
Abstract
In Tourette syndrome (TS), apart from multiple motor and vocal tics, there are often myriads of associated conditions apparently similar to attention-deficit-hyperactivity-disorder (ADHD), obsessive-compulsive-disorder (OCD), mood-and-conduct disorder, learning difficulties, etc. On the other hand, tic disorders often occur as co-morbidity with many neurodevelopmental disorders such as ADHD, OCD and mood disorders, and pharmacotherapy of these behavioral conditions may worsen the tics. So, the confusion lies whether to separately code and manage the different neurodevelopmental disorders or assume an umbrella construct of “TS-plus,” as suggested by some researchers. In this background, we share three cases of children and adolescents having multiple tics with mixed behavioral presentations of ADHD/OCD/mood disorders that created a lot of diagnostic dilemma and treatment-related complications in prior psychiatric consultations. They were finally diagnosed as “TS-plus” and managed with low-dose-risperidone-mono-pharmaco-therapy and psychological interventions. In conclusion, psychiatrists should be vigilant for Tourette-syndrome while handling children with repetitive motor behaviors along with hyperactivity, obsession-compulsion, mood-conduct, etc. Assumption of an umbrella-construct approach of “TS-plus” may be beneficial in limiting the number of diagnosis and their separate pharmacotherapy, which may worsen the clinical scenario.
Introduction
Tourette syndrome/disorder (TS) is a childhood neurodevelopmental disorder with multiple motor and vocal tics lasting for more than one year, not necessarily concurrently but also not secondary to any substance or general medical condition.1,2 For diagnosis, tics are to be differentiated from other childhood movement disorders such as chorea (Wilson’s), myoclonus, automatism of complex partial seizures, stereotypy in autism and compulsive movements of obsessive-compulsive disorder (OCD). 2 Tic disorders in their different forms often appear as a comorbidity in different childhood neurodevelopmental disorders such as attention-deficit hyperactivity disorder (ADHD), OCD, learning difficulties, anxiety, mood-conduct disorders, etc.3,4 On the other hand, in TS, during its chronic waxing–waning course, behavioral features similar to obsession-compulsion, inattention-hyperactivity and mood and conduct often appear in a fleeting–fluctuating manner independent of tic symptoms or at times may precede tic symptoms.5,6 This creates a lot of diagnostic confusion among clinicians who often miss the diagnosis of TS and consider them ADHD, OCD, or mood-and-conduct disorders. Based on that heterogeneity of presentation, some researchers 7 subdivided the TS patients in three groups: (a) “pure TS”—those with solely motor and phonic (simple vocal) tics; (b) “full-blown TS”—those who exhibit coprolalia/echolalia/palilalia in addition; (c) “TS-plus”—those with additional behavioral problems. This group of researchers proposed a multidimensional TS-Global Scale (TSGS), 8 which also accounts for associated behavioral conditions other than simple–complex motor and vocal tics, which may save time for the clinicians to evaluate the treatment outcome of TS patients other than using separate rating scales for tics, ADHD, OCD, etc. However, this umbrella-construct approach has eluded the nosology till date. Apart from diagnostic dilemma, clinical situations become more complex with regard to selection of treatment in TS-plus conditions, as common medicines used in ADHD (stimulants) and OCD (SSRI-selective serotonin reuptake inhibitors) may worsen tics while typical antipsychotics may cause extrapyramidal and cognitive side effects. 5
With this background, three cases of “TS-plus” in children and adolescents, handled by the authors in their respective clinics, are presented here with proper informed consent of their parents, where confusion in diagnosis and treatment caused a lot of distress to those children.
Case I
A 14-year-old Muslim boy from lower socioeconomic family status with a rural background, with below-average scholastic performance and social skill since childhood, nil contributory birth, past medical psychiatric history, and family history, presented with a five-year-history of repetitive grimacing, shrugging, touching, tapping and occasionally writhing on the ground without any alteration of consciousness. There were also repetitive senseless utterances and unprovoked shouting of obscenities. He used to remain anxious, restless, and agitated, left schooling for two years, mostly roamed around and avoided others. Much to his plight, he was diagnosed and managed differently by different psychiatrists during the course of illness. Initially, he was diagnosed as having complex partial seizure due to non-specific EEG changes and treated with carbamazepine (600 mg), due to which he developed Steven–Johnson syndrome; the medicine was omitted and managed conservatively by a dermatologist. After a gap of six months, another psychiatrist diagnosed him as having ADHD with obsessive-compulsive symptoms and treated him with a combination of atomoxetine (20 mg)/fluoxetine (20 mg)/risperidone (2 mg), due to which his movements worsened along with severe agitation. Immediately, on changing the psychiatrist for the third time, he was diagnosed as having mania-with-psychotic symptoms, was treated with divalproex (750 mg)/haloperidol (10 mg) per day. He developed acute dystonia and was rushed to hospital emergency. After a six-month lay-off, the child came for the current treatment with the author. His course of illness was fleeting–fluctuating and at times improving without any treatment but a chronic downhill functioning was obvious.
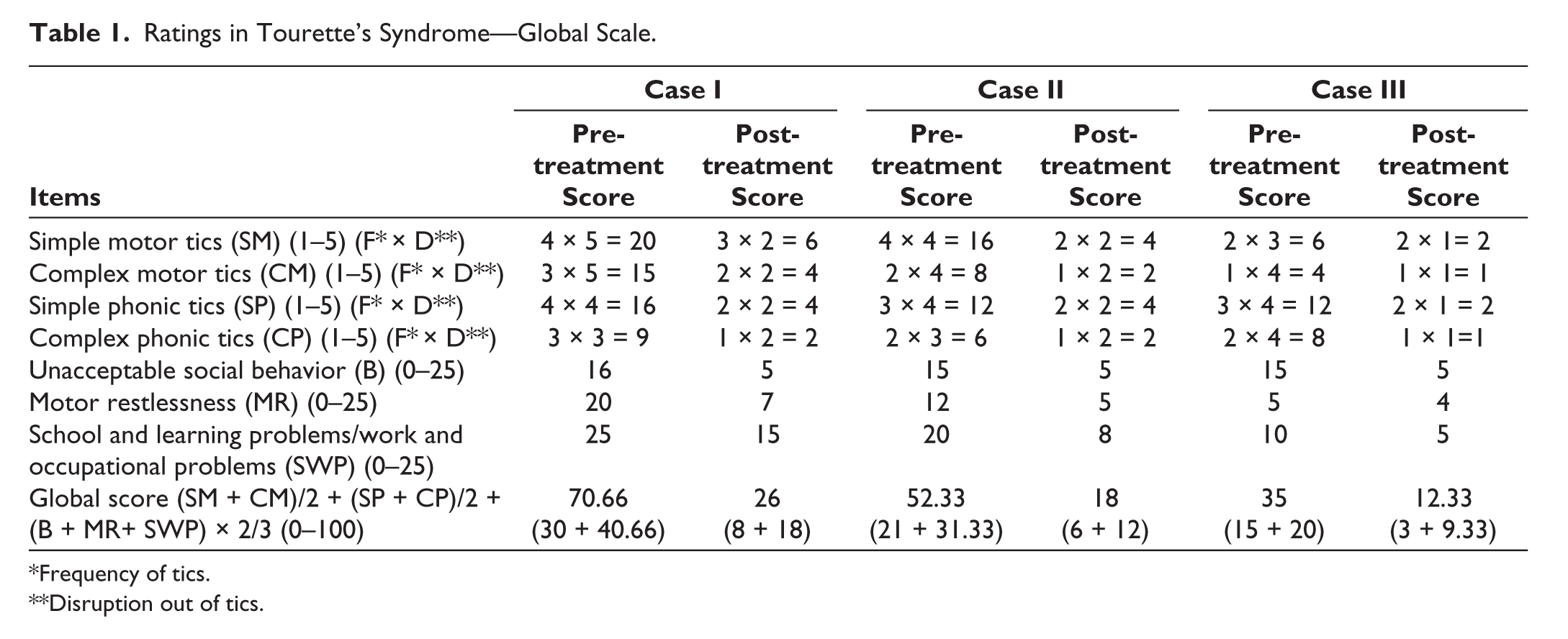
On current contact a provisional diagnosis of TS was made after exclusion of KF-ring by slit-lamp examination of the eyes and EEG, CT-brain, and serum ASO titer showing normal report. Physical examination was normal, and MSE revealed irresistible “urge” before those movements and accompanying utterances and not finding “peace” until those were completed, which differentiated it from stereotypic movements. There was no additional subjective complaints of intrusive thoughts and doubts or a need for repetitive ritualistic behavior. Diagnosis was kept as “TS-plus” after exclusion of Wilson’s, PANDAS, seizure, stereotype movement disorder, and OCD. The patient was monitored with Tourette’s Syndrome Global Scale (TSGS). 8 His baseline TSGS score was 70.66 (tic score 30 + other behavior scores 40.66), which fell in the extreme category (60–100, tic score > 25 and other behavior score >30) as per TSGS (Table 1). He was treated with risperidone (0.5 mg) twice daily along with a tapering dose of clonazepam (1 mg) over the next four weeks. Apart from pharmacotherapy, the patient was subjected to relaxation and habit reversal therapy (HRT). The patient tolerated the medicine and gradually improved not only with regard to tics but also in all other domains of associated abnormal behaviors. After four weeks, he continued only on risperidone (0.5 mg) twice daily and showed a TSGS score of 26 (8 + 18) on follow-up at six weeks (Table 1). After improvement of symptoms, his IQ was assessed, which came to 80, and he was rehabilitated in some vocational work. His improvement remained stable in functional daily activities with intermittent fluctuations in symptoms over the next one year of observation with the same treatment.
Ratings in Tourette’s Syndrome—Global Scale.
*Frequency of tics.
**Disruption out of tics.
Case II
A 10-year-old Hindu boy from lower socioeconomic urban family status studying in class IV, with nil contributory birth development, past medical psychiatric history, and family history, presented with gradually progressing poor attention in studies, restlessness, and some repetitive behavior characterized by repeated touching of various objects along with occasional transient shrugging of the shoulders and belly, grimacing, and intermittent grunting for the past two years. For the past few months, the patient started spending more time in the toilet and repeated, prolonged washing behavior. He was still maintaining school and other daily activities. On psychiatric consultation, a diagnosis of obsessive-compulsive spectrum disorder was made, and the patient was put on fluoxetine (20 mg) and clonazepam (0.5 mg). Within 15 days, the patient’s abnormal jerky movements along with vocal grunting became very much prominent with the occasional appearance of obscene utterances and no improvement in touching and washing behavior. The patient stopped going to school, mostly remained anxious, restless, and agitated with persistent irresistible “urge” before those movements-grunting and not finding “peace” until those were completed. On examination, apart from multiple simple and complex motor and vocal tics with irresistible urge and anxiety, there was report of repetitive intrusive urge for washing and lack of satisfaction on prolonged washing. Diagnosis was revised as TS with obsessive-compulsive behavior after ruling out Wilson’s by the slit-lamp examination of the eyes and PANDAS by ASO-titer. His baseline TSGS score was 52.33 (tic score 21 + other behavior scores 31.33), which fell in the severe category (40–59, tic score 10–30 and behavior/social score 20–45) as per TSGS (Table 1). Medications were changed to risperidone (0.5 mg) twice daily and a short course of tapering dose of clonazepam (0.5 mg) for two weeks, along with relaxation and HRT. On the next follow-up at six weeks, his TSGS score was 18 (6 + 12). The patient resumed schooling with normal daily activities. During follow-up over the next one year on risperidone monotherapy, he remained stable with intermittent short, lasting fluctuations in tics, which were managed with relaxation and HRT.
Case III
A 16-year-old girl from Hindu middle-socioeconomic urban family status studying in class X, with nil contributory birth development and family history, came with complaints of irritability, frequent anger outbursts, excessive demands, age-inappropriate temper tantrums, and frequent oppositionality with parents over the past six months. She was already diagnosed as having Tourette’s syndrome since 12 years of age and was well maintained on risperidone (0.5 mg) twice daily till six months back, from when her complaints of mood disturbance gradually started along with worsening of tics. Her earlier psychiatrist diagnosed it as TS with comorbid hypomanic episode and tried to manage with twice daily dose of risperidone (2 mg) and sodium valproate (300 mg). She came with side effects of nausea, cog-wheel rigidity, tremor, not much improvement in presenting symptoms of irritability, increased demands, and disregard for parental authority. There was mild elevation in enzymes on liver-function test. Her diagnosis was revised as TS-plus-mood-conduct/oppositional symptoms along with adverse drug reactions. Medications were changed with reduction of risperidone to 0.5 mg BD; clonazepam (1.5 mg) and propranolol (20 mg/day) were added in divided daily dosage, tapering over four weeks in place of valproate. Supportive counseling and psychoeducation were done to explain the emergence of mood-conduct issues in the course of TS, and the client was referred to a psychologist for relaxation and cognitive-behavioral therapy for her newly emergent mood-conduct symptoms. Her parents were counseled to assume non-confrontational attitude. Her baseline TSGS score was 35 (tic score 15 + other behavior score 20), which fell in the moderate category (25–39, tic score 10–20 and behavior/social score 10–30) as per TSGS (Table 1). She improved on treatment and at follow-up after six weeks, her TSGS score was 12.33 (3 + 9.33). Her condition remained stable over the next one year of follow-up till current reporting with risperidone monotherapy and parallel psychological intervention with relaxation and HRT.
Regarding non-pharmacological interventions in all the above cases, they were done by separate clinical psychologists in their respective clinics on referral basis, whose outlines were known to the authors, but not the detailed planning and implementation.
Discussion
The above cases are glaring examples of diagnostic confusion in “TS-plus” where confusion in treatment selection led to further distress in those children. Psychiatrists are more conversant with behavior problems of ADHD, OCD, mood disorders, and encounter tics as comorbidity in these childhood conditions.1,2 As evident in Cases I and II, the diagnosis of TS remained masked under the variable presentations of hyperactivity, agitation, or obsessive-compulsive behaviors. However, in our work-up we did not use any diagnostic schedules or neurocognitive assessments to unravel any other symptom domains, which could have helped in further improvement in our work-up.
Diagnosis of TS becomes obvious in “TS-pure” and “TS-full-blown” forms, as described by Leckman et al, 7 but psychiatrists come across them relatively less and TS is thought to be a rare condition. 1 With increasing field research in the past three decades, the current estimate of prevalence of TS in DSM5 is 3–8/1000 compared to previous estimates of prevalence (0.5/1000). 3 In “TS-plus” cases, whether diagnosis would be a unitary neuropsychiatry construct of only TS or there would be multiple diagnoses of psychiatric comorbidities, confusion is likely to continue. Like in Case III, where the diagnosis of TS was already established for years, appearance of new mood symptoms warrants for an additional diagnosis of hypomania or can be considered as the emergence of fleeting mood-conduct symptoms in the chronic course of TS, which is a baffling situation for the treating psychiatrist. But if these fleeting abnormal behaviors of hyperactivity, obsessive-compulsive behavior, or mood-and-conduct symptoms are considered under the umbrella construct of “TS-plus,” the medication burden may remain under control in these “neuro-typical” children, where medication side effects are always a major concern. Moreover, regarding the selection of treatment, many of the medications used for ADHD and OCD worsen tics. Effectiveness of risperidone monotherapy, as seen in the above three cases, is beyond doubt in TS.9,10 In an Indian study at NIMHANS, low-dose risperidone was the most preferred treatment for tic disorders, and children showed better improvement on mono-pharmaco-therapy along with psychological interventions than when treated with poly-pharmaco-therapy even in cases with tics with comorbidities. 4 Apart from tics, risperidone is also widely and effectively used in ADHD/OCD/mood disorders with well-known safety in childhood population. 11 This co-occurrence of a myriad of symptoms similar to ADHD/OCD/mood disorders in TS cases are well known, but their common neurobiological link is very interesting and baffling. Some recent animal studies have suggested the role of striatal disinhibition resulting from GABA-argic alterations. 12 Thus, medications such as risperidone and clonidine, which are effective in TS, probably act through manipulation of this dopamine-GABA-argic pathways of the basal–ganglia–limbic–system circuit. 10
Conclusion
In children visiting psychiatrists with a mixture of ADHD/OCD/mood-conduct symptoms, tics should be minutely examined so that “TS-plus” is not missed. In a majority of TS, associated behavioral presentations are a rule than an exception. An umbrella construct of “TS-plus” may be an effective approach of management than separately coding and treating the childhood neuropsychiatric conditions because that may often complicate the clinical scenario as evident in our cases.
Footnotes
Authors’ Contribution
Cases I and II were seen by both the authors, while Case III was solely seen by AKR. Both the authors contributed in necessary literature search and construction of the write-up.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed assent and consent were obtained from the patients and their parents respectively.
Informed Consent
Written informed consent has been taken from the parents of all the children/adolescents reported in the article.