
Abstract
Background:
In Pakistan, where unintentional injuries among toddlers pose a significant public health challenge, understanding the factors that contribute to elevated injury risks is crucial. A two-dimensional approach including parental factors (internal/external health locus of control and perceived vulnerability) and child factors (the child’s temperament) is explored as contributing to the unintentional injury behaviors of toddlers.
Method:
The study involved 241 parents of toddlers aged 18–36 months from daycare centers in three major Pakistani cities who had observed multiple recent injuries in their children. The comprehensive online assessment, lasting 15–20 minutes, incorporated the child vulnerability scale, injury behavior checklist, parent health locus of control questionnaire, and early childhood behavior questionnaire. Demographic details included child and parent age distributions, with a focus on educational backgrounds. The participants comprised both fathers and mothers, and the data analysis employed Smart-PLS software for structural equation modeling.
Result:
The results suggested there is no direct relationship between parental health locus of control (internal/external) and injury behaviors in children. However, an indirect and significant path was observed from the parental health locus of control (internal/external) to perceived child vulnerability and injury behaviors through moderation of temperamental characteristics.
Conclusion:
Our research underscores the indirect link between parental factors, child temperament, and toddler injuries in Pakistan. Culturally sensitive interventions targeting parental awareness can play a pivotal role in safeguarding the well-being of the youngest members of society.
Introduction
Unintentional injuries have significantly affected the mortality of children in the developing world.1,2 The study delves into the root causes of injuries affecting children, aiming to mitigate the alarming frequency of these unfortunate incidents. By focusing on early childhood, the research sheds light on pivotal factors influencing injury behaviors. Specifically, it examines parental perceptions of their child’s behavioral and psychological attributes, along with the child’s temperamental characteristics. This investigation also considers how a parent’s perception of their child’s vulnerability is shaped by internal or external parental health loci of control. Emphasizing the significance of understanding parental perspectives, this connection underscores the development of effective measures to safeguard children from injuries. 3 Parental perception of child vulnerability is defined in current research as parents who perceive their child as vulnerable to injury, illness, and/or death despite any clinical evidence to the contrary. 4 Parents who display perceived vulnerability tend to be more vigilant and concerned about potential unforeseen events affecting their children than other parents. This heightened perception is grounded in the concept of health locus of control (HLOC), which can be either internal or external. This distinction reflects the degree to which parents perceive themselves as having influence over their child’s health outcomes. 5 Parental health locus of control can be further addressed as a set of belief systems a parent has about their influence on a child’s health. 6 When a parent operates with an internal locus of control, they believe that their actions directly impact their child’s health. Conversely, an external locus of control suggests reliance on powerful external entities like God, the media, peers, or health professionals for authority and influence. 7
Locus of control is a psychological concept that encompasses specific attitudes and behaviors, serving as a perceived influence over the events in an individual’s life. Parental beliefs regarding their child’s health locus of control have demonstrated an impact on both parental supervision and the risk of injury to children. 8 Parents who attribute their child’s health to external factors rather than their own beliefs or parenting practices tend to exercise less supervision, both at home and in external settings. This shift in responsibility perception may contribute to varying levels of parental vigilance and, subsequently, influence the risk of injury to children. As a result, these children have a high record of accidents causing physical injuries. 9 On the contrary, parents with an internal locus of control believe that they are responsible for their child’s health and constantly supervise their kids both in home and outdoor settings; consequently, a lesser injury rate is observed.9,10 In addition to the influence of parental beliefs on supervision and injury risk, another significant contributing factor to this relationship may be the temperamental characteristics of a child. The logic behind this connection lies in understanding how a parent’s perception of their control over a child’s health may interact with the child’s inherent behavioral traits. Parents who attribute their child’s health control externally might respond differently to a child’s temperament, potentially affecting their level of supervision and, consequently, the risk of injuries. This interplay underscores the importance of considering both parental beliefs and the temperamental aspects of a child in comprehending and addressing injury risks. Building on this, the researchers11-13 suggest that the frequency of accidents resulting in injuries is potentially influenced by the behavioral attributes of the child. This underscores the interconnected roles of parental beliefs, both internal and external loci of control, and parental perceptions of the child’s vulnerability. By considering the dynamics between these factors, the research aims to provide a comprehensive understanding of the multifaceted elements contributing to accidents and injuries in children.
Attribution research14-16 serves as a framework for comprehending how individuals perceive causation. This theoretical paradigm deconstructs the attribution process into antecedents, encompassing motivations and beliefs and subsequent behaviors and attitudes. Employing this framework, our research explores the intricate interplay of variables under examination. Accidents resulting in injuries often trigger attribution activities among parents, especially when the cause of an event is ambiguous—an inherent characteristic of childhood injuries. Take, for example, a child’s fall from a chair, which may be attributed to the child’s behavior, environmental conditions, situational factors, or the parent’s momentary unavailability. The inherent ambiguity in injury causation motivates parents to draw causal attributions, contributing to our understanding of how these attributions shape parental responses to toddler injuries.
This study delves into the cognitive aspects and beliefs of parents, specifically focusing on parental health locus of control, to comprehend how parents attribute causes to events. Parental health locus of control refers to a parent’s perception of their influence in their relationship with their child. Recognizing that certain behavioral traits are associated with injury behaviors, such as distractibility, impulsivity, and activity, motivates our investigation into the connection between injury-prone behaviors and temperament. Previous research has already identified a correlation between temperament characteristics and injuries in infants, highlighting a robust causal relationship, particularly with what is termed as “difficult temperament.”17,18 For instance, studies have shown that infants displaying negative mood patterns and withdrawing behaviors at the age of six months are more susceptible to injuries in their early years.19,20 This discovery prompts a significant question about the factors influencing the frequency of injury behaviors and susceptibility in children. Specifically, researchers aim to identify commonalities among children with challenging behaviors that make them more prone to injuries.
To conclude, this study intricately examines factors influencing unintentional injury behaviors among toddlers in the developing world, with a particular focus on the Pakistani context. By examining parental perceptions of their child’s behavioral and psychological attributes through the lens of health locus of control, the study sheds light on the nuanced dynamics that contribute to injury risks. The internal or external orientation of the parental health locus of control emerges as a crucial determinant, impacting the degree of parental supervision and, subsequently, the occurrence of injuries in children. Moreover, the research acknowledges the significant role of a child’s temperament, including attributes such as distractibility, impulsivity, and activity, in shaping injury-prone behaviors. Drawing on attribution theory, the study explores how parents attribute causes to childhood injuries, especially when the circumstances are ambiguous. The research proposes a mediated moderation model to unravel the intricate relationships between parental health locus of control, perceived child vulnerability, temperamental characteristics, and unintentional injury behaviors. By elucidating these connections, the study aims to offer valuable insights for future interventions and preventive measures, fostering a comprehensive understanding of the multifaceted determinants that contribute to toddler injuries in Pakistan and beyond.
Conceptual Framework
In crafting the framework, we rely on established theories in child development and health psychology to rationalize the inclusion of variables in our research. Extensive literature acknowledges the pivotal role of parental beliefs in shaping parenting behaviors and influencing child outcomes.21,22 Aligned with this proposition, we introduce perceived vulnerability as an intermediary between internal and external health loci of control and our outcome variable, namely the unintentional injury behaviors of toddlers. This choice is corroborated by existing research indicating the significant impact of parental perceptions of vulnerability on child safety practices.4,23,24 In addition, we consider temperament as a moderator in the relationship between perceived vulnerability and injury behaviors, a plan supported by studies highlighting the significant role of temperament characteristics in shaping child behavior and susceptibility to injuries.25-28 Grounded in the understanding that parental beliefs wield substantial influence over their perceptions of their child’s vulnerability and subsequent caregiving behaviors, our investigation posits that the parental perceptions, shaped by both internal and external health locus of control, not only exert a direct impact on toddler injury behaviors but also operate through a nuanced mechanism. We introduced perceived vulnerability as an intermediary element that encapsulates how parental beliefs decode into heightened awareness and protective actions for their children. Furthermore, the introduction of temperament into this intricate web adds an additional layer of intricacy. This moderating factor is envisioned to affect the strength of the relationship between perceived vulnerability and toddler injury behaviors, shedding light on the intricate dynamics involved. Research studies29-32 underscore the varying influence of temperament on child behaviors and susceptibility to injuries, supporting our theoretical framework. By embracing the concept of mediated moderation, our research not only delivers a theoretical lens but also probes into the practical intricacies of parenting behaviors. For instance, consider the contrasting approaches of a parent who firmly believes in their substantial influence over their child’s health (internal health locus of control) versus a parent who attributes their child’s health to external factors. These beliefs, we postulate, not only directly shape parenting strategies but also interact differently with the temperament of the child. This holistic approach, grounded in both theory and practical insights, aims to disentangle the multifaceted connections, offering a richer understanding of the pathways through which parental beliefs and perceptions contribute to unintentional injury behaviors among toddlers. Such insights pave the way for targeted interventions and approaches, informed by real-world dynamics and tailored to diverse parental belief systems and child temperaments.
Methodology
Measurements
Procedure
In implementing the study, the researcher began contact with daycare facilities in three major cities in Pakistan. We employed a purposive sampling strategy to identify parents who had noted more than two recent accidents resulting in injury to their preschoolers over the preceding two weeks. To determine the appropriate sample size for our study employing structural equation modeling (SEM), we conducted a power analysis using the G-Power software. We specified an effect size of 0.3, which represents a moderate effect according to Cohen’s guidelines. Additionally, we set an alpha level of 0.05 and a power level of 0.80, reflecting standard values in statistical analysis. Considering a moderate number of predictors in our SEM model, the software calculated that a minimum sample size of 210 was needed to achieve adequate statistical power. This approach confirms that our study is sufficiently powered to detect meaningful effects within our SEM model, providing confidence in the reliability and validity of our findings. Parents willing to participate were presented with a 15- to 20-minute assessment proforma. The comprehensive form integrated four key measures: the Child Vulnerability Scale, the Injury Behavior Checklist (IBC), the Parent Health Locus of Control Questionnaire, and the Early Childhood Behavior Questionnaire. Additionally, participants were requested to furnish demographic details on a designated sheet. To facilitate the seamless exchange of proformas, parents were asked to provide their email addresses. It is imperative to note that permission for our research was granted by the research committee of ICP 12004272, all study procedures were granted prior approval by the relevant institutional body, and participants were ensured informed consent as a fundamental ethical consideration.
Results
Demographic Profile of Participants
The research included 241 parents as representatives of a child’s behavior. Inclusion criteria limited our data to children within the age range of 18–36 months. The more frequent types of unintentional injuries included wounds from sharp/blunt surfaces, falls, scalds, and bruises. Demographic characteristics, the child’s age (M = 26.4133, SD = 5.60463) in months, and the parents’ age (M = 33.8533, SD = 6.89556) in years were inquired about in a continued form and later converted to categories based on mean and standard deviation. Also, 44.8% of the children’s ages ranged between 18 and 24 months, 31.2% ranged between 25 and 30 months, and 21.4% ranged between 31 and 36 months. Among the children, 57.1% were boys and 40.3% were girls. Moreover, 30.5% of parents’ ages ranged between 21 and 28 years, 28.6% were between 28 and 35 years, 25.3% were between 35 and 42 years, and 13% were between 42 and 50 years old. The research included 39.6% fathers as a representative, and 57.8% were mothers. Also, 3.9% of parents were educated up to the 12th grade (high school), 29.2% completed a college education, and 64.3% completed a post-graduate degree from a university.
Data Analysis
Smart PLS software was used to perform SEM-PLS because it is suitable for theory development, can handle small data, and is flexible on data assumptions of normal distribution.36,37 The assessment procedure used in this study was recommended by Hair et al, 38 in which we first evaluate the dimension model, followed by the structural model. In survey-based studies, common method variance (CMV) should be scrutinized, particularly when you are collecting data for both dependent and independent variables at the same point in time. Procedural remedies suggested by MacKenzie and Podsakoff 39 were used to overcome CMV, such as providing clear instruction, avoiding confusing and complex questions, and assuring confidentiality. CMV was not a concern, as confirmed by Table 1, and no correlation matrix was greater than 0.9. 40 Second, we performed another test proposed by Kock, 41 named the collinearity test. Variance inflation factor values less than 3.3 stated in Table 2 prove that CMV is negligible in the current study.
Fornell-Larcker Criterion.

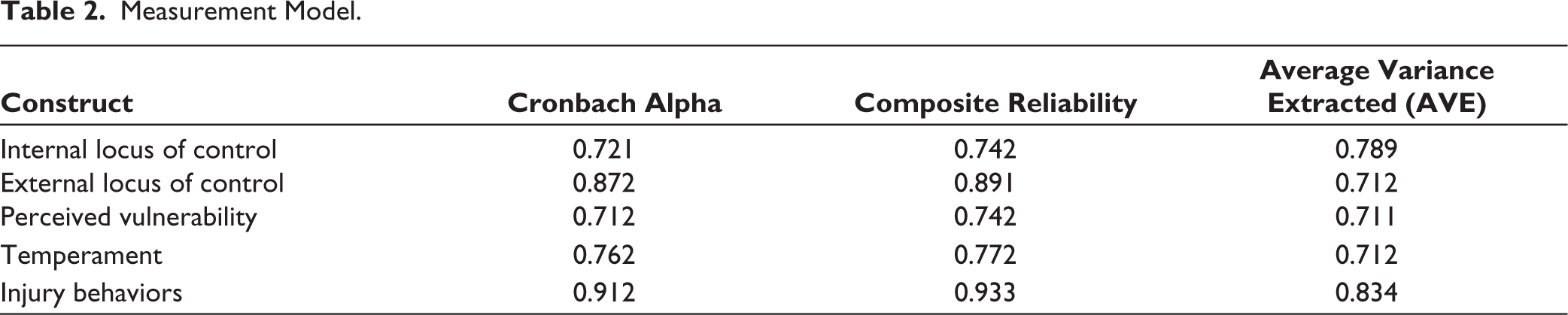
Measurement Model.
Measurement Model
The measurement model 38 provided assessment procedures for examining discriminant validity, convergent validity, internal consistency, and reliability. The Fornell-Larcker criterion, authorized as the square root of AVE, was also acceptable. Discriminant validity determined by the Fornell–Larcker criterion and the Heterotrait-Monotrait ratio (HTMT) 42 suggested that the value for the HTMT criterion should not be greater than 0.85, and as observed in Table 1, the Fornell–Larcker criterion and the HTMT criterion determines a discriminant validity value lower than 0.85. The collinearity results showed that all variance inflation factor (VIF) values are close to 1, with the highest being 1.172 for injury behavior. Generally, VIF values below 5 are considered acceptable, suggesting that collinearity is not a significant concern in this analysis. The low VIF values affirm that the variables included in the model are not highly correlated, supporting the reliability of the regression coefficients estimated for each variable. The measurement constructs (Table 2) were evaluated for reliability and validity using indicators such as Cronbach’s alpha, composite reliability, and average variance extracted (AVE). The constructs, including internal and external locus of control, perceived vulnerability, temperament, and injury behavior, demonstrated overall good to excellent reliability and validity, suggesting their suitability for assessing the intended variables.
Structural Model
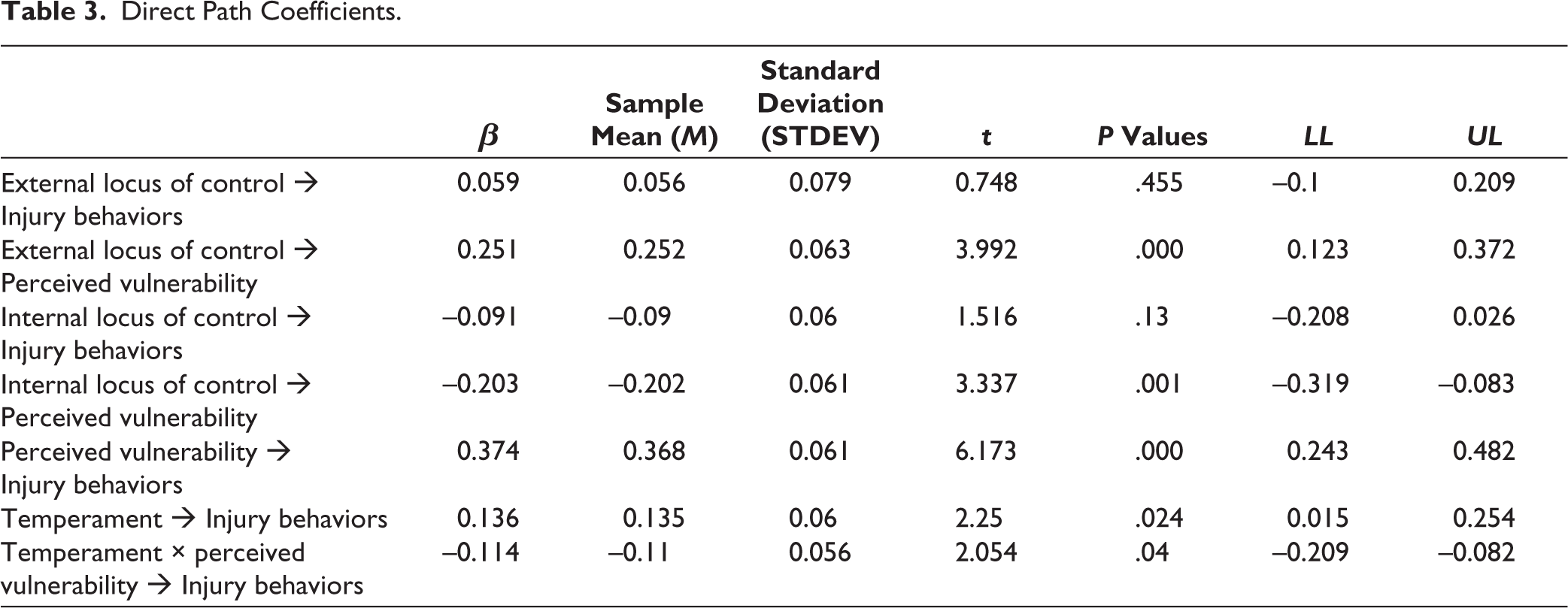
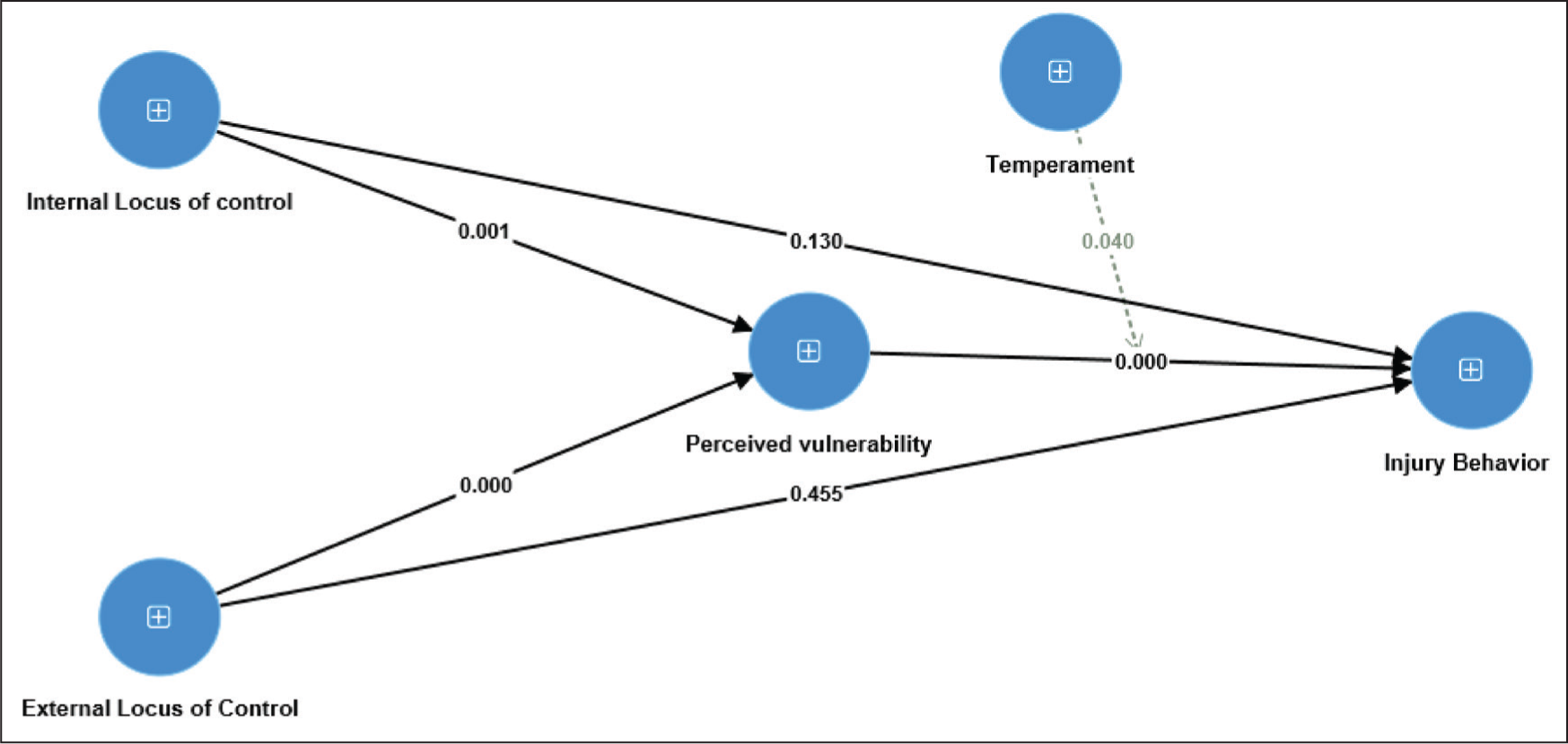
The assessment of the structural model included an examination of predictive relevance (Q 2 ), the coefficient of determination (R2), the significance of path coefficients, and effect size (f 2 ). To enhance the robustness of the findings, a bootstrapping procedure involving 5,000 resamples was conducted to obtain standard errors and compute t-values. This methodological approach was chosen to ensure a comprehensive evaluation of the model’s predictive power, explanatory capability, and statistical significance. It was found that the external locus of control and internal locus of control have no direct significant impact on injury behavior (β = 0.059, t = 0.748, P = .456) (β = –0.091, t = 1.516, P = .130). Whereas the external locus of control and internal locus of control have a significant effect on perceived vulnerability (β = 0.251, t = 3.992, P = .000) (β = –0.023, t = 3.337, P = .001). Additionally, perceived vulnerability and temperament directly impact injury behavior (β = 0.374, t = 6.173, P = .000) (β = 0.136, t = 2.50, P = .024) (Table 3). We evaluated the moderating effect of temperament on the direct relationship between perceived vulnerability and injury behavior and supported our study hypothesis; that is, temperament moderates the relationship between perceived vulnerability and injury behavior, as these interactions are significant (β = –0.114, t = 2.054, P = .040) (Figure 1). To confirm the mediation hypothesis, we assessed the mediating effect of perceived vulnerability on the indirect relationship of internal and external locus of control with injury behavior (β = 0.095, t = 3.120, P = .002) and (β = –0.076, t = 3.043, P = .002), respectively (Table 3). The significant interaction terms in Table 4 show the full mediation between the constructs.The observed results suggest the presence of mediated moderation in the examined structural model and highlight the intricate dynamics involved in the relationship between parental health locus of control and toddler injury behaviors. The significant negative relationship between the interaction of temperament and perceived vulnerability with injury behaviors indicates that the influence of perceived vulnerability on injury behaviors varies based on the child’s temperament. This finding implies that the connection between parental perceptions of their child’s vulnerability and following injury behaviors is nuanced and dependent on the child’s temperamental characteristics.
Direct Path Coefficients.
The Indirect Path Result Between Constructs.
Indirect Relationship Between Constructs.

Additionally, the indirect effects discovered in Table 4 shed light on the pathways through which parental health locus of control impacts toddler injury behaviors. The positive indirect effect of external locus of control on injury behaviors through perceived vulnerability (β = 0.094, P = .002) suggests that parents who attribute their child’s health to external aspects may indirectly contribute to injury behaviors by fostering a heightened sense of vulnerability. On the other hand, the negative indirect effect of internal locus of control on injury behaviors through perceived vulnerability indicates that parents with a stronger belief in their impact on their child’s health may mitigate injury behaviors by influencing the perception of vulnerability.
Discussion
The current study aims to identify key risk factors contributing to toddler injuries, with a particular focus on exploring the roles of parents’ locus of control and perceived vulnerability, along with child temperament, as potential determinants of accidental injury behaviors in young children. The investigation sought to address three crucial questions: (a) whether parental locus of control influences the heightened injury behavior in children; (b) if perceived vulnerability stands as the sole determinant of child risk-taking behavior; and (c) whether child temperament moderates the relationship between perceived vulnerability and injury behavior. In the Pakistani cultural context, where familial and societal influences play a significant role, the results emphasize the importance of tailoring interventions to align with cultural nuances. Parental beliefs, shaped by internal and external health loci of control, not only directly influence injury behaviors but also function through a nuanced mechanism. The cultural significance of familial influence and collective decision-making may further shape these mechanisms, influencing how parents perceive and respond to their child’s vulnerability to injuries.
Despite the fact that parents acknowledge the inevitability of injuries in children, they maintain a belief that their actions significantly influence their child’s health, encompassing accidents and the risk of death. Furthermore, researchers posit that an external locus of control, which includes factors such as reliance on God, unsafe play practices, environmental hazards, influence from friends, and exposure to television, constitutes key risk factors for child injuries. This underscores the intricate interplay between parental perceptions, beliefs, and external factors in shaping the landscape of child safety and injury prevention.5,28,34 Some parents acknowledge that the external locus of control is beyond their direct influence, perceiving a sense of helplessness and a belief in the ineffectiveness of their actions in this domain.43,44 Consequently, they display lower engagement in adopting preventive measures to manage their child’s tendency for risk-taking behavior. Interestingly, our study lines up with previous research, representing that the external locus of control may not directly impact child injury behavior but exercises its influence through parents’ perceived vulnerability to their child’s injury. 45 Therefore, to prevent targeted injuries, new creative measures must be addressed using the underlying beliefs that parents have about protecting their children against injuries.
Concerning internal locus of control, there is a noteworthy trend among parents of children facing health challenges, demonstrating heightened concern for their child’s well-being and development, irrespective of socioeconomic factors and intellectual levels.46,47 Practical justifications for this observation lie in the inherent nature of caring for a child with health challenges, necessitating a more vigilant approach. Furthermore, existing research supports the notion that parents of vulnerable children tend to exhibit an elevated level of protectiveness, manifesting as unfounded anxiety regarding their child’s safety. Consequently, they often impose more stringent age-appropriate limits on their child’s behavior compared to their counterparts.28,48,49 This heightened vigilance is a practical response to the increased vulnerability of their children, reflecting a proactive caregiving approach. 50
Furthermore, researchers also support the evidence that parents have considerably good control over injury protections in the first 24 months of a child’s life.4,51 Nevertheless, as children begin to crawl, roll, and walk, they become more exposed to accidental injury, specifically in the absence of their caregivers (parents). Thus, the present findings are consistent with prior studies in the pieces of evidence that parents with a higher internal locus of control are more likely to remember, make a note, and report child injuries as they have a higher perceived vulnerability compared to an external locus of control.52,53 This integration of the parents’ perceptions has the potential to help the new childcare programs to always aim to control childhood injuries.
The results suggest perceived vulnerability is influenced by the health locus of control which is defined as persons’ beliefs regarding their health status, determined by internal (perception and own behaviors) and external (God, fate, and luck) bases. 54 To date, many previous pieces of research have simply linked the health locus of control with other constructs, for example, delayed gratifications, 55 persistence, 56 and resistance 57 are parents’ internal LOC factors that help them shape their child’s risk-taking behavior. Similarly, the child adopts the parent’s tendencies in both internal and external ways in a full range of control expectancies.43,58 Furthermore, consistent with prior studies, injuries are more frequent in the first two years of life in children when parents have a low internal locus of control58,59 because it may result in perceived helplessness that lessens parents’ action in injury avoidance.43,45,60 Taken together, the current study results confirm that locus of control regarding the health of a child is a basic determinant of the perceived vulnerability of a child, which is later on influenced by the temperamental characteristics of the child and leads to accidental injuries. In the Pakistani cultural context, where collectivism and familial interconnectedness often prevail, the temperament of a child may be intertwined with broader family dynamics, influencing parental caregiving practices.
Concerning children’s role, their temperamental characteristics also place them at higher risk of injury. In the common method variance, the temperament characteristic was related to several traits such as anger, frustration, parenting, gender role, etc.32,61 Furthermore, a child’s self-reported perception of their family environment, particularly in situations where parents exhibit a high external locus of control, plays a crucial role in influencing the child’s risk-taking behaviors.29,62 In addition, the incidence of injury is high when toddlers extend themselves beyond their competency range and engage in a new activity that is inconsistent with their standard of comfort.63-65 Additionally, children characterized by fearlessness and lower activation control are more inclined toward adopting high-risk approaches compared to their counterparts with lower constraints. This inclination is attributed to intentionally controlled children being more likely to minimize risk-taking behaviors and adopt precautionary approaches.30,66
The research extends beyond traditional approaches by exploring not only direct relationships but also the unique interplay among key determinants. Drawing on established theories, such as the Health Belief Model, 67 Social Cognitive Theory, 68 and Temperament, 69 our investigation aligns with the understanding that parental beliefs significantly impact caregiving behaviors and child outcomes. The Health Belief Model postulates that individuals’ health-related behaviors are influenced by their perceived susceptibility, severity, benefits of action, and barriers to these actions. In our context, parents’ perceptions of their child’s vulnerability, influenced by the health locus of control, align with the Health Belief Model’s emphasis on perceived susceptibility. Social Cognitive Theory, on the other hand, explains the role of observational learning and social influence in shaping behaviors. Our study integrates these theoretical frameworks, suggesting that parental beliefs are socially constructed and observed, influencing their actions in safeguarding their children from injuries. Furthermore, given temperament as a moderator, we draw on the Rothbart and Derryberry’s 69 propositions, which posit that individual differences in emotional, motor, and attentional reactivity play a vital role in shaping behaviors. According to this theory, a child’s temperament interacts with environmental factors and influences how parents perceive and respond to their child’s behaviors. This theoretical foundation enhances the robustness of our research approach, providing a comprehensive lens through which to understand the intricate dynamics between parental beliefs, perceived vulnerability, temperament, and toddler injury behaviors.
Our results regarding the interaction between temperament and perceived vulnerability highlight the importance of considering temperament as a moderating factor in the relationship between parental beliefs and toddler injury behaviors. The positive indirect effect of external locus of control on injury behaviors through perceived vulnerability aligns with attribution theories, suggesting that external attributions may heighten parental perceptions of vulnerability.4,70 On the other hand, the negative indirect effect of internal locus of control on injury behaviors through perceived vulnerability echoes the potential mitigating role of internal attributions. In crux, the mediated moderation framework tested in this study not only aligns with existing theories but also contributes to bridging theoretical gaps. The incorporation of parental health locus of control, perceived vulnerability, and temperament into a unified model proposes a more comprehensive understanding of the composite dynamics influencing unintentional injury behaviors among toddlers. This approach, grounded in both theory and empirical findings, provides a robust foundation for future research and highlights the need for health professionals and educators to consider the multifaceted interaction of these factors when designing injury prevention programs for young children.
Conclusion
The highlight of this study is the indirect connection of parental locus of control to a child’s health and injury behaviors because the results suggested a direct path from an internal and external locus of control to the perceived vulnerability, which further leads to injury behaviors in alliance with a child’s temperament. Moreover, this study provides evidence that parents with a higher level of perceived vulnerability have a powerful impact on a child’s injury behavior because the more the parents are concerned, the lower the rate of injury among children, and a moderating factor is temperamental characteristics. Although regulatory guides are necessary to teach parents about safety methods to prevent future injuries, additionally, they need to manage their health locus of control, and the consequent perceived vulnerability of a child will impact accidental injuries in children. Further research investigating the children’s playground design and outdoor programs that promote positive risk-taking behavior should be addressed to provide a new foundation for interventions to prevent unintentional injuries among children.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee approval vide Ethics Committee of Nanchang Institute of Technology, Jiangxi, China. Dated: 13 May 2023. Written/verbal informed consent was taken from all the participants. The study was carried out in accordance with the principles enunciated in the Declaration of Helsinki.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.