
Abstract
Background:
There is a significant body of evidence on the various psychosocial and psychiatric correlates of juvenile offending. However, few Indian studies shed light on which mental health correlates are the most concerning compared to the general population. This study examined several risk factors for juvenile offending including attention-deficit hyperactivity disorder, aggression, self-esteem, non-suicidal self-injury, relations with family, childhood trauma, learning difficulties, and substance use in comparison with age, sex, and socioeconomic-status-matched community-based controls.
Method:
The study was conducted at a juvenile detention center and government-run school in Mumbai, India. Participants aged 13-17 years (n = 158, 79 each in case and control groups) were evaluated using a structured, self-reported questionnaire consisting of the Conners-3-self-report (short form), Rosenberg self-esteem scale (RSES), and questions on self-harm, substance use, and childhood physical and sexual abuse. Data were analyzed using SPSS version 20.0.
Results:
Adolescent offenders reported significantly higher rates of non-suicidal self-injury (58.2% compared to 12.6% in the control group; P < .001), substance use (57.0% compared to 10.1%; P < .001), childhood physical abuse (48.1% compared to 16.5%; P < .001) and learning difficulties (51.9% compared to 26.6%; P = .002) and scored lower on the RSES (P < .001). Attention-deficit hyperactivity disorder (P = .184) and aggression (P = .164) were not statistically significant. On regression analyses, self-esteem (adjusted odds ratio [aOR] = 0.73; P < .001), non-suicidal self-injury (NSSI) (aOR = 4.07; P = .017), and substance use (aOR = 3.88; P = .022) emerged as significant predictors of juvenile offending.
Conclusion:
Further research, screening, and targeted interventions are needed to mitigate adverse psychiatric and psychosocial outcomes among adolescent offenders.
Keywords
Introduction
In 2022, the National Crime Records Bureau (NCRB) in India reported a juvenile crime rate of 6.9% Maharashtra recorded a crime rate of 12.2%, and the highest crime rate of 42.3% was reported in New Delhi. 1 Studies have found that children from lower socioeconomic backgrounds, 2 living in single-parent households 3 or whose parents work for long periods away from home, are at a higher risk for conflict with the law.4,5 Childhood behavioral disorders like attention-deficit hyperactivity disorder (ADHD), oppositional defiant disorder (ODD) and conduct disorder (CD) are thought to mediate juvenile offending through elevated arousal, risk-taking behavior, derisive attitudes toward authority, and difficulty showing empathy and regard for the rights of others. 6 A study from India found that 59.4% of children in a juvenile home in New Delhi had symptoms of ADHD and related disorders. 7 Another major concern among children in conflict with the law (CICL) is substance use, which is found to significantly predict first-time offending, recidivism, as well as behavioral issues like ADHD and aggression. 8 Many biological and psychosocial factors are thought to be significantly associated with conflict with the law as a minor.
In India, the Juvenile Justice (Care and Protection of Children) Act (2015) recognized the importance of psychosocial factors in juvenile offending and encouraged the involvement of mental health professionals (MHPs) in the system. 9 Despite this, there is a paucity of mental health services for CICL and a need for further research on the mental health concerns of CICL to inform the rational allocation of the nation’s resources.
Literature from around the world and our clinical practice indicate that internalizing, externalizing, and cognitive domains all play a role in aggravating psychological distress among juvenile offenders, but these have not been comprehensively studied in India. Potential risk factors among CICL outside of ADHD, ODD, CD, and substance use include cognitive problems, learning disabilities, low self-esteem, non-suicidal self-injury, adverse relations with family, and traumatic experiences like childhood physical, emotional, or sexual abuse. Few studies controlled for age, sex, and socioeconomic status or elucidated mental health correlates of heightened concern needing the most urgent attention from a juvenile justice perspective.
Hence, the aim of this study was to examine mental health risk factors like ADHD, substance use, and aggression among juvenile offenders through a case–control design. Additionally, an attempt was made to study potential risk factors previously not studied in Indian CICL including learning difficulties, self-esteem, non-suicidal self-injury, relations with family, and childhood physical and sexual abuse.
Materials and Methods
Research Design
This study was formulated as an observational, questionnaire-based, case–control study designed to assess mental health risk factors that may be present among CICL in excess over age and sex-matched controls, namely community-based children at a civic-run school in a lower-income neighborhood in Sewree, Mumbai, with no history of conflict with the law.
Sample Size
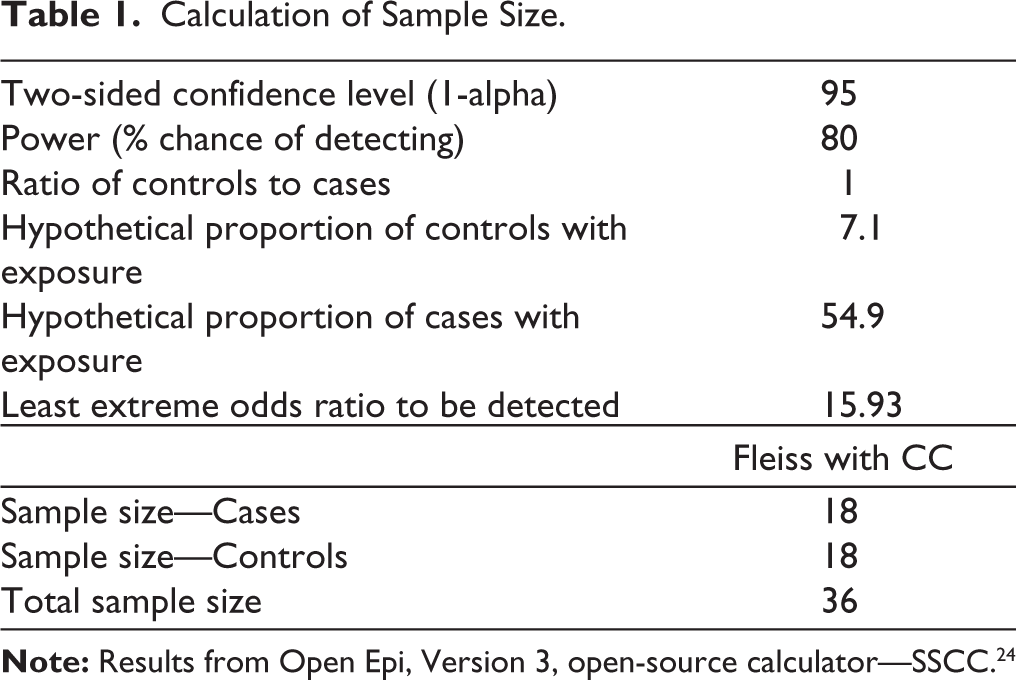
The pooled prevalence of ADHD among children and adolescents in India has been estimated at 7.1%. 10 Using a formula for case–control study designs 11 and a previous study 7 that estimated the prevalence of ADHD and related disorders at 54.9% among CICL in India, the sample size for this study (Table 1) was calculated to be 36. However, since resources existed in sufficient quantity and the total population of CICL housed at the study site during the study duration was 79, we enrolled all 79 children for the case group. This was subsequently matched with an equal number of age and sex-matched, community-based non-CICL controls.
Calculation of Sample Size.
Sampling was done by complete enumeration method for cases and simple random sampling using a random number table juvenile justice for controls.
Inclusion and Exclusion Criteria
CICL living in the Dongri Observation Home, Mumbai during the study period, and students at a randomly selected Municipal Corporation of Greater Mumbai (MCGM) operated secondary school in Sewree, Mumbai, willing to engage in an in-person interview, were included in the study. Detainees over the age of 18 or under the age of 12 years at the time of the interview, as well as those having a physical or intellectual disability precluding them from participating, were excluded from the study. Additionally, juvenile offenders also categorized as Children under the Protection of the Law 9 as per the Juvenile Justice Act (2015) and children from the control group with a history of conflict with the law were excluded.
Study Procedure
The study was commenced after approval from the Institutional Ethics Committee, concerned authorities at the Dongri Observation Home, and the Education officer overseeing a randomly selected Municipal school in Sewree, Mumbai. Participants were approached at the Dongri Observation Home, Mumbai, and at a municipal school. Following screening for eligibility, informed consent procedures were initiated. For the CICL group, the observation home superintendent was designated as the surrogate legally authorized representative (LAR). For the control group, parents of eligible students were invited to the school premises at a designated date and time to introduce the study and invite participation.
The informed consent document was administered to the parent/guardian/LAR in the language best understandable to them (English, or Hindi or Marathi). No interpreter was required as all investigators were fluent in the three languages. Time was allotted to ask questions. For all consenting participants, written assent was administered to the participating child. Subsequently, participants were engaged in an in-person, questionnaire-based assessment of 20-30 minutes duration. The interviews were conducted in a quiet room with relative privacy and minimum disturbance. Appropriate coronavirus disease 2019 (COVID-19)-related precautions were followed during recruitment and data collection. Interviews were conducted over a 45-day duration from September to October 2022.
Study Instruments
Conners 3 Self-report (Short Form)
The Conners 3 self-report (short form) is a validated questionnaire to assess five domains of ADHD (inattention and hyperactivity), aggression, learning difficulties, and family relations, among children aged 6-18 years. 12 It consists of 39 items, each scored on a 4-point Likert scale from 0 to 3. Participants were considered to exhibit elevated concern for each individual domain using t-score cutoff of 67. The psychometric properties of this scale are adequate 9 with a Cronbach’s α ranging from 0.63 to 0.79. The Conners 3 self-report (short form) was permitted for use in this study through our institution.
Rosenberg Self-esteem Scale
The Rosenberg Self-esteem Scale (RSES) was used as a self-report measure for self-esteem. It consists of 10 items rated on a 4-point Likert scale from 1 to 4. Score range was taken as 4 to 40. The scale can be used in individuals aged 12 years and older and has excellent psychometric properties and wide acceptability. 13 The RSES is freely available in the public domain.
Substance use screening was carried out in brief through semi-structured interviews by medical student data collectors. Type of substance, 14 onset, amount, frequency, and last use were assessed. Substance use was considered significant if the child had used a substance in the past month at a frequency of once a week or more. 15
Additionally, data regarding non-suicidal self-injury (NSSI) and physical and sexual abuse were recorded using screening questions adapted from the deliberate self-harm inventory, 16 self-harm inventory, 17 and sexual and physical abuse questionnaire. 18 Questionnaire translations into Hindi and Marathi were done based on the Translation, Review, Adjudication, Pretest, and Documentation (TRAPD) method for fluency and cross-cultural appropriateness. 19 This involved separate forward translation by two noninvestigator expert faculty members in the department of psychiatry who were fluent in the three languages, piloting in lay individuals in the community, iterative adjudication by an independent expert faculty and back-translation and synthesis.
Data Analysis
Data were compiled in Microsoft Excel 2019, and subsequently fed into SPSS version 20.0 for statistical analysis. Frequencies and descriptive statistics were used to express data in the form of mean ±SD (standard deviation), median [interquartile ranges (IQR)], frequencies, and percentages. Regression analyses were performed using backward elimination, at P < .05 level of significance.
Results
This study had a total sample of 158 consisting of 79 adolescents from the juvenile offenders group and 79 controls. The sample consisted entirely of male adolescents aged 14-17 years, with a median age of 17 years (IQR: 16-17 years). Controls had the same age-sex composition by reason of 1:1 matching.
Table 2 displays the descriptive statistics of the total sample as well as bivariate analyses to observe significant differences between the cases and controls. The total sample had an ADHD prevalence of 15.19%. 18.99% (15/79) of cases had elevated concern for ADHD compared to only 11.39% (9/79) among controls. However, on chi-squared testing, the difference was not statistically significant (P = .187).
Descriptive Statistics of the Total Sample and Comparison Between CICL and Non-CICL Groups.
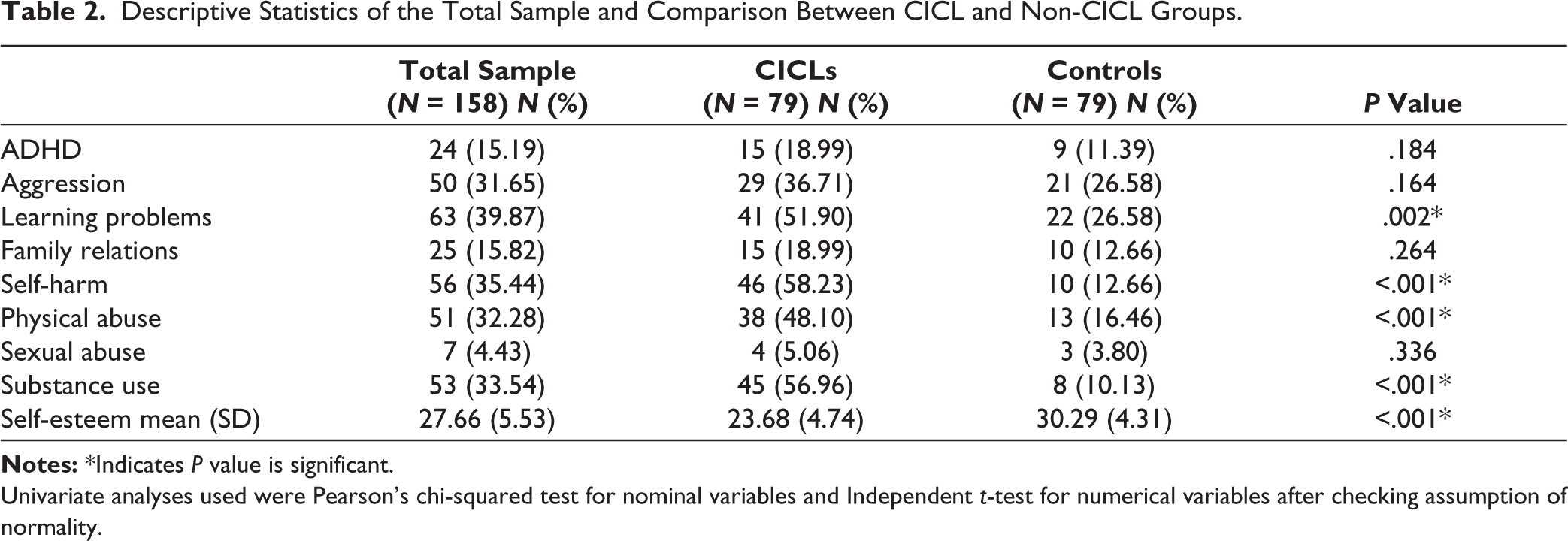
Univariate analyses used were Pearson’s chi-squared test for nominal variables and Independent t-test for numerical variables after checking assumption of normality.
The total sample had a high prevalence of aggression (31.65%), poor family relations (15.82%) and learning difficulties (40%). On chi-squared analysis, the prevalence of learning difficulties was significantly higher in CICL, with 51.90% of juvenile offenders reporting difficulties with either learning, mathematics, or language comprehension, compared to 26.58% controls (P = .002). Substance use was present in 33.54% of the total sample, with stark differences between cases and controls; 56.96% in CICL compared to only 10.13% in controls (P < .001).
The mean score on the RSES of the total sample was found to be 27.66 ± 5.53 (mean ± standard deviation). On independent sample t-test, average self-esteem scores were found to be almost seven points lower among juvenile offenders at 23.68 ± 4.74 (P < .001). There was an alarming prevalence of self-harm in the total sample (35.44%) with significant differences between cases and controls; 58.23% among CICL compared to only 12.66% among controls (P < .001). Similarly, about 50% of the cases reported a history of physical abuse including corporal punishment at home or abuse by peers, compared to 16.46% in the control group (P < .001).
Binary logistic regression analyses were performed via backward elimination method to arrive at a regression model with the maximum goodness of fit (adjusted R 2 = 0.648) for significant predictors of juvenile offending (Table 3). Self-esteem emerged as a significant negative predictor with an adjusted odds ratio (aOR) of 0.73 (95% confidence interval 0.65-0.82, P < .001). Self-harm and substance use emerged as significant positive predictors of juvenile offending (aOR = 4.07, P = .017, aOR = 3.88, P = .022, respectively).
Binary Regression Analysis for Juvenile Delinquency.
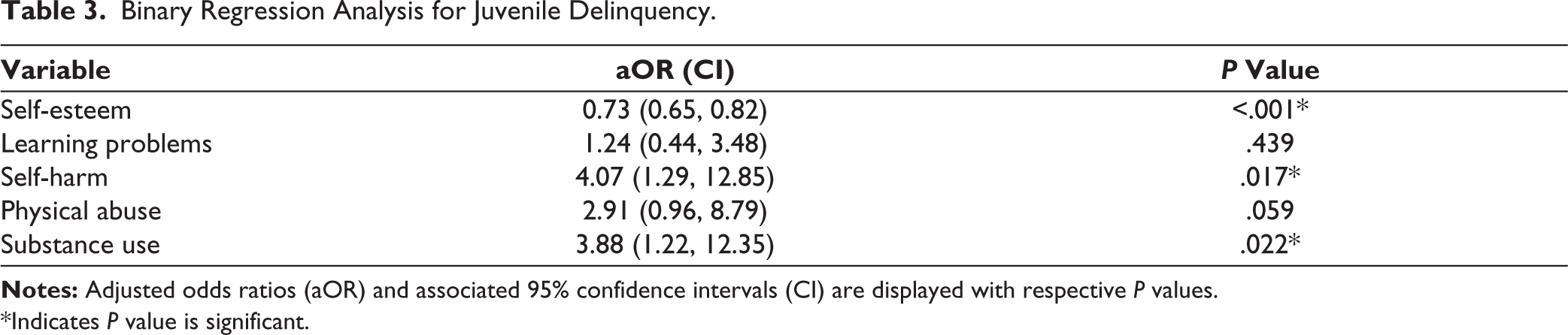
*Indicates P value is significant.
Discussion
The present case-control analysis yielded a number of insights regarding the mental health of juvenile offenders in India. The CICL sample was entirely composed of male offenders. This may be explained by the fact that only 0.46% of juvenile offences in India in 2022 were committed by females. 1
About a fifth of the adolescent offenders (18.99%) were found to have concern for ADHD. These findings are much lower than the 59.4% prevalence 7 reported in a previous Indian study from 2013 but are comparable to the 17.3% prevalence reported among adolescent offenders in a meta-analysis in 2020. 20 Therefore, the present estimates, though lower than previous research from India, 7 do point toward ADHD being an area of concern in the Indian CICL population and a direction of future research.
Although concern for ADHD was numerically elevated among juvenile offenders (18.99%) compared to controls (11.39%), the difference was not statistically significant. This is in conflict with previous literature6,20,21; multiple studies have reported that ADHD predicts juvenile offending, violent offences, and recidivism. In an analysis of the Pathways to Desistance database, Wojciechowski 21 found baseline ADHD to be a strong predictor of multiple patterns of recurrent violent offence among juveniles controlling for gender, race, and socioeconomic status. Similarly, although CICL were observed with numerically higher levels of aggression (36.71%) compared to controls (26.58%), the difference was not statistically significant. In a previous study by Gupta et al., 2 there was a significantly higher prevalence of aggression among CICL compared to community-based controls. Hence, the present study’s results warrant further evaluation with a larger sample size and increased statistical power.
While there is a strong neurodevelopmental basis for the relationship between ADHD, aggression, and juvenile offending rooted in poor cognitive, emotional, and impulse control, 22 environmental factors like parenting styles, childhood trauma and socioeconomic background do moderate these effects. 23 Additionally, it has been observed that the association between ADHD, ODD and/or CD, and juvenile offending strengthens with severity of offence 23 from no significant associations seen in mild offences [X2 (8) = 6.55, P = .59] to strong associations in severe offences [X2 (5) = 37.35, P < .01]. This points toward a need for further data on externalizing risk factors to be analyzed in the context of severity of offence as well as environmental influences.
In this study, more than half the CICL sample reported learning difficulties, including problems with reading, comprehension, and mathematical reasoning, at a rate twice as high as the control group. This finding is in line with previous research24,25 linking juvenile offending with problems in global cognitive functioning and learning difficulties. Learning difficulties are more likely to go uncorrected through remedial teaching and rehabilitation among detained youth. The resulting impairment in education and job opportunities may mediate poor socioeconomic and life outcomes. 26 There are no data in the Indian context on the relationship between cognitive issues, learning difficulties and juvenile offending.
CICL reported significantly lower self-esteem than controls. Low self-esteem has been linked to juvenile offending in multiple previous studies.6,27 We also found non-suicidal self-injury to be a significant predictor of juvenile offending. 28 NSSI is known to be driven by emotional dysregulation and serves as a coping mechanism in response to stress. 29 Given the relationships between deliberate self-harm, anxiety, depression, and suicidality, 30 the elevated prevalence of NSSI and low self-esteem found among CICL is concerning and warrants further inquiry. No Indian data exist on self-harm and its significance among juvenile offenders. A previous study from the United States 31 showed that self-harm among justice-involved youth was associated with female gender, bisexual orientation, and post-traumatic stress. Previous research also showed that 87.6% of adolescents with NSSI meet criteria for a psychiatric disorder and 67.3% meet criteria for a personality disorder. 32
Substance use emerged as a significant predictor of juvenile offending, a finding that corroborates with previous literature. 33 Being a structured and regulated environment, juvenile detention centers could be potential service points for deaddiction. Further research is needed to understand the relationship between juvenile offending, substance use, dependence, and whether substance use serves as a gateway into recidivism and more serious offences.
Adolescent offenders were likelier than controls to report that they had faced physical abuse at home or due to peers in their childhood, but this association lost statistical significance on regression analyses. Nevertheless, this study supports the need for further research in this domain. Previous evidence 34 points toward screening for adverse childhood experiences (ACE) in at-risk children and the need to address trauma in the mental health rehabilitation of juvenile offenders.
The limitations of this study include a small sample size from a single center and a lack of more in-depth assessment of some of the psychosocial risk factors including substance use and NSSI. We also could not assess detailed sociodemographics due to CICL confidentiality concerns expressed by the observation home authorities. Larger, multicentric studies are needed to further assess externalizing, internalizing, cognitive, and environmental factors over a longer duration and gather more generalizable data, as well as prospective studies to understand the recidivism, socioeconomic, and mental health outcomes of at-risk adolescents. This study did not utilize full-length questionnaires for NSSI, physical and sexual abuse and substance use and instead relied on broader screening questions, which may have resulted in higher prevalence rates. These should be confirmed with larger prevalence studies. Based on our study’s findings, the association between NSSI and juvenile offending should be further examined along with an assessment of psychopathology including suicide, personality disorders, and substance use disorders.
Conclusion
This study found a high burden of mental health concerns among CICL. Substance use, non-suicidal self-injury, and self-esteem were found to be significantly elevated among CICL compared to community-based controls. Learning problems were associated with conflict with the law on bivariate analyses but only approached significance after controlling for other factors. The association between juvenile offending and well-known risk factors like ADHD and aggression was not established, warranting further research using a larger study sample.
Implications and Practical Applications
This study adds to our current understanding of risk factors that determine juvenile offending in the Indian context, and paves the way for further research across externalizing, internalizing, and cognitive domains. Based on the findings of this study, several domains including internalizing problems like non-suicidal self-injury and self-esteem and cognitive problems like learning disabilities may be key areas of concern and should be further researched. Higher-level evidence is needed to drive the rational allocation of behavioral, social work, occupational, and other resources to address the mental health needs of CICL through a comprehensive, rehabilitative approach.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was awarded financial support through the Indian Council of Medical Research Short-term studentship (ICMR-STS) program of 2022.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Institutional Ethics Committee-III (No. EC/OA-08/2022 dated 29.08.2022). Written Informed Consent was taken from parents/guardians/Legally Authorized Representative (LAR) as applicable. Written Informed assent was taken from all participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.