
Abstract
Background:
Due to a concerning rise in reported cases of childhood abuse in India, this study was initiated with the aim of uncovering the social determinants contributing to childhood trauma. Moreover, the second objective of the study was to discuss substance use initiation and patterns among children with cumulative trauma.
Method:
As a result, an in-depth interview served as a primary source of viewpoints to examine the essential objective. The study was conducted on children with a history of abuse. Twenty-eight children in the age group of 13–18 years (Mage = 16) residing in child-care institutes in Assam were taken into consideration.
Results:
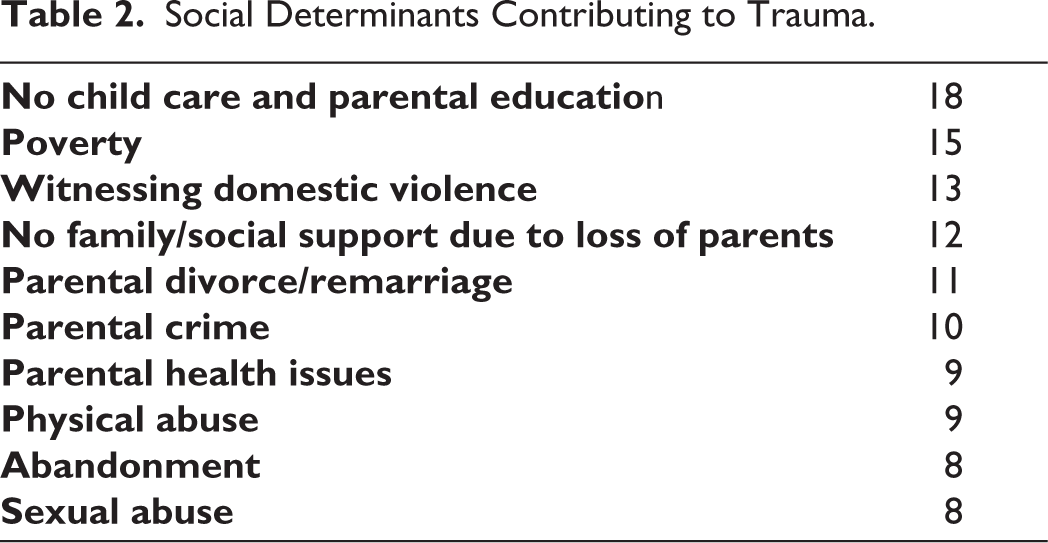
Content analysis indicated child care and education, parental divorce or remarriage, domestic violence, family mental illness, household substance misuse, parental health, parental crime, poverty, and sexual and physical violence as social determinants of health for childhood trauma. Children reported using alcohol, marijuana, tobacco, cough syrup, inhalants such as paint, and glue, chewables such as betel nut and Gutka (chewing tobacco), and pharmaceutical tablets. Initiation and pattern of substance use among early initiators were likely to be encouraged by detrimental peer influence, indicating substance abuse as normal behavior and the family’s role in shaping children’s pattern of substance use. Problematic patterns of substance use were identified, for instance, health consequences, neglect of responsibilities, and increased daily frequency.
Conclusion:
The results of this study may offer practical insights for healthcare professionals, enhancing their comprehension and addressing the social determinants of health indicating trauma and referring them to appropriate treatments. A holistic approach, which encompasses the collaboration of policymakers and healthcare providers, is vital for fostering health equity, thereby potentially preventing child abuse, childhood trauma and subsequent recidivism of substance use.
Introduction
The World Health Organization (WHO) has reported the widespread occurrence of early childhood adversity affecting a quarter of adults globally encompassing direct experiences such as physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect, as well as indirect ones like bullying, parental violence, parental substance misuse, parental incarceration, parental divorce or separation, and parental suicide or self-harm.1,2
Nevertheless, it’s important to note that not every traumatic experience serves as a reliable predictor of the development of substance misuse behaviors. It can be influenced by various factors, including the occurrence of a single adverse experience, multiple or the recurrence of adverse experiences and this vulnerability seems to be linked to different racial and ethnic backgrounds. An investigation conducted in the United States revealed that adverse experiences were linked to substance misuse, specifically tobacco and alcohol. 3 Nevertheless, the applicability of this perspective to India is constrained by distinctive geographical, cultural, and socioeconomic factors in play. In India, externalizing disorders, such as substance abuse and dependence, play a significant role in contributing to the global burden of disease.4,5 Lifetime alcohol use among school-attending adolescents in India is associated with tobacco and drug use, as well as a history of child sexual abuse. 6 Additionally, one in four Indian adolescents aged 13-15 uses tobacco, including chewing and smoking. Furthermore, cannabis is the most commonly used prohibited substance among school students, street children, and working adolescents in India. 7
Squeglia et al. 8 have noted that numerous neuropsychological and neuroimaging studies have shed light on neural vulnerabilities that contribute to the initiation of substance misuse during adolescence. Underage alcohol and drug use pose significant public health and societal challenges for individual adolescents, their families, communities, and the nation as a whole. India, with its population of over 200 million adolescents, constitutes a substantial “at-risk” demographic vulnerable to substance misuse and addiction. 9
As per the 2020 World Drug Report 10 published by the United Nations Office on Drugs and Crime, approximately 35.6 million individuals worldwide grapple with substance abuse, increasing in parts of Asia, mostly adolescents. As evidenced by the 2018 Swiss Health Behavior in School-aged Children study, 11 approximately 17% of 13-year-olds have already experimented with tobacco, 1% are active smokers, and 2% consume alcohol weekly. These figures rise at the age of 15, with 7% being current tobacco smokers and 7% reporting weekly alcohol consumption. Regarding cannabis, the study findings reveal that 12% of 14-year-olds and 22% of 15-year-olds have tried cannabis at least once. Among 15-year-olds, 4.1% are frequent users (more than 6 days per month). 11
This study addresses the rising cases of childhood abuse in India, aiming to uncover social determinants contributing to abuse and triggering childhood trauma. The second objective involves discussing substance use initiation and patterns among children with cumulative trauma, utilizing theories to explore the role of interpersonal relationships in substance use. By exploring social factors contributing to vulnerability, the research aims to reveal nuanced pathways of substance use in this population, reporting on children’s direct experiences with childhood abuse to construct an objective reality.
This study endeavors to investigate the escalating incidences of childhood abuse in India with a twofold purpose: firstly, to elucidate the underlying social determinants fueling abuse and exacerbating childhood trauma; secondly, to examine the initiation and behavioral patterns of substance use among children experiencing cumulative trauma. The research seeks to unravel the intricate dynamics that underlie substance use in this demographic. By delving into the social factors that render children vulnerable, the study aims to uncover nuanced pathways to substance use, anchored in the direct testimonies of children who have experienced childhood abuse, thus providing a more comprehensive understanding of their lived realities.
Method
Following the acquisition of the necessary permissions, the researcher collected data from different child-care institutes from November 2022 to June 2023. A total of 28 children, age group 13-18 years (Mean age 16 years) were selected from Assam, India. None of them refused the interview. Children’s Trauma Assessment Centre (CTAC) Trauma Screening Checklist (Henry et al., 2010) was used to measure the social determinants of health indicating known or suspected exposure to several potential childhood trauma. Using a purposive sampling technique, children were recruited based on criteria such as age, exposure to traumatic events, and a history of substance use. The rationale for the inclusion of traumatized children from institutions in the current study is rooted in the ongoing rise in child-related crimes in Assam despite the existence of government laws and policies. This trend has been acknowledged by the Assam Minister for Finance and Social Welfare. 13 The safety of children, encompassing protection from physical, emotional, and sexual abuse, remains a pressing concern in Assam. Detrimental practices such as child marriage, child labor, and child trafficking persist, posing significant threats. The escalating incidence of child-related crimes underscores the immediate necessity of giving precedence to the safeguarding of these vulnerable children. 14 The study has a specific focus on the trauma experiences of children and their substance use patterns and initiation.
In-person interviews were conducted within the institutes due to restrictions on the children’s movement. Following the approval of the ethical committee of Sikkim University under Reference No: SU/REG/F-1/03/2019/Vol-II/890, and approval from the state government of Assam, on December 31st, 2021, the recruitment of participants commenced. Government organizations were carefully chosen by the State Child Protection Service Assam, No. SCPS(G)217/2015/124 for data collection: Butterfly Children’s Home, Nabajiban Children’s Home and Children Home for Girls (Nagaon), Children Home for Girls and Children Home for Boys (Kamrup), Gramya Unnayan Sangstha (Morigaon), and SOFTSEED Child Home (Sonitpur). In addition, before the collection of data, consent was taken from the specific organization committee, and participant written consents were obtained as well. Rapport and trust were established, clarifying the visit’s purpose. Moreover, semi-structured interview questions, aligned with previous literature and research goals, were used without preconceived assumptions. Each interview, lasting over an hour, varied based on conversational flow. The interview was conducted in the local language which was later transcribed and translated by the authors. Two faculties assisted in reviewing the transcribed and translated verbatims. This study was carried out by the principles as articulated in the Declaration of Helsinki. Some of the interview questions, for instance, were: Can you describe your initial experience with substance use? What factors do you believe influenced your decision to try substances for the first time? Could you elaborate on any specific situations or environments where substance use tends to occur? How do you perceive the role of peer influence and family in your substance use habits? Can you discuss any patterns or routines associated with your substance use behavior?
The researchers approached content analysis from a realist perspective, assuming that participants’ language accurately reflected their experiences, meanings, and realities. 15 The data underwent analysis utilizing the traditional content analysis technique introduced by Graneheim and Lundman. 16 Subsequent to each interview, the principal investigators meticulously reviewed the recorded content, diligently transcribing it into Microsoft Word. The transcripts were not returned to the participants, wherein each interview was treated as an independent analytical unit, wherein we identified significant sections in the text, subsequently converting them into initial codes. The codes were generated inductively, as we repeatedly delved into the transcripts, noting recurring patterns of motivations and reactions articulated by the participants. The codes underwent numerous iterations during the testing phase, involving the coding of randomly selected interviews. They continued to evolve throughout the entirety of the data coding process. Any disparities observed in the interviews that were double-coded underwent thorough scrutiny, and consensus was reached to address and rectify these disparities. The participants offered positive feedback, expressing a range of emotions during the interview session. Some participants felt a sense of relaxation, while others even shed tears, as the process allowed them to vent their emotions. They perceived the presence of someone willing to listen to their buried stories.
Results
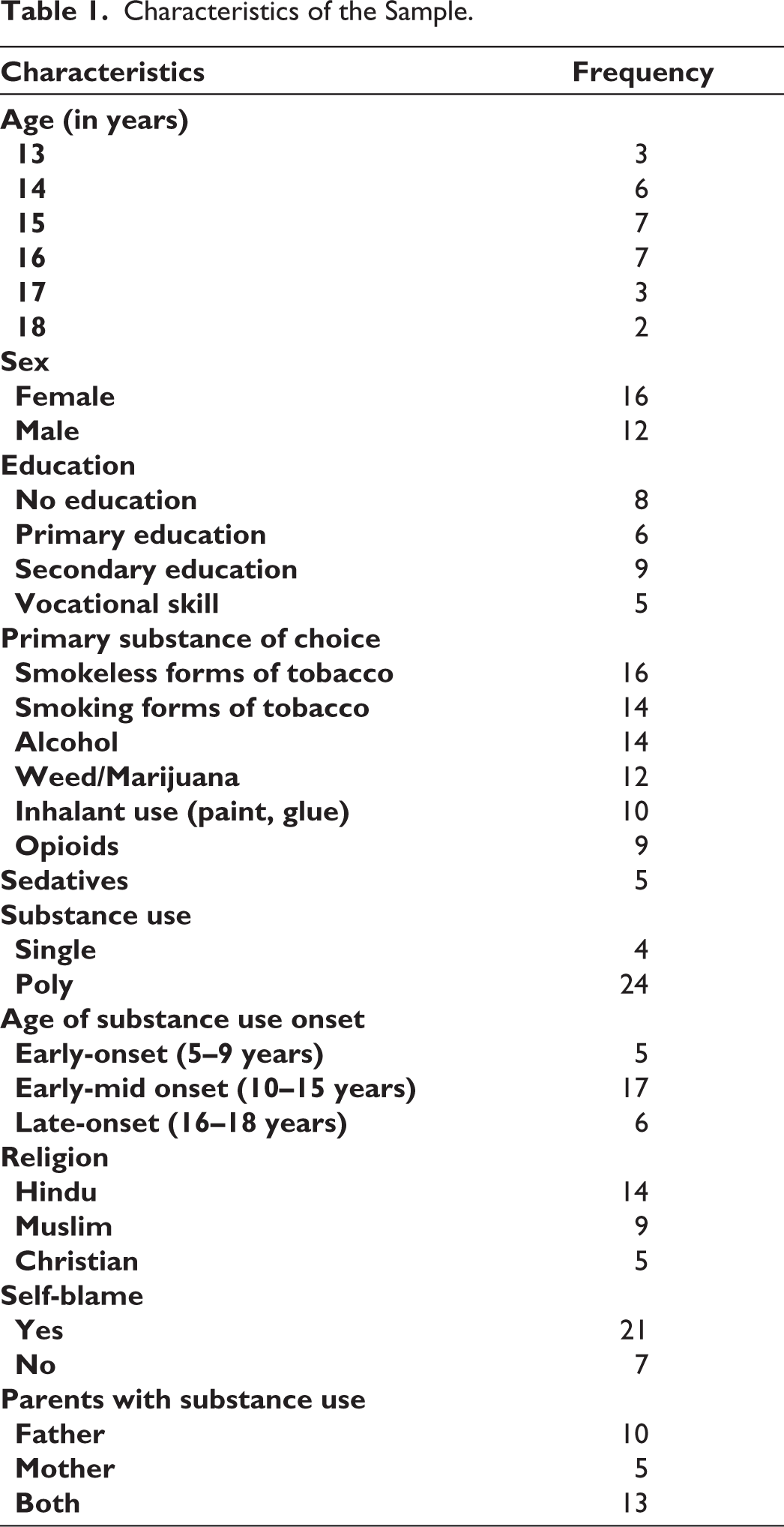
Table 1 presents the demographic attributes of the participants. Notably, 85.71% were polysubstance users, while 14.29% used a single substance. Family history information provided insights into participants’ parents, revealing a significant proportion had a socially unstable upbringing marked by factors like family living arrangements, economic hardships, housing instability, and parental mental and physical health issues. Participants recalled periods of extreme poverty during their childhood. Parental employment status varied, including cases with both paternal and maternal unemployment and a range of different jobs typically held by parents.
Characteristics of the Sample.
Social Determinants Contributing to Trauma.
Mapping of the Themes.
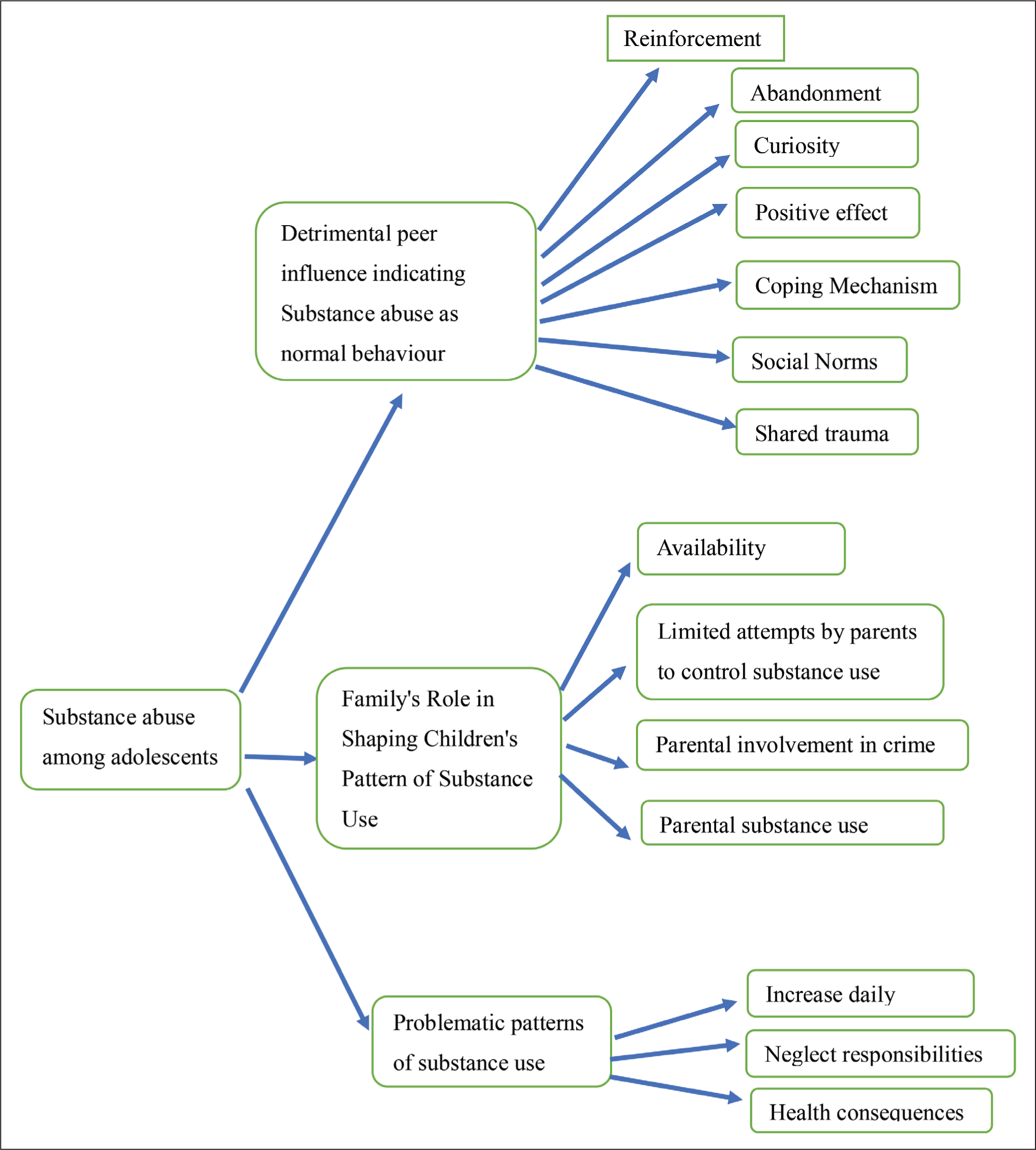
Themes 1: Detrimental Peer Influence Indicating Substance Abuse as Normal Behavior
The typical scenarios of initiation, suggest that the commencement of substance use is perceived as a customary behavior among adolescents, one that is anticipated to yield pleasurable physical and psychoactive effects. Most participants embarked on their substance use journey with alcohol, cigarette, tobacco, or marijuana, Friendship served as a support system and offered social occasions that made it easier for those to engage in alcohol and/or tobacco use who have experienced childhood trauma.
Reinforcement
In order to reinforce their friendships, respondents would augment their alcohol and tobacco usage by adapting their behavior to align with that of their friends since the home environment was always negative due to parental fights.
For instance, one participant explained, “I didn’t decline because I wanted to be part of the group. I aimed to blend in. I feel like my parents are least bothered about me and I need to make new friends.”
This perception that substance use was necessary to fit in with peers was reinforced by the belief that substance use was a normal activity for their age group.
Abandonment
In some cases, individuals who have experienced abandonment may be more susceptible to peer pressure, including pressure to use substances, as they seek acceptance and belonging. These friends may normalize substance use as a way to escape or temporarily alleviate emotional discomfort.
One participant stated
I felt so alone after my father abandoned me. My mother died and soon after my father remarried, I was asked to stay with my grandmother. I felt so lonely and was desperate to make some connections. When I met these new friends, they offered me drugs, and I thought, ‘Why not?’ I just wanted to be part of something.
Curiosity
Curiosity also played a role, with participants expressing a desire to personally experience substance use and gauge its effects.
One participant mentioned, “I simply wanted to experience it, find out if it was genuinely harmful or not, and so on. Since nobody was there to stop me.”
Positive Effect
Furthermore, it was common for participants to hold neutral or positive views about initiating substance use, with few expressing feelings of nervousness, guilt, or ambivalence. When describing the effects of substances during their initial use, participants typically reported experiencing pleasurable emotional and perceptual effects.
For instance, one participant described it as follows: “It brought me happiness. In the past, I used to feel stressed due to the abuses, but when I tried it, all my worries vanished from my mind. I found myself laughing, sharing stories, and not dwelling on my concerns anymore.”
Participants held the belief that substance use often began as a means to alleviate feelings of depression or a lack of happiness. Consequently, some young individuals turn to substances due to psychological issues.
Participant replied “cigarette makes me relax and forget my problem”
Coping Mechanism
Some trauma survivors may turn to substance use as a coping mechanism to numb emotional pain or distress. When friends provide emotional support without encouraging healthier coping strategies, individuals may resort to substances to self-medicate.
One participant described, “My friend helped me go through the pain. He was with me during my bad days. And he introduced me to alcohol, tobacco, and cigarette which gradually helped me forget my pain.”
Social Norms
In cases where a survivor’s circle of friends frequently partakes in substance use as a social activity, this behavior can become normalized within the group dynamics. This normalization process can inadvertently lower the barriers for trauma survivors to engage in substance use without fully acknowledging the potential risks associated with it. This phenomenon was a recurring theme in our qualitative study, as indicated by the verbatim responses of participants.
For instance, participants explained “Well, everyone around me was doing it, so it didn’t feel like a big deal. It was just what we did when we hung out.”
Another participant “I never really thought about it as a problem because, you know, all my friends were doing it too. It seemed like the norm.”
Shared Trauma
Friends who have also experienced trauma may bond over shared experiences, including substance use as a coping strategy. This mutual trauma bonding can reinforce substance use patterns within the group.
Responses from participants in our study include: “It was like we understood each other because we’d all been through tough stuff. So, when one of us suggested using something to feel better, the rest just went along with it.”
Another participant described “We’d been through so much together that it felt like we deserved some relief, even if it meant using stuff. It was like our way of coping.”
Theme 2: Family’s Role in Shaping Children’s Pattern of Substance Use
Limited Attempts by Parents to Control Substance Use
When parents became aware of their children’s substance use, their responses varied, ranging from actively supporting and facilitating the use to expressing disapproval or implementing punishments. However, in the majority of cases, parents and guardians were uninformed of their children’s substance use throughout the early stages. Participants frequently used methods such as minimizing or avoiding contact with their parents while intoxicated to avoid being detected by them. Some individuals accomplished this by spending the night at a friend’s home. Regardless of parental monitoring and views toward substance use, a lack of supervision by adults within communities can independently facilitate substance use: “When I drink alcohol or smoke marijuana I stay at my friend’s place. Since his mother is dead and father mostly stays outside, as he is a security guard. So nobody stays at home except he, my other friends and me.”
Sometimes, even after knowing their children are being intoxicated parents do little care and approve them for substance use.
One participant reported, “My parents never really said much about it. They knew I was using, but it was like they turned a blind eye to it. They never really tried to stop me.”
In some cases, parents who are preoccupied with their substance use may neglect proper supervision and monitoring of their children. This lack of oversight can create an environment where children are more likely to experiment with substances.
A participant mentioned
My parents often didn’t pay much attention to what their kids were doing. It was like they had other priorities; you know? They weren’t keeping an eye on us, and that made it easier for us to try things out. They didn’t know what was happening.
Another participant “It’s weird, but looking back, I think my parents’ substance use made them sort of unaware of what was happening to me. I could sneak around and try stuff without them ever noticing. They were too caught up in their world.”
Parental Involvement in Criminal Activities
Children growing up in such environments may be exposed to higher levels of stress, instability, and disrupted family dynamics. As a result, they might be more prone to turn to alcohol as a coping mechanism or a way to escape the challenges and traumas associated with their family’s involvement in crime. Additionally, the lack of proper parental guidance and supervision in such households can create an environment where children have greater access to alcohol and fewer deterrents against its use.
Participants mentioned
When your parents are always caught up in illegal stuff, they don’t have time for you. You’re kind of on your own, and that’s how I got into drinking. It was easy to sneak around and grab a bottle when no one was paying attention.
Another participant “You see, my dad was always in trouble, he steals, fights, and now is in jail for murder. Our home was often chaotic. There was yelling, and fighting, and it was just stressful. I guess I started drinking too. It was an escape.”
Parental Substance Use
In certain instances, parents influence the participants’ alcohol and tobacco consumption. Children often look up to their parents as role models. When they witness their parents’ using substances, whether it’s alcohol, tobacco, or drugs, it normalizes that behavior in their eyes. They may perceive substance use as an acceptable way to cope with stress or unwind.
One participant reported “Both the parents are alcoholics and my father even smokes marijuana. So that’s a normal thing for me to witness them drinking and smoking every day. This is how I started drinking and smoking”
Availability of Substances
Moreover, in households where parents use substances, there is a higher likelihood that these substances are readily available within the home. This easy access can facilitate experimentation among children.
When I was 9 years of age, I tried alcohol for the first time. Since it was easily available for me, as my father drinks at home. I even started smoking bidi at the same age. After drinking he beats me and my mother. This encouraged me to get into substances.
Theme 3: Problematic Patterns of Substance Use
Problematic patterns of substance use among adolescents refer to behaviors and habits related to the use of substances like alcohol, tobacco, or drugs that have negative consequences on their physical, mental, or social well-being. Individuals who began using substances at an early age were more likely to report problematic usage patterns.
Increasing their Usage to a Daily Frequency
Participants in the study revealed that adolescents grappling with problematic substance use tend to partake in substance consumption more frequently than their peers. They began using substances sporadically or on occasion but gradually transitioned to a point where they consumed these substances every day. One participant described his pattern of drinking:
For me, it was like a way to cope. I was often bullied in school and was physically abused by my friends. I started doing it now and then, but you know before I knew it, I was doing it every day. I felt it was the only way to escape from my harsh feelings, and eventually became a habit.
When discussing their substance use patterns during the initial year of use, they mentioned that they transitioned to daily usage within a very short period.
“I would never miss any chance to drink and smoke. Because the after effects help’s my mind free from those negativity”
Neglect of Responsibilities
Adolescents with problematic substance use may neglect their responsibilities, such as schoolwork, extracurricular activities, or family obligations, in favor of substance use. This can result in declining academic performance and strained relationships with family and friends. One participant stated: “I’ll be honest, there were times when I skipped school just to keep drinking. It was like I didn’t care about anything else. In the end, I dropped out of school.”
Adolescents with problematic use reported losing interest in activities they once enjoyed including hobbies, sports, or social interactions that no longer hold their attention.
I remember when I used to play cricket, do my paintings, and spend time with friends in the neighborhood and family members. But ever since I started using it, things changed. Those hobbies and hanging out with people, just don’t excite me like they used to. I’m more focused on finding ways to get my stuff. I’ve let down my friends, stolen money from them even my parents. It’s not that I want to be this way, but it’s like the substances took over, and now I’ve lost touch with the things that once brought me happiness.
Health Consequences
A significant portion of the participants have experienced physical and mental health consequences with substance abuse issues. These effects varied among participants, offering the researcher a wide range of experiences and perspectives on the matter. The following narratives were demonstrated:
I used to engage in marijuana or alcohol consumption, and there were instances when I had to go without meals or sleep without having dinner at night. As a result, I experienced weight loss and began encountering liver issues. I’ve lost my appetite and constantly feel a sense of sadness. I can’t deny it; using those substances took a toll on my health. My body feels weaker, and I’ve even had these weird chest pains. It’s not just physical; it’s in my head too. I’m anxious all the time. My mind feels foggy, and I’m not the happy person I used to be.
Other participants have reported having weak immune systems, digestion problems, sleep disturbances, nutrition deficiencies and increased vulnerability to injuries.
Discussion
The research findings underscored that children in the study population were exposed to traumatic experiences resulting from a range of factors, these included parental involvement in criminal activities, instances of abandonment, occurrences of sexual violence, incidents of physical violence, prevailing poverty, absence of adequate child care, and limited parental education, are consistent with prior studies. 17
Trauma represents the social determinant of health encompassing geographic, demographic, educational, financial, or environmental factors that serve as obstacles within a community, hindering individuals from fulfilling diverse needs. 18 The WHO 19 defines social determinants of health as “the conditions in which people are born, grown, work, live, and age, and the wider set of forces and systems shaping the conditions of life.” A study by Gigli and Vallivedu 20 stated that children and adolescents had documented social determinants of health associated with problems with housing, upbringing, and financial conditions, as well as lack of family support. Another study reported that social determinants of health for children with trauma were associated with poverty and financial problems were associated with neglect and abandonment.21,22 Housing instability, for instance, hazardous living conditions and homelessness, low parental education, and food insecurity are also associated with trauma such as child maltreatment.23,24,25 Experiencing sexual and physical abuse is linked to a higher likelihood of using both legal and illicit substances26,27 Challenges can be exacerbated by a range of factors, such as socioeconomic status, poverty, urbanization (highlighting differences between rural or slum areas and urban zones), as well as social group distinctions. Additionally, experiences like domestic violence, sexual abuse, bullying and assault by peers are linked to a cascade of psycho-social and behavioral challenges.28,29 The living conditions experienced by children and adolescents render their growth and development susceptible. Childhood and adolescence represent critical phases necessitating particular attention, given their significance in physical, psychological, and emotional development. Negotiating these intricate processes inherently makes children and adolescents unique individuals.30,31
The current findings indicated that tobacco/gutka, betelnut, cigarette, alcohol, marijuana, glue, or paint were the most common substances used, and are similar to other studies conducted.32,33 These substances were easily available, accessible, and affordable due to the majority of the local community’s economic dependence on substance cultivation, especially tobacco, betelnut, and alcohol. Assam is known for its traditional homemade alcoholic beverage “Lao-Phani.” These brews are often produced locally and may be more accessible than commercially produced alcohol. In some areas of Assam, tobacco cultivation is a significant source of income for farmers, and consumption of tobacco is highest in Assam. 34
Adolescents tend to exhibit significantly problematic attitudes toward substance use and engage in more adverse usage patterns coupled with a reduced commitment to prosocial goals. 35 The interviews have revealed that they often commence substance use within home environments where adult supervision is lacking. This absence of monitoring grants them the freedom to use substances within the confines of their own homes or outdoor spaces, and in some instances, substances are obtained by pilfering from their homes. Furthermore, in certain cases, adults are actively enabling or facilitating substance use by being users themselves.35,36 Additionally, the presence of substances in the household increases accessibility, parental intoxication hampers their ability to detect their children’s substance use or monitor their activities, and positive parental attitudes toward substance use can prompt some parents to actively support and enable their children’s substance use.
Findings have indicated that another primary factor driving youth substance use is substance use among family members. This discovery is consistent with previous studies conducted in different regions. 37 It highlights that a significant number of young individuals turn to substance use as a result of the substance use habits observed within their families, including parents, siblings, and other relatives. This propensity to mimic and adopt behaviors witnessed in their family environment underscores the importance of family members serving as positive role models by refraining from substance use. Additionally, fostering strong family bonds, open communication, mutual support, and understanding are recognized as pivotal protective measures to prevent substance use among youth.
Our investigation revealed that peer influence played a predominant role in youth substance use, a finding that aligns with similar studies conducted in various locations.37,38,39 This underlines the significance of peers as a compelling force driving youth into substance use, as many young individuals tend to emulate the behaviors and practices of their friends who share common characteristics. Social networks emerged as a pivotal avenue through which different substances were accessed. Consequently, addressing this issue entails parents actively monitoring and guiding their children’s daily activities, while school health programs should prioritize health education, with a specific focus on imparting knowledge about the detrimental effects of substance use on health, social relationships, and the economy.
Our study has pinpointed that psychological factors serve as catalysts for youth engagement in substance use. These factors, encompassing the desire for relaxation, pursuit of happiness, temporary escape from problems, stress relief, resolution of depression and anxiety, and self-stimulation, emerged as the primary motivators for substance use. This discovery resonates with the findings of another study conducted elsewhere.40,41 It emphasizes the significance of psychological factors such as anxiety, boredom, stress, and overall dissatisfaction with life as the principal risk elements associated with youth substance use.
Limitations
The study has some limitations that should be mentioned. The relatively small sample size may restrict the generalization of findings. The findings may not be universally applicable to other cultural or geographical contexts hindering the generalization of conclusions to a more diverse population. The lack of a longitudinal approach and the cross-sectional nature of the study is another limitation, as it prevents understanding the dynamics between childhood adversity and substance use over time. Potential bias in self-reported data, including recall bias and social desirability bias, needs to be acknowledged as a limitation. Additionally, the limited exploration of protective factors is another limitation of the study.
Further Research and Conclusion
In the Indian context, supporting traumatized children requires a multi-faceted approach, including trauma-informed cognitive behavioral therapy, play therapy, debriefing, eye movement desensitization and reprocessing, and support groups. Accessible mental health professionals who understand cultural sensitivities are essential, alongside trauma-informed schools that offer safe spaces and emotional support. Engaging community resources and providing family support is vital, as is integrating holistic healing approaches that respect cultural beliefs. A systematic approach including psycho-education, consultation with school personnel and parents, crisis hotlines, and community-based programs advocates great promise toward healing traumatized children. 42 Advocating for policy change, conducting research, and offering long-term support are also crucial elements in fostering the resilience and well-being of traumatized children in India.
This study’s findings have crucial implications for preventing and addressing substance use among children with adverse experiences in government organizations. Besides trauma, various factors contribute to substance use in these children, offering focal points for health promotion efforts. Recommendations include collaboration among public health professionals, NGOs, and educational institutions to provide comprehensive health education at lower grade levels. Emphasis should be on educating about the harmful effects of substance use. Creating Information, Education, and Communication (IEC) materials and Behavior Change Communication (BCC) materials is vital. Proactive steps by the government, such as job creation for youth, encouraging NGO investment in youth initiatives, and establishing recreational centers, can help reduce current youth substance use.
Footnotes
Acknowledgements
The authors express their gratitude to the children and the staff of the Child Care Institutes for their support and cooperation during the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Sikkim University under Ethical Reference Code: SU/REG/F-1/03/2019/Vol-II/890.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent
Necessary informed consent were received and obtained respectively before initiating the study from all participants.