analyze referral patterns and rates of psychiatric diagnoses among patients referred to a tertiary hospital’s CGC.
Material and Methods
The study was conducted at a rural medical college that has a postgraduate psychiatric department with 24-h consultation-liaison psychiatry services. The procedure followed for referred patients is as follows: referred patients were assessed by both the resident and consultant, and a diagnosis was made according to the International Classification of Diseases, Tenth Revision (ICD-10). Assistance from a clinical psychologist and psychiatric social worker was sought whenever necessary, and psychological and pharmacological interventions were then started. This retrospective study was started after approval from the institutional ethics committee.
Records of children and adolescents (up to the age of 18) referred to the CGC from 2018 to 2023 were assessed and analyzed using the case record section of the clinic. Sociodemographic and clinical information was collected using a semi-structured proforma, including age, gender, socioeconomic status, and family details. The proforma also included the department of referral, reasons for referral, and comorbidity of the referred child or adolescent. A total of 750 pediatric patients were referred to the CGC from 2018 to 2023, and all of them were included in the study by convenient sampling method. All these referrals were studied for data adequacy. The only exclusion criterion was inadequate information in the case records. After applying the exclusion criterion, records of 737 patients were analyzed.
Statistics
Descriptive and statistical inferences were made using Epi Info-7 software. Data were tabulated using MS Excel. SPSS 21 software was used for analysis. The chi-square test was used for inferential statistics, and P < .05 was considered significant.
Results
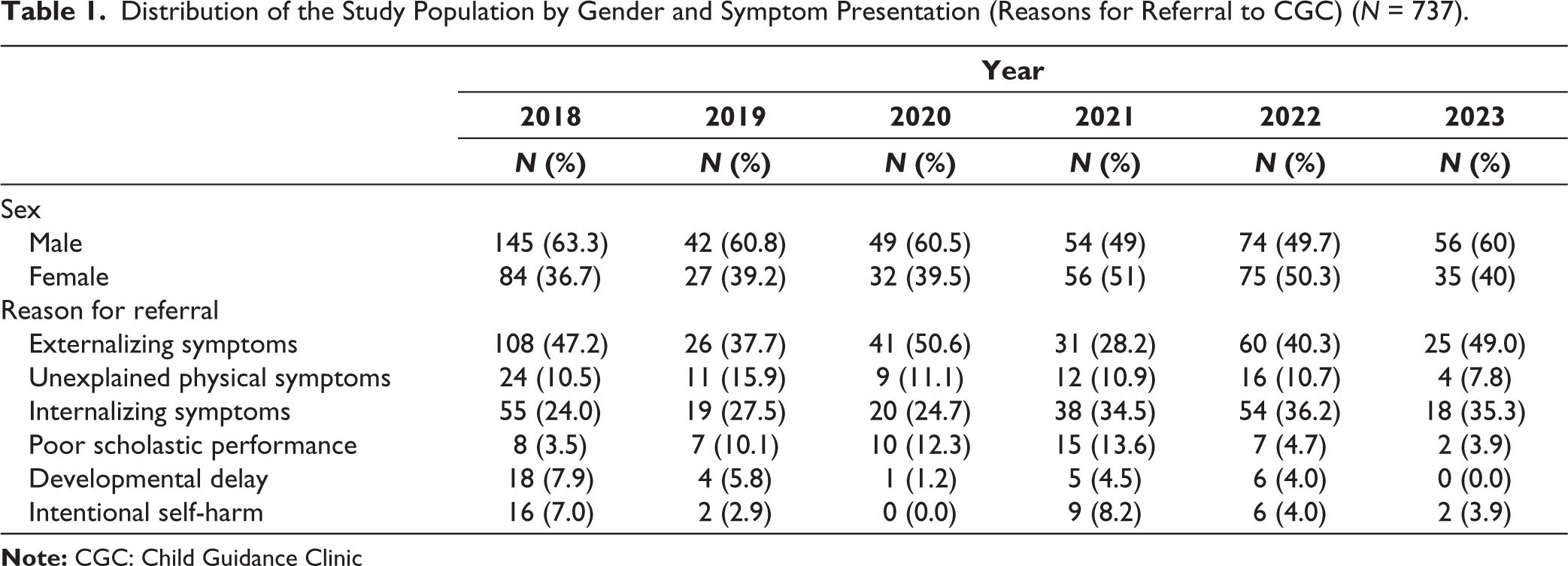
A total of 750 pediatric patients were referred to the CGC from 2018 to 2023. Out of those, after excluding the records with inadequate information and data cleaning, a total of 737 patient records were analyzed. The mean age was 13 years, and 57% of referrals were males. Children and adolescents were referred for varied symptoms such as irritability, restlessness, aggressive behavior, self-harm attempts, sadness, and poor scholastic performance. Only 5% of them had a family history of any psychiatric illness. The most common reasons for referrals were externalizing symptoms related to poor impulse control such as aggression, disruptive behavior, rule breaking, etc. (42.2%). The second most common referral was for internalizing symptoms such as sadness of mood and reduced communication (30.3%). When compared to adolescents, a significant proportion of children were referred for externalizing symptoms, whereas internalizing symptoms were the common reason for referral in adolescents (Table 1).
Distribution of the Study Population by Gender and Symptom Presentation (Reasons for Referral to CGC) (N = 737).
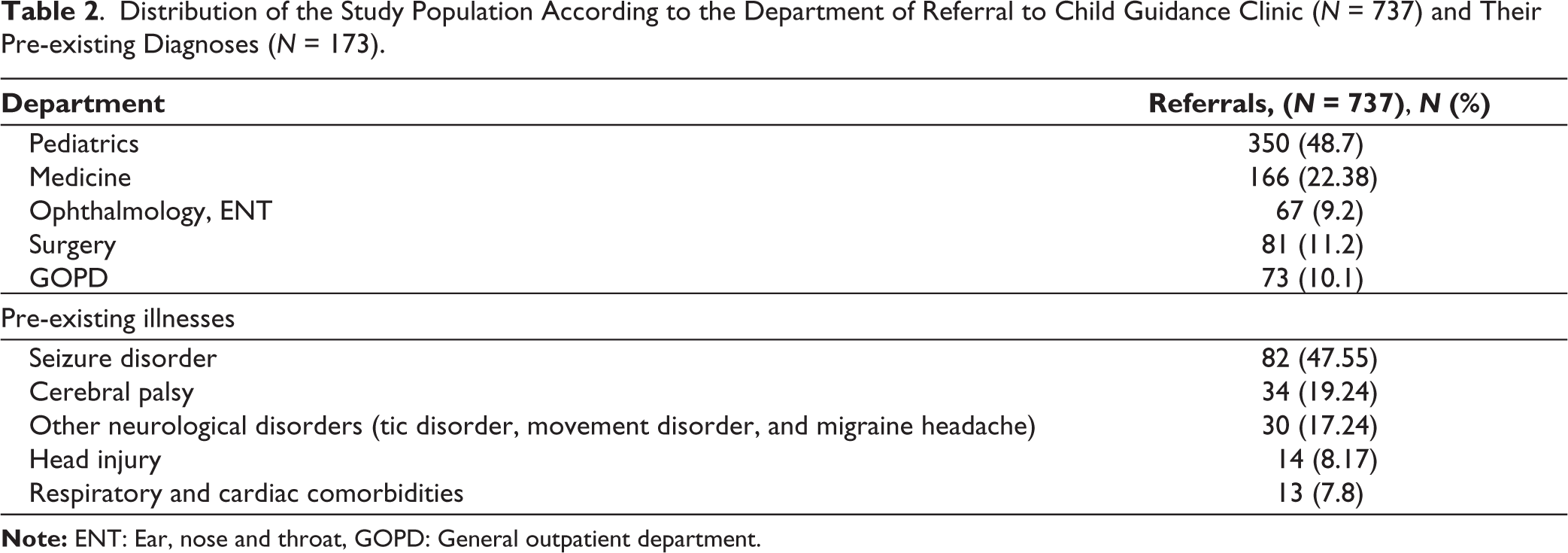
A significant proportion of referrals originated from the pediatrics department (48%), followed by medicine (22%), surgery (11%), and 9% from other departments. Out of all those referred, 173 (23.45%) children and adolescents had pre-existing neurological illnesses, among which the most common were seizure disorders (47.55%), cerebral palsy (19.24%), and other disorders (tic disorder, movement disorders, migraine headaches, etc.) (17.24%). A total of 564 children (76.55%) had no underlying illness (Table 2).
Distribution of the Study Population According to the Department of Referral to Child Guidance Clinic (N = 737) and Their Pre-existing Diagnoses (N = 173).
Among the ICD-10 psychiatric diagnoses, mental retardation was found to be the most common (25.8%). Conduct disorder (7%) and attention deficit hyperactivity disorder (6.5%) were found to be the next most prevalent. Autism spectrum disorder was found in 3.6% of cases. Additionally, 6.9% of children and adolescents referred for various symptoms did not receive any psychiatric diagnosis. When children and adolescents were compared amongst themselves for reasons for referral and psychiatric diagnoses, children were mainly referred for externalizing symptoms, whereas adolescents were referred for internalizing symptoms. Children were more likely to be diagnosed with hyperkinetic and developmental disorders, while adolescents were more likely to be diagnosed with depressive disorder (Table 3).
Reason for Referral and Psychiatric Disorders Among Children and Adolescents (N = 737).
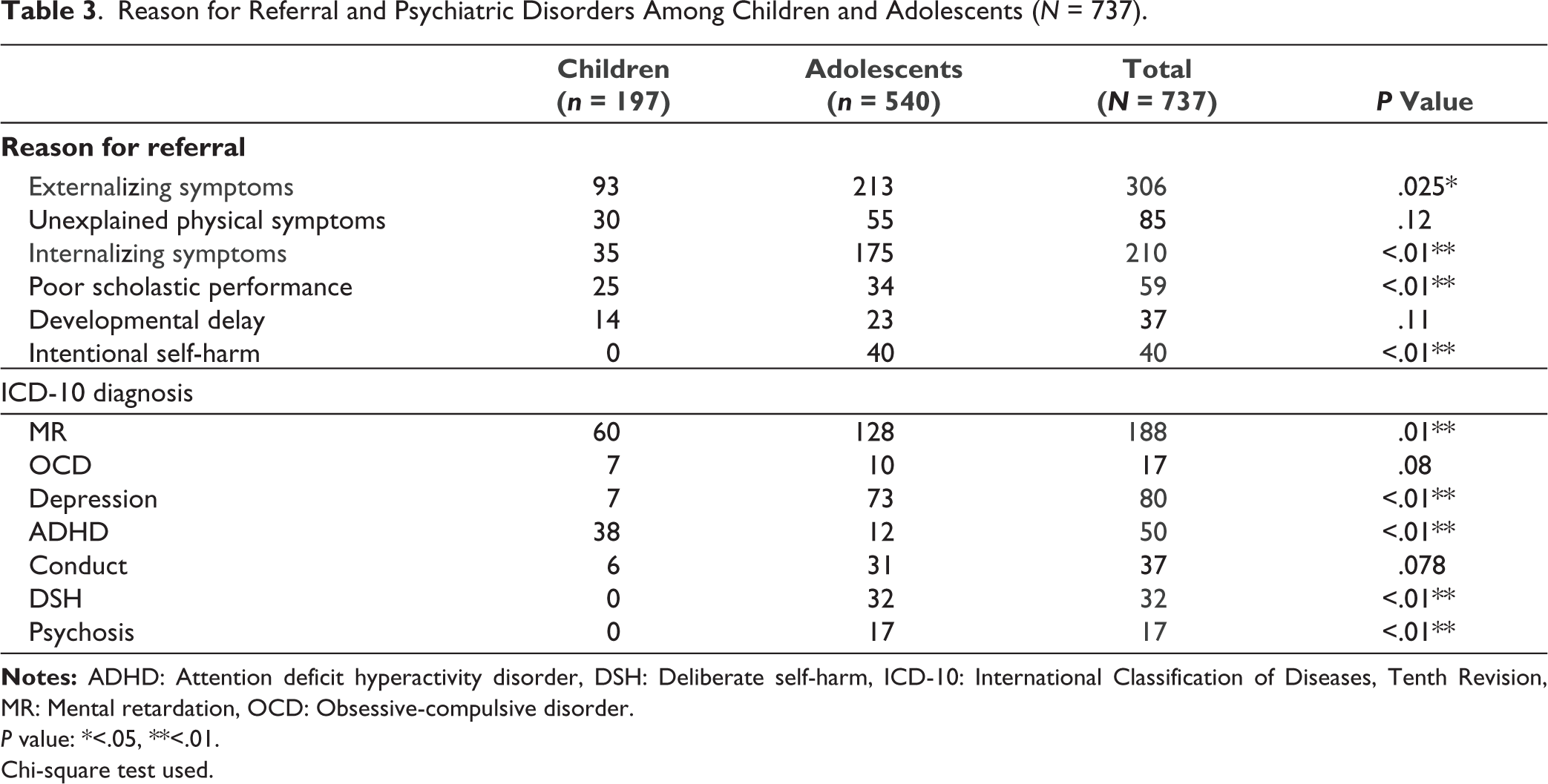
P value: *<.05, **<.01.
Chi-square test used.
Referred children and adolescents were considered for both psychotherapy and pharmacotherapy (antidepressants, mood stabilizers, and antipsychotics). The patients along with parents were advised to have regular follow-ups in the CGC, but only 38.08% of them were found to have subsequent follow-ups.
Discussion
The study is focused on pediatric psychiatric referrals in a rural tertiary healthcare setting. Considering the significant disparities in the care pathways for psychiatric disorders—including help-seeking behavior, stigma, and the sociocultural characteristics of Indian patients, especially in the context of child mental health issues—we felt it was important to explore this area further.
The mean age of the sample was 13 years, which falls within the age group commonly reported by most previous researchers.1,2,5,7 Boys outnumbered girls (57%), a finding consistent with earlier research.8–11 Sociocultural factors may play a role in help-seeking behavior, as Indian parents are often more concerned about the health of their male children than that of their female children.8–11 On the other hand, a community-based Indian epidemiological research study of child and adolescent mental health by Srinath et al. found that there were no gender differences. 7 An American study by Costello et al. found that younger children exhibited a higher frequency of psychopathology than adolescents, and disparities between psychopathological presentations may indicate a lack of understanding among parents and the medical community in different countries about mental health. 12
The majority of patients (48%) were referred from the Department of Pediatrics. Studies conducted in the Indian context by Desai et al. about psychiatric referrals in tertiary care, and a study by Bhogale et al. in a multispeciality hospital noticed a similar pattern.8,11 Similarly, studies about liaison services done in the American context by Briggs-Gowan et al. and Lipowski also reflected similar findings.13,14
Psychological issues in children can present as physical symptoms, necessitating pediatric consultation. The Department of Medicine was the second most common source of referral (22%), likely due to the fact that many psychiatric conditions, such as conversion reactions and dissociative motor and sensory disorders, can mimic neurological problems. Studies indicate that around 15% of patients evaluated by neurologists have no identifiable physical basis for their symptoms, while another 15% exhibit symptoms that are disproportionate to the underlying condition. As a result, these patients are often referred for psychiatric evaluation.3,4,7
A total 564 children (76.55%) among the 737 had no underlying physical illness, yet most of them were referred to Psychiatry from the Departments of Pediatrics, Medicine, and Surgery. This finding is consistent with the study on the clinical profile of children and adolescents attending the Behavioral Pediatrics Unit by R. Jayaprakash. It may be attributed to the standard practice of first ruling out physical causes for behavioral symptoms in children and adolescents, which often leads them to consult a pediatrician or physician before being referred to a psychiatrist. 15 The same finding has also been mentioned in a study by Grover et al. in the Indian context 16 ; Al Haidar in the Saudi Arabian context 17 and in a referral study about psychiatric-related visits to Pediatric Emergency Departments by Grupp-Phelan et al. in the American context. 18
The pathway of care for psychiatric illness is another important consideration, as in India, mental health professionals are seldom the first point of contact for individuals with psychiatric issues. In a study conducted on psychopathology in pediatric primary care by Costello et al., the importance of primary care pediatricians in the identification, prevention, and treatment of “the new hidden morbidity” (emotional and behavioral issues in children) is highlighted; which signifies the need for early and proper referral. 19
Depressive disorders, hyperkinetic disorders, and stress-related disorders were the most frequently diagnosed psychiatric conditions among children attending the CGC. Chronic physical illness in children is well-known to be associated with psychosocial repercussions such as depression and anxiety. The most common comorbidity among the referred children and adolescents in this study was found to be neurological (including seizure disorder, cerebral palsy, tic disorder, movement disorder, and migraine headache). Behavioral and psychiatric symptoms among these children could be related to a common neurobiological etiology underlying both psychiatric and neurological disorders, or may occur as a reaction to the impairment due to physical illness.
Patients with mental retardation and behavioral disturbance requiring significant attention and treatment were the most frequently followed up in the OPD. The fact that hyperkinetic and disruptive disorders begin at a younger age than depressive and anxiety disorders explains why children were more frequently referred for externalizing symptoms and diagnosed with hyperkinetic disorders, whereas adolescents were more frequently referred for internalizing symptoms and diagnosed with depressive disorders.
Forty children (5.4%) were referred for deliberate self-harm evaluation. Grover et al. discovered that 0.82% of children and adolescents were referred for evaluation of self-harm behavior in a major hospital-based study from India. 16 In contrast, a much higher proportion of children engaged in purposeful self-harm during studies conducted abroad. 18 The cause for this variance could be differences in research settings (e.g., studies conducted in emergency departments) or underreporting of intentional self-harm in India due to stigma and fear of legal repercussions. 16
The fact that only 38.08% of patients had subsequent follow--ups may be due to improvement of symptoms after the first consultation, but it also highlights help-seeking behavior, stigma, and sociocultural features of Indian patients. However, in a study of psychiatric referrals in a multispeciality hospital by Bhogale et al. conducted at KLE Hospital, Belgaum, 57.38% of pediatric outpatient referrals to the Psychiatry OPD were seen in subsequent follow ups. 11 The disparity in this finding may be due to improvement in externalizing problems after pharmacotherapy was started during the first evaluation.
Conclusion
The majority of participants were male adolescents referred from the pediatrics or medicine departments. Neurological disorders were the most common comorbidity among them and three-fourths of referrals had no other illness. The most common causes for referral were externalizing problems and unexplained physical complaints. The most prevalent psychiatric diagnoses included intellectual disability, conduct disorder, and attention deficit hyperactivity disorder. In terms of age differences, children were more commonly diagnosed with hyperkinetic and pervasive developmental disorders, while adolescents were often diagnosed with depressive disorder.
There is a need for detailed analysis of follow-ups in the referrals, and a longer duration of study with a longitudinal design over a period of time would help us learn more about the attitudes of parents regarding help-seeking behavior and their knowledge about behavioral manifestations in children.
Limitations
The number of patients in the CGC during 2020 and 2021 was reduced due to the COVID lockdown.
Copyright Declaration
The authors declare that the manuscript, to the best of the author’s knowledge, does not infringe upon any copyright or property right of any third party.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was approved by the Institutional Review Board of MGIMS Sevagram (Approval Number: MGIMS/IEC/PSY/309/2023). Necessary ethical clearances and informed consent were received and obtained respectively before initiating the study from all participants.