
Abstract
Introduction:
Impairments in hand coordination and fine motor skills are common among children and adolescents with attention deficit hyperactivity disorder (ADHD), particularly when faced with complex and speedy tasks. The assessment of hand coordination and performance difficulties in adolescents with ADHD compared to healthy children is poorly understood.
This study aimed to assess the level of hand coordination and performance difficulty of adolescents with ADHD in comparison with healthy controls.
Material and Methods:
This case-control study included 60 adolescents (30 with ADHD in the case group and 30 healthy individuals in the control group) recruited from patients attending specialized psychiatric clinics in Tabriz, Iran, in 2021. The Conner’s Parent Rating Scale-Revised (CPRS-R) questionnaire and semi-structured diagnostic interview (PL SADS-K) were used to diagnose ADHD. The Vienna Test System (VTS) was utilized to evaluate hand coordination performance. The study groups were compared regarding hand coordination, duration, difficulty level, and error rate.
Results:
No statistically significant differences were found in the mean age of the participants, the age of their parents, or any other demographic or baseline variables between the two groups (P > .05). The difference between the mean times of hand coordination in the case group (31.4) and the healthy group (29.4) was not statistically significant (P > .05). However, the case group exhibited a considerably higher mean and level of performance error than the control group (3.48 vs. 1.77), which was statistically significant (P = .007). In terms of coordination difficulty, no statistically significant difference was found between the two groups (2.4 vs. 2.29).
Conclusion:
Findings showed no significant statistical differences between the two groups regarding the duration and difficulty of hand coordination tasks. However, the error duration was higher in adolescents with ADHD than in healthy adolescents. Results suggest the potential presence of errors in the hand coordination task among adolescents with ADHD.
Keywords
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by hyperactivity, inattention, and impulsivity, typically onset before the age of 12. 1 The global prevalence of ADHD is approximately 5%–10% in children and adolescents, which has increased compared to the past decade. Recent estimates indicate that approximately 57% of diagnosed cases continue into adulthood.1,2 The importance of this diagnosis is evident in the decreased life expectancy, comorbidity with other psychiatric disorders, drug use, and diminished quality of life for affected individuals and their families.3,4
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, children diagnosed with ADHD must exhibit at least 6 out of 9 symptoms from each category of inattention and/or hyperactivity-impulsivity. Each child with an ADHD diagnosis may manifest symptoms of inattention, hyperactivity, impulsivity, or a combination thereof. Primary symptoms of inattention include distractibility, forgetfulness, organizational skill deficits, and a lack of stability in tasks. On the other hand, hyperactivity-impulsivity is more associated with boredom with long-term rewards, difficulty in controlling untimely and inappropriate motor responses, and the inability to modulate motor activities appropriately for each relevant spatial situation. 5 Common comorbidities of this disorder include oppositional defiant disorder (ODD), conduct disorders, mood disorders, anxiety disorders, tic disorders, autism spectrum disorder, and various learning disabilities such as dyslexia. The connection between these symptoms and executive dysfunctions is significant, and studies have shown functional abnormalities in cognitive or executive function tests. 6
The primary executive functioning aspects identified include working memory, inhibitory control, and cognitive flexibility. Motor coordination deficits or impairments in motor functions are another common issue in ADHD children, which has not received much attention in research.7,8 Most children with ADHD have poor praxis motor skills, primarily associated with working memory. Clinical and epidemiological studies have reported that 30%–50% of children with ADHD suffer from motor coordination problems. 9 The variance in these percentages is attributed to differences in motor assessment tools, referral sources, and cutoff points. Motor coordination difficulties have long been acknowledged under several labels. Since 1994, they have been officially referred to as developmental coordination disorder (DCD), primarily characterized by impairments in the execution of motor skills. 10 These deficits negatively impact daily activities such as dressing, eating, cycling, and academic achievements through poor handwriting skills. However, this condition should not be due to medical conditions like cerebral palsy, and the diagnosis is only for children with an IQ above 70. The precise pathophysiological mechanism underlying the comorbidity of these two disorders is currently unclear. In ADHD, impaired functioning of the fronto-striatal cortical structures and reduced brain volume have been well documented. There is a decrease in dopamine activity and the noradrenergic system in ADHD. The imbalance in basal ganglia neural pathways induced by dopamine can justify motor coordination impairments in children with ADHD. It was previously assumed that motor problems in children were secondary to their attention deficits. However, subsequent studies have shown that motor deficits are distinct from attention deficits.11,12
Fliers et al. in the Netherlands (2008) concluded that there is a close relationship between ADHD and motor coordination problems, which may be the result of abnormal brain development. 9 Mokobane et al. (2019) discovered that fine motor skill deficiencies are prevalent in primary school-aged children with ADHD, particularly when they are required to complete complex and fast-paced tasks. 13
Considering the limited evidence on hand coordination in children with ADHD versus to healthy children, the primary aim of this study is to assess the duration and frequency of errors in hand coordination performance. The secondary objective is to assess the level of difficulty in hand coordination among adolescents with ADHD in comparison with controls.
Materials and Methods
Study Design and Population
A case-control study was conducted on adolescents aged 12–18 diagnosed with ADHD who visited psychiatric clinics affiliated with Tabriz University of Medical Sciences in 2021. Patients were randomly selected from child and adolescent psychiatric clinics affiliated with Tabriz University of Medical Sciences.
Study Groups
The case group consisted of children with confirmed ADHD who visited psychiatric clinics affiliated with Tabriz University of Medical Sciences. The control group was selected from family members of the patients and matched based on age and gender. In the group matching method, an equal relative frequency of age and gender was selected from both groups for the study.
Using G-Power software and by examining previous pilot assessments, considering the default mean difference of 4, within-group standard deviation of 4.7, equal sample sizes in both intervention and control groups, alpha of 0.05, and power of 0.9, a sample size of 30 individuals for each group and a total of 60 individuals was determined.
The study aimed to develop a continuous response outcome (scale) from independent controls and cases, with one control(s) per case. In a previous study, each subject group’s responses were normally distributed with a standard deviation of 4.7. Suppose the actual difference between the experimental and control means is 4. In that case, 30 experimental and 30 control subjects will need to be studied in order to reject the null hypothesis with a probability power of 0.9.
Inclusion and Exclusion Criteria
The inclusion criteria comprised consent to participate, an age range of 12 and 18 years, a preliminary diagnosis of ADHD, and specifically having combined type ADHD. Participants who were diagnosed with severe or very severe untreatable diseases or disorders such as severe vision or hearing impairment, psychosis, or a history of disorders (as members of welfare centers and support organizations) were excluded from the study. Other exclusion criteria were comorbid psychiatric conditions such as anxiety disorders, intellectual disabilities, communication disorders, autistic spectrum disorder, and mood disorders, as well as comorbidity with physical illnesses such as thyroid dysfunction, physical disabilities, and adrenal gland disorders.
Measurements
ADHD was diagnosed using the Conner’s Parent Rating Scale-Revised (CPRS-R) 14 questionnaire and the semi-structured diagnostic interview - Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (SADS-K).
The CPRS-R developed by Conner et al. in 1998 consists of 27 items designed for 3-17-year-olds. This questionnaire is utilized to identify and measure the severity of ADHD symptoms. It comprises four scales:
Scale A: Oppositional Behavior (5 items) Scale B: Cognitive Problems/Inattention (5 items) Scale C: Hyperactivity (5 items) Scale D: ADHD Index (5 items)
Each item is scored on a four-point scale (0 = Never to 3 = Very often). Using a specific formula, the scores for each subscale are converted into a score ranging from zero to 100. Higher scores indicate a greater severity of the corresponding symptoms. Scores are adjusted for age and gender, and scores above 65 indicate the presence of ADHD disorder.
The construct validity of CPRS-R has been confirmed in Helton et al.’s study, and concurrent validity has been reported with Pearson correlation coefficients between 0.47 and 0.63 with scales of attention problems, delinquent problems, and aggressive problems related to the Child Behavior Checklist. 15 Its sensitivity and specificity are 0.69 and 0.67, respectively. CPRS-R is widely used in various Iranian studies.16,17 This study assessed reliability using Cronbach’s alpha coefficient for each subscale, which ranged from 0.69 to 0.81.
The Semi-structured Diagnostic Interview: SADS-K
This questionnaire is a semi-structured diagnostic interview based on IV-DSM criteria and is conducted as an interview with a psychiatrist with both parents and the child. The SADS-K-PL can effectively diagnose psychiatric disorders. In Iran, Ghani Zadeh et al. 18 reported the reliability of the Persian version of the SADS-K-PL using the test-retest method as 0.81 and inter-rater reliability as 0.69. In this study, the SADS-K-PL was used to diagnose ADHD as well as other psychiatric disorders. This study evaluated all diagnoses of comorbid psychiatric disorders over the past six months.
The Vienna Test System (VTS) for Assessing Performance in Hand Coordination
The VTS is one of the earliest computerized psychological, neurological, transportation, and sports assessment tools. The VTS covers a wide range of new tests and has flexible methods that can be adapted to the requirements of various assessment conditions. This device includes response and control panels to measure reaction speed, stress resilience, and sensorimotor coordination. It also includes optical sensors and other auxiliary tools for specific tests. The VTS provides four test systems for HR, neurological, transportation, and sports. Each VTS test includes dimension lists and tests tailored for specific domains. They also include multiple test sets for examining complex and specialized issues. In this study, the bilateral coordination test was used, which consists of four tasks of moving a small circle along the path of a cylinder without deviating from it; any deviation from the path is considered an error. The duration and number of errors determine the individual’s performance. The reliability and validity of this tool have been confirmed by its developers and used in various studies. 19
Analysis
For data analysis, SPSS (version 21.0, Chicago, IL, USA) software was utilized. Descriptive statistics were used to describe the distribution of data by study groups. The independent t-test (if the data were normally distributed) and the Mann–Whitney U test (if the data were non-normally distributed) were carried out to compare quantitative variables. The chi-square test was utilized to compare binary and categorized variables. In cases where the expected frequency in at least 80% of the cells in the table was less than 5, Fisher’s exact test was used. 20 A significance level of less than 5% was considered for all tests.
Results
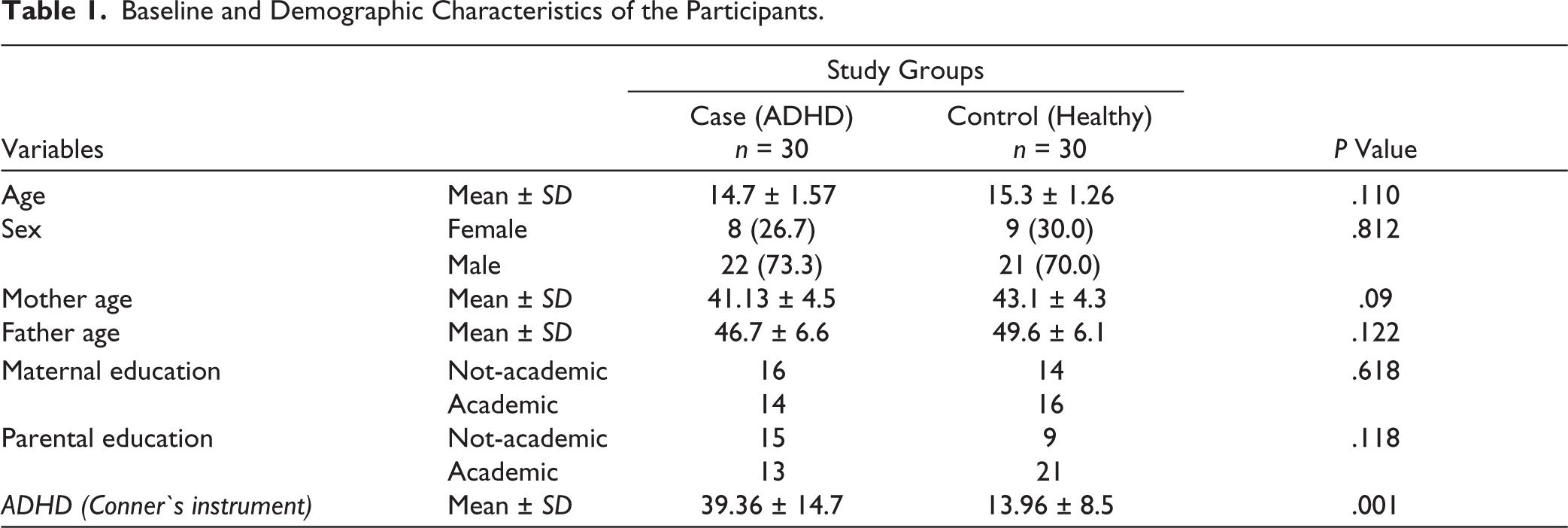
In total, 60 participants, including 30 adolescents diagnosed with ADHD and 30 healthy adolescents, were compared regarding hand coordination performance assessment. The minimum and maximum ages of participants in both groups were 12 and 18 years, respectively. The mean age of participants in the experimental group was 14.7, while in the control group, it was 15.3. The mean age of participants’ parents and other demographic and baseline variables by study groups is presented in Table 1. There was no statistically significant difference in participants’ age, parental age, parental education, or other demographic variables between the two groups (P > .05). As expected, the mean score of the CPRS-R in the group of adolescents with ADHD was significantly higher than in the healthy group (P = .001). Mean score of motor coordination of hands between ADHD and healthy adolescents regarding overall time, error, and difficulty is shown in Figure 1.
Baseline and Demographic Characteristics of the Participants.
Comparison of Mean Score of Motor Coordination of Hands Between ADHD and Healthy Adolescences.
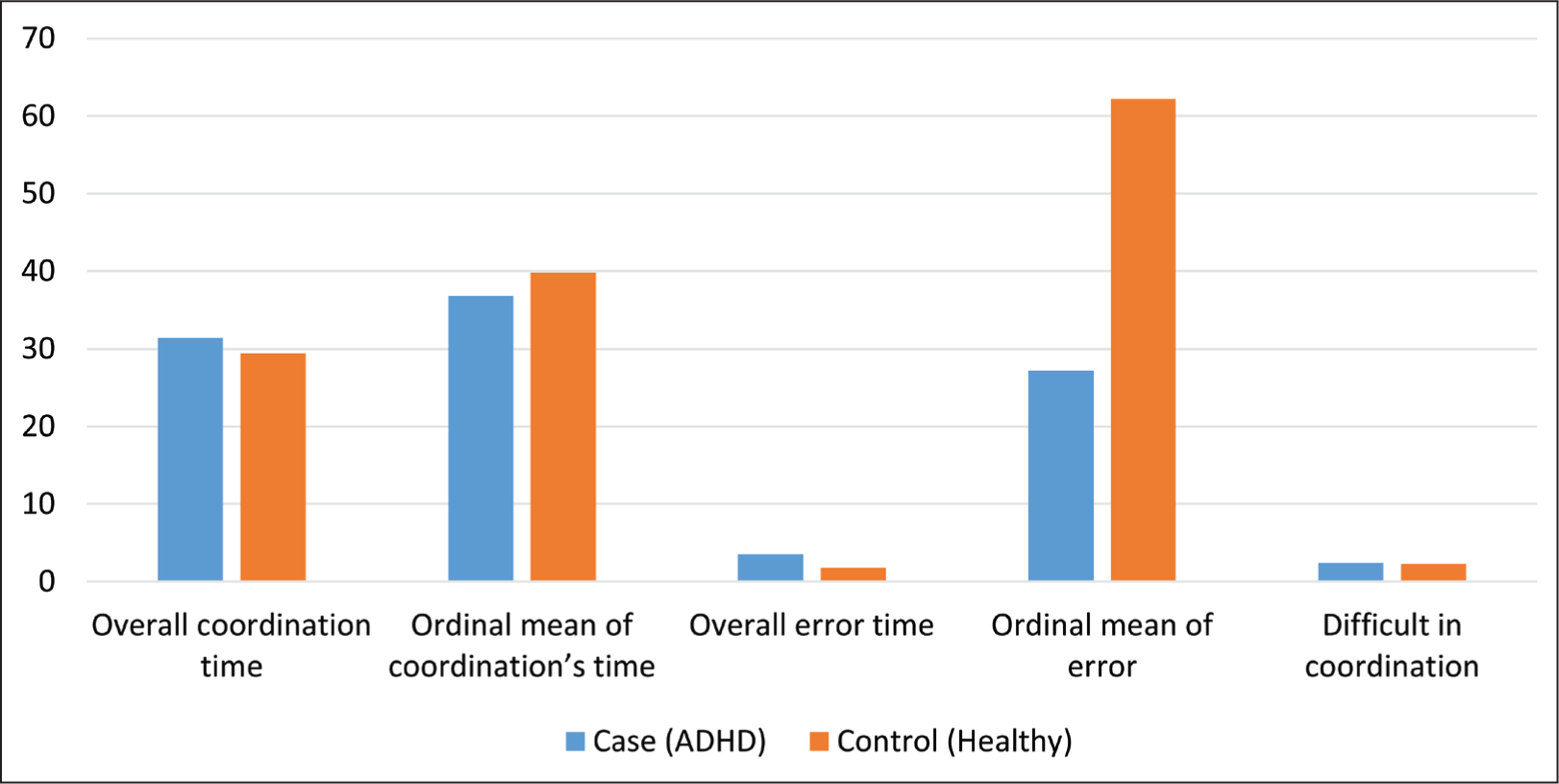
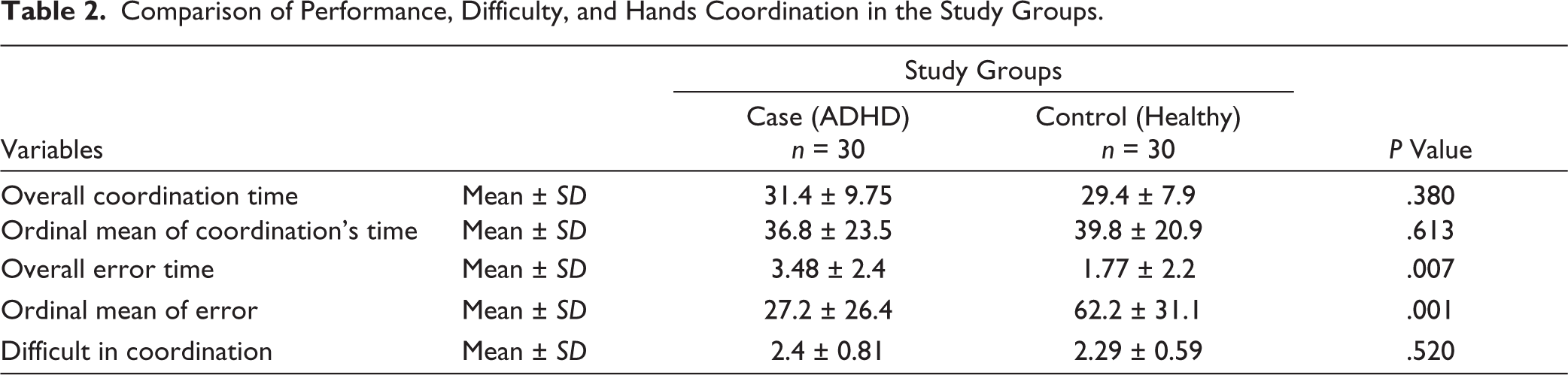
Table 2 displays the coordination, errors, and difficulty level in hand coordination tasks between adolescents with ADHD and healthy adolescents. The mean coordination time of hands in the case group was 31.4, while in the control group, it was 29.4; however, this difference was not statistically significant (P = .380). However, the case group’s mean error rate and level of errors were significantly higher than those of the control group (3.48 vs. 1.77), which was statistically significant in terms of mean numerals and mean levels (P = .007). Regarding the difficulty of coordination, no significant difference was found between the two groups (P = .520). However, the difficulty score in the experimental group was slightly higher than the control group (2.4 vs. 2.29).
Comparison of Performance, Difficulty, and Hands Coordination in the Study Groups.
Discussion
The study compared the level and difficulty of hand coordination between adolescents with ADHD and the control group. We found that adolescents with ADHD exhibited a longer duration of errors in hand coordination tasks. However, it was shown that the average time for hand coordination in adolescents with ADHD and the control group did not significantly differ.
Concerning the difficulty level of hand coordination, no significant difference was found between the study groups. Overall, the number of errors and the duration of performance errors observed in hand coordination tasks contribute to a decline in performance among adolescents with ADHD. However, in terms of total task completion time and task difficulty, no differences were found between adolescents with ADHD and their healthy counterparts. Therefore, the findings of the present study revealed differences in both the number and duration of performance errors.
These findings are consistent with the research conducted by Miklos et al., 21 which reported poor executive functions in children and adolescents with ADHD. Additionally, a meta-analysis reported that children with ADHD have less accuracy in coordinating movements within the phase and significantly less speed and coordination for movements outside the phase. 22 Another study has also reported that children with ADHD have weaker motor skills compared to control children. 23
Furthermore, Tehrani-Doost et al. showed that executive functions in children with ADHD, compared to healthy children, exhibit degrees of impairment, especially evident in inhibitory control.16,17 Tehrani-Doost reported that commission errors in children with ADHD were significantly higher than in the control group. Although previous studies emphasize the existence of motor problems in children with ADHD, the findings of this study highlight the presence of multiple motor errors in individuals with ADHD, with no significant differences observed in task difficulty or task completion time compared to control individuals. However, prior research24,25 has shown that one-third of children with ADHD struggle with motor coordination, whether they are male or female. Another report also showed that women without ADHD performed better in set-making tasks. However, our research findings did not align with Shen’s findings regarding task completion time. 26 The criteria for assessing abilities and motor coordination in Shen’s study may contribute to discrepancies in findings. They evaluated manual dexterity abilities as a component of motor coordination performance. In contrast, in our study, hand coordination was assessed as a task of passing through a cylindrical maze.
Krenzki et al. examined children with ADHD in Canada and concluded that the performance of these children in simple motor skills was normal. Although both groups had difficulties in sequential one-handed or two-handed motor skills that could be improved with practice to a normal level, the percentage of errors in the ADHD group was higher. 27 In the United States, Silverstein et al. evaluated executive function deficits in children with ADHD and concluded that ADHD symptoms are strongly associated with executive function deficits. 8 Additionally, others Iranian studies indicated that the ADHD group showed significant differences in balance with eyes closed, bilateral motor coordination, movement accuracy, and hand movement speed compared to the normal group.28-30
Conclusions
The current study’s findings indicate that the duration of performing the dual-hand coordination task and the task’s difficulty do not show statistically significant differences between the two groups of adolescents: those with ADHD and controls. However, the error duration in adolescents with ADHD is greater than in healthy adolescents. This finding supports the probable presence of various errors in the dual-hand coordination task among adolescents with ADHD. This finding can be practically utilized for planning interventions aimed at reducing errors in adolescents with ADHD.
Footnotes
Acknowledgements
This study is derived from the thesis of Dr. Zahra Mohammadi Bina, a psychiatry resident. We thank the statistical and epidemiological supports of the “Clinical Research Development Unit of Al-zahra” Educational, Research, and Treatment Center, Tabriz University of Medical Sciences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee Tabriz University of Medical Sciences, with reference number IR.TBZMED.REC.1400.793 and dated November 15, 2021. The study was carried out/not carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tabriz University of Medical Sciences.
Patient Consent
Written informed consent was taken from all the participants. Participants also provided verbal informed assent and consent (wherever applicable).