
Abstract
Introduction:
Functional constipation (FC) is a common pediatric problem which has the propensity to affect the quality of life of the child and the family. This study aimed to assess the health-related quality of life (HRQoL) in children with FC and its impact on families as compared with healthy children.
Material and Methods:
This study enrolled children 2–12 years old along with their primary caregiver presenting to the Pediatric OPD of a tertiary care teaching hospital with complaints of constipation and were diagnosed as FC as per ROME-IV criteria. Age and gender matched controls were enrolled from healthy children attending OPD for routine check-up or minor ailment such as URI. Pediatric Quality of Life (PedQL 4.0) inventory developed by Varni et al. was used for assessment of Quality of Life in children and Family impact. It has three components—Generic core scale, Family impact module and gastrointestinal symptom module. Data was analyzed using SPSS-23.
Results:
The study enrolled 38 children with constipation and 34 controls along with their respective caregivers. There was no significant difference in age, gender distribution, family nature and type of toilet used between the two groups. Two-thirds of the cases were living in a joint family. The mean score in physical, emotional and social functioning were significantly lower among the cases compared to controls. The scores in different domains of family impact modules were not statistically different.
Conclusion:
Children with FC have significantly lower scores in physical, emotional and social domains of the Generic core scale of PedQL 4.0.
Introduction
Functional constipation (FC) is a common pediatric problem, which accounts for around 30% of the Pediatric gastroenterology referrals; 4%–5% of all the referrals to the pediatric gastroenterology tertiary care center and 0.8%–1% of all the pediatric cases. 1 FC is defined as per ROME IV criteria 2 and accounts for 85% of all the causes of constipation in children. 3 FC may cause significant impairment of the normal functioning of the child and will also affect the parents and family. Many studies have shown that health-related quality of life (HRQoL) is poorer among the children with FC and their families also have poorer HRQoL.4,5 Wang et al. reported that children with FC has significant lower score on physical, emotional, social and school function compared to healthy children. They also reported that the child’s age, duration of symptoms, child and caregiver relationship, family economic status and caregiver education had a significant impact on HRQoL of children, caregivers, and family. 6
In a meta-analysis of 13 studies done by Vriesman et al., HRQoL was found to be significantly lower in children with FC compared to the healthy children and the difference was similar for the children’s self-report and parent reporting for a child. 7 Another study in school age children found that HRQoL and sleep quality were significantly poor among children with FC. 8
Indian studies involving adults have reported poorer quality of life among those with chronic constipation.9,10 In addition, studies have also reported many psychological maladjustments and poorer HRQoL in adolescents with chronic constipation.11,12
There is a paucity of Pediatric data from India in this regard. In this study, we plan to evaluate the impact of FC on the quality of life of the child and the family.
Materials and Methods
This cross-sectional cohort study was conducted at the out-patient department of pediatrics at a tertiary care teaching hospital in North India over a period of six months.
Children 2–12 years who presented to OPD and were diagnosed with FC as per the ROME IV criteria and their primary caregiver were consecutively included as the case population. Age and gender matched healthy control children and their primary caregiver were included from the immunization clinic and OPD (children attending OPD for routine check-up or with minor ailments such as URI) and made the comparison group.
Children diagnosed with an organic cause for constipation, those with associated neurological conditions or chronic diseases which may affect the HRQoL were excluded from the study. Children of the parents who did not comprehend either Hindi nor the English language were also excluded.
After obtaining written informed consent from the parents/care taker, demographic data including age, gender, education of parents, child’s school grade; clinical data such as age of onset, duration of symptoms, presence or absence of incontinence or blood in stools, diet especially daily milk intake and treatment history were recorded on a pre-structured proforma. Children were investigated as clinically indicated. The study was approved by an institutional ethical committee.
Study Tool
Pediatric quality of life inventory (PedQL) 4.0 questionnaire developed by Varni et al. was used to assess HRQoL for this study. This questionnaire is a pediatric specific tool and has shown very good reliability in western studies across all age groups (Chronbach’s alpha 0.89–0.92).
13
This questionnaire has previously been used in many Indian studies, previously14,15 and has also been validated in the Indian population with substantial reliability (Cronbach alpha = 0.82, P < .00001) and fair validity.
16
It has three parts:
PedQL 4.0 Generic core scale: It is a 23-item questionnaire to assess the impact of the disease on various functional domains (physical, emotional, social and school function). Parent reporting for the child was used for all the children, and the mother or the primary caregiver will be asked to fill out the questionnaire. PedQL 4.0 Family impact module: This assesses the impact of the child’s disease on the functioning of the primary caregiver. It contains 36 items in eight functional domains (physical, emotional, social, communication, worry, daily activities, family relationship, and cognitive). This questionnaire was filled by the mother or the primary caregiver. PedQL 4.0 Gastrointestinal symptom module: To assess the severity of constipation. It is a 14-item assessment questionnaire for the symptoms of constipation. The questionnaire was filled by the mother or primary caregiver. All the questions are scaled from zero to four (zero = never; four = almost always).
Reverse scoring was done for the purpose of analysis (Zero =100, 1 = 75, 2 = 50, 3 = 25, 4 = 0).
Statistical Analysis
Data was analyzed by SPSS version 23. Data was presented as mean (SD) or median (IQR) for normally and non-normally distributed parameters. Chi square test was used to compare two categorical variables. Student t test or Mann Whitney U test were used to compare means of two groups based on normality of distribution of data for continuous variables. Pearson correlation coefficient was used to correlate two continuous variables.
Results
A total of 45 children visited the pediatric OPD for complaint of constipation during the study period. Seven children were excluded (four could not comprehend Hindi or English, two children with organic cause of constipation, for one child the primary caregiver was not available). A total of 38 children with constipation (Group A) and 34 controls (Group B) were enrolled. Demographic details of the two groups are compared in Table 1. There was no significant difference in the age and gender distribution of both groups. In the study group, median (Q1, Q3) age of onset of symptoms was 27.5 (17, 48.75) months, with median (Q1, Q3) duration of 12 (3.75, 21) months. The majority of mothers were home-makers in both groups. Stool frequency per week ranged from 1 to 5 per week. Most common associated symptoms of constipation were retentive posturing seen in 21 (55.3%) children followed by abdominal pain in 18 (47.3%) and bleeding per rectum in 11 (28.9%). Twelve (31.6%) children had anemia and in 15 (39.5%) fecaliths could be palpated; none of them had features of hypothyroidism. There was no significant difference in the daily average milk intake between the two groups (P = .27). Proportion of children taking at least one serving of fruits was not significantly different between the two groups (P = .058), although a significantly lower proportion of children with constipation were eating at least one serving of vegetables per day (P = .03).
Comparison of the Demographic Characteristics of Cases and Control Groups.
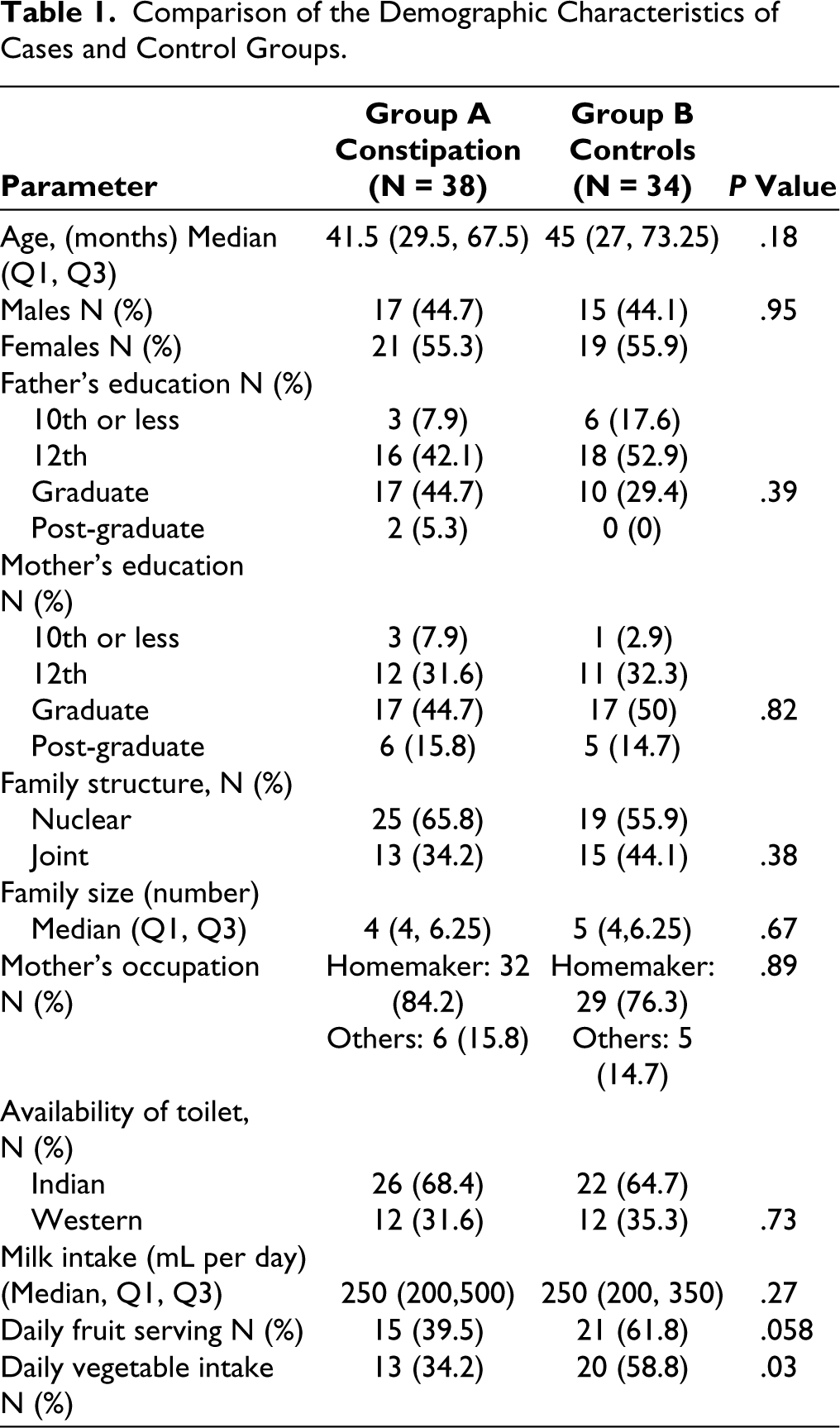
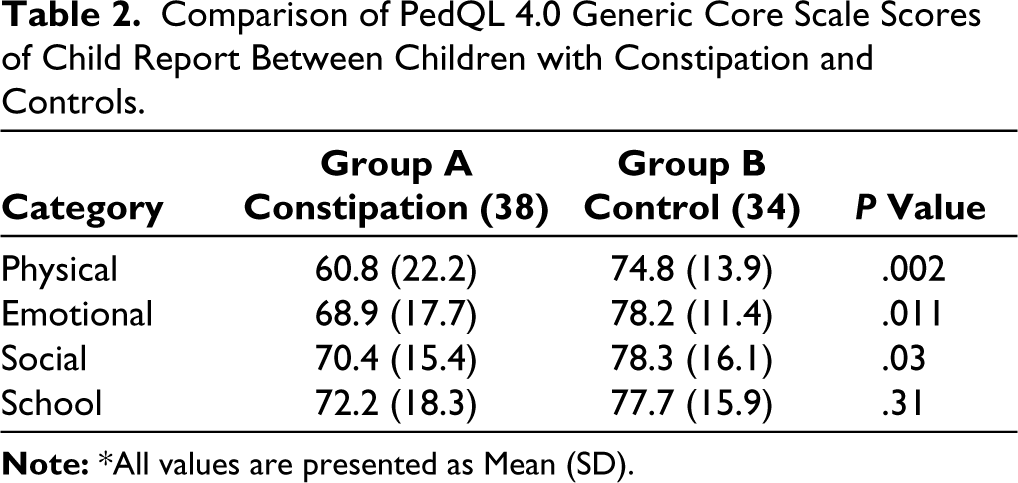
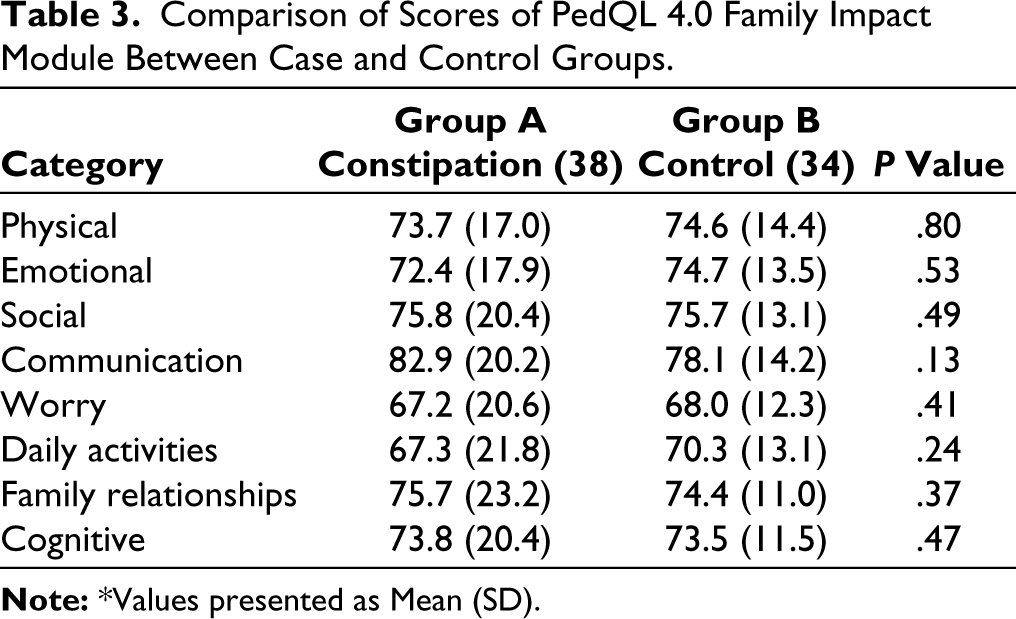
Table 2 shows mean (SD) scores of the various domains of child report. The scores in physical, emotional, and social domains were significantly low in children with FC. Table 3 shows mean (SD) scores of PedQL 4.0 family impact module. There was no significant difference between cases and control groups. In the constipation group, there was no significant correlation between constipation scores and various domains of child report and family impact report (P > .05 for all the comparisons).
Comparison of PedQL 4.0 Generic Core Scale Scores of Child Report Between Children with Constipation and Controls.
Comparison of Scores of PedQL 4.0 Family Impact Module Between Case and Control Groups.
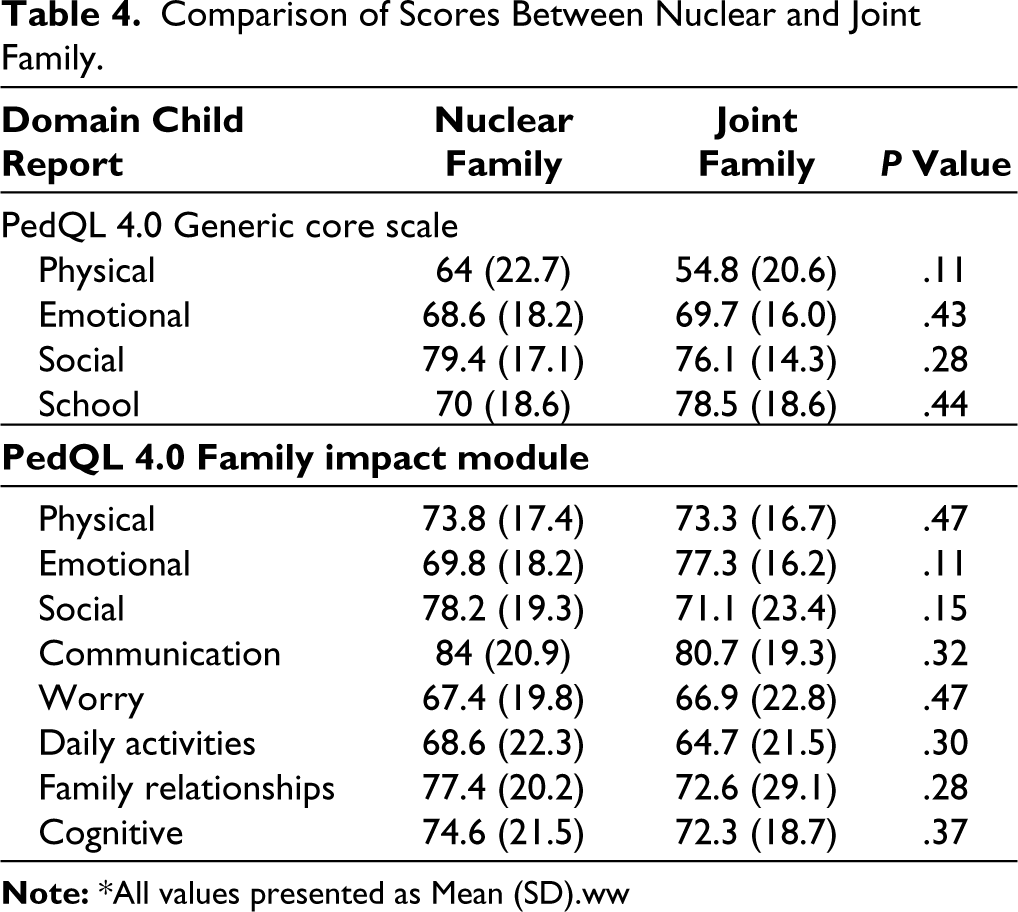
There was no significant difference in the PedQL 4.0 generic core scale scores between those with nuclear or joint families (Table 4). There was no significant difference in the constipation score between children from nuclear versus joint family (P = .14). Also, there was no significant difference in constipation score based on type of toilet use (Indian/western) (P = .05).
Comparison of Scores Between Nuclear and Joint Family.
Discussion
This study compared the HRQoL scores of children with FC and controls with the help of PedQL 4.0 generic core scale and that of the family with the help of PedQL 4.0 Family impact module.
Children with chronic illnesses may have a poor HRQoL owing to the illness, impact on school, play and peer relationship, etc. Studies have reported a poorer quality of life in children with many chronic illnesses such as cerebral palsy,17-19 epilepsy,20,21 and asthma. 22
In fact, presence of any chronic disorder in children may affect the quality of life of the children as well as that of the family. Family plays a very important role in the management of these children, and has the capacity to affect the HRQoL of the child and also may get affected by the illness. Parents of the children with chronic illnesses have been found to have low quality of life indicators. Positive predictors include schooling, age, Family income, social support, family functioning, while depression has been found to be a negative predictor of quality of life. 23 Study conducted in Thailand to assess the role of family functioning as assessed by Family Management Style Framework concluded that easy family management style was positively associated with quality of life in children with chronic diseases and vice versa. 24
Children with chronic constipation have a multitude of somatic symptoms which may lead to poorer quality of life such as abdominal pain and fecal incontinence. 6 These children struggle to pass stool due to the presence of hard stool, which leads to further stool retention and may voluntarily hold stools as evidenced by retentive posturing. The prevalence of retentive posturing was high in our study, similar to previous ones.4,25 These children are prone to shaming and bullying at school, especially those with fecal incontinence. 26 Presence of fecal incontinence is associated with lower HRQoL scores.27,28 There were only two children with fecal incontinence in our study, so such a comparison could not be made.
The present study found that the children with FC had significantly lower scores in physical, social and emotional domains, which is similar to previous studies.6,29 Systematic review and meta-analysis done by Vrisman et al. including 13 studies reported significantly lower HRQoL in children with constipation compared to healthy children. They found similar scores in self-report compared to parent proxy report. They did not find any association of fecal incontinence with QOL scores. 7
Another reason for poorer quality of life in the children with constipation may be presence of behavioral and psychological comorbidities. These children have a higher prevalence of negative personality traits. 12 Children with constipation have also been reported to have emotional and behavior problems as suggested by higher CBCL (child behavior checklist) score compared to controls. 5 Presence of such behavioral comorbidities may lead to family frustration towards the child and also may increase parental stress. In addition, variety of psychological factors have been reported as risk factors for constipation in children such as parental marital disharmony, sibling rivalry, school phobia and fear of using toilets.25,30,31 Presence of behavioral and psychological problems was not formally evaluated in the present study.
We did not find any significant correlation between constipation severity score and the PedQL Generic core scale score, which is in contrast to previous findings which reported duration and severity of constipation as a risk factor for poorer quality of life.6,32
Diet low in fiber, lacking fruits and vegetables, plays an important role in the occurrence of constipation in children.30,33 Higher milk intake has been associated with poor bowel movements in children owing to low fiber content of milk and also due to probable role of cow milk protein allergy as reported in literature.34,35 In the present study, proportion of children eating at least one serving of fruits and vegetables was lower in the constipation group, although only vegetable intake reached statistical significance.
In the present study, scores in various domains of family functioning were not significantly different between the study and control population. This finding is in contrast to a previous study. 6 There may be an explanation for such a finding that the resilience of Indian families may be better due to the availability of support of elders as almost 2/3 of the study population and almost half of the controls belonged to joint family. Presence of more family members may help the mother or the parents to handle the symptoms of the child in a much better way. Although there was no significant difference in scores between those with nuclear versus joint families (Table 4). Another reason may be that the majority of the mothers were homemakers, allowing them to spend more time with children and avoiding work-related stress to the mother.
The strength of the study is that this study provides pediatric data from India, which is lacking. Also, we tried to analyse the role of social factors such as availability of joint family support. Limitations are a small sample size, lack of follow-up HRQoL after improvement in symptoms and lack of evaluation for behavioral and psychological problems. Also, as the number of children with fecal incontinence was very low, its role in QOL could not be assessed.
Conclusion
Children with FC have significantly lower quality of life involving their physical, emotional, and social functionality. This may also affect their cognitive growth and school learning. In addition to timely diagnosis and management of symptoms, these children may require additional emotional and social support.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee, Army College of Medical College, New Delhi, India, No. IEC/05/2021/28 dated 18.08.2021. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written/Verbal Informed Consent was taken from all the participants.