
Abstract
Background:
Children, especially those with neurodevelopmental disorders, often experience challenges in memory functioning. This literature directs to the imperative implications of working memory (WM), especially in academics.
Objective:
Given the distinct nature of WM in children and those with neurodevelopmental disorders, our study explored the role of alpha and beta visual entrainment on their WM performances.
Methods:
NCPs (n = 19) and CPs with ADHD and comorbid conditions of autism (n = 15) participated in our study. We adopted a repeated measure intervention-based design along with alpha-and-beta visual entrainment. Pretest, posttest, and follow-up data were collected using digit span tests. Electroencephalography (EEG) was further recorded during the entrainment phase. We administered statistical and coherence factor analysis to derive our results.
Results:
We observed that experimental participants performed better following the visual entrainment sessions. We further observed that alpha entrainment affected the digit span scores among clinical participants, whereas beta entrainment affected the performance of the nonclinical group. The entrainment effects additionally varied depending on the participant’s clinical symptoms. However, we found negligible long-term entrainment effects on their WM.
Conclusion:
Our observations explore the probability of individual effects of alpha and beta entrainment sessions on children’s WM performances and open an avenue for further research in the clinical domain. The study suggests translating brainwave entrainment into an intervention to promote cognition among children, especially those with neurodevelopmental disorders.
Introduction
Working memory (WM) is the cognitive ability to hold limited information over time by controlling, updating, and manipulating information.1–3 Among children, WM plays an important role in the field of learning, mainly due to its information processing approach.4–7 Children’s academic success is majorly supported by attention and WM capacity.6,8 However, children diagnosed with neurodevelopmental disorders, such as attention-deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD), often have impaired WM systems.9,10 These impairments intensify further due to the comorbid nature of ADHD and ASD. 11
Research comparing the WM performance of typically developing children and those with ADHD/ASD shows impaired performance in the latter group.12–14 However, factors, such as age, the symptom subtype (hyperactive, impulsive, inattentive, and combined), and general intelligence also affect the performance of the clinical participants (CPs)15–18 and may account for the mix-results available in the related literature. 2 Nonetheless, cognitive deficits in ADHD and ASD further predict academic challenges, socio-behavioral issues, and difficulties leading a quality life.19–22 Further, ADHD diagnosis often stems from the time when children start experiencing academic challenges. 23
While several WM theories exist,24–26 Baddeley’s multi-domain model, consisting of the central executive, the phonological loop, and the visuospatial sketchpad, is the most associated with ADHD research. 24 Further, Barkley’s inhibition model indicates the role of WM deficits as the endophenotype of ADHD, 14 which is further substantiated by the core symptoms of inattentiveness, hyperactivity, and impulsivity outlined by the DSM-5. 27 Further, functional magnetic resonance imaging (fMRI) studies have associated poor WM among ADHD cases with structural and functional deficits in the caudate and other brain activations such as the basal ganglia and medial prefrontal cortex.28,29
Recent research has highlighted the role of brainwaves in the pathology of ADHD symptoms. Frontocentral theta band activity is associated with cognitive control and WM, thereby suggesting the role of alpha-theta coupling in the assimilation of task-relevant information. 30 Alpha oscillations in the top-down executive control regulates attention and WM tasks by selectively inhibiting or disinhibiting the associated brain areas. Since children with ADHD experience challenges in these domains,31–34 various studies have focused on the role of alpha oscillations in their cognitive systems. For instance, the atypical regulation of alpha band is additionally associated with ADHD, ASD, and their comorbid conditions. 30 Thus, the importance of WM for cognitive demands and academic success, and the discrepancies in the related brain activations between the clinical and nonclinical cases necessitate intervention-based research to promote its capacity among individuals.
Although interventions, such as pharmacotherapy, behavioral therapy, and cognitive therapy, are majorly used for such disorders, they often have limitations, such as a lack of long-term benefits and inaccessibility to treatment.35–37 Further, the demand to improve cognitive deficits among ADHD/ASD cohort has brought out an over-medicalized model of ADHD leading to increased misdiagnosis and pharmacological exploitation by individuals to enhance their cognition.38–40 Although an intervention for WM can be beneficial for children to improve their competencies, 41 a noninvasive intervention without a pharmacological influence is necessary to combat the challenges of pharmacological exploitation and address the limitations of the existing therapies.
The relevance of brain oscillations in memory has gained increased popularity among the scientific community. 42 Brainwave entrainment (BWE) is a sensory stimulation that naturally induces oscillatory rhythms, such as theta, alpha, beta, and gamma in human brains. 42 Growing BWE research since the 1980s has signified its scope in the field of cognition.43,44 From adopting BWE as a tool for alleviating headaches and migraines45,46 to improving memory and attention, among others,47,48 we have come a long way in establishing its therapeutic relevance. Recent studies have established BWE’s predominant role in improving various memory domains.43,49,50
Although meta-analysis findings support the effectiveness of BWE in cognition, they also indicate the potential effect of the study’s methodological differences on the magnitude of research outcomes. 51 While there is a demand to improve the cognitive skills of children with psychological impairments, 19 most research has been conducted on the healthy adult population.52–54 Hence, there is a need to substantiate BWE as a treatment modality for the children. Further, there exists an additional necessity to utilize EEG measures for exploring neurological changes during cognitive processing. 55
Thus, on one hand, there is a need for establishing a non-pharmacological intervention for improving cognition among children diagnosed with ADHD, while on the other hand, BWE has been showing promising results for improving cognition. Consequently, the current study aims to (1) explore the effect of alpha and beta visual BWE on children’s memory (digit span) scores, (2) to establish an association between the digit span scores and EEG entrainment measures, and (3) to compare the digit span scores and EEG findings between nonclinical participants (NCPs) and CPs.
The digit span task has been extensively used to measure WM in clinical research and practice. 1 It is a subset of the Weschler Scale and consists of digit forward (DF) and digit backward (DB) tasks.2,56 The former, considered to be a measure of short-term memory, requires the immediate recall of the digits presented orally.1,56 While the latter, closely associated with WM, requires the oral recall of the digits in the reverse order.1,56 Research suggests the use of digit span tests as one of the primary paradigms to assess cognition due to its indication of the span of apperception and active reordering process.1,57 Further, the resting state neurophysiological activity patterns differ in children with neurodevelopmental disorders and typically developing children. 34 Thus, understanding the comparative effects of BWE on these distinct populations, along with EEG, will assist in the systematic characterization of BWE intervention.
Material and Method
Sample Characteristics
A total of 34 children participated in the study, excluding the 21 dropouts. Out of the 34 participants, 19 were in the nonclinical group (M = 11.18, SD = 2.07) and 15 were diagnosed with ADHD (clinical group) (M =10.73, SD = 2.45). Of the 21 participants who dropped out, some did so due to their inability to travel long distances, and difficulty in managing school/cocurricular work along with participating in the study. A few others dropped out in the middle of the sessions due to their unavailability on the required dates.
CPs were selected based on government certificate that provides the official diagnosis and IQ. Comorbidity with ASD (mild to moderate) were also observed. In some of the cases, participants were diagnosed with moderate ADHD and mild ASD, as also seen in the existing literature. 58 Although we aimed for only ADHD cases, due to the unavailability of the required sample size, CPs with comorbid conditions of mild ASD were also selected. All participants spoke Hindi and English languages. The age range was strictly maintained at 7 to 14 years for both groups. The exclusion criteria included individuals with a history of epilepsy and those undergoing pharmacological treatment (for both clinical and nonclinical groups). The demographic characteristics of the participants are summarized in Appendix 2.
Research Design
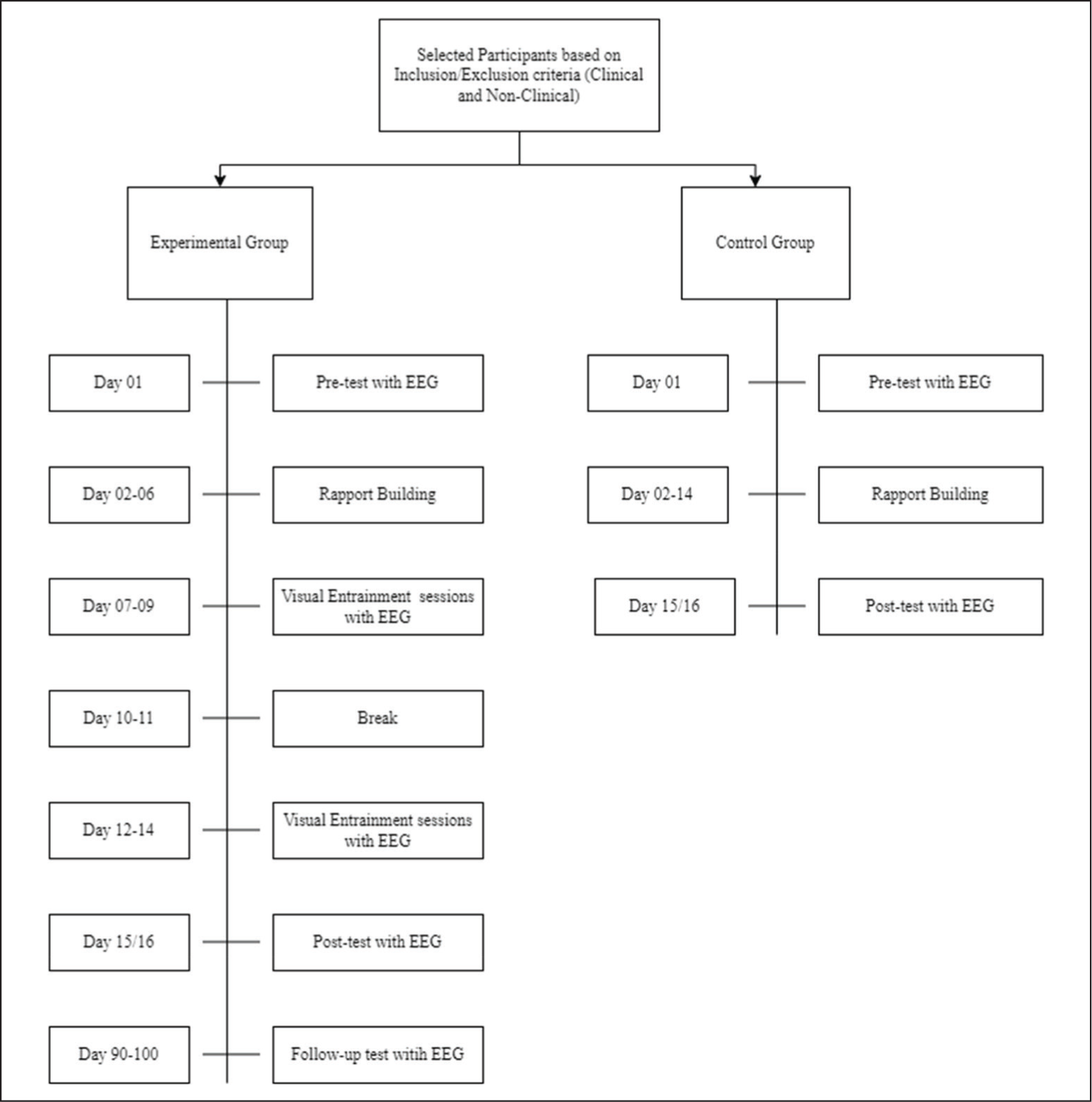
The study utilized a matched control, repeated-measures design with convenience sampling. We categorized the participants into two broad groups, namely, NCPs and CPs, based on their clinical diagnosis. The selected participants were matched based on their age, gender, and IQ (CPs), respectively, for their categorization into experimental and control groups. We conducted the digit span tests pre- and post-intervention on all participants at an interval of 15 to 16 days (based on the participant’s availability). The study was conducted in a technical institute’s laboratory in Mumbai.
Participants in the control group did not receive any entrainment and were encouraged to follow their daily routines, provided they were not participating in other cognitive training sessions and medicated treatments. The experimental procedure is illustrated in Figure 1. Due to their behavioral symptoms, the CPs underwent entrainment with their eyes open. They were engaged in storytelling and were given clay to reduce hyperactivity during the sessions. EEG was recorded throughout the entrainment sessions. We conducted a follow-up test on WM tasks with the experimental group 90 days from the last entrainment session.
Equipment and Materials
Visual Entrainment
The entrainment procedure was developed by Phogat and Parmananda. 59 A digital to analog converter (MCC USB-1616HS-4) was used to provide the signal using a set of 8 LEDs mounted on a board. EEG was recorded in five entrainment phases, as summarized in Appendix 1 (The EEG was conducted in five sessions. The first session was the resting state (dark room with no stimulation), followed by visual entrainment of alpha frequency, resting state, visual entrainment of beta frequency, and resting state. Each session lasted for 10 minutes. The total duration of EEG per day was 50 minutes. These sessions continued for 5 days). All sessions were conducted in a quiet, dark room. The lights were directed at the participant’s eyes at a distance comfortable to them.
Behavioral Tasks
Personal Data Record Form. We administered a self-developed survey form to record participant’s demographic characteristics.
The Digit Span Task. The test-retest reliability scores of DF and DB tasks correlate at 0.96 and 0.73, respectively. 56 The digits are presented at random, auditorily, and the participants are asked to repeat the digits, either forward or backward. 60 The string of digits gets progressively longer at every trial. 56
EEG
Electrode Placement. EEG electrodes were fitted on the participant’s head according to the international 10 to 20 electrode placement system. 61 Apart from the reference electrode (placed on the forehead), and the ground electrode, the other electrodes were placed in the participants’ occipital lobe (O1, O2, Oz), because of the entrainment’s nature and the convenience of the CPs. 62 Before beginning the EEG recording, the impedance of all electrode positions was checked and maintained below 100 kΩ for consistency across participants.
EEG Recording. The EEG software package called “Acquire Ink” (SuperSpec) was used for recording brainwaves during the entrainment sessions. It provided a time series to observe recorded brainwaves. The wave recording format was then converted into MATLAB (version 2021a) files according to the duration of the sessions. All wave-recording formats were processed using MATLAB’s smoothing function and were checked both visually and using an automated artifact removal algorithm to ensure that all movement artifacts were removed. The analog EEG waves (amplitude measured as voltage over time) were sampled at a rate of 250 Hz. They were translated by the MATLAB software into digital values accounting for the voltage of each 10-second epoch.
Analyses
Statistical Analysis
We analyzed data using the Statistical Package for Social Sciences, Version 22.0 for Windows (SPSS 22.0). The confidence level was fixed to 0.05 to interpret the significance of the results in the current study. Independent and paired-sample t-tests were used to explore the mean differences in the scores between and within the experimental and the control groups, respectively. Friedman’s tests were computed to compare the experimental groups’ pretest, posttest, and follow-up tests.
EEG Analysis
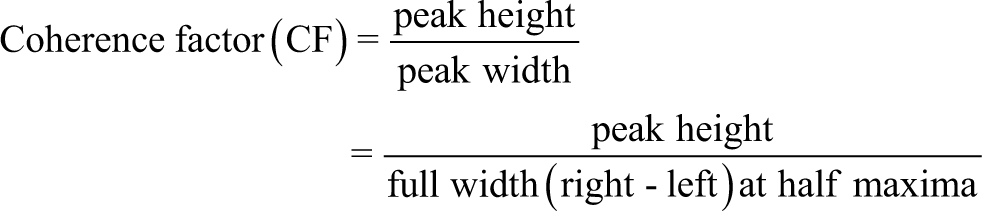
Coherence factor (CF) was calculated for the alpha and beta peaks for each individual and the respective sessions.63,64 It quantifies the degree of BWE to the external stimuli (10 Hz and 15 Hz visual stimuli). The CF value was then correlated with the change in scores (posttest–pretest) of the digit span test, using Pearson’s correlation and graphical methods:
Ethical Considerations
The Institutional Review Board approved the study. The caregivers of all participants signed the consent forms. Additionally, all participants also signed the assent forms. Further, clinical psychologists were present during all sessions concerning CPs.
Results
Outlier Detection
In the outlier detection algorithm, the test scores were put in an array to calculate the standard deviation. Test scores 2.5 times higher than the standard deviation of this array were considered outliers and were exempted from further analysis. Further, participants with higher score improvements were contacted to check for practice effects. Following the outlier detection results, only one participant from the clinical group was excluded from further analysis. Three NCPs and two CPs were additionally excluded from analysis due to miscellaneous factors such as medication, corrupt data, dropout from the session, and hyperactivity. Hence, 16 NCPs and 13 CPs were selected for the final analysis.
In the following sections, given the limited sample size of our study, we have looked at an individual’s CF and psychometric scores to derive probable associations to get an in-depth understanding of our findings. Through these observations, we aim to develop larger hypotheses for future research.
The Shapiro-Wilk test was conducted to examine the distribution of the participant’s scores. The descriptive statistics of both clinical and nonclinical groups are summarized in Appendix 3. None of the CPs could perform the digit span backward (DSB) task. Hence, only the digit span forward (DSF) scores have been statistically analyzed.
NCPs
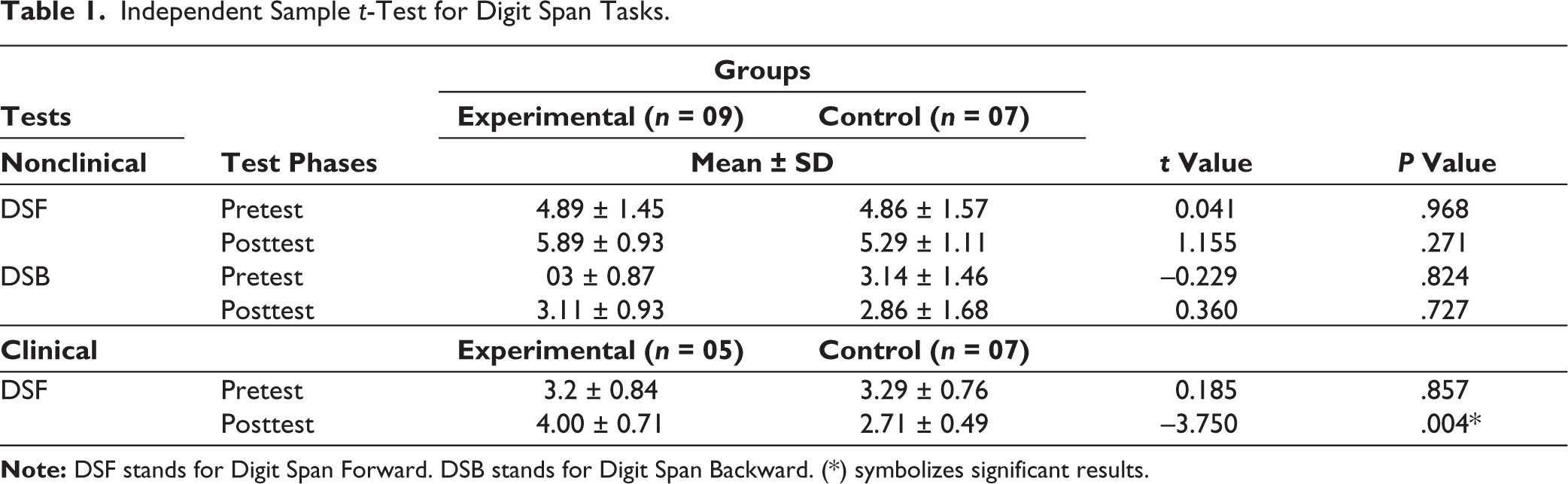
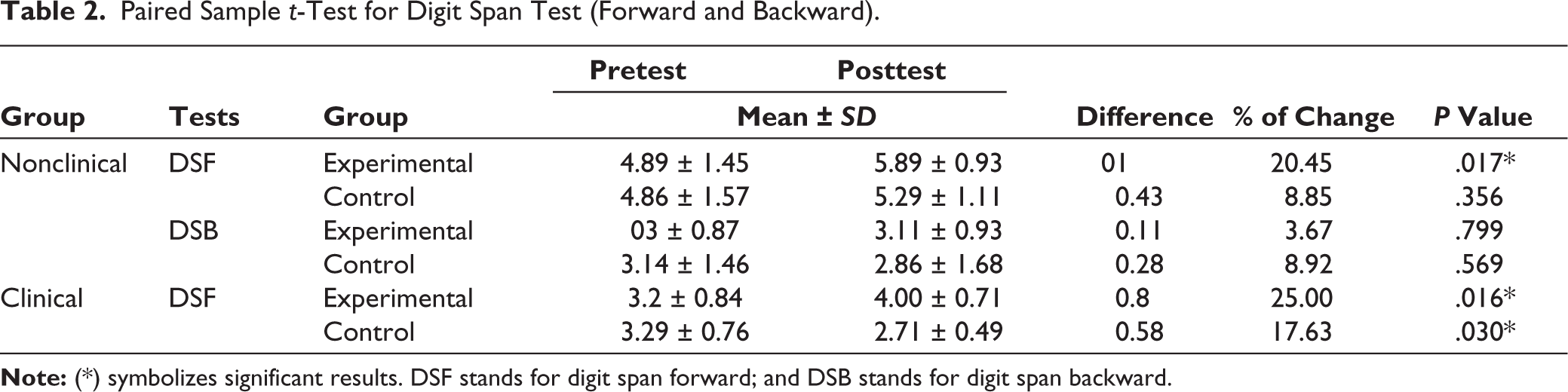
The independent sample t-test on digit span scores (forward and backward) suggests no significant differences between the experimental and control groups. However, findings of the paired sample t-test on DSF show a significant difference between the pre- and post-test scores of the experimental group only. Tables 1 and 2 summarize the statistical findings. Thus, the findings suggest a lack of visual entrainment effect on the DSF and DSB.
Independent Sample t-Test for Digit Span Tasks.
Paired Sample t-Test for Digit Span Test (Forward and Backward).
EEG Data Analysis
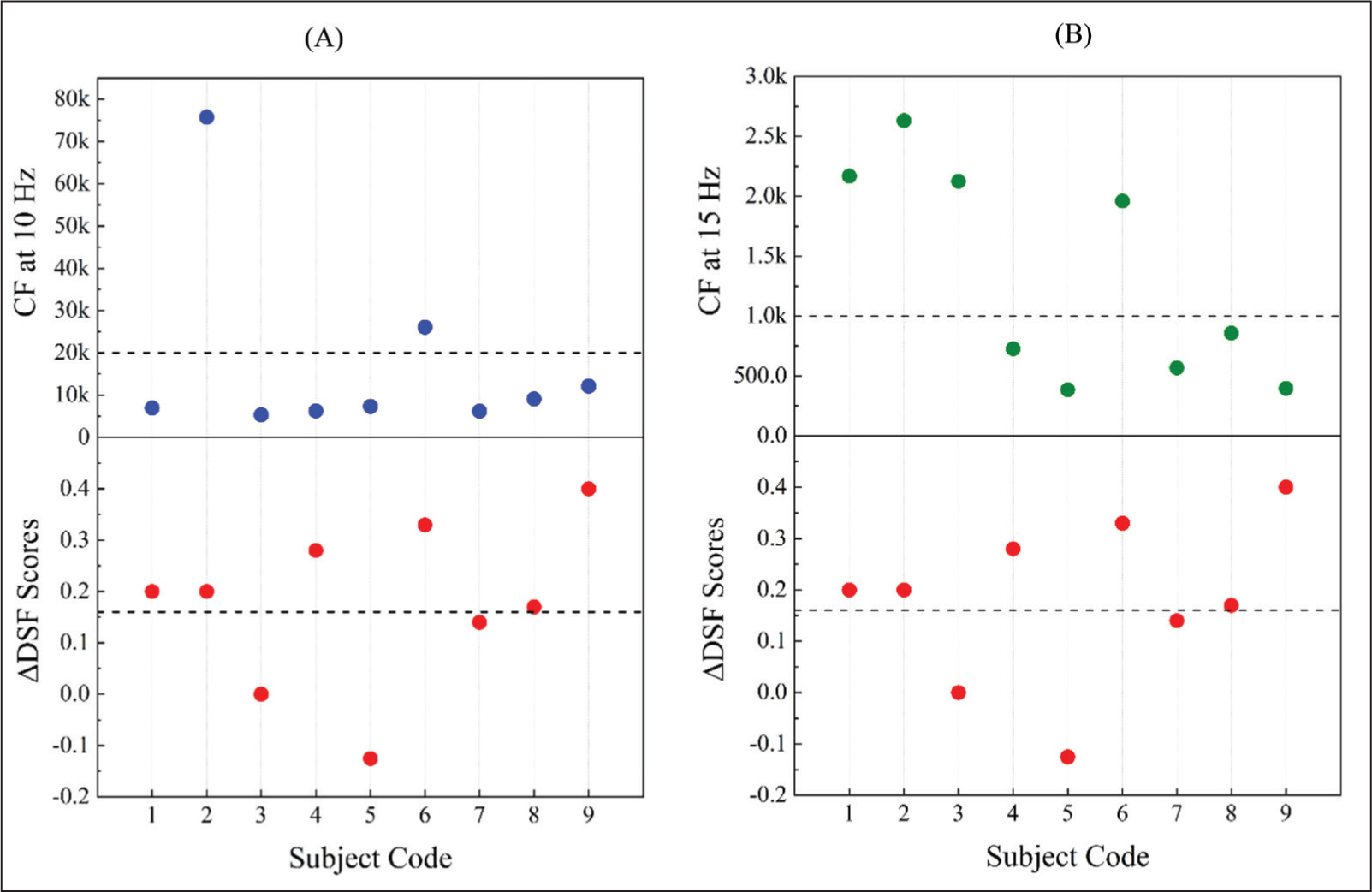
Findings from the CF analysis suggest a lack of correlation between the change in the psychometric scores and the 10 Hz CF values (Figure 2A), suggesting that a 10 Hz visual entrainment does not significantly improve the DSF scores among the participants. Nonetheless, graphical observations from Figure 2B affirm that the change in the DSF scores obtained by participants 1, 2, 5, 6, 7, and 8 correspond to the CF values, indicating a certain degree of interdependence. This finding is additionally consistent with the significant results obtained from paired sample t-test of the experimental group. Thus, visual beta entrainment (15 Hz) can improve DSF scores among the participants, provided that the significant psychometric results (Table 2) can be attributed to the quality of beta entrainment acquired by some of the participants.
CF Values and DSF Score: NCPs.
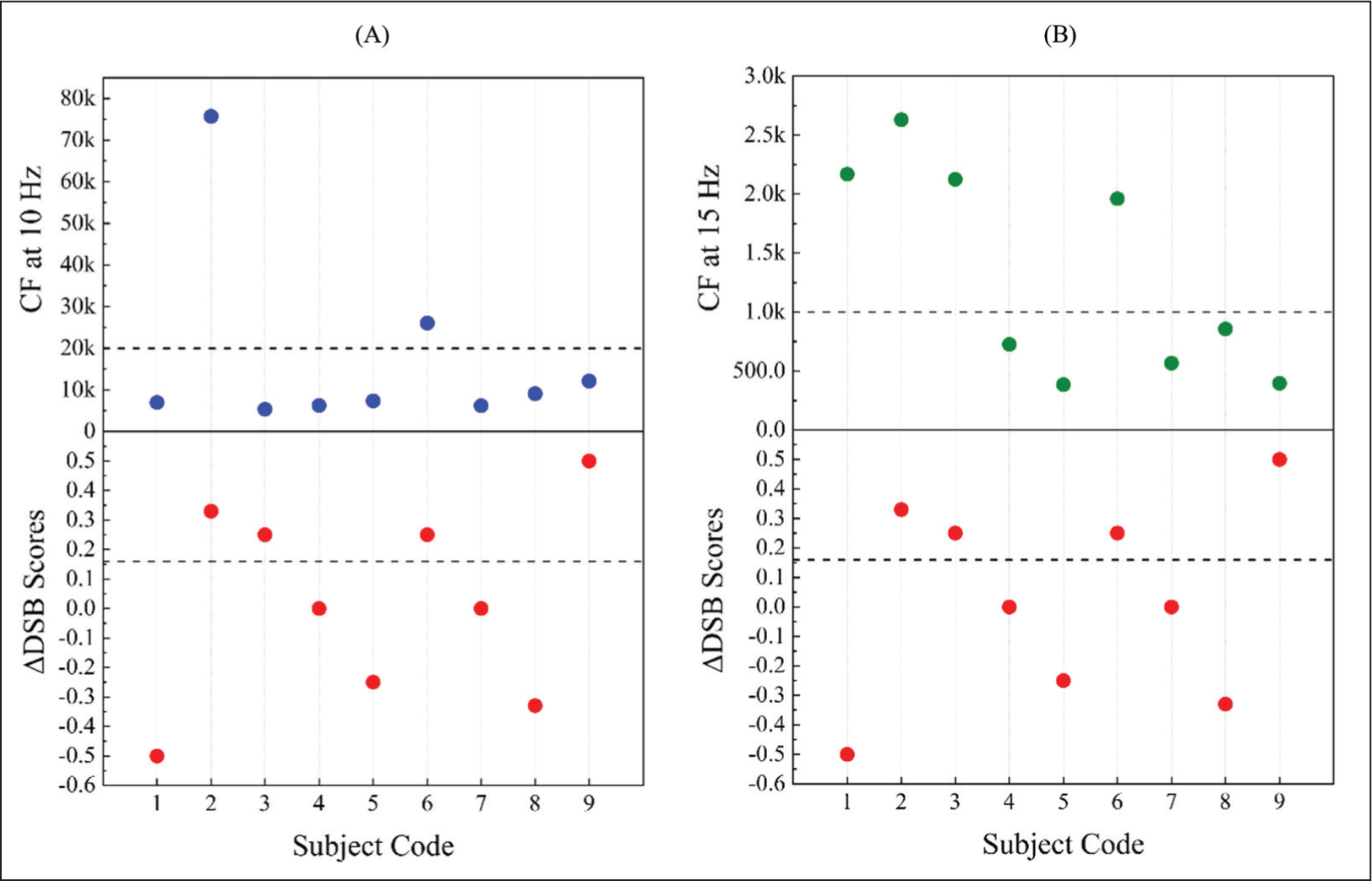
Moreover, the CF values of 10 Hz visual entrainment indicate no correlation with the change in DSB scores (Figure 3A). However, Figure 3B suggests participants 2, 3, 4, 5, 6, 7, and 8 have corresponding DSB and CF values at 15 Hz entrainment even though the psychometric analysis indicates a lack of significant results.
CF Values and DSB Scores: NCPs.
CPs
Statistical findings suggest a significant difference between the experimental and control groups, and between the pre- and post-test scores of the experimental group (Tables 1 and 2).
EEG Data Analysis
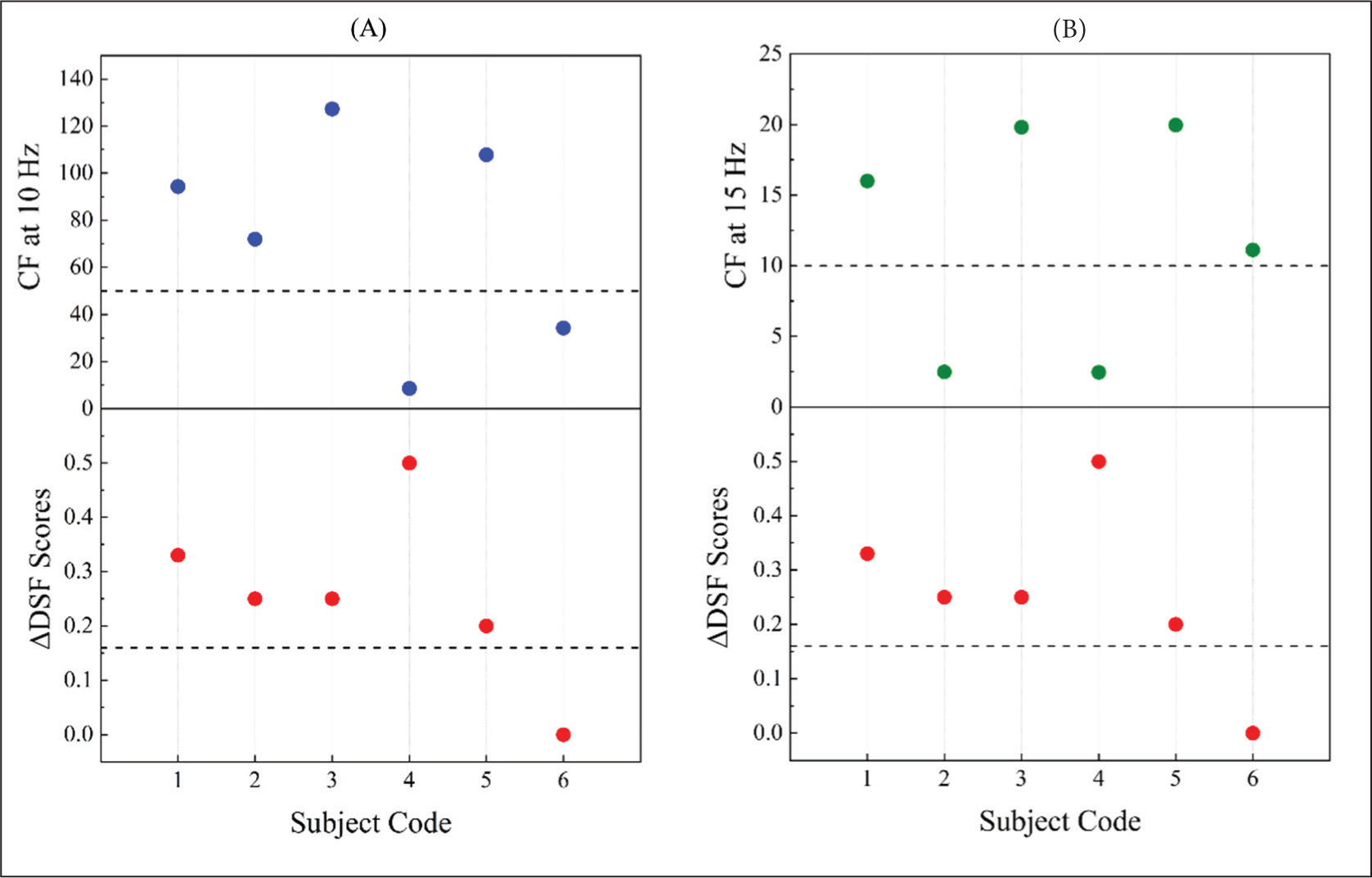
Graphical observations from Figure 4A illustrate all participants (1, 2, 3, 5, and 6) having associated psychometric and CF values at 10 Hz entrainment. However, the same does not hold true for 15 Hz entrainment (Figure 4B). The observations also suggest a higher entrainment at 10 Hz session compared to the 15 Hz session. Thus, the results indicate that 10 Hz entrainment has the possibility of improving DSF scores among the CPs.
CF Values and DSF Scores: CPs.
Follow-up Results (NCPs and CPs)
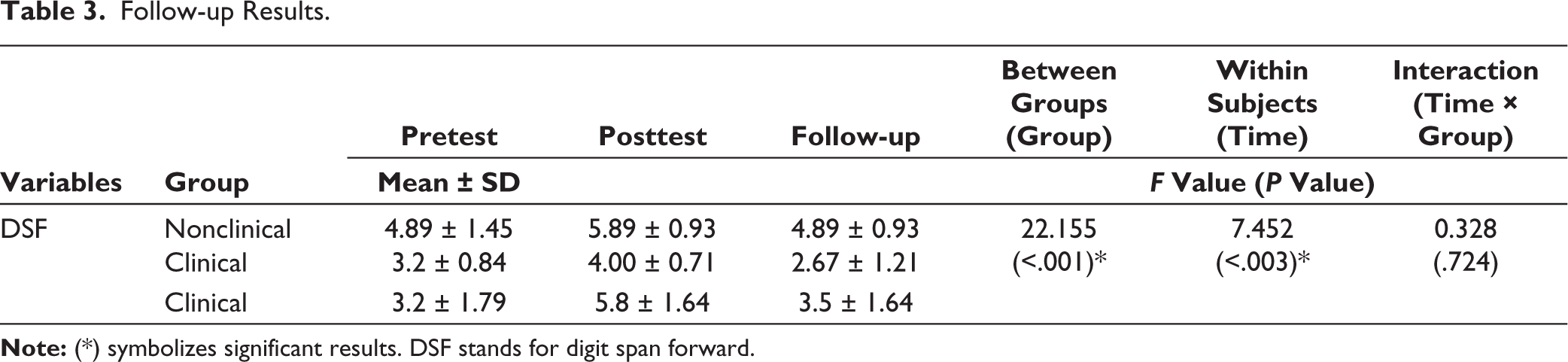
A nonparametric Friedman test of differences among repeated measures was conducted to explore any differences in the pretest, posttest, and follow-up test scores of the digit span tasks (forward and backward) among the CPs and NCPs of the experimental group. The nonclinical results indicated a lack of statistical difference in the distribution of the scores in the pretest, posttest, and follow-up tests for DSF task, χ2(2) = 5.687, P = .58 and DSB task, χ2(2) = 2.000, P = .368. Further, pair-wise comparisons also suggest a lack of significant difference in the three-time points. However, the findings from the clinical group indicated significant differences in the scores obtained at the three-time points, χ2(2) = 7.900, P = .019. Additionally, pair-wise comparisons suggest a significant difference in the scores obtained in the posttest and follow-up tests.
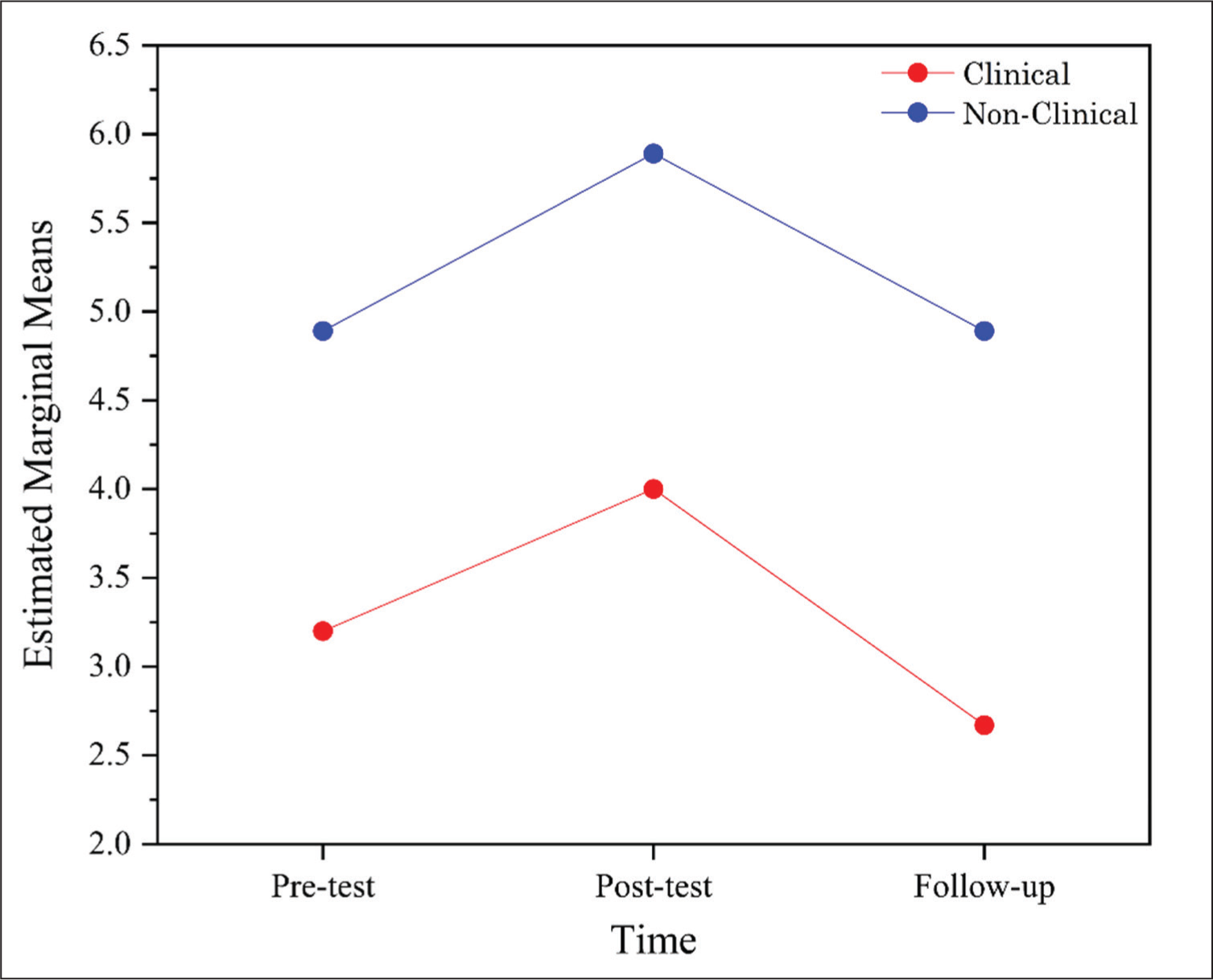
Comparative analysis of the DSF scores between the clinical and nonclinical groups indicates that the scores change over time for both groups. Observations from Figure 5 and Table 3 suggest that both groups performed better during the posttest (Pretest is marked as 1, posttest as 2, and follow-up test as 3 in all the graphs under the section “Follow-up Results.”) than the pretest; however, the scores declined during the follow-up test. Moreover, Table 2 suggests a significant difference in the treatment effect between the clinical and the nonclinical groups but a nonsignificant time × treatment interaction.
DSF Scores Overtime.
Follow-up Results.
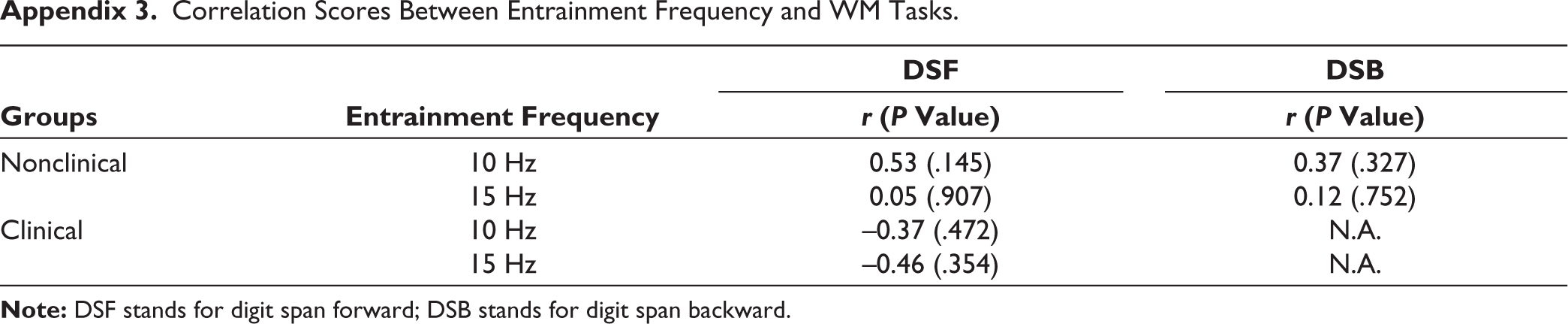
Although the associations between CF values and psychometric scores are nonsignificant (Appendix 3), graphical observations suggest the probable role of entrainment effects on the improvement in participant’s posttest performance, as elaborated in the Discussion section.
Discussion
This study explored the effectiveness of alpha and beta visual entrainment sessions on the digit span tests’ performances. Comparisons between the CPs and NCPs were investigated for the digit span scores and EEG findings. Given the limited sample size of the study, an individualized approach was also utilized to observe each participant’s reception of the entrainment and their respective psychometric scores through graphical observations.
The mean scores (DSF) among the experimental NCPs improved after the entrainment sessions but were not statistically different from the control group. The EEG findings indicated a plausible beta visual entrainment effect on NCP’s prepost significant results. However, the DSB scores remained unchanged following the entrainment sessions.
On the other hand, CP’s significant DSF scores after the entrainment sessions and the EEG findings attribute this to the possible role of alpha visual entrainment. This is an unexpected finding since we realized that the reception of alpha entrainment was higher than that of beta entrainment in both groups. A possible explanation could be that the alpha entrainment increases the baseline cortical activity of ADHD (demonstrating slow alpha wave frequency) that subsequently improves cognitive performance. 65 Given the differences in resting state EEG of CPs versus NCPs, alpha and beta entrainments may manifest differently across these two groups.
Additionally, oscillatory alpha neural activity underlying ADHD increases memory retention during a WM task through maintenance.66,67 Alpha suppresses distracting information in visual WM, increasing its capacity. 68 Even though our findings align with these theories, further research on alpha entrainment and WM among ADHD individuals is warranted. Nonclinical findings on DSF are congruent with previous research, suggesting that beta entrainment positively affects verbal WM performance. 69 Nonsignificant findings on DSB also affirm the findings of a recent study. 55
To the best of our knowledge, our study is one of the first to explore the long-term effects of alpha-and-beta visual entrainment on digit span tasks. Findings from the follow-up test show that the scores for both CPs and NCPs deteriorated after 3 months. Thus, suggesting a lack of lasting entrainment effect on digit span tasks. We additionally found differences in the treatment effect between CPs and NCPs, indicating the distinctive impact of the entrainment based on clinical pathology.
Among the NCPs, the EEG and the psychometric findings show partial correspondence with each other. For instance, although correlation between the CF and the DSB values is nonsignificant, graphical observations show a probable association between them. In our opinion, this correspondence is an interesting observation and points toward the need for exploring other entrainment markers. For example, resting state EEG, ratios of the frequency bands,65,70 and neural entrainment 51 to provide an in-depth understanding of our findings. There may be a possibility that the participant’s cognitive performance is not exclusively due to the ongoing entrainment but the changes in the brainwaves following the entrainment sessions. Moreover, although positive entrainment results exist among individuals with ADHD,53,54 limited studies and related methodological differences (such as frequencies used, memory tasks, and sample characteristics) limit the generalizability of our findings.
Observations of the CF scores suggest variability in terms of participant’s reception of the entrainment. One reason for this variation could be the individual differences in receiving entrainment, which, in turn, affects the psychometric results. Research suggests that the participant’s innate baseline alpha and beta EEG powers predict the degree and lasting duration of the entrainment. 71
Further, previous research affirms the age dependency of alpha and theta waves. 72 Higher age and lower theta and alpha band frequencies have shown associations. 73 Hence, the variations in the CF scores within the experimental group can additionally be attributed to their age and IQ levels. Moreover, the difference in LED distance (light) across participants may have contributed to the variations in the entrainment. 74 Thus, for further research, we propose that the quality of entrainment plays an important role in improving digit span memory.
Lastly, the variations in the CF values could also be due to the open-eyes (CPs) versus closed-eyes (NCPs) conditions in the groups. This, coupled with the individual differences, such as age and IQ (CPs) in receiving the entrainment among CPs and NCPs, speculates the existence of the differences in the voluntary-versus-involuntary entrainment reception. Although several studies have adopted the eyes-open versus eyes-closed comparisons for EEG recordings,34,75 the current study may be one of the first to explore active and passive entrainment modalities.
The study limitations include the small sample size and gender disparity in the clinical sample (males form a majority), thereby restricting the generalizability of the findings. Hence, our observations are a stepping stone to future research directions. Further, we have only used visual entrainment in the study. A comparative study between binaural beats and visual stimulations of alpha and beta frequencies can provide a more comprehensive picture. Lastly, given CP’s behavioral symptoms, we used a limited number of electrodes, which may have restricted data from other cortical structures.
Nonetheless, the study has strengthened the understanding of BWE mechanisms by including children with both clinical and nonclinical characteristics as the sample. Further, the study has also, for the first time, attempted to explore the long-term benefits of the BWE sessions. It additionally looks at both statistical analysis and graphical observations of participants’ scores which highlight the differences based on age, IQ, and innate brainwave rhythms contributing to individual differences for entrainment reception.
In summary, our study indicates that visual entrainment sessions can improve digit span performance among participants. Increased cognitive demands and stress among children and cognitive challenges among ADHD children necessitate successful replication and further studies to establish BWE as a therapeutic intervention for improving their cognition.
Key Messages
Participant’s psychometric performance on WM task improved after alpha and beta entrainment sessions. The findings suggest the differential effects of alpha and beta entrainment sessions on the clinical participants and nonclinical participants, respectively. Individual differences exist in the reception of the entrainment among participants. Results suggest the higher the quality of entrainment, the better is the participant’s improvement in psychometric scores. Participant’s baseline alpha wave, age, and IQ may affect their receptivity towards entrainment.
Footnotes
Acknowledgements
We would like to thank Ms Priyanka Parthasarathi, Mr Mayur Jartarkar, Dr Jai Tushar, Mr Snehashis Alam, and Mr Mohd. Mubashshir for reviewing and assisting with the technicalities of our manuscript. We also wish to extend our appreciation to the Department of Physics, IIT Bombay, and the Department of Humanities and Social Sciences, BITS Pilani Goa campus, for providing us with access to various resources.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Clearance Statement
The clearance has been received from the concerned Institute Review Board. Additionally, written consent and assent were obtained from all participants and their caregivers.
The study was accorded Ethical Committee Approval vide Ethics Committee (mention Name and Institute) No. 2020-10 dated 26-02-2020. Written and Verbal Informed Consent was taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project is partially funded by CSIR (Richa Phogat).
Appendix
Correlation Scores Between Entrainment Frequency and WM Tasks.
| Groups | Entrainment Frequency | DSF | DSB |
| r (P Value) | r (P Value) | ||
| Nonclinical | 10 Hz | 0.53 (.145) | 0.37 (.327) |
| 15 Hz | 0.05 (.907) | 0.12 (.752) | |
| Clinical | 10 Hz | –0.37 (.472) | N.A. |
| 15 Hz | –0.46 (.354) | N.A. |